

Abstract
Introduction
A scuba diving fatality usually involves a series of related events culminating in death. Several studies have utilised a chain of events-type analysis (CEA) to isolate and better understand the accident sequence in order to facilitate the creation of relevant countermeasures. The aim of this research was to further develop and better define a process for performing a CEA to reduce potential subjectivity and increase consistency between analysts.
Methodology
To develop more comprehensive and better-defined criteria, existing criteria were modified and a template was created and tested using a CEA. Modifications comprised addition of a category for pre-disposing factors, expansion of criteria for the triggers and disabling agents present during the incident, and more specific inclusion criteria to better encompass a dataset of 56 fatalities. Four investigators (raters) used both the previous criteria and this template, in randomly assigned order, to examine a sample of 13 scuba diver deaths. Individual results were scored against the group consensus for the CEA. Raters' agreement consistency was compared using the Index of Concordance and intra-class correlation coefficients (ICC).
Results
The template is presented. The index of concordance between the raters increased from 62% (194/312) using the previous criteria to 82% (257/312) with use of this template indicating a substantially higher inter-rater agreement when allocating criteria. The agreement in scoring with and without template use was also quantified by ICC which were generally graded as low, illustrating a substantial change in consistency of scoring before and after template use.
Conclusion
The template for a CEA for a scuba diving fatality improves consistency of interpretation between users and may improve comparability of diving fatality reports.
Keywords: Scuba diving, Incidents, Deaths, Investigations, Analysis, Epidemiology
Introduction
Some accident investigations utilise a root cause analysis (RCA) technique. This follows the ‘domino mechanism'[ 1] whereby an initial causal factor leads to other factors ending in injury or death. However, it can be difficult to determine a single causal factor as the more thoroughly an incident is investigated, the more potential causal factors appear.[ 2]
A scuba diving fatality usually involves a series of related events culminating in death. Identification of various contributory factors is hampered by the reality that most diving incident reports are relatively sparse on detail. Given the difficulty in tracking a root cause, such an analysis is more appropriately described and conducted as a 'chain of events' or 'sequential analysis' where there may be multiple possibilities at some of the stages.
The process of chain of events analysis (CEA) was first applied to diving incidents in the examination of 947 fatalities in the USA.[ 3] The incident sequence was divided into four components: (1) the trigger; (2) the disabling agent; (3) the disabling injury and (4) the cause of death. Later, CEA was applied to a series of 351 Australian compressed-gas diving fatalities.[ 4] Modifications included the re-defining of several subcategories within the four major categories of the CEA to better reflect the available data. Subsequently, others have used similar categories for their analyses.[ 5] However, in the absence of definitive criteria, there is a potential for subjectivity in the categorisation of events and classifications can vary substantively from case to case and study to study. A detailed breakdown of predisposing factors, triggers, disabling agents and disabling injuries are presented in Tables 1, 2, 3, 4.
Table 1. Predisposing factors for a scuba diving fatality .
| Predisposing factors |
| Definition: A predisposing factor (as used here) is a relevant factor that was present prior to the dive, and/or prior to the trigger occurring, and which is believed to have predisposed to the incident and/or to key components in the accident chain (e.g., the trigger or disabling agent). |
| Health-related: May include factors such as a history of cardiovascular disease, epilepsy, diabetes as well as factors such as mental or physical fatigue. |
| Organisational/training/experience/skills-related: Includes factors that may have impacted a diver’s practical readiness to dive. Factors such as the suitability of training course design and conduct and the overall dive organisation by a dive operator are included as well as the level of skill and/or experience of the diver relevant to the circumstances. |
| Planning-related: Applies to obviously poor pre-dive planning decisions, whether made well before the dive or immediately prior. This includes factors such as a decision to dive in conditions that were obviously unsuitable, or should have reasonably have been assessed as unsuitable or a decision to dive alone, among others. |
| Poor communication or coordination: If communication between buddies and/or the dive supervisor (prior to or during the dive) is poor, the opportunity of misunderstandings and unexpected and inappropriate actions is increased. |
| Absence of appropriate equipment; using obviously faulty equipment: Although this is somewhat planning-related, this particular category is equipment-specific. |
| Activity-related: Some activities (e.g., spearfishing/seafood collecting, penetration diving) are associated with particular inherent risks. For example, spearfishing is well known to attract sharks and can predispose to an accident triggered by the arrival of an aggressive shark. Penetration diving can predispose to an incident triggered by entrapment. |
| Unsafe supervision: This can apply to supervision by the divemaster overseeing a dive, an instructor supervising students or to a diver's interactions with his buddy. |
| Other: Includes anything that cannot appropriately be allocated to one of the defined categories. This category should be used sparingly and only after a serious attempt to utilise an existing category. |
| Unknown/none: There is insufficient information on which to make a reasonable suggestion of a possible predisposing factor. |
Table 2. Triggers for a scuba diving fatality .
| Triggers |
| Definition: A trigger (as used here) is the earliest identifiable event that appeared to transform an unremarkable dive into an emergency |
| Environment-related: Relates to the diving environment and may arise from the topography or conditions of the dive site itself or as a result of contact with other users or inhabitants. |
| • Conditions |
| Water − e.g., difficulty in dealing with current, swell, surge, chop, water outflow/inlet; visibility, temperature; |
| Weather − e.g., problem arising from rain, wind, lightning; |
| • Marine animal contact − e.g., aggression from shark; |
| • Watercraft-related − e.g., boat impact, propeller injury; |
| • Entrapment − e.g., tangled in line or net, disoriented in cave or wreck; |
| • Events triggered from the direct effects of immersion, submersion and/or sensory deprivation, e.g., cardiac arrhythmia. |
| Equipment-related: Includes a problem with any item of the diver’s equipment that precipitates an accident. The list below is not exhaustive and other equipment may trigger an accident and so can be included. |
| • Regulator, surface-supplied breathing apparatus or rebreather functional problem leading to gas supply reduction or interruption; |
| • Buoyancy compensator device (BCD) failure − e.g., sticky inflator, dump valve failure but not including its misuse; |
| • Weights-related − e.g., unintentional release, unable to be released but not including over- or under-weighting from the outset of the dive; |
| • Mask − e.g., leak, broken strap, broken/displaced lens; |
| • Fins − e.g., poor fit, broken strap, loss of fin; |
| • Exposure suit − e.g., tight wetsuit, flooded drysuit but not including drysuit 'blow-up'; |
| • Cylinder - e.g., valve-failure, slippage but not including problems from gas content or valve insufficiently opened; |
| • Faulty depth or contents gauge; |
| • Hose failure; |
| • Breathing hose entanglement. |
| Gas supply-related: Includes any problem relating to the on-going supply, purity and suitability of the breathing gas but not loss of gas supply due to equipment failure. |
| • Inappropriate breathing gas mixture; |
| • Contamination; |
| • Exhaustion of breathing gas supply. |
| Buoyancy-related: Includes buoyancy problems generally related to poor knowledge or skills but not problems arising from equipment failure. It includes factors such as: |
| • Overweighted or underweighted; |
| • Poor skills; |
| • Drysuit 'blow-up'; |
| • Loss of buoyancy control arising from deployment of surface marker buoy. |
| Exertion-related: Includes problems arising from situations such as carrying equipment, exiting the water post-dive, dragging a heavy object underwater, etc. but not exertion as a result of sea conditions. |
| Anxiety/stress-related: Anxiety/stress can often be associated with diving, especially in the relatively inexperienced, and can be a trigger for an accident. However, in order for this to be listed as a trigger, it cannot be assumed but must have been observed and reported by a witness. |
| Primary diver error: Diver error, which is an inherent part of many diving accidents, can be a precursor to or the actual trigger in a sequence. It can be closely associated with another trigger(s) and, in such cases, can be reported in combination. |
| Other: Includes anything that cannot appropriately be allocated to one of the defined categories. This category should be used sparingly and only after a serious attempt to utilise an existing category. |
| Unknown: There is insufficient information on which to make a reasonable suggestion of a possible trigger(s). |
Table 3. Disabling agents in a scuba diving fatality .
| Disabling agents |
| Definition: A disabling agent (as used here) is an action or circumstance (associated with the trigger) that caused injury or illness. It may be an action of the diver or other persons, reaction of the equipment, effect of a medical condition or a force of nature. |
| Gas supply-related: Includes any problem relating to the on-going supply, purity and suitability of the breathing gas but not loss of gas supply due to equipment failure. |
| • Inappropriate breathing gas mixture; |
| • Contamination; |
| • Exhaustion of breathing gas supply. |
| Ascent-related: Includes any problem that was likely precipitated by or associated with the ascent from a dive. This may include but is not restricted to: |
| • Breath holding during ascent; |
| • Gas sharing during ascent; |
| • Rapid ascent. |
| Medical-related: Includes any problem that was likely precipitated by or associated with a pre-existing or imminent medical condition (which may or may not be the same as the disabling injury). It may include but is not restricted to: |
| • Cardiovascular disease; |
| • Other medical condition. |
| Buoyancy-related: Includes buoyancy problems related to poor knowledge or skills and secondary to some trigger. It can also include loss of buoyancy control subsequent to equipment failure (e.g., loss of buoyancy subsequent to a faulty BCD). |
| • Inadequate buoyancy control underwater; |
| • Lack/loss of buoyancy on surface; |
| • Drysuit 'blow-up' subsequent to equipment failure. |
| Environment-related: Includes problems where a diver is disabled as a result of environmental circumstances such as: |
| • Adverse sea conditions; |
| • Entrapment − this entrapment is secondary to an initial trigger such as narcosis, silting, poor buoyancy or surge. It often leads to exhaustion of the breathing gas (in which case, the disabling agent is recorded as environmental – entrapment, then out of breathing gas. |
| • Impact with watercraft, rocks, reef; |
| • Dangerous marine animal contact (e.g., shark attack). |
| Equipment-related: Includes a consequence of a problem associated with an item of the diver’s equipment, but secondary to some accident trigger. |
| Other: Includes anything that cannot appropriately be allocated to one of the defined categories. This category should be used sparingly and only after a serious attempt to utilise an existing category. |
| Unknown: There is insufficient information on which to make a reasonable suggestion of a possible disabling agent. |
Table 4. Disabling injuries and causes of death .
| Disabling injuries |
| Definition: A disabling injury (as used here) is directly responsible for death or incapacitation followed by death from drowning. |
| Asphyxia: Asphyxia with or without aspiration of water and with no indication of a prior disabling injury |
| Cerebral arterial gas embolism: Gas in the cerebral arteries with or without evidence of lung rupture |
| Cardiac: Acute chest discomfort indicated by the diver, history of cardiac disease, or autopsy findings |
| Trauma: Witnessed trauma, traumatic findings at autopsy |
| Other medical: Stroke, gastrointestinal haemorrhage, carbon monoxide toxicity, etc |
| Other: This includes anything that cannot appropriately be allocated to one of the defined categories. This category should be used sparingly and only after a serious attempt to utilise an existing category. |
| Unknown: Body not recovered; no autopsy available; no indications of disabling injury at autopsy. |
| Cause of death |
| Definition: The cause of death is that specified by the medical examiner, which could be the same as the disabling injury or could be drowning secondary to injury. |
| Although the disabling injury is often more informative in determining why the diver became incapacitated, the actual cause of death can sometimes provide important information for preventative and emergency management strategies. |
To minimise subjectivity and increase consistency between investigators, it is important to carefully define the CEA categories. The aim of this study was to design a template to assist researchers to more objectively categorise the components of a CEA and so facilitate greater compatibility within and between diving incident studies. Where sufficient information is available, the template also provides the opportunity to identify and include some of the human factors which may have influenced events prior to the dive and during some segments of the chain of events. More consistent reporting will help to better inform the diving industry of various contributors to diving injuries and so enable the identification of appropriate countermeasures to help mitigate future deaths.
Methods
Access to data for this study was approved by the Justice Human Research Ethics Committee, Department of Justice, Victoria, Australia (No. CF/06/31). The program of research was also approved by the Human Research Ethics Committee at Deakin University, Victoria, Australia (No. 2013-210).
TEMPLATE CREATION
Each of the 54 Australian scuba diving fatalities from 2004 to 2010 was re-examined and a CEA applied, using the previous criteria.[ 4 , 6 – 12] A sequence category of 'pre-disposing factors' was added, the criteria for the other sequential event categories were expanded, and more specific inclusion criteria were created to better encompass the dataset. As a result, a broader yet better-defined template for the CEA was constructed.
TEMPLATE ASSESSMENT AND ADJUSTMENT
The resulting template was subsequently utilised by four investigators experienced in analysing diving deaths in the examination of 13 of the 14 scuba diving fatalities that occurred in Australia in 2011, for which the usual coronial reports were available at the time.[ 13] The process involved the following steps:
Careful scrutiny of the available data on the relevant medical and diving history of the victim and circumstances of each incident;
consideration of the possible causative factors and chain of events;
comparison with the categories and subcategories of the available template;
selection and recording of the preferred categories and subcategories.
For example, in deciding whether there were any potential predisposing factors, the investigator considered the victim's health, training, experience and skills as well as the planning and supervision of the dive, the equipment used and the nature of the activity. If there was no obvious predisposing factor, it was marked as 'unknown/none'. If a possible factor was identified which did not align with a defined category, it was allocated to 'Other' and noted for further consideration of template modification.
Two investigators were randomly assigned to perform an initial analysis of each incident without using the template (but using the previous criteria). The other two used the template. Subsequently, the roles were reversed and those who initially used the template were asked to conduct a second analysis using the original criteria, while the others used the template. Analyses were conducted two to four weeks apart. All results were collated, discussed and a consensus was reached for the final CEA to be used with this fatality series. The template was further adjusted to reflect feedback received and the final template is presented under results.
The Index of Concordance (IC)[ 14] between investigators was calculated with and without template use. The IC is defined as the number of inter-rater agreements divided by the number of coding attempts and multiplied by 100 to yield a percentage.[ 14] The IC between investigators when using the template was calculated and an IC of greater than 70% was taken as indicating agreement.[ 15] In addition, each rater's selection was compared to the consensus selections and graded either '1' if in agreement or '0' if not. In this manner, a score of 0–4 (0 = no agreement; 4 = all raters matched consensus) was given for each of the categories for each incident. These scores were summed to create a total incident score.
The Intraclass Correlation Coefficient (ICC(2)) was calculated for each category of the CEA and for the total incident score, comparing these scores with and without use of the template. In a repeated measures ANOVA involving four raters and 13 subjects, ICC(2) assumes both raters and subjects are random effects. Cut-off values of < 0.7, 0.7–0.9 and > 0.9 have been considered as poor, acceptable and good agreement.[ 16]
Result
TEMPLATE DESCRIPTION
The major sequence categories and their definitions in this CEA were as follows:
Predisposing factor: A relevant factor(s) that was present prior to the dive, and/or prior to the trigger occurring, and which was believed to have predisposed to the incident and/or to key components in the accident chain (e.g., the trigger or disabling agent);
Trigger: The earliest identifiable event that appeared to transform an unremarkable dive into an emergency;
Disabling agent: An action or circumstance (associated with the trigger) that caused injury or illness, e.g., an action of the diver or other persons, function of the equipment, effect of a medical condition or a force of nature;
Disabling injury: Injury or condition directly responsible for death or incapacitation followed by death from drowning;
Cause of death: As specified by the medical examiner, which could be the same as the disabling injury or could be drowning secondary to injury.
Note that, although the disabling injury is often more informative in determining why the diver became incapacitated, the actual cause of death can sometimes provide important information for preventative and emergency management strategies.
Suggested sub-categories for each of the categories are shown in Tables 1, 2, 3, 4, whilst Table 5 provides illustrative examples of how these taxonomies may be used. Figure 1 provides a summarised flowchart for a CEA.
Table 5. Examples of the use of the CEA template – predisposing factor, triggers and disabling agents .
| PREDISPOSING FACTORS |
| Health-related: |
| • A diver with significant cardiovascular disease may be predisposed to a cardiac event with immersion and/or exertion. |
| • A diver who is intoxicated is at an increased risk of making poor decisions. |
| Organisational/training/experience/skills-related: |
| • A dive organisation offers services to non-English-speaking (NES) clientele. A NES group booked for a dive and no arrangements were made to translate the dive briefing into the clients’ language. As a result, several divers act contrary to the brief and one subsequently dies. |
| • A person untrained or poorly trained in the use of a buoyancy compensator device may be more likely to have a buoyancy-related problem, so triggering an accident. |
| Planning-related: |
| • A diver went diving alone and without a lookout to retrieve a craypot. He became entangled in a line and was unable to free himself. |
| • When two divers arrived at their planned dive site, although there were large waves constantly breaking over the entry and exit points from the rocks, they decided to dive there anyway. When trying to enter the water, one diver was swept off the ledge, struck his head on rocks and drowned. |
| Poor communication or co-ordination: |
| • One of a buddy pair was aware of a strong current on the other side of a 'swim-through', but failed to communicate this to the other, who subsequently swam into the current and was swept away. |
| • Regulator, surface-supplied breathing apparatus or rebreather functional problem leading to gas supply reduction or interruption; |
| Absence of appropriate equipment or using obviously faulty equipment: |
| • A diver who dives without a BCD may be predisposed to a buoyancy-related problem. |
| • A diver who dives with air from a faulty or poorly maintained compressor may be predisposed to contaminated air. |
| Unsafe supervision: |
| • Poor supervision by the divemaster and/or buddy may result in an inexperienced diver entering the water without all equipment in place and functional and so predispose to an accident. |
| TRIGGERS |
| Environment-related:Faulty depth or contents gauge; |
| • A diver got into difficulties while struggling to make headway against a strong current. |
| Trigger = Environment-related (current) |
| • A spearfisherman was confronted by an aggressive shark. |
| Predisposing: Activity-related (collecting seafood). |
| Trigger = Environment-related (shark) |
| • A diver breathing air at a depth of 55 metres' sea water was suffering severe narcosis, misread his contents gauge and ran out of air. |
| Predisposing: Activity-related (deep air diving) |
| Trigger = Environment-related (narcosis at depth) |
| Equipment-related: |
| • A diver's BCD inflator became stuck open resulting in a buoyant ascent. |
| Trigger = Equipment-related (sticky BCD inflator) |
| • A diver's regulator failed, causing a loss of air supply. |
| Trigger = Equipment–related (regulator failure) |
| Gas supply-related: |
| • A technical diver using a rebreather became unconscious at depth due to hypercapnia resulting from overloading of the CO₂ scrubber. |
| Predisposing = Faulty equipment (CO₂ scrubber inadequate) |
| Trigger = Gas supply-related (CO₂ scrubber exhausted) |
| • A diver ran out of breathing gas while trying to complete required decompression and was forced to make a rapid ascent. |
| Predisposing = Poor planning (unless something unpredictable occurred) |
| Trigger = Gas supply-related (out of gas) |
| Buoyancy-related: |
| • After deploying his surface marker buoy (SMB), a diver became entangled in its line and was dragged to the surface. |
| Trigger = Buoyancy-related (SMB entanglement) |
| • An inexperienced drysuit user became inverted, was unable to dump air from the suit and had an uncontrolled ascent. |
| Predisposing = Experience-related (inexperienced) |
| Trigger = Buoyancy-related (drysuit blow-up) |
| Exertion-related: |
| • A (healthy) diver collecting abalone became exhausted and distressed while dragging his heavy catch bag and then struggled to stay afloat on reaching the surface. |
| Trigger = Exertion-related (heavy catch bag) |
| Anxiety/stress-related: |
| • A student on an introductory dive was seen to panic and rush to the surface after encountering a large stingray. |
| Predisposing = Experience-related (inexperience) |
| Trigger = Anxiety/stress-related (panic from stingray encounter) |
| Primary diver error: |
| • A rebreather diver on the surface forgot to turn off her bailout valve before removing her mouthpiece. Water entered the scrubber and when she replaced the mouthpiece and breathed from the unit she suffered a 'caustic cocktail'. |
| Trigger = Diver error (equipment-related) |
| • A diver forgot to open his tank valve before jumping in. Being negatively buoyant, he sank without an available air supply. |
| Trigger = Diver error (gas supply-related) |
| DISABLING AGENTS |
| Gas supply-related: |
| • A diver became entangled in a line inside a wreck, was unable to free herself and ran out of air. |
| Predisposing = Activity-related (wreck penetration) |
| Trigger = Environmental (entanglement) |
| Disabling agent: Gas supply-related (out of gas) |
| Ascent-related: |
| • A preoccupied underwater photographer failed to check his air, ran out of air, held his breath during ascent and suffered a pulmonary barotrauma. |
| Trigger = Gas-supply-related (out of air) |
| Disabling agent: Ascent-related (breath-holding) |
| Medical-related: |
| • Faulty oxygen sensors in a rebreather enabled the PO₂ to rise sufficiently to cause a hyperoxic convulsion in the diver. |
| Predisposing = Equipment fault (old/poorly-calibrated oxygen sensors) |
| Trigger = Gas supply-related (incorrect breathing gas mix from sensor failure) |
| Disabling agent: Medical-related (hyperoxic convulsion) |
| • A diver with a history of epilepsy is seen to become unconscious and have a seizure during a shallow air dive. |
| Predisposing = Health-related (epilepsy) |
| Trigger = Environmental (sensory effects) |
| Disabling agent: Medically-related (seizure) |
| Buoyancy-related: |
| • A diver surfaced in rough conditions after losing a fin due to a broken fin strap. He was negatively buoyant, failed to replace his regulator, inflate his BCD or ditch weights and was swamped by a wave and sank. |
| Trigger = Equipment-related (torn fin strap) |
| Disabling agent: Buoyancy-related (lack of buoyancy on surface) |
| • A drysuit inflator stuck open causing over-inflation and inversion in the water. During the process, the diver aspirated some water and became unconscious. |
| Trigger = Equipment-related (drysuit inflator malfunction) |
| Disabling agent: Buoyancy-related (inversion underwater) |
| Environment-related: |
| • A diver lost control of her buoyancy, ascended into and became entangled in the shotline and subsequently ran out of air. |
| Trigger = Buoyancy-related (poor buoyancy control) |
| Disabling agent: Environment - entrapment (out of air) |
| • A diver in rough water was thrown against rocks by a large wave, hit his head and became unconscious. |
| Trigger = Environmental (rough conditions) |
| Disabling agent: Environmental (head impact with rocks) |
| • An abalone diver was approached and subsequently attacked by a shark. |
| Predisposing = Activity-related (collecting seafood) |
| Trigger = Environmental (aggressive shark) |
| Disabling agent: Environmental – shark attack |
| Equipment-related: |
| • A rebreather diver on the surface momentarily forgot to turn off her bailout valve before removing her mouthpiece, enabling water ingress. The water entered the scrubber and when she replaced the mouthpiece and breathed from the unit she suffered a 'caustic cocktail'. |
| Trigger = Diver error (equipment-related) |
| Disabling agent: Equipment-related ('caustic cocktail') |
TEMPLATE ASSESSMENT
The index of concordance between the raters when using the template was 82% (257/312) compared with 62% (194/312) when not using it. This absolute IC difference of 20% is substantial and clinically significant. Table 6 shows the comparison of the raters’ agreement with and without template use for each scuba-related category and total score.
Table 6. Comparison of investigator scores of scuba deaths with (T) and without template (NT) use; note that the score is not intended to be used when investigating a diving accident; it was just a simple method to try to quantify any gross difference in score allocation by the raters with and without template use; it does not represent how the data is used .
| Case | Predisposing factor | Trigger | Disabling agent | Disabling injury | Total (∗/16) | |||||
| NT | T | NT | T | NT | T | NT | T | NT | T | |
| 1 | 4 | 4 | 3 | 4 | 4 | 4 | 3 | 4 | 14 | 16 |
| 2 | 3 | 3 | 1 | 3 | 4 | 4 | 4 | 3 | 12 | 13 |
| 3 | 3 | 4 | 3 | 3 | 3 | 4 | 4 | 4 | 13 | 15 |
| 4 | 3 | 4 | 3 | 4 | 1 | 1 | 3 | 4 | 10 | 13 |
| 5 | 4 | 4 | 2 | 4 | 3 | 4 | 3 | 4 | 12 | 16 |
| 6 | 2 | 4 | 2 | 3 | 2 | 3 | 3 | 4 | 9 | 14 |
| 7 | 3 | 4 | 2 | 4 | 2 | 3 | 2 | 3 | 9 | 14 |
| 8 | 3 | 4 | 3 | 4 | 4 | 4 | 4 | 4 | 14 | 16 |
| 9 | 3 | 4 | 2 | 3 | 3 | 4 | 4 | 4 | 12 | 15 |
| 10 | 4 | 4 | 3 | 4 | 4 | 4 | 4 | 4 | 12 | 16 |
| 11 | 1 | 3 | 2 | 2 | 2 | 4 | 4 | 4 | 9 | 13 |
| 12 | 3 | 3 | 3 | 3 | 3 | 3 | 4 | 4 | 13 | 13 |
| 13 | 2 | 2 | 2 | 4 | 3 | 4 | 3 | 4 | 10 | 14 |
Table 7 shows the mean and standard deviation (SD) scores with each category of the CEA both with (T) and without (NT) template use, as well as the ICC(2) for each category and for the total scores. As it is illustrated, all post-template mean scores are higher with smaller SDs, indicating a higher agreement and less between-raters heterogeneity. Three out of four categories had poor agreement consistency, with an ICC(2) less than 0.70 illustrating poor agreement between before and after template use. This illustrates a systematic improvement in between-rater scores after template implementation.
Table 7. Mean (SD) scores for category and total with (T) and without (NT) template use; ICC(2) – intraclass correlation coefficient; CI – confidence intervals .
| Category | NT | T | ICC (2) | (95% CI) | ||
| Predisposing factor | 2.9 | (0.9) | 4.0 | (1.0) | 0.68 | (0 - 0.90) |
| Trigger | 2.4 | (0.7) | 3.54 | (0.66) | 0.49 | (0 - 0.85) |
| Disabling agent | 2.9 | (1) | 3.54 | (0.88) | 0.86 | (0.53 - 0.96) |
| Disabling injury | 3.46 | (0.66) | 3.85 | (0.38) | 0.42 | (0 - 0.82) |
| Total(out of 16) | 11.7 | (2.1) | 14.5 | (1.27) | 0.73 | (0.13 − 0.92) |
Discussion
In this study, the use of the template improved consensus in the evaluation of the diving fatalities as indicated by the large increase in IC when using the template. This was supported by the relatively low ICC(2) ratings which indicate a marked difference in scoring (consistency of agreement) with and without template use. An ICC of 0.70–0.90 may be acceptable for use in research purposes but not for policymaking.[ 17]
An advantage of using ICC(2) to compare measurement methods is that it can be used when the measurements are given on different scales or metrics, as the ICC(2) is a dimensionless ratio. Because reliability depends on the heterogeneity of the true error-free values in the sampled population, it is essential that reliability ICC(2)s are compared only if they have been estimated from the same population.[ 18] Usually, assessments made by two different raters are less similar than are two assessments made by the same rater. Assessments from two raters may differ systematically due to bias between the raters (a rater 'effect'), and their measurement errors may also have different SDs. For example, assessments from a rater who can make more precise assessments will have a smaller SD than those made by a less precise rater. Since assessments in the future are to be made by different raters, we need to describe and quantify the differences between such assessments in order to judge whether differences are genuine or may be due to measurement error. As such, the ideal way to study this was for each rater to make at least two assessments of a sample of subjects. The design of such a study and the type of appropriate statistical analyses was guided by the fact that our interest lay in drawing inferences about a wider population of potential raters, not only the particular set of raters. Due to the fact that the raters in the study are considered a random sample from the population of potential raters, we analysed the study using a model that treats the rater 'effect' as a random effect. Thus, we used a two-way random-effects model, with random subject effects and random observer effects.
Although factors such as experience and medical history, where known, are included, the traditional sequential analysis for diving-related injury largely failed to address other human factors often associated with such incidents.
In a study of 1,000 (mainly non-fatal) diving incidents, The Diver Incident Monitoring Survey (DIMS) reported that 87% of the incidents were associated with diver error.[ 19] Given the inhospitable environment in which diving takes place, in addition to adequate health and fitness, the foundation for safe diving includes 'human factors' such as adequate knowledge and skill acquisition and retention and clear, often rapid decision-making. A CEA may provide a useful tool to identify 'how' an incident occurred, i.e., the sequence of events in the dive incident itself. However, preceding and/or underlying many of the components in such an analysis is the potential for diver error or inappropriate behaviour from human factors.
Using techniques from research into aviation accidents, a Human Factors Analysis and Classification System (HFACS) was applied to recreational scuba diving incidents in an attempt to determine 'why' they occurred.[ 20 , 21] The HFACS comprised two major divisions: 'active failures' (unsafe acts) which involved "diver error", and 'latent failures', which included factors that occurred prior to the incident and which influenced the active failure. A "Swiss cheese model"[ 22] was used to argue that a dive incident does not simply result from diver error alone but is ultimately the result of the alignment of several 'holes' in each of the layers of latent and active failures (Figure 1).
Figure 1.
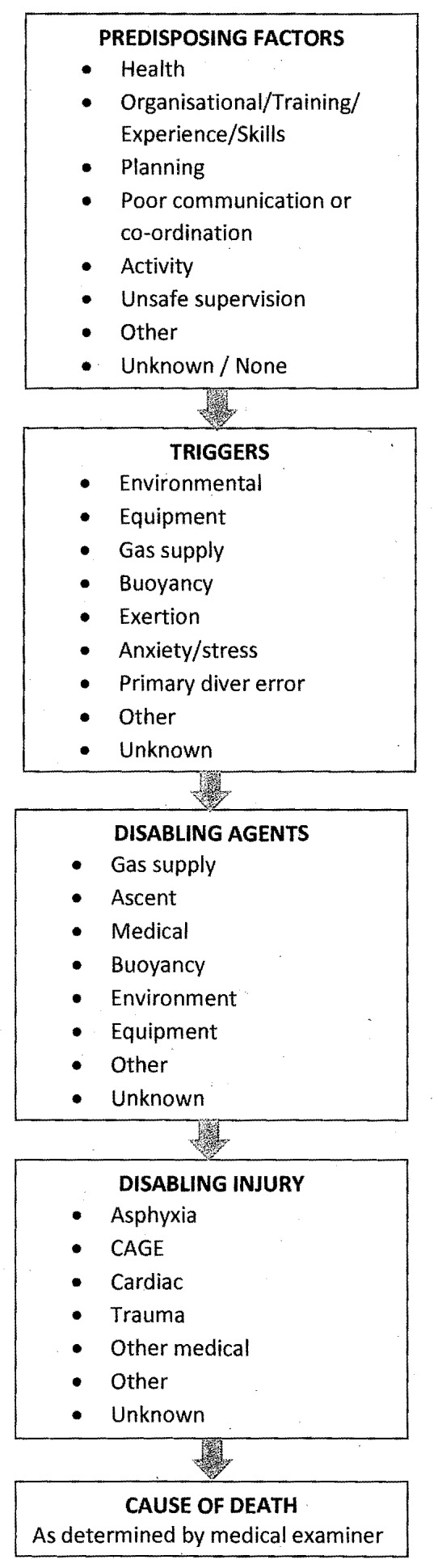
Flowchart of chain of events analysis of a scuba diving accident
This protocol is more readily applicable to non-fatal incidents where greater detail is often available and where the diver can provide feedback and personal insight into the various human factors involved. However, sometimes witness reports and other background information can indicate where, and which human factors contributed to the cascade of events leading to the death of a diver. So the addition of known or reasonably suspected human factor considerations to a CEA of diving fatalities is valuable in order to obtain a fuller picture of the entire scenario. Such human factors include pre-existing health conditions, inadequate training and skills, inappropriate/poorly-functional equipment; or more deeply-rooted organisational problems that may underpin some of these. An example of an underlying organisational problem is an inadequate training focus and practice in weight-ditching. Given the large number of diving fatality victims whose bodies are found with their weights still in situ,[ 5 , 23] this is an important area to address from training agency level down.
Another important organisational-level consideration is improved education about how certain co-existing conditions can impact on diving safety. Pre-certification diving medical examinations are now uncommon in many countries, with an increasing reliance on a diver to honestly and accurately answer a self-reporting medical questionnaire. This places a greater onus on dive professionals and existing or intending divers to understand the questions and the associated implications, and to take these seriously and act accordingly. This has become increasingly evident with the increasing representation of divers with pre-existing medical conditions (especially cardiac-related) and older divers in dive fatality reports.[ 4 , 13 , 24]
In reality, multiple factors, discrete or linked, may simultaneously influence an action or circumstance within an incident. It is important for the investigator to logically and systematically consider all possibilities and influences when trying to determine a possible sequence of events. This can be a daunting task, prone to substantial subjectivity and variation between investigators.
When developing this template, one of the main aims was to reduce the variability in categorisation in existing protocols in order to make determinations more uniform between assessors and so increase comparability both within and between studies. This was done by increasing specificity within the categories. In addition, where possible, the categories were designed to be mutually exclusive and as encompassing as practicable to minimise the need to record a component as 'other' and so improve the consistency.[ 25]
A certain degree of subjectivity is inescapable given the frequent gaps in the information available to diving incident investigators. However, by creating taxonomies that achieve reasonable consensus between users, subjectivity is reduced. To this end, it remains important to test the consistency between users when allocating events using such taxonomies. There are a variety of suggested methods for determining this but the IC is reportedly the industry standard for use with safety data.[ 26]
The study did highlight several minor categorisation problems, which were adjusted in the template presented here. Undoubtedly, more improvements will be identified with further use and the template will need to be modified accordingly. Users are encouraged to send feedback to the corresponding author.
LIMITATIONS
There was likely a net learning effect to both the raters who used the template first and those who did not. Despite the delay between allocations, those who did not use it initially may have been more familiar with the case by the time they re-examined it. Similarly, those who used it first may have recollected some of the categorisation within the template. The template allocations were mixed in an attempt to balance these issues and likely served to narrow the difference between allocations with and without the template. Given the limited information that is often available, and the continued challenges associated with the subjectivity and categorisation of aspects of diving deaths, there will inevitably be variation between reporters.
Conclusions
A CEA can be useful in diving fatality investigations to identify the likely sequences of events that lead to the divers' demise. However, there is often limited information on which to base such an analysis and this can lead to substantial variation in the interpretation of events by different investigators. An effective template for allocating the components of a chain of events may be useful in reducing the variability between investigators within a study and increase the comparability of different diving fatality studies. Although still imperfect and likely to be modified with future use, this CEA template has been shown to improve consistency of interpretation between users.
Footnotes
Acknowledgements
The authors are grateful to Chris Lawrence, Andrew Fock and Scott Jamieson for their help in the scoring exercises, and to Petar Denoble for his comments on the draft.
Contributor Information
J Lippmann, Divers Alert Network (DAN) Asia-Pacific, Ashburton, Victoria, Australia; School of Health and Social Development, Deakin University, Geelong, Victoria, Australia.
C Stevenson, School of Health and Social Development, Deakin University, Geelong, Victoria, Australia.
D McD Taylor, Emergency Department, Austin Hospital, Victoria, Australia; Department of Medicine, University of Melbourne, Australia.
J Williams, School of Health and Social Development, Deakin University, Geelong, Victoria, Australia.
M Mohebbi, Biostatistics Unit, Deakin University, Geelong, Victoria, Australia.
References
- Heinrich HW. New York: McGraw Hill; 1936. Industrial Accident Prevention ; p. 37. [Google Scholar]
- Wallace B, Ross A. Boca Raton, FL: Taylor and Francis; 2006. Beyond human error – taxonomies and safety science ; p. 25. [Google Scholar]
- Denoble PJ, Caruso JL, de L Dear G, Vann RD. Common causes of open-circuit recreational diving fatalities . Undersea Hyperb Med. 2008;35:393–406. [PubMed] [Google Scholar]
- Lippmann J, Baddeley A, Vann R, Vann RD, Walker D. An analysis of the causes of compressed gas diving fatalities in Australia from 1972-2005 . Undersea Hyperb Med. 2013;40:49–61. [PubMed] [Google Scholar]
- Vinkel J, Bak P, Hyldegaard O. Danish diving fatalities 1999-2012 . Diving Hyperb Med. 2016;46:142–149. [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Fock A, Jamieson S. Provisional report on diving-related fatalities in Australian waters 2010 . Diving Hyperb Med. 2015;44:154–175. [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Wodak T, Fock A, Jamieson S. Provisional report on diving-related fatalities in Australian waters 2009 . Diving Hyperb Med. 2013;43:194–217. [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Wodak T, Fock A, Jamieson S, Walker D, Harris R. Provisional report on diving-related fatalities in Australian waters 2008 . Diving Hyperb Med. 2013;43:16–34. [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Wodak T, Fock A, Jamieson S. Provisional report on diving-related fatalities in Australian waters 2007 . Diving Hyperb Med. 2012;42:151–170. [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Wodak T, Fock A, Jamieson S. Provisional report on diving-related fatalities in Australian waters 2006 . Diving Hyperb Med. 2011;41:70–84. [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Wodak T, Fock A, Jamieson S. Provisional report on diving-related fatalities in Australian waters 2005 . Diving Hyperb Med. 2010;40:131–139. [PubMed] [Google Scholar]
- Walker D, Lippmann J, Lawrence C, Houston J, Fock A. Provisional report on diving-related fatalities in Australian waters 2004 . Diving Hyperb Med. 2009;39:138–161. [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Fock A, Jamieson S. Provisional report on diving-related fatalities in Australian waters 2011 . Diving Hyperb Med. 2016;46:207–240. [PubMed] [Google Scholar]
- Ross AJ, Wallace B, Davies JB. Technical note: measurement issues in taxonomic reliability . Saf Sci. 2004;42:771–778. [Google Scholar]
- Wallace B, Ross A. Boca Raton, FL: Taylor and Francis; 2006. Beyond human error – taxonomies and safety science ; p. 86. [Google Scholar]
- Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability . Psychological Bulletin. 1979;86:420–428. doi: 10.1037//0033-2909.86.2.420. [DOI] [PubMed] [Google Scholar]
- Martins WP, Nastri CO. Interpreting reproducibility results for ultrasound measurements . Ultrasound Obstet Gynecol. 2014;43:479–480. doi: 10.1002/uog.13320. [DOI] [PubMed] [Google Scholar]
- Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement . Lancet. 1986;1:307–310. [PubMed] [Google Scholar]
- Acott CJ. Human error and violations in 1,000 diving incidents: a review of data from the Diving Incident Monitoring study (DIMS) . SPUMS Journal. 2005;345:11–17. [Google Scholar]
- Lock G. Human factors within recreational scuba diving - an application of the human factors analysis and classification system (HFACS). 21 March 2011 . [cited 2016 August 10]. Available at: https://cognitasresearch.files.wordpress.com/2012/08/human-factors-in-sport-diving-incidents.pdf.
- Lock G. 2014 DISMS Annual Report. Cognitas Incident and Management Ltd. 01 Feb 2015 . [cited 2016 Sept 27]. Available at: https://cognitasresearch.files.wordpress.com/2015/02/2014dismsannualreport_final.pdf.
- Reason J. Human error: models and management . BMJ (Clinical Research Ed) 2000;320:768–770. doi: 10.1136/bmj.320.7237.768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lippmann J. Diving deaths downunder . In: Vann RD, Lang MA, editors. Durham, NC: Divers Alert Network; 2011. pp. 86–97. Recreational diving fatalities. Proceedings of the Divers Alert Network 2010 April Workshop . [Google Scholar]
- Denoble PJ, Pollock NW, Vaithiyanathan P, Caruso JL, Dovenbarger JA, Vann RD. Scuba injury death rate among insured DAN members . Diving Hyperb Med. 2008;38:182–188. [PubMed] [Google Scholar]
- Wallace B, Ross A. Boca Raton, FL: Taylor and Francis; 2006. Beyond human error - taxonomies and safety science ; p. 48. [Google Scholar]
- Wallace B, Ross A. Boca Raton, FL: Taylor and Francis; 2006. Beyond human error - taxonomies and safety science ; p. 93. [Google Scholar]