

Abstract
National registration of hemiarthroplasties after hip fractures has been established in both Norway and Sweden. We aimed to investigate differences in demographics, choice of implant selection, surgical approaches, and reoperations between the Norwegian Hip Fracture Register (NHFR) and the Swedish Hip Arthroplasty Register (SHAR). As part of the Nordic Arthroplasty Register Association (NARA) project a common hemiarthroplasty dataset has been established. 36,989 primary hemiarthroplasties (HAs) for acute hip fractures reported to NHFR (n = 12,761) and SHAR (n = 24,228) for the period 2005-2010 were included. Cemented prostheses were used in 78% of the operations in Norway and in 95% of the patients in Sweden. In Norway HAs almost exclusively had bipolar design (98%), whereas in Sweden HAs with unipolar design were used in 42% of the cases. Monoblock (non-modular) prostheses were uncommon, but still more frequently used in Sweden than in Norway (6.9% and 2.1% respectively). The lateral approach was more common in Norway (83%) than in Sweden (52%), where the posterior approach was used in 42% of the cases. The five-year survival of all HAs was 95.5% (95% CI: 94.8-96.2) in Norway and 94.8% (95% CI: 94.4-95.3) in Sweden. We concluded that surprisingly large differences between the two countries in demographics, implant design, and surgical technique had been revealed. This common dataset enables further investigations of the impact of these differences on revision rates and mortality.
Keywords: Hip fractures, Hemiarthroplasty, Registries, Reoperation
Introduction
To evaluate and improve the treatment of hip fractures, and to provide epidemiological data, the Norwegian Hip Fracture Register (NHFR) was established in 2005 (1). In Sweden, registration of hemiarthroplasties (HAs) was initiated in 2005 as a part of the Swedish Hip Arthroplasty Register (SHAR) (2). During the last decade an increasing number of patients with hip fractures has been treated with hemiarthroplasties in both Norway and Sweden (3, 4). Accordingly, one main issue in hip fracture research is to facilitate selection of the arthroplasties that can be expected to provide optimum results and minimum frequency of complications. A collaboration between the Nordic arthroplasty registers has been initiated (the Nordic Arthroplasty Register Association – NARA) which has resulted in common datasets for total hip and knee replacements (5). One of the purposes with these datasets is to obtain more reliable outcome data not limited by national demographics and treatment traditions. Within the NARA organisation, the two countries (Norway and Sweden) with national registers of HAs in the treatment of hip fractures have now established a common dataset for these procedures as well. This is the first report on this dataset. The aim was to compare demographics, choice of implant, surgical technique, and reoperations after hemiarthroplasties in Norway and Sweden.
MATERIALS AND METHODS
In this common dataset, based on data from the NHFR and the SHAR, hemiarthroplasties for acute hip fractures were included. The completeness of HAs in the NHFR and SHAR has been found to be 99% and 96% respectively (2, 6). Both primary operations and reoperations are registered. By using the unique identification numbers given to all inhabitants in both Norway and Sweden, all reoperations were linked to their index operation. Further, mortality data were obtained from the national death registries and linked to the patients with these identification numbers. The two registries had different registration forms, and accordingly there were different variables in the respective databases. A common set of variables were defined and re-coded in order to get similar definitions of the variables resulting in two homogeneous databases before merging. In the SHAR, the registration of ASA-class (American Society of Anaesthesiologists, 1963) (7) did not start until 2008. Even so, data on ASA-class was included in the common variable set. Cognitive impairment was classified as “none”, “uncertain”, or “present”. The fractures were classified as intracapsular fractures, trochanteric fractures, and subtrochanteric fractures. Combination of two or more fractures, and fractures that could not be classified into one of the three other fracture groups were classified as “other”. The surgical approaches were coded into four different types: anterior (i.e. between m. sartorius and m. tensor fasciae latae), anterolateral (i.e. between m. tensor fasciae latae and m. gluteus medius), lateral (i.e. transgluteal), and posterolateral (i.e. posterior to m. gluteus medius). The two national datasets were prepared by each individual register. Finally de-identification of the patients was done before the two data-sets were merged into a common dataset. Institutional Review Board (IRB)/Ethics Committee approval was obtained.
Statistical analysis
We calculated descriptive statistics for the two countries. The Student's t-test was used for continuous variables and the Chi Square test was used for categorical variables. The significance level was set to 0.05. Patients were followed until time of reoperation, death, or December 31, 2010. A reoperation was defined as any further open surgery, including open reduction of dislocated HAs and soft tissue reoperations without removal or exchange of prosthesis components. Survival based on reoperation as endpoint at one and five years postoperatively was calculated using the Kaplan Meier method. Cox multiple regression models, with adjustments for age and gender, were used to calculate differences in relative risk (RR) for reoperation between the two countries. The proportional hazards assumption was not fulfilled when investigated visually by use of log-minus-log plots. As the Kaplan-Meier country curves crossed each other for prostheses survival of all HAs and all uncemented HAs, we performed additional Cox regression analyses with the follow-up divided into two periods. The first period ran from the day of surgery until 1.5 years postoperatively and the second period commenced at 1.5 years postoperatively and ran until December 31, 2010. The proportional hazard assumption was fulfilled within the two time-periods. Through the effect of competing risk (here death) there was a chance of potential overestimation of incidence of reoperations, and hence the relative risk estimates. With the methods described by Fine and Grey (8) and Gillam (9) we performed three separate competing risk analyses and calculated RR estimates for each category: cemented, uncemented and follow-up less than 1.5 years, and uncemented and follow-up 1.5 years or more (8, 9). These estimates were found to be close to the ones from the adjusted Cox analysis.
Respectively 37.9% and 44.0% of the patients died during the follow-up period in Norway and Sweden. With our short follow-up (median follow-up was 1.5 years) we found that the use of the Kaplan-Meier method to estimate prosthesis survival was sufficient. All statistical analyses were performed by use of the statistical package PASW Statistics version 18 (SPSS Inc., Chicago, IL) and with the statistical package R (Gray RJ (2010) Cmprsk: Subdistribution Analysis of Competing Risks. http://CRAN.R-project.org/Package = cmprsk).
Results
Totally 36,989 primary hemiarthroplasties (Norway: n = 12,761, Sweden: n = 24,228) were included. Mean follow-up was 1.67 (0–6) years in Norway and 1.82 (0–6) years in Sweden.
Demographics
The characteristics of the patients are presented in Table I. In Sweden the patients were older (84.0 vs. 82.6 years), but less cognitively impaired compared to patients in Norway. Further, females constituted 72% of the patients in Sweden and 74% in Norway. More patients in Sweden compared to Norway had been classified as ASA class 1 or 2 (42.8% and 39.5% respectively). There were only minor differences in fracture type distribution between the countries. In Norway, uncemented HAs constituted 22% of all HAs. In Sweden the proportion of uncemented procedures was only 5.5%. HAs used in Norway had almost exclusively a bipolar design. In Sweden, nearly 50% of the HAs had a unipolar or monoblock design. The lateral approach was the most frequently used in both Norway and Sweden. However, the posterior approach was more frequently used in Sweden. There were substantial differences in choice of prosthesis brands. The most commonly used combinations of stems and heads are listed in Table II. The ETS prosthesis (Stryker) was the only monoblock prostheses used in Norway (n = 231). Monoblock HAs were in Sweden used in 1,681 patients. Austin Moore and Thompson monoblock prostheses from different manufacturers were used in 610 and 746 patients. The ETS prosthesis was used in 325 patients.
Table I.
CHARACTERISTICS OF THE HEMIARTHROPLASTY PATIENTS AND OPERATIONS REGISTERED IN THE NARA DATASET 2005-2010
| Norway | Sweden | p-value | |
|---|---|---|---|
| Total number | 12,761 | 24,228 | |
| Mean age (SD) at fracture (years) | 82.6 (7.5) | 84.1 (6.7) | <0.001* |
| Women (%) | 9,473 (74) | 17,359 (72) | <0.001† |
| ASA class (%)‡ | <0.001† | ||
| ASA 1 | 566 (4.5) | 308 (2.8) | |
| ASA 2 | 4,440 (35) | 4,427 (40) | |
| ASA 3 | 6,834 (54) | 5,675 (51) | |
| ASA 4 | 714 (5.7) | 602 (5.5) | |
| ASA 5 | 6 (0.0) | 12(0.1) | |
| Missing data§ | 201 | 13,204 | |
| Cognitive impairment (%) | <0.001† | ||
| Yes | 3,212 (26) | 4,345 (21) | |
| Uncertain | 1,397 (11) | 2,058 (10) | |
| No | 7,813 (63) | 14,032 (69) | |
| Missing data§ | 339 | 3,793 | |
| Fracture type (%) | <0.001† | ||
| Intracapsular | 12,524 (98) | 23,895 (99) | |
| Trochanteric | 35 (0.3) | 247 (1.0) | |
| Subtrochanteric | 4 (0.0) | 72 (0.3) | |
| Other | 161 (1.3) | 14 (0.1) | |
| Missing data§ | 37 | 0 | |
| Fixation (%) | <0.001† | ||
| Cemented | 9,688 (78) | 22,896 (95) | |
| Uncemented | 2,711 (22) | 1,330 (5.5) | |
| Missing data | 362 | 2 | |
| Design (%) | <0.001† | ||
| Bipolar | 12,477 (98) | 12,300 (51) | |
| Unipolar | 11 (0.1) | 10,241 (42) | |
| Monoblock | 273 (2.1) | 1,681 (6.9) | |
| Missing data§ | 0 | 6(0.0) | |
| Approach (%) | <0.001† | ||
| Anterior | 30 (0.2) | 13 (0.05) | |
| Anterolateral | 969 (7.7) | 15 (0.06) | |
| Lateral | 10,507 (83) | 12,594 (52) | |
| Posterolateral | 1,105 (8.8) | 11,564 (48) | |
| Other | 0 | 1(0.0) | |
| Missing data§ | 150 | 42 | |
Student's t-test.
Chi square test.
ASA class registration in Sweden from 2008.
Missing data not included in percent calculations in this table.
Table II.
THE 10 MOST COMMONLY USED COMBINATIONS OF STEMS AND HEADS IN EACH COUNTRY
| Stem | Head | Fixation | Design | Number (%) |
|---|---|---|---|---|
| Norway | ||||
| Exeter (Stryker) | UHR Universal Head (Stryker) | Cemented | Bipolar | 3,257 (26) |
| Charnley (DePuy) | Hastings (DePuy) | Cemented | Bipolar | 2,285 (18) |
| Corail (DePuy) | Bi-Polar Head (DePuy) | Uncemented | Bipolar | 1,158 (9.1) |
| Corail (DePuy) | Cupule Mobile (DePuy) | Uncemented | Bipolar | 922 (7.2) |
| Lubinus SPII (LINK) | Vario-Cup (LINK) | Cemented | Bipolar | 897 (7.0) |
| Spectron EF (S&N) | Tandem Bipolar(S&N) | Cemented | Bipolar | 825 (6.5) |
| Charnley Modular(DePuy) | Hastings (DePuy) | Cemented | Bipolar | 810 (6.4) |
| Titan (DePuy) | Cupule Mobile (DePuy) | Cemented | Bipolar | 697 (5.5) |
| Filler (Biotechni) | Biarticular cup (Permedica) | Uncemented | Bipolar | 252 (2.0) |
| Titan (Depuy) | Bi-Polar Head (DePuy) | Cemented | Bipolar | 228 (1.8) |
| Sweden | ||||
| Lubinus SPII (LINK) | Vario-Cup (LINK) | Cemented | Bipolar | 5,573 (23) |
| Lubinus SP II (LINK) | Large Prosthesis Head (LINK) | Cemented | Unipolar | 4,758 (20) |
| Exeter (Stryker) | UHR Universal Head (Stryker) | Cemented | Bipolar | 3,570 (15) |
| Exeter (Stryker) | V40 Unipolar (Stryker) | Cemented | Unipolar | 2,715 (11) |
| Spectron EF (S&N) | Tandem Unipolar (S&N) | Cemented | Unipolar | 1,148 (4.7) |
| CPT (Zimmer) | Ultima Monk (Zimmer) | Cemented | Bipolar | 1,068 (4.4) |
| Corail collarless (DePuy) | Ultima Monk (Zimmer) | Uncemented | Bipolar | 456 (1.9) |
| CPT (Zimmer) | VerSys Endo (Zimmer) | Cemented | Unipolar | 430 (1.8) |
| Thompson | Ultima Monk (Zimmer) | Cemented | Bipolar | 376 (1.6) |
| MS 30 (Zimmer) | Unipolar Head (Zimmer) | Cemented | Unipolar | 352 (1.4) |
Time trends
The bipolar design of the HAs was the dominating design in Norway during the whole study period (2005-2010). In Sweden, there was a gradual shift towards prostheses with unipolar design during the last years of the study period (Fig. 1). The disappearance of Austin Moore prostheses in Sweden led to a decrease in the total number of uncemented implants, but even modern modular uncemented stems showed a slight decrease. These prostheses were more frequently used in Norway throughout the study period and in particular in 2010 (Fig. 2). The lateral approach was the dominating approach in Norway during the whole study period. In Sweden, the lateral approach increased at the expense of the posterolateral, but at the end of the study period the latter was still used in almost 40% of the procedures (Fig. 3).
Fig. 1.
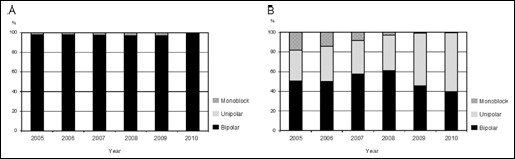
Time trends of implant design used in: A) Norway; and B) Sweden.
Fig. 2.
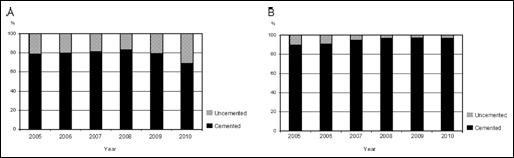
Time trends of fixation technique for hemiprostheses in: A) Norway; and B) Sweden.
Fig. 3.
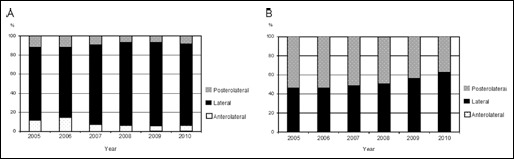
Time trends of surgical approach used for hemiprostheses in: A) Norway; and B) Sweden.
Reoperations
Four hundred and forty-five (3.5%) of the HAs in Norway and 869 (3.6%) of the HAs in Sweden had been reoperated. There were more reoperations due to infection in Norway than in Sweden (1.8% vs. 1.0% respectively, p<0.001). On the other hand, there were more reoperations due to dislocation (1.6% vs. 0.9% respectively, p<0.001) and periprosthetic fractures (0.6% vs. 0.3% respectively, p<0.001) in Sweden compared to Norway. Reoperation because of acetabular erosion was only recorded in the SHAR (n = 56). The one-year and five-year survival of the HAs, cemented HAs and uncemented HAs are presented in Table III, whereas the Kaplan-Meier survival curves for all HAs, cemented HAs, and uncemented HAs are presented in Figure 4. As the country curves crossed for all HAs and uncemented HAs after about one and a half year, we only performed overall Cox regression analyses for cemented HAs. We found a higher risk of reoperations for cemented HAs in Sweden compared to Norway (RR, 1.26, 95% CI: 1.10-1.45). For uncemented HAs, the follow-up was divided into two periods before Cox regression analyses were performed. No statistically significant differences in risk of reoperation was found between the countries for uncemented HAs neither when analysing the first 1.5 years of follow-up nor the period thereafter (Tab. IV).
Table III.
KAPLAN MEIER ESTIMATES OF SURVIVAL OF IMPLANT AT 1 AND 5 YEARS FOLLOW-UP
| No of |
Survival (%) KM |
Survival (%) KM |
|||
|---|---|---|---|---|---|
| Country | HAs | Reop | At 1 years (95% CI) | At 5 years (95% CI) | |
| All HAs | Norway | 12,761 | 445 | 96.3 (96.0-96.7) | 95.5 (94.8-96.2) |
| Sweden | 24,228 | 869 | 96.5 (96.2-96.7) | 94.8 (94.4-95.3) | |
| Cemented HAs | Norway | 9,688 | 273 | 97.0 (96.7-97.4) | 96.7 (96.3-97.1) |
| Sweden | 22,896 | 794 | 96.6 (96.3-96.8) | 94.9 (94.5-95.4) | |
| Uncemented HAs | Norway | 2,711 | 149 | 94.2 (93.2-95.1) | 91.0 (87.7-94.2) |
| Sweden | 1,330 | 75 | 94.7 (93.4-96.0) | 92.6 (90.9-94.3) | |
CI = Confidence Interval, HA = Hemiarthroplasty, KM = Kaplan Meier.
Fig. 4.
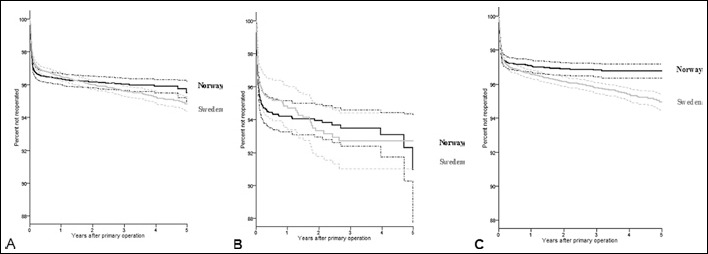
Kaplan - Meier estimated curves with 95% confidence intervals until reoperation of any cause for: A) all primary hemiarthroplasties; B) uncemented hemiarthroplasties; and C) cemented hemiarthroplasties in Norway and Sweden.
Table IV.
COX REGRESSION AND COMPETING RISK ESTIMATES OF SURVIVAL AND RELATIVE RISK OF ANY REOPERATION
| RR | 95% CI | p-value* | |
|---|---|---|---|
| Cemented HAs | |||
| Norway | 1 | ||
| Sweden (Cox) | 1.26 | 1.10-1.45 | <0.001 |
| Sweden (Fine&Gray) | 1.27 | 1.10-1.46 | <0.001 |
| Uncemented HAs. Follow-up < 1.5 years | |||
| Norway | 1 | ||
| Sweden (Cox) | 0.96 | 0.71-1,29 | 0.8 |
| Sweden (Fine&Gray) | 0.94 | 0.70-1.27 | 0.7 |
| Uncemented HAs. Follow-up < 1.5 years | |||
| Norway | 1 | ||
| Sweden (Cox) | 1.54 | 0.55-4.31 | 0.4 |
| Sweden (Fine&Gray) | 1.48 | 0.49-4.42 | 0.5 |
CI = Confidence Interval, HA = Hemiarthroplasty
adjusted for differences in age and gender.
Discussion
This first study of the new common dataset with hemiarthroplasties (HAs) from the NHFR and the SHAR has revealed several major differences between the two countries. Uncemented HAs were used more frequently in Norway than in Sweden. More monoblock prostheses and unipolar HAs were used in Sweden compared to Norway. The lateral approach was used in a vast majority in Norway, but only in slightly more than half of the Swedish procedures.
Demographics
The fact that other treatment modalities for hip fractures (i.e. total hip arthroplasty and internal fixation) were not included in our dataset could explain some of the differences in demographics found between the two countries. Different treatment traditions for hip fractures, with more total hip arthroplasties for the youngest patients in Sweden, may be one reason for the higher mean age found for the Swedish patients (10, 11). Differences in patients’ baseline characteristics may also partly explain some of the national differences found in prosthesis designs and surgical technique. In order to get a full overview of demographics regarding hip fracture treatment future studies should also include other treatment modalities such as total hip arthroplasties and internal fixation.
Prostheses and surgical technique
We found large differences in prosthesis brands between the two countries. Similar differences have previously been found for total hip arthroplasties in the Nordic countries (5). These differences are most likely a result of both traditions and marketing strategies. Our results showed that the stems most commonly used in THAs were also used in HAs. This could indicate that most hospitals use the same femoral stems for both THAs and HAs. There were few unipolar implants in the Norwegian registry. In Sweden, however, unipolar HAs were more frequently used during the last part of the study period. One explanation can be results from recent studies from the SHAR showing an increased risk of reoperation for bipolar prostheses compared to unipolar prostheses (12, 13). Similar investigations have not been performed in the Norwegian register since the number of unipolar HAs has been too small. The reason for this difference in the use of bipolar heads between our countries is not known. Probably, local traditions and differences in prostheses marketing between the two countries play a significant role. In Norway, uncemented prostheses are used with increasing frequency. In Sweden the use of uncemented HAs have decreased mainly because the Austin Moore prostheses were abandoned (2). Register studies have found increased risk of reoperations and revisions after uncemented HA when compared to cemented ones in older populations, mainly because of more infections, loosening, and more periprosthetic fractures (13, 14). There are, however, concerns about a possible higher peroperative and immediately postoperative mortality after cemented HA-procedures (15). Further studies on the mortality after cemented HAs should be done.
Reoperations
There were more reoperations due to infection in Norway. This can probably be explained by the more frequent use of uncemented HAs which have been found to increase the risk of infection in earlier studies (6, 14, 16). There were more reoperations due to dislocation in Sweden. The reason for this difference is not obvious, but one explanation could be the more frequent use of the posterior approach which in earlier studies has been found to increase the risk of dislocations (13, 17). The cemented implants performed worse in Sweden than in Norway. This could be due to different indications for revisions in the two countries. A difference in completeness of reoperation procedures reported to the two registries may also affect the results. So far, however, we have no certain explanation to the differences found and this must be further investigated. Despite the large differences found in types and fixation of HAs between Norway and Sweden the results of the two countries were almost comparable. This does not mean that the type of prostheses, type of fixation, and surgical approach used did not influence the results. More likely, this shows the large complexity of the situation. Confounding by indication and other confounding factors must be investigated further before final conclusions can be made. A study on reoperations in this common data set has been initiated to more thoroughly investigate to what extent different prosthesis designs, types of fixation and surgical approaches influence the survival of the implants.
Strengths and limitations of study
The strength of our study is the high number of patients included, and that the findings represent the average results that can be achieved from orthopaedic surgeons on a national level. It was also possible to analyse changes over time. On the other hand, only information present in both national databases could be included in the common dataset. Accordingly, one major weakness is that the dataset includes less information on each operation than originally present in the national databases. The common dataset lacks information on patient reported outcome measurements. These data are also important when trying to choose the correct implant or the correct operation method for different types of patients. One concern is the possibility of under-reporting of reoperations, and in particular minor reoperations. We have, however, no reason to suspect that the completeness of the reporting of reoperations is different in the two countries. With large number of prostheses also small differences may reach statistical significance. Accordingly, the magnitude of any differences must be considered and especially when they are numerically small.
In conclusion, even between two neighboring countries, large differences in implant design, surgical technique, and – to some extent – demographics have been revealed. One can only speculate to what extent these differences can be regarded to exist worldwide. Such differences must be considered when comparing studies from different countries. Nonetheless, our common dataset of hemiarthroplasties will be a platform for future studies. Such studies, with or without further data collection, will address more specific issues with the ultimate goal to expand our knowledge about femoral neck fractures and how to reach an optimum treatment algorithm.
Footnotes
Financial Support: None.
Conflict of Interest: None.
References
- 1.Gjertsen JE Engesaeter LB Furnes O et al. The Norwegian Hip Fracture Register. Experiences after the first 2 years and 15,576 reported hips. Acta Orthop 2008;79(5):583–93 [DOI] [PubMed] [Google Scholar]
- 2.Leonardsson O Garellick G Karrholm J Akesson K Rogmark C Changes in implant choice and surgical technique for hemiarthroplasty. 21,346 procedures from the Swedish Hip Arthroplasty Register 2005-2009. Acta Orthop 2012;83(1):7–13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Engesaeter LB Furnes O Havelin LI The Norwegian Arthroplasty Register. Annual report 2011. Available at: http://nrlweb.ihelse.net/Rapporter/Rapport2011.pdf. Accessed November 19 2012
- 4.Rogmark C Spetz CL Garellick G More intramedullary nails and arthroplasties for treatment of hip fractures in Sweden. Acta Orthop 2010;81(5):588–92 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Havelin LI Fenstad AM Salomonsson R et al. The Nordic Arthroplasty Register Association: a unique collaboration between 3 national hip arthroplasty registries with 280,201 THRs. Acta Orthop 2009;80(4):393–401 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Dale H Skramm I Lower HL et al. Infection after primary hip arthroplasty. Acta Orthop 2011;82(6):646–54 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.American Society of Anaesthesiologists. New classification of physical status. Anaesthesiology 1963(24):111 [Google Scholar]
- 8.Fine JP Gray RJ A proportional hazards model for the subdistribtion of a competing risk. J Am Stat Assoc 1999;94(446):496–509 [Google Scholar]
- 9.Gillam MH Salter A Ryan P Graves SE Different competing risks models applied to data from the Australian Orthopaedic Association National Joint Replacement Registry. Acta Orthop 2011;82(5):513–20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Leonardsson O Arthroplasty for Femoral Neck Fracture. Results of a nationwide implementation Malmö, Sweden: Lund University, 2012. Dissertation. [Google Scholar]
- 11.Thorngren KG Rikshöft. Yearly Report 2011. Available at: http/:wwwrikshoftse/se/2012. Accessed November 19 2012
- 12.Garellick G Karrholm J Rogmark C Herberts P Annual Report 2010. Swedish Hip Arthroplasty Register Available at: http://wwwshprse/Libraries/Documents/AnnualReport-2010-3sflbashx2011. Accessed November 19 2012
- 13.Leonardsson O Karrholm J Akesson K Garellick G Rogmark C Higher risk of reoperation for bipolar and uncemented hemiarthroplasty. Acta Orthop 2012;83(5):459–66 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gjertsen JE Lie SA Vinje T et al. More re-operations after uncemented than cemented hemiarthroplasty used in the treatment of displaced femoral neck fractures: an observational study of 11,116 hemiarthroplasties from a national register. J Bone Joint Surg Br 2012;94(8):1113–9 [DOI] [PubMed] [Google Scholar]
- 15.Talsnes O Vinje T Gjertsen JE et al. Perioperative mortality in hip fracture patients treated with cemented and uncemented hemiprosthesis: a register study of 11,210 patients. Int Orthop 2013;37(6):1135–40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dale H Hallan G Espehaug B Havelin LI Engesaeter LB Increasing risk of revision due to deep infection after hip arthroplasty. Acta Orthop 2009;80(6):639–45 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Enocson A Tidermark J Tornkvist H Lapidus LJ Dislocation of hemiarthroplasty after femoral neck fracture: better outcome after the anterolateral approach in a prospective cohort study on 739 consecutive hips. Acta Orthop 2008;79(2):211–7 [DOI] [PubMed] [Google Scholar]