

Abstract
Rationale:
The anatomical variant of the distal biceps femoris muscle with regard to common peroneal nerve entrapment neuropathy (CPNe) was suggested through magnetic resonance images (MRI) study.
Patient concerns:
An unusual variant of distal biceps femoris muscle was observed in 78 years old male cadaver.
Diagnoses:
The short head of biceps femoris muscle (SHBFM) was extended more distal and posteriorly.
Intervention:
The popliteal area was dissected at knee joint level in a cadaveric limb.
Outcomes:
Common peroeal nerve (CPN) was situated within tunnel formed between the lateral head of the gastrocnemius muscle (LGCM) and the SHBFM. Also, the length of tunnel was 4.4 cm.
Lessons:
The case illustrated here, to the best of our knowledge, is the first one with cadaveric findings of variant of distal biceps femoris muscle associated with CPNe. The tunnel formed between the more posterior or distal extension of the SHBFM and the LGCM could be possible entrapment area of CPN, clinically.
Keywords: anatomy, biceps femoris muscle, common peroneal nerve, neuropathy
1. Introduction
The common peroneal nerve (CPN) is the lateral division of the sciatic nerve and it courses from the posterolateral side of the popliteal area around the biceps femoris tendon and the fibular head.[1,2] These anatomical features contribute to the vulnerability of the peroneal nerve to damage around the knee. The most frequent mononeuropathy in the lower extremity has been reported as the common peroneal nerve entrapment neuropathy (CPNe) around the fibular head and neck.[3] Through the investigating the course of the CPN between popliteal muscles, including the short head of biceps femoris muscle (SHBFM) and the lateral gastrocnemius muscle (LGCM) using magnetic resonance images (MRI), the possibility of anatomical variation of distal femoris muscle related to the CPNe by entrapment or compression was proposed.[4] However, there was a limitation of the lack of cadaveric correlation as a result based on MRI. Herein, we reported a case of unusual variant of distal biceps femoris muscle associated with CPNe in Korean cadaver for first time and discussed its clinical significance.
2. Case presentation
During the routine dissection of the popliteal area at knee joint level in a cadaveric limb, diamond-shaped popliteal fossa was exposed with 4 borders, consisting of semimembranosus, biceps femoris, medial head of the gastrocnemius, and lateral head of the gastrocnemius muscles. The specimen was a Korean male cadaver whose age at death was 78 years old. Typically, during the dissection, the common peroneal nerve arises from the sciatic nerve at the upper level of the popliteal fossa and runs obliquely along the lateral side of the biceps femoris muscle and then superficial to the lateral head of the gastrocnemius muscle (Fig. 1). In this cadaver, the tibial nerve was found at the popliteal fossa, but the common peroneal nerve was not observed at the lateral margin of the popliteal fossa (Fig. 2). The distal biceps femoris muscle was identified and then it was reflected to examine its deep layer. The common peroneal nerve descended below the long head of biceps femoris muscle and along the lateral side of the short head of biceps femoris muscle (Fig. 3A). The short head of biceps femoris muscle was extended more distal and posteriorly. Thus, more inferiorly, common peroneal nerve was situated within tunnel consisted of floor by the lateral head of the gastrocnemius muscle and roof by the short head of the biceps femoris muscle due to variation in the muscular structure (Fig. 3B). The length of tunnel was 4.4 cm. There was no evidence of any pathological involvement of the muscular and nervous structures.
Figure 1.
Typically, the common peroneal nerve runs obliquely along the lateral side of the biceps femoris muscle and then superficial to the lateral head of the gastrocnemius muscle. BFM = biceps femoris muscle, CPN = common peroneal nerve, LGCM = lateral head of the gastrocnemius muscle, MGCM = medial head of the gastrocnemius muscle, SMBM = semimembranosus muscle, TN = tibial nerve.
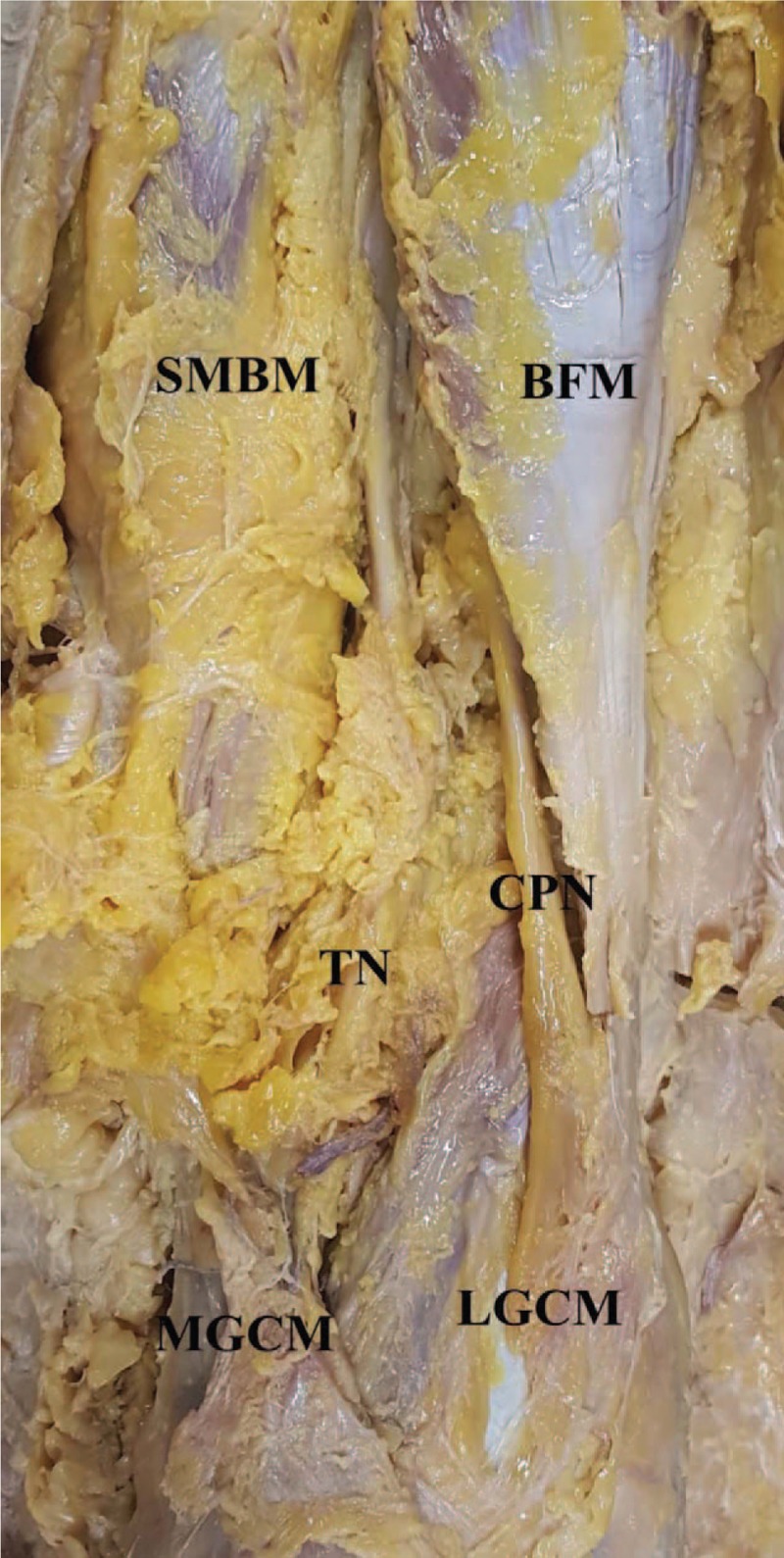
Figure 2.

The common peroneal nerve was not seen at the lateral margin of the popliteal fossa. BFM = biceps femoris muscle, LGCM = lateral head of the gastrocnemius muscle, MGCM = medial head of the gastrocnemius muscle, SMBM = semimembranosus muscle, TN = tibial nerve.
Figure 3.
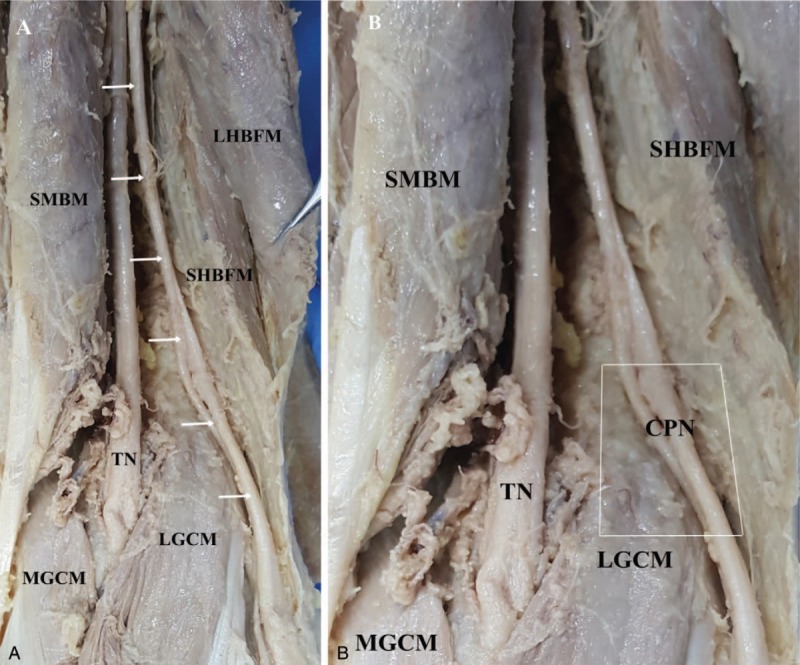
A, The common peroneal nerve (white arrows) descended below the long head of biceps femoris muscle and along the lateral side of the short head of biceps femoris muscle. B, Enlarged image of Fig. 3A. The short head of biceps femoris muscle was extended more distal and posteriorly. The common peroneal nerve runs within tunnel (white lines) formed between the lateral head of the gastrocnemius muscle and the short head of the biceps femoris muscle. CPN = common peroneal nerve, LGCM = lateral head of the gastrocnemius muscle, LHBFM = long head of biceps femoris muscle, MGCM = medial head of the gastrocnemius muscle, SHBFM = short head of biceps femoris muscle, SMBM = semimembranosus muscle, TN = tibial nerve.
The cadaver used in the present study was donated to our institutions with consent for education and research. In addition, this study was confirmed to be an exemption of the approval from an Institutional Review Board committee at our institutions, as a cadaveric study.
3. Discussion
The common peroneal nerve (CPN) branches from the sciatic nerve and descends obliquely along the lateral side of popliteal fossa to the head of the fibula. It runs close to the medial margin of the biceps femoris muscle laying between the tendon of the biceps femoris and lateral head of the gastrocnemius muscle, and then winds around the neck of the fibula (fibular tunnel).[1,2,5,6] In addition, MRI findings have demonstrated that CPN courses posterior to the short head of biceps femoris muscle (SHBFM), and then superficially to the lateral head of the gastrocnemius muscle (LGCM). More inferiorly, it winds around the neck of the fibula (fibular tunnel).[2,7] Due to the superficial location of the CPN around the knee, it is known to be the most vulnerable to compression or entrapment at the fibular head and neck.[3] On the other hand, there have been reported that compression or entrapment may occur due to anatomical variations of the CPN itself.[1,5] The anatomical variant of the distal biceps femoris muscle as predisposing factor for common peroneal nerve entrapment neuropathy (CPNe) was first suggested by Vieira et al.[4] Through MRI-based study, the authors described the presence of narrow fatty tunnel formed between the SHBFM and the LGCM as a possible entrapment area. This tunnel could be formed when there is a more posterior or distal extension of the SHBFM and, rarely, when there is a more distal extension of the long head of the biceps femoris muscle (LHBFM). In our cadaveric finding, SHBFM was extended more distal and posteriorly and this muscle variant existed as a roof-like structure for CPN. Thus, CPN passed through a tunnel formed between the SHBFM and the LGCM. In the previous MRI study, the length of the tunnel in the symptomatic patient was 4.5 cm and only 1 case (4.2%) of the asymptomatic population had a tunnel length of 4 cm or greater, interestingly. The length of tunnel in our cadaver was 4.4 cm and then, this cadaveric finding may represent unusual variant of distal biceps femoris muscle associated with CPNe.
The biceps femoris muscle as a strong flexor of the knee joint and has 2 heads of origin. The long head arises together with the semitendinosus muscle from the ischial tuberosity, crosses laterally, and becomes tendinous 7 to 10 cm above the knee joint.[8] In this cadaver, the distance between the distal myotendinous junction of the LHBFM from the joint level was 3.2 cm and this finding was different from the previously reported data. Thus, if the tunnel is formed with regard to the CPNe, it would not be able to rule out the possibility to be accompanied by variation of SHBFM as well as variation of LHBFM. Meanwhile, the SHBFM arises from the lateral prolongation of the linea aspera of the femur. The tendons of the short head and long head merge above the knee joint, and the combined tendon inserts into the head of the fibula.[8] But, there is no evidence in the literature of the distal extent of the SHBFM relative to the knee joint level. Therefore, a prospective cadaveric study regarding the distal muscle extension of biceps femoris by dividing SHBFM and LHBFM at the knee joint level would be required in the future.
Common peroneal nerve entrapment (CPNe) could have variable causes. The common cause includes trauma to the nerve, such as blunt trauma, proximal fibular fracture, surgical complications, or compression from an improperly positioned cast.[9] Most of traumatic causes may involve the CPN around the fibular head and neck area; while idiopathic or posture-induced CPNe could occur after maintaining a certain posture for a long time. The kneeling and squatting postures most often induced CPNe in Asians.[10] However, the authors could not define a possible compression site of the CPN during hyper-flexion of knees, except for the fibular tunnel. Also, Masakado et al[6] mentioned fibular tunnel, as a compression site of the CPN when knee was hyper-flexed, but could not describe the mechanism for entrapment of CPN. Since the popliteal fossa would be affected by hyper-flexion of knee during kneeling and squatting postures, CPN could be compressed at popliteal fossa rather than fibular tunnel if the tunnel formed by variant of distal biceps femoris muscle was existed. Thus, we assumed that unusual variant of distal biceps femoris muscle could be predisposing factor with regard to CPNe, especially idiopathic or posture-induced neuropathy.
4. Conclusions
In this report, we first present cadaveric findings of unusual variant of distal biceps femoris muscle associated with common peroneal entrapment neuropathy (CPNe). The tunnel formed between the more posterior or distal extension of the SHBFM and the LGCM could be possible entrapment area of CPN, clinically. Therefore, this anatomical variant of distal biceps femoris muscle should be evaluated in the patient not diagnosed the CPNe around fibula head and neck.
Acknowledgments
The authors thank all those who donate their bodies and tissues for the advancement of education and research.
Author contributions
J-HP and K-RP collected the patient's clinical data and wrote the manuscript. They contributed equally to the article. J-HP, K-RP, JY, G-HP, and JC reviewed the literature and drafted the manuscript. JC designed the study and edited the manuscript. All authors read and approved the final manuscript.
Conceptualization: Jinseo Yang.
Investigation: Kwang-Rak Park, Gun-Hyun Park.
Writing – original draft: Jaeho Cho.
Writing – review & editing: Jeong-Hyun Park, Kwang-Rak Park, Jaeho Cho.
Footnotes
Abbreviations: CPN = common peroneal nerve, CPNe = common peroneal nerve entrapment neuropathy, LGCM = lateral head of the gastrocnemius muscle, LHBFM = long head of the biceps femoris muscle, MRI = magnetic resonance imaging, SHBFM = short head of biceps femoris muscle.
J-HP and K-RP contributed equally to this work and should be considered co-first authors.
The authors have no conflicts of interest to disclose.
References
- [1].Arora AK, Verma P, Abrol S. An anomalous variation in the division pattern of the common peroneal nerve. Int J Appl Basic Med Res 2011;1:118–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Loredo R, Hodler J, Pedowitz R, et al. MRI of the common peroneal nerve: normal anatomy and evaluation of masses associated with nerve entrapment. J Comput Assist Tomogr 1998;22:925–31. [DOI] [PubMed] [Google Scholar]
- [3].Aprile I, Caliandro P, La Torre G, et al. Multicenter study of peroneal mononeuropathy: clinical, neurophysiologic, and quality of life assessment. J Peripher Nerv Syst 2005;10:259–68. [DOI] [PubMed] [Google Scholar]
- [4].Vieira RL, Rosenberg ZS, Kiprovski K. MRI of the distal biceps femoris muscle: normal anatomy, variants, and association with common peroneal entrapment neuropathy. AJR Am J Roentgenol 2007;189:549–55. [DOI] [PubMed] [Google Scholar]
- [5].Deutsch A, Wyzykowski RJ, Victoroff BN. Evaluation of the anatomy of the common peroneal nerve. Defining nerve-at-risk in arthroscopically assisted lateral meniscus repair. Am J Sports Med 1999;27:10–5. [DOI] [PubMed] [Google Scholar]
- [6].Masakado Y, Kawakami M, Suzuki K, et al. Clinical neurophysiology in the diagnosis of peroneal nerve palsy. Keio J Med 2008;57:84–9. [DOI] [PubMed] [Google Scholar]
- [7].Donovan A, Rosenberg ZS, Cavalcanti CF. MR imaging of entrapment neuropathies of the lower extremity. Part 2. The knee, leg, ankle, and foot. Radiographics 2010;30:1001–19. [DOI] [PubMed] [Google Scholar]
- [8].Sneath RS. The insertion of the biceps femoris. J Anat 1955;89:550–3. [PMC free article] [PubMed] [Google Scholar]
- [9].Anderson JC. Common fibular nerve compression: anatomy, symptoms, clinical evaluation, and surgical decompression. Clin Podiatr Med Surg 2016;33:283–91. [DOI] [PubMed] [Google Scholar]
- [10].Yu JK, Yang JS, Kang SH, et al. Clinical characteristics of peroneal nerve palsy by posture. J Korean Neurosurg Soc 2013;53:269–73. [DOI] [PMC free article] [PubMed] [Google Scholar]