

INTRODUCTION
Dynamic systolic compression of the coronary arteries is frequently observed due to the existence of myocardial bridging and most commonly localized in the middle segment of the left anterior descending (LAD) coronary artery.1 However, it has rarely been reported in patients with pericardial adhesions, trauma, tumor, foreign body, postinfarction dyskinetic left ventricular aneurysm, or pseudoaneurysms.2-4 As this clinical phenomenon may present with several forms, in this paper, we report the case of a 56-year-old male patient with a myocardial bridge-like systolic compression of the distal right coronary artery (RCA) caused by postinfarction dyskinetic left ventricular aneurysm presenting to our clinic with subacute inferior myocardial infarction.
CASE
A 56-year-old man, with no history of coronary artery disease (CAD), presented to our cardiology clinic due to the chief complaint of recurrent episodes of retrosternal pain, which started three days ago. The episodes lasted 10 to 15 minutes and were accompanied by sweating. The patient reported that the symptoms occurred mainly during exercise. His vital signs on admission were as follows: blood pressure: 123/72 mmHg; heart rate: 74 beats/min. Medical history was significant for dyslipidemia and diabetes mellitus. He was an ex-smoker and had no family history of CAD or sudden death. Immediately after admission, electrocardiography (ECG) showed mild ST-segment elevation and accompanying QS pattern in inferior leads (II, III, and aVF) (Figure 1A). Transthoracic echocardiography revealed an inferior wall left ventricle aneurysm with an estimated left ventricular ejection fraction of 48%. Cardiac magnetic resonance imaging showed a huge inferior wall left ventricular aneurysm (Figure 1B). An increase in the troponin T was also detected. Considering these findings, he was diagnosed with subacute inferior myocardial infarction and post-infarction angina and transported to catheter laboratory for urgent coronary angiography. Coronary angiography revealed 95% thrombotic lesion in the distal portion of the RCA, significant obstruction causing 80% narrowing in the proximal portion of the LAD coronary artery, and significant obstruction causing 80% narrowing in the proximal portion of left circumflex high-obtus marginatus (Cx-OM) coronary artery, respectively. RCA lesion was considered as infarct-related artery. Subsequently, sequential balloon expansion was performed, and the distal-RCA lesion was successfully stented (2.5 mm × 30 mm drug-eluting stent) with an excellent angiographic result. The patient was transferred to coronary intensive care unit and treated with acetylsalicylic acid, clopidogrel, atorvastatin, perindopril, metoprolol, and lansoprazole therapy. The patient was discharged from hospital with stable clinical status and optimal medical treatment four days later. Two weeks after the first procedure due to the continuation of anginal symptoms, an elective coronary angiography and percutaneous coronary intervention was planned to the patient. Subsequent coronary angiogram of the RCA demonstrated absence of restenosis/thrombosis of the previously implanted RCA stent, and showed a dynamic myocardial bridge-like systolic compression of the distal RCA (Figure 2). LAD and Cx-OM lesions were directly stented with 2.5 mm × 30 mm and 3 mm × 15 mm drug-coated stents, respectively. The coronary angiography performed 15 days ago was reviewed again, showing the absence of this systolic compression of RCA immediately after coronary stent implantation. The patient stayed at stable clinical status with optimal medical treatment and discharged from the hospital.
Figure 1.
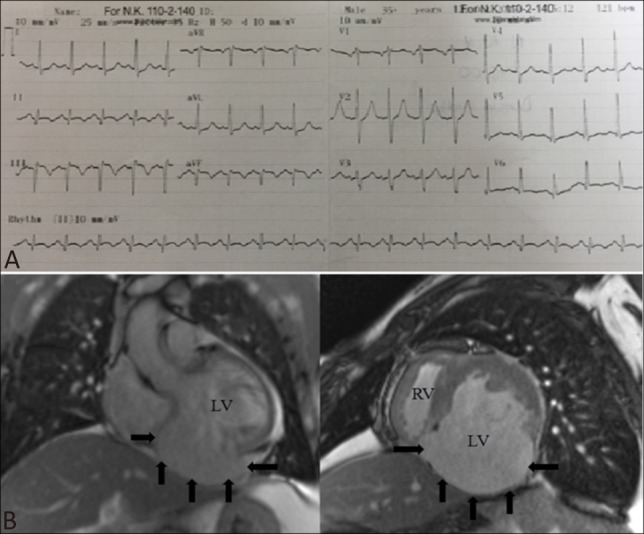
Electrocardiography and magnetic resonance imaging findings of the patient (A) Admission electrocardiography revealed normal sinus rhythm with narrow QRS duration, mild ST-elevation accompanying QS formation in leads II, III, and aVF. (B) Cardiac magnetic resonance imaging revealed an inferior wall left ventricle aneurysm (black arrowed).
Figure 2.
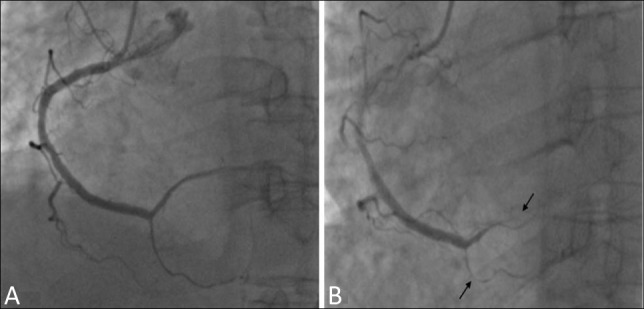
Elective coronary angiography of RCA performed 15 days later the ACS. (A) Coronary angiogram of RCA during diastole (B). Coronary angiogram of RCA during systole showing significant milking-like effect (black arrowed) secondary to dynamic compression. ACS, acute coronary syndrome; RCA, right coronary artery.
DISCUSSION
In this case report, we have described a case of a dynamic systolic compression of RCA secondary to dyskinetic left ventricular aneurysm, which was not observed in the first coronary angiogram performed during acute coronary syndrome (ACS) clinical setting. To the best of our knowledge, such an observation has not been described in the literature previously. Myocardial bridging is a congenital abnormality of a coronary artery and systolic compression of the myocardial tissue to the intra-myocardial navigating coronary artery segment.5 During the coronary angiography, it is recognized as systolic compression of an epicardial coronary segment resulting in systolic compression of that segment. Although systolic compression of the coronary artery is commonly associated with myocardial bridging, it has rarely been reported in patients with pericardial adhesions, tumor, foreign body, or pseudoaneurysms.6-8 Only rare case reports exist regarding myocardial bridge-like coronary compression by a dyskinetic left ventricular aneurysm.6,8-10 Marti et al. previously reported coronary milking-like effect caused by systolic expansion of a traumatic focal left ventricular aneurysm.10 Moreno et al. presented a patient with a postinfarction left ventricular aneurysm in which coronary angiography revealed a milking-like effect with systolic compression of the distal LAD coronary artery.9 Dogan et al. presented a patient with a myocardial bridge-like systolic compression of the distal LAD caused by postinfarction dyskinetic left ventricular aneurysm.2 Ferrer Hita et al. showed the posterior descending artery milking-like effect caused by ventricle pseudoaneurysm compression.4 Acute myocardial infarction associated myocardial bridges have been described in the literature previously; however, in our case, myocardial bridge was not detected in the first coronary angiogram. Although myocardial bridges are almost exclusively localized in the middle segment of the LAD coronary artery;1 in this case, the systolic compression was prominent at the distal part of the RCA in where an unusual position for myocardial bridging but associated with dyskinetic inferior wall aneurysm. Therefore, we suggest that dyskinetic parts of left ventricular wall caused the systolic external compression of the distal portion of the RCA mimicking myocardial bridging-like appearance during systolic ventricular aneurysm filling.
The main observation needs to be discussed in the light of this case report is the absence of systolic compression and milking-like effect in the first coronary angiography which was performed in the clinical setting of ACS. Systolic compression and milking-like effect was observed in the second elective coronary angiography. We think that this inconsistency may be due to the expansion of infarction despite successful reperfusion or accompanying vasospastic process in the coronary artery endothelium during the ACS.
LEARNING POINTS
• Dynamic systolic compression of the epicardial coronary arteries is frequently observed due to the existence of myocardial bridging which is most commonly localized in the middle segment of the LAD coronary artery.
• However, it has rarely been reported in patients with pericardial adhesions, tumor, foreign body, postinfarction dyskinetic left ventricular aneurysm, or pseudoaneurysms.
• Herein, we presented the first case report, in which milking-like effect secondary to dynamic systolic compression of the RCA by a postinfarction dyskinetic left ventricular aneurysm, which was hidden in the ACS clinical setting.
REFERENCES
- 1.Möhlenkamp S, Hort W, Ge J, Erbel R. Update on myocardial bridging. Circulation. 2002;106:2616–2622. doi: 10.1161/01.cir.0000038420.14867.7a. [DOI] [PubMed] [Google Scholar]
- 2.Dogan P, Oksuz F, Grbovic E, et al. Dynamic systolic compression of the left anterior descending coronary artery by a postinfarction dyskinetic left ventricular aneurysm. Int J Angiol. 2016;25:14–15. doi: 10.1055/s-0034-1396790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Channer KS, Pugh PJ. Interfering with healing: the benefits of intervention during acute myocardial infarction. Heart. 2001;85:620–622. doi: 10.1136/heart.85.6.620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ferrer-Hita J, Tuesta ID, Lacalzada J, et al. Posterior descending artery milking-like effect caused by ventricle compression. Circulation. 2005;111:453–454. doi: 10.1161/CIRCULATIONAHA.104.495119. [DOI] [PubMed] [Google Scholar]
- 5.Corban MT, Hung OY, Eshtehardi P, et al. Myocardial bridging: contemporary understanding of pathophysiology with implications for diagnostic and therapeutic strategies. J Am Coll Cardiol. 2014;63:2346–2355. doi: 10.1016/j.jacc.2014.01.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Angelini P, Leachman RD, Autrey A. Atypical phasic coronary artery narrowing. Cathet Cardiovasc Diagn. 1986;12:39–43. doi: 10.1002/ccd.1810120110. [DOI] [PubMed] [Google Scholar]
- 7.Parashara DK, Jacobs LE, Kotler MN, et al. Angina caused by systolic compression of the left coronary artery as a result of pseudoaneurysm of the mitral-aortic intervalvular fibrosa. Am Heart J. 1995;129:417–421. doi: 10.1016/0002-8703(95)90031-4. [DOI] [PubMed] [Google Scholar]
- 8.Minami KT, Fergusson DJ. Systolic compression of the right coronary artery by a pseudoaneurysm following mitral valve replacement. Cathet Cardiovasc Diagn. 1989;18:31–35. doi: 10.1002/ccd.1810180110. [DOI] [PubMed] [Google Scholar]
- 9.Moreno R, Perez del Todo J, Macaya C. Milking-like effect secondary to systolic expansion of a post-infarction left ventricular aneurysm. J Invasive Cardiol. 2003;15:608–609. [PubMed] [Google Scholar]
- 10.Martí V, García J, MaAugé J. Coronary milking-like effect caused by systolic expansion of a traumatic focal left ventricular aneurysm. Heart. 2001;85:622. doi: 10.1136/heart.85.6.622. [DOI] [PMC free article] [PubMed] [Google Scholar]