

Abstract
Background:
Awareness of the trends of cancer incidence in each geographic region is an important. The aim of present study was to determine the incidence trends of cancer in Chaharmahal and Bakhtiari (Ch and B) province in Southwest of Iran.
Materials and Methods:
In this secondary data analysis, retrospective existing data were used from cancer registry reports in Ch and B in Southwest of Iran in 2003–2016. Data on epidemiologic trend were analyzed using Joinpoint software package and annual percentage change (APC) with 95% confidence interval (95% CI) was computed.
Results:
Age-standardized incidence rate per 100,000 persons in the province in 2003 was 31.74 that increased to 147.14 in 2016. APC during 2003–2016 was 12.58% (CI: 9.3–16) and significant, which was 10.22% (7.4–13.1) and 14.47% (10.2–18.9) in men and women, respectively. Incidence of the stomach, breast, colorectal, thyroid, lymph node, and ovarian cancers is increasing and the highest incidence was observed in two age groups of 25–34 and 55–64 years.
Conclusion:
In general, cancers are of increasing trend. Surveillance and monitoring the incidence of cancer and studying the causes of environmental or genetic in the cancer changes can help for cancer prevention and control.
Keywords: Cancer, epidemiology, Iran, joinpoint, neoplasm, trends
INTRODUCTION
In Iran, cancers are considered as the third cause of mortality with cardiovascular diseases and accidents are the first cause. The mortality from myocardial infarction in patients with and without diabetes is high in Iran.[1,2] Pattern of cancer incidence is different in various population and is associated with such factors as occupational, social, cultural, ethical, and geographical issues, custom, and nutrition.[3] Epidemiologic studies such as time-trend analysis of disease incidence in different parts of the world lead to the emergence of differences and similarities resulted from comparing their results. Consequently, observation of differences obtains a proof for findings its causes and Due to lack of information about cancer in the geographical area.[4] Knowledge of various cancers in any particular geographical area can help planning the health services for patients and screening the high-risk group of that area.[5] Cancer registration and time-trend analysis is a management tool for measuring the cancer incidence in a specific population over a period of time, so that the effect of cancer can be evaluated and controlled in the community.[6] Economic, social, and demographic changes throughout the years in Iran have yielded significant changes in the patterns and trends of cancer.[7] Up to now, no valid report of the trends of cancers has been presented in Chaharmahal and Bakhtiari (Ch and B) province in Southwestern Iran. This is the first study which has been designed and aimed at investigating the trend of cancer incidence in this province.
MATERIALS AND METHODS
Study design
This study was secondary data analysis and done based on existing data that were conducted using all data of pathology-based cancer incidence (2003–2016) in Ch and B province in Southwestern Iran. These data were collected retrospectively reviewing all new cancer patients registered in Cancer Registry Center by Health Deputy of Shahrekord University of Medical Sciences (SKUMS) and covers >95%.[8] The target population included all patients with cancer having definite pathology sample of cancer. Data based on a definitive pathologic diagnosis of cancer registry were collected from various resources including clinics, laboratories, and centers of histology and cytology throughout the province, the hospitals, death certificates, and forensic offices. Cancer diagnosis has been based on pathology laboratory and book coding International Classification of Disease (ICD)-O2 and ICD.[8]
Statistical analysis
Two types of analyzes were conducted in this study. The first analysis was performed according to the main objective of the study to calculate the incidence trends of cancers during the years 2003–2016. In the second analysis, due to the lack of access to details of all patients’ data during the aforementioned years and access to data from 2014 to 2010, only the data of this period were analyzed separately. In order to determine the fundamental changes in the process, age-standardized incidence rate (ASIR) per 100,000 persons using direct standardized method and world standard population in 2003–2016 was used. For analysis, we used joinpoint regression model using the software Joinpoint Regression Program, Version 4.6.0.0 (National Cancer Institute, The Surveillance, Epidemiology, and End Results (SEER) Program, USA) to identify the years when significant changes took place in the age-standardized rates (ASRs). This model is a method for segmentation of the nonlinear regression model into separate linear fragments, which are separated by joinpoints. Joinpoint regression analyzes and estimates the trend of cancer.[9] Joinpoint regression analysis involves fitting a series of joined straight lines on a log scale to the trends. The final model selected was the most parsimonious of these, with the estimated annual percent change (APC) based on the trend within each segment. All statistical tests were two-sided. In describing trends, the terms “significant increase” and “significant decrease” signify that the slope of the trend was statistically significant (P < 0.05).[10,11,12]
Assume i = 1, 2, n is independent variable that can indicate the process of death or incidence and can be a crude numerical value, modified amount, or the age. Moreover, i = 1, 2, n is the time variable whose trend we want to study.
Joinpoint regression equation is as follows:

Where (β0, β0, δk,......δk) are the parameters of the regression model.
Equation (1) shows the joinpoint regression model. This formula consists of the width from the origin and the regression coefficients. k indicates the number of unknown points, ti for i = 1....., k represents the locations of the unknown change points, and are the regression coefficients of the fragments.
δk(ti)=(t-τk)t (2)
Equation (2) shows the regression coefficients of the fragments, where represents the joinpoint.
And τkt=(τ1,τ2, τk) (3)
Equation (3) shows the number of joinpoints for k change(s). Is the random error with mean of 0. Furthermore, logarithmic log (rate) can be considered as response variable. Parameter APC (percent change annually) is used to check the trend between 2 years which is calculated as follows:

Equation (4) shows the APC (yt) calculated by Equation (1).
When there is a trend distance, P ≤ 0.05. This study did not have any particular moral constraint. Researcher studied the registered statistics observing all ethics in research and without any intervention. Confidentiality and integrity were considered in all phases of the study and all stages of the work were done with the permission of SKUMS.
RESULTS
Crude incidence rate of cancer per 100,000 persons in the province in 2003 was 22.08 that increased to 136.42 in 2016. ASIR per 100,000 persons in the province in 2003 was 31.74 that increased to 147.14 in 2016. APC during 2003–2016 was 12.58% (confidence interval [CI]: 9.3–16) and significant, which was 10.22% (7.4–13.1) and 14.47% (10.2–18.9) in men and women, respectively. The average annual incidence rate of cancer was 70.14/100,000 people. Annual incidence rates during the years 2003–2016 in men and women are presented in Table 1. The overall incidence trend of cancers in 2003–2016 had been significantly increased (APC = 12.6%, P < 0.01). The APC of cancer in men and women in the years 2003–2016 in the Ch and B province had a significant and increasing trend (P < 0.05). Joinpoint analysis showed the significant increasing trend of ASIR for both sexes. Figure 1 illustrates the incidence of cancer in the years 2003–2016 in Ch and B province. The results of the cancer data analysis for 2010–2014 are as follows:
Table 1.
Case number, crude rate and age adjusted incidence of cancer rate per 100,000
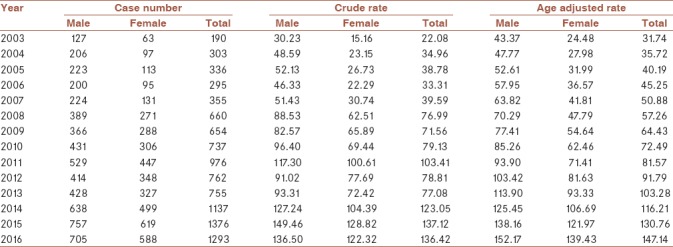
Figure 1.

Cancer incidence trend by annual percentage change in joinpoint analysis 2003–2016
This study showed out of 2918 new cases of cancers occurred in Ch and B in 2010–2014; 1183 cases were female (40.54%) and 1735 (59.46%) were male. Annual incidence of all cancers was 68.2/100,000 population in 2010–2014, so that it was 38.5 and 26.2/100,000 population in male and female, respectively. Trend of incidence of the stomach, breast, colorectal, thyroid, lymph node, and ovarian cancer was rising. In 2014, the observed incidence ratios of common cancers, including stomach, breast, colorectal, thyroid, lymph nodes, ovaries, and bladder, were 0.11, 0.12, 0.09, 0.06, 0.02, 0.03, and 0.08, respectively. Overall observed trend and common cancers are given in Figure 2 for Ch and B in 2010–2014. The highest incidence in term of age group was in 25–34 and 55–64 years. The incidence trend of observed cancers in Ch and B province by age group in 2010 and 2014 is shown in Figure 3.
Figure 2.
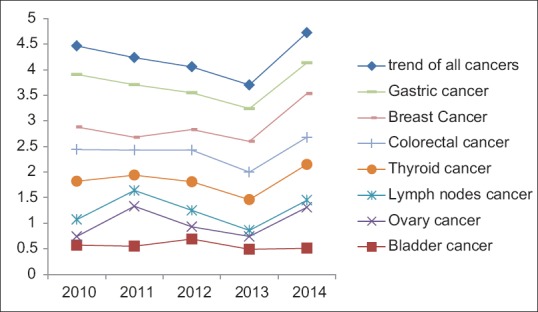
Trend of observed overall and common cancers - incidence in Chaharmahal and Bakhtiari 2010–2014
Figure 3.
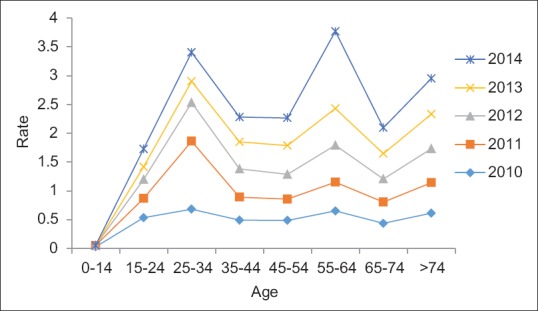
Trend of all cancer - incidence in Chaharmahal and Bakhtiari province by age group 2010–2014
DISCUSSION
According to obtained results, time trend of all cancer incidences in Ch and B in Southwest of Iran has an increasing trend. Pattern of incidence of various cancers was different in the various populations and is related to such factors as occupational, social, cultural, ethical, and geographical issues, custom, and nutrition.[2] The average annual incidence of cancer in Ch and B province was 70.41/100,000 people, less than the average annual incidence of cancer in Iran and the world. According to the official report of Iran population-based cancer registry, the annual incidence of cancer in Iran was reported to be 158/100,000 people (including skin cancer) and 143,000 people (regardless of skin cancer). Furthermore, the average annual incidence of cancer (regardless of skin cancer) in the world based on the World Cancer Registry Report in five continents is 182/100,000 people.[13] Annual incidence of all cancers was more in males than females in Ch and B. In terms of gender pattern, it is consistent to with statistics 2012 GLOBOCAN, but in terms of quantitative comparison, however, the incidence of cancer in the province of Ch and B was less than that of the GLOBOCAN statistics, so that ASR of cancer incidence in developing countries for males was 163 and >135.8% for women.[14] In 2016, compared to the base year (2003), the incidence of cancers in Ch and B province was more than triple and a half. This statistics shows that the incidence of cancers has risen in this area. Part of the increase in early years is due to the completion of the cancer registration process and the improvement of diagnostic services and partly due to the extremely increased incidence of cancer in this geographical area. Like this study, limited studies including ones in China and Spain have been done. A study by China reported a rise in the incidence of prostate cancer in the last four decades with APCs of 2.2% (95% CI: 0.3%–4.3%), 13.2% (11.4%–15.0%), and 3.2% (−0.3%–6.8%), respectively. The mortality trend was stable before 1985 and increased slowly but steadily after 1985, with APC of −0.6% (−4.4%–3.3%) and 5.3% (4.7%–6.0%), respectively.[15,16] The findings of this study were compared with other studies in other provinces of Iran including Qom.[17] There was an increasing and significant trend, according to APCs equal to 8.08% (CI: 5.1–11.1) for all site cancer in women. Trend of all cancer incidences in Ch and B in Southwest of Iran is higher in men than women. In several studies, the incidence of cancer in men was higher than that of women. Rafiemanesh in his study showed that the trend of esophageal cancer over 6 years is higher in men than women, and the APCs was 7.9 (95% CI: 3.3–12.6) for women and 9.6 (95% CI: 6.0–13.2) for men.[10]
The results of the study showed that during the related years, trend of gastric, colorectal, breast, thyroid, lymph nodes, and ovaries was rising. This raising trend was significant. Haidari, in his study, attributed the increase in the incidence of gastric cancer in Iran to the high prevalence of Helicobacter pylori infection and the change in diet patterns that are supplemented by fried foods and the lack of fresh fruits and vegetables and the improvement of cancer diagnostic techniques in the country and the improvement of the quality of the cancer registration system[18] that is consistent to our study. Various studies have shown an increasing trend in colorectal cancer in Iran,[4,19] which is consistent with our study. The pattern of Iranian food consumption shows an increase in the incidence of colorectal cancer, so that in the recent years, people have replaced traditional foods with their prepared and fatty foods.[20,21,22]
According to the results of this study implying an increase in the incidence of ovarian cancer in Ch and B province, Sharifian et al. in their study showed that the incidence trend and mortality of ovarian cancer has been significantly increased in Iran from 1999 to 2013.[23] Factors such as the prevalence of unhealthy fat consumption in Iran have contributed to cancer, so that about 70% consumed fat of Iranian is saturated fat,[24] and in the recent decades, population growth and birth rates in Iran have declined and consumption of oral contraceptives has changed,[25] increasing the risk of ovarian cancer in Iran. Safavi et al. showed the increasing trend of incidence of thyroid cancer in Iran in 2004–2010.[26] In comparison to the past, improvement of diagnostic technique for thyroid cancer has influenced the increase in the incidence of thyroid cancer.[27] In accordance with our results, various studies in Iran showed the ascending trend in the incidence of breast cancer.[28] Increasing the women's awareness and diagnostic screening tests,[29] increasing life expectancy, and changing lifestyle in the Western style[30] lead to an increase in the number of patients in the recent year. The results of the study showed that the incidence of bladder cancer in Ch and B province is constant. According to various reports, the incidence of bladder cancer in Iran has an ascending trend and high provincial dispersion. Improving the cancer registration system and increasing life expectancy, lifestyle, and smoking have led to an increase in the incidence of bladder cancer in Iran.[31]
In the present study, trend of incidence of lymphoma cancer was raising. Lymphoma cancer has been increasing across the world in 2004–2008. In Yazd, Ahvaz, Isfahan, and Kerman, the most incidence of lymphoma cancer has been observed.[32] Results of our study are consistent to that conducted in Kerman showing the increasing trend in lymphoma cancer. In the present study, increased smoking in Kerman has contributed to increase in lymphoma cancer.[33]
The result of this study showed that the incidence of cancer in Ch and B province after 65 years of age is increased. The incidence of all cancers is increased after 60 years of age.[34] One of the reasons for the increased risk of cancer with age may be decline in mobility.[35] This study is the first study to investigate the incidence of cancers in Ch and B in Southwest of Iran, which can serve as a reference for decision-makers in the health system and like an experimental study, can serve as a solid foundation for management and researchers in Iran.[36] This study has some limitations. Access to all patients’ data within 15 years was not possible based on the type of cancer and the clinical and paraclinical characteristics of the patients, and only some cancer information was available for the years 2010–2014, which was used. Cancer registration program of the province has many defaults; sometimes, the differences in the quality and coverage of data are observed, and in some cases, there is undercount and misclassification. Moreover, improving the cancer registration system may be one of the reasons of increasing the cancer. It seems that reviewing the existing plan and using different method for cancer registration based on population are necessary for correct estimation of cancer rate in the country.
CONCLUSION
The annual average incidence trend of cancers in 2003–2016 had been significantly increased 12.6%, and the incidence of stomach, breast, colorectal, thyroid, lymph node, and ovary cancers is increasing in Ch and B provinces. Therefore, the plan for the control and prevention of these cancers must be a high priority for health policy-makers. Although this increase may be partly attributed to the change and improvement in cancer registry system in the province and the improvement of diagnostic technique and awareness of people of self-assessment and referral to diagnostic centers, but in any case, the increasing incidence of cancers is significant and requires further studies to determine the causes. Considering the increasing trend of these cancers, screening and early diagnosis in high-risk individuals is recommended. Health system managers should consider the diversity of patterns and risk factors for the planning and controlling these patients. Therefore, it is necessary that health policy-makers pay special attention to increasing public awareness and raising public awareness of cancer as a health priority and to take the prevention of cancer seriously through continuously negotiating with the mass media,
Financial support and sponsorship
Shahrekord University of Medical Science and Modeling in Health Research Center, health deputy of Shahrekord University of Medical Science. The funding sources played no role in the study design, data analysis, and manuscript writing, or in the decision to submit this manuscript for publication.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This article is the result of a research projects number 636–73-07–1390 (3008) with ethical code IR.SKUMS.REC.1393.9.25 approved by SKUMS. Thereby, the authors thank to SKUMS and Modeling in Health Research Center to support this study as well as the Health Deputy at SKUMS, especially Dr. Fadaie and Mr. Nasseri and his colleagues in cancer pathology laboratories.
REFERENCES
- 1.Asmarian N, Kavousi A, Salehi M, Mahaki B. Mapping of stomach cancer rate in Iran using area-to-area Poisson Kriging. J Health Syst Res. 2012;8:681–7. [Google Scholar]
- 2.Ahmadi A, Soori H, Sajjadi H. Modeling of in hospital mortality determinants in myocardial infarction patients, with and without type 2 diabetes, undergoing pharmaco-invasive strategy: The first national report using two approaches in Iran. Diabetes Res Clin Pract. 2015;108:216–22. doi: 10.1016/j.diabres.2015.02.018. [DOI] [PubMed] [Google Scholar]
- 3.Zeinalian M, Eshaghi M, Sharbafchi MR, Naji H, Marandi SM, Asgary S, et al. A comparative study on cancer prevention principles between Iranian traditional medicine and classic medicine. Int J Prev Med. 2016;7:61. doi: 10.4103/2008-7802.179508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Abdifard E, Ghaderi S, Hosseini S, Heidari M. Incidence trends of colorectal cancer in the West of Iran during 2000-2005. Asian Pac J Cancer Prev. 2013;14:1807–11. doi: 10.7314/apjcp.2013.14.3.1807. [DOI] [PubMed] [Google Scholar]
- 5.Rohani Rasaf M, Rohani Rasaf M, Rahimi F, Mehrazma M, Golmohammadi A, Motiedoost R, et al. Distribution of cancer incidence in districts and neighbourhoods of a number of Tehran districts in 1386. Razi J Med Sci. 2011;18:34–45. [Google Scholar]
- 6.Forman D, Bray F, Brewster DH, Mbalawa CG, Kohler B, Piñeros M, et al. Cancer Incidence in Five Continents. [Last accessed on 2016 Dec 20];2014 10 Available from: http://www.iarc.fr/en/publications/pdfs-online/epi/sp164/CI5volX_Full.pdf . [Google Scholar]
- 7.Darabi M, Asadi Lari M, Motevalian SA, Motlagh A, Arsang-Jang S, Karimi Jaberi M, et al. Trends in gastrointestinal cancer incidence in Iran, 2001-2010: A joinpoint analysis. Epidemiol Health. 2016;38:e2016056. doi: 10.4178/epih.e2016056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ahmadi A, Salehi F. Evaluation of observed and the expected incidence of common cancers: An experience from Southwestern of Iran, 2010-2014. J Res Med Sci. 2018;23:4. doi: 10.4103/jrms.JRMS_788_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Program JR. Bethesda, MD: National Cancer Institute; 2013. Statistical Methodology and Applications Branch, Surveillance Research Program. [Google Scholar]
- 10.Rafiemanesh H, Maleki F, Mohammadian-Hafshejani A, Salemi M, Salehiniya H. The trend in histological changes and the incidence of esophagus cancer in Iran (2003-2008) Int J Prev Med. 2016;7:31. doi: 10.4103/2008-7802.175990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19:335–51. doi: 10.1002/(sici)1097-0258(20000215)19:3<335::aid-sim336>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 12.Kim HJ, Fay MP, Yu B, Barrett MJ, Feuer EJ. Comparability of segmented line regression models. Biometrics. 2004;60:1005–14. doi: 10.1111/j.0006-341X.2004.00256.x. [DOI] [PubMed] [Google Scholar]
- 13.National Cancer Demography Program. 2018. [Last accessed on 2018 Jun 28]. Available from: http://www.irancanreg.ir/
- 14.Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. doi: 10.3322/caac.21262. [DOI] [PubMed] [Google Scholar]
- 15.Qi D, Wu C, Liu F, Gu K, Shi Z, Lin X, et al. Trends of prostate cancer incidence and mortality in Shanghai, China from 1973 to 2009. Prostate. 2015;75:1662–8. doi: 10.1002/pros.23046. [DOI] [PubMed] [Google Scholar]
- 16.Bernal M, Gómez FJ, Gómez G. Trends in cancer mortality in Spain: 1975-2004. Tumori. 2009;95:669–74. doi: 10.1177/030089160909500605. [DOI] [PubMed] [Google Scholar]
- 17.Rafiemanesh H, Rajaei-Behbahani N, Khani Y, Hosseini S, Pournamdar Z, Mohammadian-Hafshejani A, et al. Incidence trend and epidemiology of common cancers in the center of Iran. Glob J Health Sci. 2015;8:146–55. doi: 10.5539/gjhs.v8n3p146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Haidari M, Nikbakht MR, Pasdar Y, Najaf F. Trend analysis of gastric cancer incidence in Iran and its six geographical areas during 2000-2005. Asian Pac J Cancer Prev. 2012;13:3335–41. doi: 10.7314/apjcp.2012.13.7.3335. [DOI] [PubMed] [Google Scholar]
- 19.Vakili M, Pirdehghan A, Adimi M, Sadeghian M, Akhondi M. Epidemiology and trend of cancer in Yazd, a central province of Iran, 2005-2009. J Res Health Sci. 2014;14:210–3. [PubMed] [Google Scholar]
- 20.Emami MH, Ataie-Khorasgani M, Jafari-Pozve N. Diagnostic value of alarm symptoms for upper GI malignancy in patients referred to GI clinic: A 7 years cross sectional study. J Res Med Sci. 2017;22:76. doi: 10.4103/jrms.JRMS_450_15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mousavi SM, Somi MH. Gastric cancer in Iran 1966-2006. Asian Pac J Cancer Prev. 2009;10:407–12. [PubMed] [Google Scholar]
- 22.Mirzaei H, Salehi H, Sahebkar A, Avan A, Jaafari MR, Namdar A, et al. Deciphering biological characteristics of tumorigenic subpopulations in human colorectal cancer reveals cellular plasticity. J Res Med Sci. 2016;21:64. doi: 10.4103/1735-1995.187355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sharifian A, Pourhoseingholi MA, Norouzinia M, Vahedi M. Ovarian cancer in Iranian women, a trend analysis of mortality and incidence. Asian Pac J Cancer Prev. 2014;15:10787–90. doi: 10.7314/apjcp.2014.15.24.10787. [DOI] [PubMed] [Google Scholar]
- 24.Akbari M, Khayamzadeh M. 1st ed. Tehran: Cancer Research Center, Shahid Beheshti University of Medical Sciences; 2008. Incidence, mortality and burden of cancers in Iran. Iran Cancer Report; pp. 95–125. [Google Scholar]
- 25.Arab M, Khayamzadeh M, Tehranian A, Tabatabaeefar M, Hosseini M, Anbiaee R, et al. Incidence rate of ovarian cancer in Iran in comparison with developed countries. Indian J Cancer. 2010;47:322–7. doi: 10.4103/0019-509X.64721. [DOI] [PubMed] [Google Scholar]
- 26.Safavi A, Azizi F, Jafari R, Chaibakhsh S, Safavi AA. Thyroid cancer epidemiology in Iran: A time trend study. Asian Pac J Cancer Prev. 2016;17:407–12. doi: 10.7314/apjcp.2016.17.1.407. [DOI] [PubMed] [Google Scholar]
- 27.Davies L, Welch HG. Thyroid cancer survival in the United States: Observational data from 1973 to 2005. Arch Otolaryngol Head Neck Surg. 2010;136:440–4. doi: 10.1001/archoto.2010.55. [DOI] [PubMed] [Google Scholar]
- 28.Asadzadeh Vostakolaei F, Broeders MJ, Mousavi SM, Kiemeney LA, Verbeek AL. The effect of demographic and lifestyle changes on the burden of breast cancer in Iranian women: A projection to 2030. Breast. 2013;22:277–81. doi: 10.1016/j.breast.2012.07.002. [DOI] [PubMed] [Google Scholar]
- 29.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D, et al. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 30.Mousavi SM, Gouya MM, Ramazani R, Davanlou M, Hajsadeghi N, Seddighi Z, et al. Cancer incidence and mortality in Iran. Ann Oncol. 2009;20:556–63. doi: 10.1093/annonc/mdn642. [DOI] [PubMed] [Google Scholar]
- 31.Koohi F, Salehiniya H. The trend of incidence of bladder cancer in Iran, 2003-2009. J Urmia Univ Med Sci. 2015;26:1–9. [Google Scholar]
- 32.Eatemed K, Gooya M, Ramazani R. Iranian Annual National Cancer Registration Report. Ministry of Health and Medical Education. Center for Disease Control and Prevention. 2008 [Google Scholar]
- 33.Keyghobadi N, Rafiemanesh H, Mohammadian-Hafshejani A, Enayatrad M, Salehiniya H. Epidemiology and trend of cancers in the province of Kerman: Southeast of Iran. Asian Pac J Cancer Prev. 2015;16:1409–13. doi: 10.7314/apjcp.2015.16.4.1409. [DOI] [PubMed] [Google Scholar]
- 34.Jackson R. An early selective medline: Henry Stelwagon's 1916 textbook of dermatology. J Cutan Med Surg. 2007;11:191–4. doi: 10.2310/7750.2007.00020. [DOI] [PubMed] [Google Scholar]
- 35.Parkin DM. International variation. Oncogene. 2004;23:6329–40. doi: 10.1038/sj.onc.1207726. [DOI] [PubMed] [Google Scholar]
- 36.Hasanpour Z, Nasri H, Rafieian-Kopaei M, Ahmadi A, Baradaran A, Nasri P, et al. Paradoxical effects of atorvastatin on renal tubular cells: An experimental investigation. Iran J Kidney Dis. 2015;9:215–20. [PubMed] [Google Scholar]