

Abstract
Pulpal necrosis in permanent teeth that have not completed their root development leads to teeth with a very short root, roots with very thin walls, and an inadequate crown-root ratio, which overshadows their survival prognosis. Currently, there are various therapies to treat immature permanent teeth with pulpal pathology such as the case of apexification. An electronic search was performed in the PubMed database (www.ncbi.nlm.nih.gov), Scopus (www.scopus.com), Cochrane (www.cochrane.org) to identify the clinical investigations related to evolution of the cases. The search of the literature of clinical studies on permanent teeth with open apex that present pulpar pathology and that need treatment, have been found 11 clinical studies of treatments with apexification. The apexification by calcium hydroxide has been applied for many years back to the present as a valid therapy to perform the treatment of apexification.
Keywords: Apexification, endodontic treatment, immature permanent teeth, pulp regeneration, revascularization
INTRODUCTION
Pulpal involvement as a consequence of trauma or caries in immature permanent teeth can trigger the loss of pulpal vitality as well as directly affect root development, resulting in short roots with very thin walls producing a greater risk of fracture and thus hindering the treatment conventional ducts.[1,2]
The treatment to be carried out against these pulpal pathologies is the elimination of the pulp tissue, the disinfection of the root canal system through the different irrigants that we have at present, among the most used are sodium hypochlorite and ethylenediaminetetraacetic acid. Among the possible treatments to perform in a permanent tooth with short roots that need endodontic therapy, we have the apexification that is a procedure of induction of a calcified apical barrier in the apical zone of an incompletely formed root, in which the pulp is diagnosed as necrotic.[3] The apexification may involve one or multiple monthly appointments to place calcium hydroxide (Ca(OH)2) inside the root canal and achieve the elimination of the intracanal infection, which stimulates calcification and produces the apical closure. After several monthly appointments, radiologically, the walls of the root canal of the tooth should show more thickness and a rounded apex, which allows the root canals to be sealed with conventional techniques using gutta-percha and a sealant.[2] Ca(OH)2 can alter the mechanical properties of dentin and make these teeth more susceptible to root fracture.[4,5] The traditional use of Ca(OH)2 to achieve apexification is being gradually replaced by mineral trioxide aggregate (MTA) as a one-step technique.[6,7] The MTA can be placed as an apical plug with previous applications intracanal with Ca(OH)2 to produce the disinfection of the same[8] or even the MTA can be used as a material of canal filling.[9]
METHODOLOGY OF PUBLICATION SEARCH
An electronic search was performed in the PubMed databases (www.ncbi.nlm.nih.gov), Scopus (www.scopus.com), Cochrane (www.cochrane.org) to identify the investigations of reported clinical cases related to the evaluation of apexification and revascularization in immature permanent teeth. The terms “apexification” and “immature permanent teeth” and “treatment” were used. The research was limited to publications written in English. An additional manual electronic search was carried out in the leading endodontics and pediatric dentistry journals: Dental Traumatology; International Journal of Pediatric Dentistry; Journal of Clinical Pediatric Dentistry; Pediatric Dentistry; Journal of Endodontics; International Endodontic Journal; The Journal of the American Dental Association; European Journal of Oral Sciences; and Australian Endodontic Journal. The keywords “Apexification” and “Pulp regeneration” and “Revascularization” and “Immature Permanent teeth” were used. The search included articles from the start date of each source until February 28, 2018. After the removal of the duplicate articles, the revision of the title and the selection of abstracts, full-text articles were used to verify that the content of the article was relevant [Figure 1].
Figure 1.
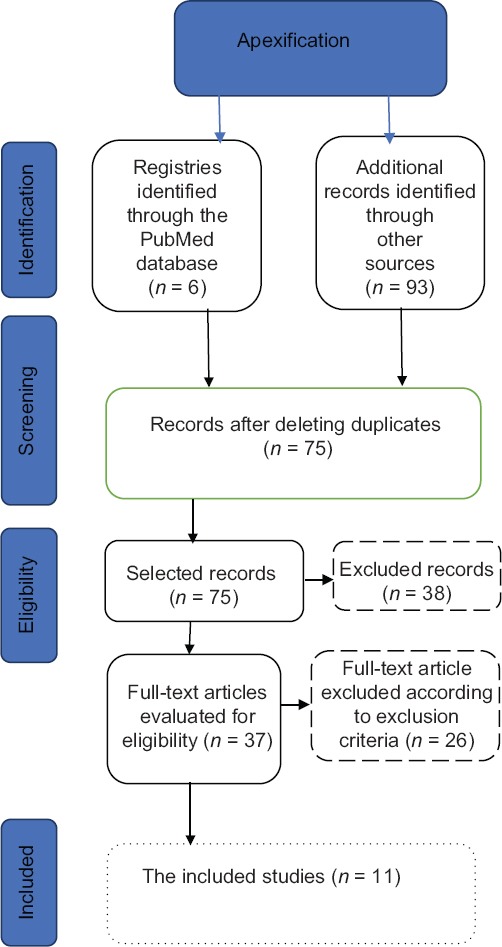
A flow diagram of records
RESULTS
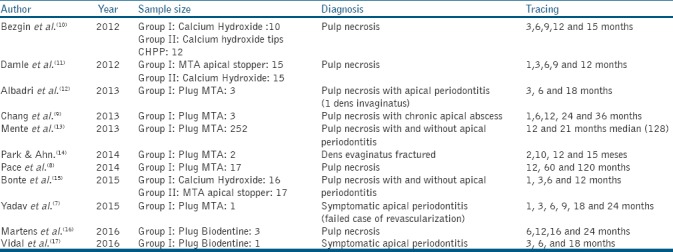
In the results of the literature search referring to clinical studies of permanent teeth with open apex treated with apico formation, 11 clinical articles have been found either using the Ca(OH)2 technique or the apical barrier technique. Among the variables are the year of publication, the size of the sample studied in each article, the diagnosis of the tooth treated with apexification, and the time of follow-up of the patients [Table 1].
Table 1.
Representation of the results of clinical studies of apexification.
DISCUSSION
Apexification
Bezgin et al.[10] carried out a study this right (Roeko, Langenau, Germany) designed to release said drug from a gutta-percha matrix as an alternative to Ca(OH)2 paste for use as intraconducting medication. Within the limitations of the study, CHPP provides acceptable results in the treatment of apexification and can be used successfully in cases where apexification with Ca(OH)2 is indicated. However, there is only one study analyzed by Oktem et al.[11] in which CHPP tips were used on a tooth with a follow-up time of 24 months in which the apex closure of the treated tooth was obtained. Due to this, the two authors cited above Bezgin et al.[10] and Oktem et al.[11] report that clinical studies are needed with a larger sample size and a longer follow-up time.
Apexification with MTA several clinical studies[8,12,13,14,15] report that MTA provides a viable alternative to achieve root closure in immature teeth or root fracture, even in cases with an open apex. The time required for the formation of the barrier is significantly less in teeth treated with MTA compared to teeth treated with Ca(OH)2. There is currently a study conducted by Mente et al.[16] in which it presents the largest sample number treated with apexification (252 samples) and with a 10-year follow-up period, which concludes that the success rates of teeth with open apices reported in this cohort study suggest that the placement of apical plugs with MTA is an appropriate treatment option for teeth with an open apex. The presence of preoperative apical periodontitis was identified as the most important prognostic factor, success rates remain constantly high, even after follow-up periods of more than 4 years.
Chan et al.[9] studied whether MTA favors apexification and periapical scarring even when a considerable amount of this material has been inadvertently extruded. Although it is recognized that the extrusion of MTA through an open apex is not a common mishap during the apexification procedure, the extruded material does not adversely affect the healing of the periapical tissues, as verified in the present study with clinical observations and X-rays with a follow-up of cases of 36–54 months; Nosrat et al.[17] analyzed whether after the extrusion of MTA in periradicular tissues, bone healing, and reabsorption of MTA may occur or may remain unactivated, and affect the healing process. Physical irritation of the oral mucosa after the extrusion of MTA is another possibility when the endodontic material is sandwiched between the bone and the mucosa, so that the result of the treatment after the extrusion of MTA in the periradicular tissues can not be limited and therefore it is unpredictable.
Among the current studies using MTA to perform apex barrier apposition, we have the study by Yadav et al.,[7] who analyzed the apexification in one visit by placing a platelet-rich fibrin apical plug (PRF) and MTA, in which PRF was used as an apical matrix and subsequent placement of the MTA since the fibrin rich in platelets have several advantages, including ease of preparation and lack of biochemical manipulation of the blood, which makes this preparation strictly autologous. PRF is also associated with slow and continuous increase in cytokine levels. Leukocytes in the PRF act as anti-inflammatory, an anti-infective agent, the regulator of the immune response, and provide the vascular endothelial growth factor to promote angiogenesis. An apical plug of MTA in the last 5 mm of the canal is used in the present case since it avoids the risk of fracture during apexification traditional Ca(OH)2,[18,19,20] which allows this new protocol with PRF and MTA is a predictable and reproducible clinical procedure.
There is an evolution in the endodontic materials to perform apexification through an apical barrier, and among them, we have the repair cement biodentine which is presenting favorable clinical and radiographic results, which can be an effective alternative when performing an apicoformation.[21,22]
CONCLUSIONS
The apexification by Ca(OH)2 has been applied for many years back to the present as a valid therapy to perform an apexification treatment.
The MTA barrier as a treatment of apexification is a technique that is applied as a substitution to Ca(OH)2 apexification; this technique does not require several appointments, and the conformation of the barrier does not need an external factor to develop, as in the case of the apexification with Ca(OH)2, as well as in the regeneration of the pulp.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Lauridsen E, Hermann NV, Gerds TA, Kreiborg S, Andreasen JO. Pattern of traumatic dental injuries in the permanent dentition among children, adolescents, and adults. Dent Traumatol. 2012;28:358–63. doi: 10.1111/j.1600-9657.2012.01133.x. [DOI] [PubMed] [Google Scholar]
- 2.Shabahang S. Treatment options: Apexogenesis and apexification. Pediatr Dent. 2013;35:125–8. [PubMed] [Google Scholar]
- 3.Nicoloso GF, Pötter IG, Rocha RO, Montagner F, Casagrande L. A comparative evaluation of endodontic treatments for immature necrotic permanent teeth based on clinical and radiographic outcomes: A systematic review and meta-analysis. Int J Paediatr Dent. 2017;27:217–27. doi: 10.1111/ipd.12261. [DOI] [PubMed] [Google Scholar]
- 4.Andreasen JO, Farik B, Munksgaard EC. Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. Dent Traumatol. 2002;18:134–7. doi: 10.1034/j.1600-9657.2002.00097.x. [DOI] [PubMed] [Google Scholar]
- 5.Iwaya S, Ikawa M, Kubota M. Revascularization of an immature permanent tooth with periradicular abscess after luxation. Dent Traumatol. 2011;27:55–8. doi: 10.1111/j.1600-9657.2010.00963.x. [DOI] [PubMed] [Google Scholar]
- 6.Purra AR, Ahangar FA, Chadgal S, Farooq R. Mineral trioxide aggregate apexification: A novel approach. J Conserv Dent. 2016;19:377–80. doi: 10.4103/0972-0707.186443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Yadav P, Pruthi PJ, Naval RR, Talwar S, Verma M. Novel use of platelet-rich fibrin matrix and MTA as an apical barrier in the management of a failed revascularization case. Dent Traumatol. 2015;31:328–31. doi: 10.1111/edt.12168. [DOI] [PubMed] [Google Scholar]
- 8.Pace R, Giuliani V, Nieri M, Di Nasso L, Pagavino G. Mineral trioxide aggregate as apical plug in teeth with necrotic pulp and immature apices: A 10-year case series. J Endod. 2014;40:1250–4. doi: 10.1016/j.joen.2013.12.007. [DOI] [PubMed] [Google Scholar]
- 9.Chang SW, Oh TS, Lee W, Cheung GS, Kim HC. Long-term observation of the mineral trioxide aggregate extrusion into the periapical lesion: A case series. Int J Oral Sci. 2013;5:54–7. doi: 10.1038/ijos.2013.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bezgin T, Sönmez H, Orhan K, Ozalp N. Comparative evaluation of Ca(OH)2 plus points and Ca(OH)2 paste in apexification. Dent Traumatol. 2012;28:488–95. doi: 10.1111/j.1600-9657.2011.01110.x. [DOI] [PubMed] [Google Scholar]
- 11.Oktem ZB, Cetinbaş T, Ozer L, Sönmez H. Treatment of aggressive external root resorption with calcium hydroxide medicaments: A case report. Dent Traumatol. 2009;25:527–31. doi: 10.1111/j.1600-9657.2009.00790.x. [DOI] [PubMed] [Google Scholar]
- 12.Albadri S, Chau YS, Jarad F. The use of mineral trioxide aggregate to achieve root end closure: Three case reports. Dent Traumatol. 2013;29:469–73. doi: 10.1111/j.1600-9657.2012.01128.x. [DOI] [PubMed] [Google Scholar]
- 13.Damle SG, Bhattal H, Loomba A. Apexification of anterior teeth: A comparative evaluation of mineral trioxide aggregate and calcium hydroxide paste. J Clin Pediatr Dent. 2012;36:263–8. [PubMed] [Google Scholar]
- 14.Park M, Ahn BD. Immature permanent teeth with apical periodontitis and abscess treated by regenerative endodontic treatment using calcium hydroxide and MTA: A report of two cases. Pediatr Dent. 2014;36:107–10. [PubMed] [Google Scholar]
- 15.Bonte E, Beslot A, Boukpessi T, Lasfargues JJ. MTA versus ca(OH)2 in apexification of non-vital immature permanent teeth: A randomized clinical trial comparison. Clin Oral Investig. 2015;19:1381–8. doi: 10.1007/s00784-014-1348-5. [DOI] [PubMed] [Google Scholar]
- 16.Mente J, Leo M, Panagidis D, Ohle M, Schneider S, Lorenzo Bermejo J, et al. Treatment outcome of mineral trioxide aggregate in open apex teeth. J Endod. 2013;39:20–6. doi: 10.1016/j.joen.2012.10.007. [DOI] [PubMed] [Google Scholar]
- 17.Nosrat A, Nekoofar MH, Bolhari B, Dummer PM. Unintentional extrusion of mineral trioxide aggregate: A report of three cases. Int Endod J. 2012;45:1165–76. doi: 10.1111/j.1365-2591.2012.02082.x. [DOI] [PubMed] [Google Scholar]
- 18.Chen X, Bao ZF, Liu Y, Liu M, Jin XQ, Xu XB, et al. Regenerative endodontic treatment of an immature permanent tooth at an early stage of root development: A case report. J Endod. 2013;39:719–22. doi: 10.1016/j.joen.2012.12.023. [DOI] [PubMed] [Google Scholar]
- 19.McTigue DJ, Subramanian K, Kumar A. Case series: Management of immature permanent teeth with pulpal necrosis: A case series. Pediatr Dent. 2013;35:55–60. [PubMed] [Google Scholar]
- 20.Valera MC, Albuquerque MT, Yamasaki MC, Vassallo FN, da Silva DA, Nagata JY, et al. Fracture resistance of weakened bovine teeth after long-term use of calcium hydroxide. Dent Traumatol. 2015;31:385–9. doi: 10.1111/edt.12185. [DOI] [PubMed] [Google Scholar]
- 21.Vidal K, Martin G, Lozano O, Salas M, Trigueros J, Aguilar G, et al. Apical closure in apexification: A review and case report of apexification treatment of an immature permanent tooth with biodentine. J Endod. 2016;42:730–4. doi: 10.1016/j.joen.2016.02.007. [DOI] [PubMed] [Google Scholar]
- 22.Martens L, Rajasekharan S, Cauwels R. Endodontic treatment of trauma-induced necrotic immature teeth using a tricalcium silicate-based bioactive cement. A report of 3 cases with 24-month follow-up. Eur J Paediatr Dent. 2016;17:24–8. [PubMed] [Google Scholar]