

Abstract
A 101 years-old woman was admitted to our Emergency Department (ED) for acute dyspnea which onset nearly two hours before presentation. She had been on hydrochlorothyazyde-amiloride therapy due to mild hypertension. No other relevant features were present in the clinical history. The old lady had never been admitted to the hospital, and she was still living alone. A few days before hospital admission, one of the daughters became ill, so that a caregiver was paid for assisting her 12/24. This new circumstance was reluctantly accepted by the old lady. At ED presentation the patient was dyspnoic but alert. The electrocardiogram showed a marked elevation of the ST segment in V2-V6 leads. The echocardiogram showed the typical apical ballooning, characteristic of takotsubo cardiomyopathy. Blood test only showed a significant increase of cardiac troponin I. Considering the very good conditions of the patient, a coronary angiography was performed, that demonstrated a coronary tree totally free of lesions, thus confirming the clinical suspicion of takotsubo syndrome. The patient was admitted to the Coronary Care Unit, where she had a very good clinical course, and was discharged on day 6th after presentation. After one month of follow-up the clinical course was uneventful and the lady remained in good clinical and lifestyle conditions as before presenting to the ED. This unique case attests that takotsubo cardiomyopathy can be also observed at extreme ages, and should hence be considered in the differential diagnosis of acute dyspnea and chest pain in oldest old patients. (www.actabiomedica.it)
Keywords: takotsubo, stress cardiomyopathy, apical ballooning syndrome, broken heart, myocardial infarction, emergency department
Introduction
The concept of “broken heart” has for long been considered a metaphorical or psychological rather than a clinical condition. The first description of a myocardial infarction-like syndrome occurring in a 44-year-old woman with a normal coronary tree, who had been informed a few hours before symptoms’ onset that her 17-year-old son had committed suicide, paved the way to broadly accepting the concept of stress cardiomyopathy (1). Some years afterwards, in 1990, Japanese scientists firstly suspected the existence of a distinct new syndrome, and they used for the very first time in Medicine the term tako-tsubo (in Japanese: octopus pot). This was due to the fact that the shape of affected left ventricle, showing a characteristic ballooning of the apex, resembled a traditional Japanese fisherman’s pot used for trapping octopuses and characterized by a wide round bottom and a narrow neck (Fig. 1) (2, 3). Despite up to 75 different descriptive names have been used so far, the term “takotsubo” is now acquiring a definite role (4).
Figure 1.

Image of a Japanese octopus pot (tako-tsubo)
After initial description, the syndrome has been increasingly diagnosed. However, it was only after the widespread use of primary percutaneous coronary intervention (pPCI) for treatment of acute myocardial infarction that takotsubo syndrome was found to be more common than previously thought (5). In acute phase, the clinical presentation, electrocardiographic findings and profile of cardiac biomarkers are often similar to those of an acute coronary syndrome (ACS), but the coronary angiography typically fails to show signs of obstructed coronary vessels. Therefore, some authors proposed that takotsubo should be simply considered as a novel form of ACS (6). After up to three decades of studies, the current knowledge about the pathophysiology of this syndrome remains limited, although the role of the brain-heart axis has been clearly described in the pathogenesis of the disease (7, 8). This condition predominantly affects elderly women and is often anticipated by emotional or physical triggers, even if in some cases a specific trigger cannot be identified (9). In the largest studies that have been published so far, most patients were women (i.e., 8090% of the whole population of takotsubo patients), the majority of whom in post-menopausal age (9, 1012). Nevertheless, even in the largest series ever published (9), no cases over the age of 95 years have been described to the best of our knowledge. As such, aim of this article is to describe a rare and paradigmatic case of takotsubo cardiomyopathy in a 101-year old woman with normal coronary vessels’ tree.
Case report
A 101 years and 7 months-old woman was admitted to our Emergency Department (ED) at 1 P.M. for acute dyspnea which onset nearly two hours before presentation. She had been on hydrochlorothyazydeamiloride therapy for about 15 years due to mild hypertension. No other relevant features were present in the clinical history. The old lady had never been admitted to the hospital, and she was still living alone. Her two daughters helped every other day in housekeeping, personal hygiene and grocery shopping. She had always refused to go to live with the daughters. A few days before hospital admission, one of the two daughters became ill, so that a caregiver was paid for assisting the old lady 12/24. This new circumstance was reluctantly accepted by the old lady. Early in the morning of the day before ED admission, the caregiver did something wrong during housekeeping, which angered the old lady.
At ED presentation the patient was dyspnoic but alert and mentally coherent. The vital parameters on admission were as follows: blood pressure (BP) 110/70 mmHg; heart rate (HR) 70 beats per minute; respiratory rate (RR) 26 breaths per minute; peripheral oxygen saturation (spO2) 89% in room air; temperature (T°) 36.7°C. The electrocardiogram showed a marked elevation of the ST segment in V2-V6 leads (Fig. 2). The patient was given oxygen, acetylsalicylic acid, and furosemide. Soon afterwards, an echocardiogram was performed, showing the typical apical ballooning, which is characteristic of takotsubo syndrome (Fig. 3). Blood test were all within the normal reference range, except for slight hyperglycaemia (179 mg/dL) and a significant increase of cardiac troponin I (0.65 ng/mL; normal value <0.05 ng/mL). A cardiologist was hence consulted and, considering the very good conditions of the patient, a coronary angiography was performed after discussion with the two daughters. The angiography showed a coronary tree totally free of lesions (Fig. 4), thus confirming the clinical suspicion of takotsubo cardiomyopathy. In consideration of the good quality of the echocardiographic images, and of the risk of further administration of contrast medium in such an advanced age, a ventriculography was not obtained. The patient was then admitted to the Coronary Care Unit (CCU), where she had a very good clinical course, despite a further large increase of cardiac troponin I values was still observed, peaking at 17.2 ng/mL at the third day of hospitalization. The patient was then discharged on day 6th after initial presentation to the ED. After one month of follow-up the clinical course was uneventful and the lady remained in good clinical and lifestyle conditions as before presenting to the ED.
Figure 2.
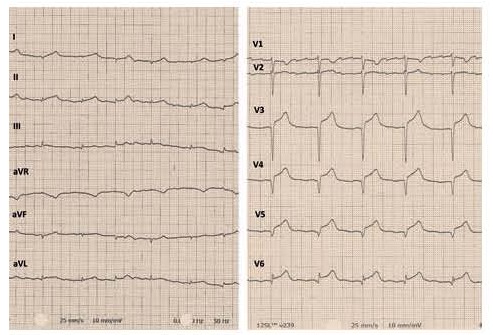
Electrocardiogram recorded at the presentation in the ED, showing a typical pattern of acute myocardial infarction with elevation of the ST segment (STEMI)
Figure 3.
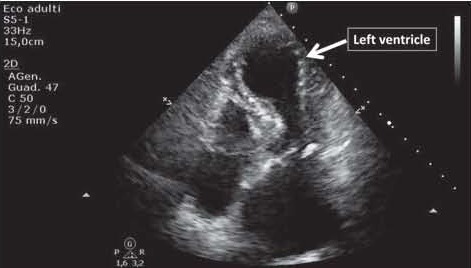
Echocardiogram recorded while in the ED, showing the typical apical ballooning, or takotsubo-like shape, of the left ventricle
Figure 4.
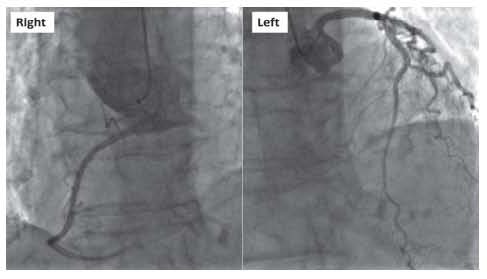
Coronary angiography, showing a normal coronary tree, with a right dominance
Discussion
Takotsubo, or apical ballooning cardiomyopathy, currently represents a widely recognized clinical condition, which challenges clinicians with some diagnostic pitfalls (i.e., the differential diagnosis with acute myocardial infarction).
The prognostic implications of a correct diagnosis need to be clearly acknowledged, since takotsubo cardiomyopathy generally has an excellent prognosis, characterized by almost complete recovery in the vast majority of patients (up to 96%), and a low recurrence rate (13). In-hospital mortality ranged between 3-5% in different studies (9, 14). The highest risk seemingly occurs within the first 48 hours, whereas long term survival rate is usually similar to age- and gendermatched controls (13).
Interestingly, in a relatively small cohort study a significantly increased rate of cancers has been observed in patients with takotsubo cardiomyopathy compared to those who suffered from acute myocardial infarction (15), and this evidence paved the way to speculate that paraneoplastic phenomena may be the ‘missing link’ in the pathogenesis of takotsubo cardiomyopathy.
Albeit it is universally acknowledged that this condition mostly affect postmenopausal women, no cases aged 95 years or older have been described so far. Our unique case report, confirmed by satisfying all four Mayo Clinic criteria (16), attests that takotsubo cardiomyopathy can be also observed at extreme ages, and should hence be considered in the differential diagnosis of acute dyspnea and chest pain in oldest old patients other than in the middle aged population.
References
- 1.Ryan TJ, Fallon JT. Case 18-1986 – A 44-Year-Old Woman with Substernal Pain and Pulmonary Edema after Severe Emotional Stress. N Engl J Med. 1986;314:1240–7. doi: 10.1056/NEJM198605083141908. [DOI] [PubMed] [Google Scholar]
- 2.Sato H, Dote K, Uchida T, Ishihara M. Tako-tsubo-like left ventricular dysfunction due to multivessel coronary spasm. Clinical Aspect of Myodardial Injury: From Ischemia to Heart Failure. In: Kodama K. H., K., Hori M., editors. Tokyo: Kagakuhyoronsha Publishing Co.; 1990. pp. 56–64. [Google Scholar]
- 3.Kurisu S, Sato H, Kawagoe T, et al. Tako-tsubo-like left ventricular dysfunction with ST-segment elevation: a novel cardiac syndrome mimicking acute myocardial infarction. Am Heart J. 2002;143:448–55. doi: 10.1067/mhj.2002.120403. [DOI] [PubMed] [Google Scholar]
- 4.Sharkey SW, Lesser JR, Maron MS, Maron BJ. Why not just call I tako-tsubo cardiomyopathy? A discussion of nomenclature. J Amer Coll Cardiol. 2011;57:1496–7. doi: 10.1016/j.jacc.2010.11.029. [DOI] [PubMed] [Google Scholar]
- 5.Desmet WJ, Adriaenssens BF, Dens JA. Apical ballooning of the left ventricle: first series in white patients. Heart. 2003;89:1027–31. doi: 10.1136/heart.89.9.1027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lüscher TF, Templin C. Is takotsubo syndrome a microvascular acute coronary syndrome? Towards a new definition. Europ Heart J. 2016;37:2816–20. doi: 10.1093/eurheartj/ehw057. [DOI] [PubMed] [Google Scholar]
- 7.Samuels MA. The brain-heart connection. Circulation. 2007;116:77–84. doi: 10.1161/CIRCULATIONAHA.106.678995. [DOI] [PubMed] [Google Scholar]
- 8.Suzuki H, Matsumoto Y, Kaneta T, et al. Evidence for brain activation in patients with takotsubo cardiomyopathy. Circ J. 2014;78:256–8. doi: 10.1253/circj.cj-13-1276. [DOI] [PubMed] [Google Scholar]
- 9.Templin C, Ghadri JR, Diekmann J, et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N Engl J Med. 2015;373:929–38. doi: 10.1056/NEJMoa1406761. [DOI] [PubMed] [Google Scholar]
- 10.Gil IJN, André M, Delia MA, Sionis A, Martìn A, Bastante T, Còrdoba Soriano JG, et al. Characterization of Tako-tsubo Cardiomyopathy in Spain: Results from the RETAKO National Registry. Rev Esp Cardiol. 2015;68:505–12. doi: 10.1016/j.rec.2014.07.026. [DOI] [PubMed] [Google Scholar]
- 11.Donohue D, Movahed MR. Clinical characteristics, demographics and prognosis of transient left ventricular apical ballooning syndrome. Heart Fail Rev. 2005;10:311–6. doi: 10.1007/s10741-005-8555-8. [DOI] [PubMed] [Google Scholar]
- 12.Previtali M, Repetto A, Panigada S, et al. Left ventricular apical ballooning syndrome: prevalence, clinical characteristics and pathogenetic mechanisms in a European population. Int J Cardiol. 2009;134:91–6. doi: 10.1016/j.ijcard.2008.01.037. [DOI] [PubMed] [Google Scholar]
- 13.Elesber AA, Prasad A, Lennon RJ, et al. Four-year recurrence rate and prognosis of the apical ballooning syndrome. J Am Coll Cardiol. 2007;50:448–52. doi: 10.1016/j.jacc.2007.03.050. [DOI] [PubMed] [Google Scholar]
- 14.Sharkey SW, Windenburg DC, Lesser JR, et al. Natural history and expansive clinical profile of stress (Tako-Tsubo) Cardiomyopathy. J Am Coll Cardiol. 2010;55:333–41. doi: 10.1016/j.jacc.2009.08.057. [DOI] [PubMed] [Google Scholar]
- 15.Burgdorf C, Kurowski V, Bonnemeier H, et al. Long-term prognosis of the transient left ventricular dysfunction syndrome (Tako-Tsubo cardiomyopathy): focus on malignancies. Eur J Heart Fail. 2008;10:1015–19. doi: 10.1016/j.ejheart.2008.07.008. [DOI] [PubMed] [Google Scholar]
- 16.Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J. 2008;155:408–17. doi: 10.1016/j.ahj.2007.11.008. [DOI] [PubMed] [Google Scholar]