

Abstract
Context:
Due to increased life expectancy worldwide, women are expected to spend a significant portion of their lives in menopause. Proven prevention strategies against serious risks and tested effective treatments for common symptoms may remain unutilized in our population if these women are not asked about these symptoms.
Aim:
This study aims to assess the prevalence of different menopausal symptoms and their severity according to menopause rating scale (MRS) in women.
Setting and Design:
The present study was a cross-sectional survey, conducted in the outpatient department of gynecology and obstetrics.
Subjects and Methods:
After written and informed consent, 121 women having their last menstrual period at least 1 year ago were included. The menopausal symptoms were assessed using the MRS. The primary outcome measure in this study was the prevalence of menopausal symptoms in these women according to MRS and the severity of these symptoms.
Statistical Analysis Used:
Data were analyzed using the SPSS software program, version 15.0 (IBM, Armonk, New York, USA).
Results:
The most common symptom was mental and physical exhaustion which was reported by 88 (72%) women, followed by joint and muscular discomfort which was reported by 83 (68.59%). Hot flushes were reported by 54 (44.62%) respondents. Majority of women reported mild-to-moderate symptoms.
Conclusions:
The prevalence of menopausal symptoms is high, and a health policy needs to be generated for the region.
KEYWORDS: Menopausal symptoms, menopause rating scale, severity
INTRODUCTION
Menopause is the cessation of menstrual periods in adult females. The word “Menopause” derived from the Greek “meno” (month) and “pausis” (pause) meaning the cessation of monthly period cycle, literally is the last stage of the reproductive cycle.[1] It represents the total loss of reproductive potential and marks the beginning of old age. It is associated with a physiological transition for the woman which in most instances manifests as unpleasant symptoms and leads her to seek medical care for these symptoms. This transition thus also signals the change in the health needs of the woman. These needs may be minor but bothersome like hot flushes, or, serious but neglected such as cardiovascular risks and risk of fractures. Increase in vaginal dryness, insomnia, lower urinary tract symptoms and emotional lability are also common in this population.[2]
Due to increased life expectancy worldwide, women are expected to spend a significant portion of their lives in this phase of the reproductive cycle. The age of menopause in western countries is 50.8 years and in India is 47.5 years.[3] The age of menopause in rural Sindh, according to a cross-sectional survey was 46.2 ± 6.4 years.[4] The implication of this finding is that the transition associated with menopause starts earlier in our population who might be caught off guard. Proven prevention strategies against serious risks and tested effective treatments for common symptoms may remain unutilized in our population if these women are not asked about these symptoms.[5]
Menopause rating scale (MRS) is a standardized tool to assess the menopausal symptoms. It has been widely used to assess the symptoms of menopause and their severity in populations worldwide.[6] A recent survey from rural Sindh incorporated the use of this scale and established that the prevalence of symptoms was high in the rural region.[7] According to the author's knowledge, no study on the topic using MRS has thus far been conducted in urban setting.
We undertook this study to assess the prevalence of different menopausal symptoms and their severity according to MRS in women.
SUBJECTS AND METHODS
The present study was a cross-sectional survey, conducted in the outpatient department of gynecology and obstetrics. Women aged 45–60 years, who had their last menstrual period at least 1 year ago, were included. Women who had undergone hysterectomy, taking contraceptives, or those with acute illness were excluded. Those satisfying the inclusion criteria were asked to participate in the study.
After obtaining written and informed consent 121 women were recruited using nonprobability consecutive sampling.
In lieu of a Formal Ethics Committee, the principles of the Helsinki Declaration were followed. Data were coded and confidentiality was ensured.
A pro forma was used to collect data. It included three sections: sociodemographic data, reproductive and menstrual characteristics, and menopausal symptoms experienced according to MRS [Figure 1]. The sociodemographic data included the age of the woman, her ethnic background, marital status, educational status, and her predominant lifestyle (i.e., active or sedentary). The reproductive and menstrual characteristics included age of menarche, age at marriage, number of children and whether she is sexually active these days. The menopausal symptoms were assessed using the MRS [Figure 1].
Figure 1.
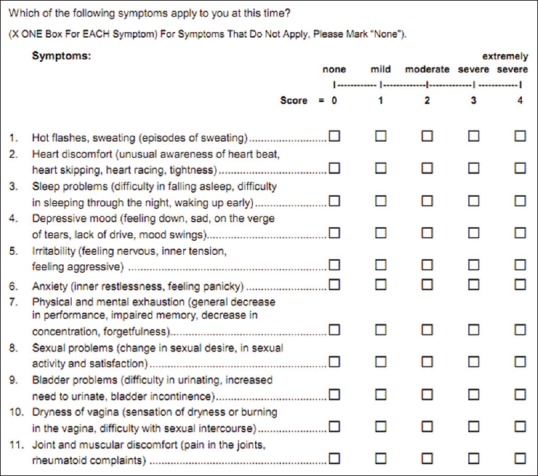
Menopause rating scale
It is a validated questionnaire that consists of 11 items grouped into three categories – somatic, psychological, and urogenital. Each item is a menopausal symptom which is graded on a 5-point Likert scale with a minimum score of 0 and maximum of 4. Each symptom is rated from 0 to 4 as “no symptom,” “mild,” “moderate,” and “severe,” respectively. The MRS is available in many languages; the English version was retrieved and was translated into Urdu for this project. MRS is a formally validated scale according to the requirements for quality of life instruments. After informed consent, the women were enrolled in the study and the questionnaire administered in Urdu. All interviews were performed by the members of the research team and the responses were recorded into the pro forma.
The primary outcome measure in this study was the prevalence of menopausal symptoms in these women according to MRS and the severity of these symptoms.
Data were analyzed using the SPSS software program, version 15.0 (IBM, Armonk, USA).
RESULTS
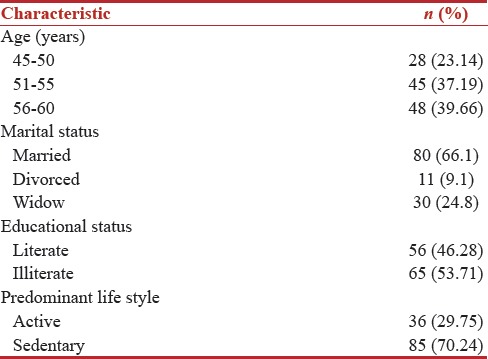
A total of 121 women having their last menstrual period at least 1 year ago were included in this study. The sociodemographic characteristics of the study population are summarized in Table 1. Most women (n = 48, 39.66%) were of ages 56–60 years, were married (n = 80, 66.1%) and illiterate (n = 65, 53.71%) and had a predominantly sedentary lifestyle (n = 85, 70.24%).
Table 1.
Sociodemographic data of the study population
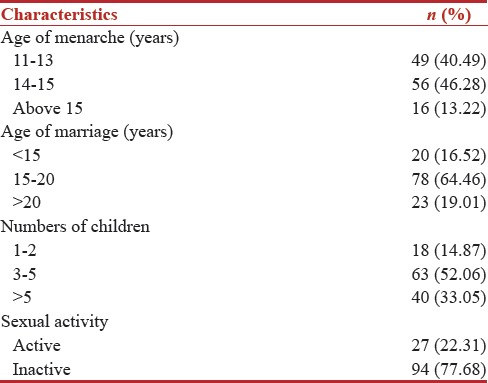
Among those interviewed 56 (46.28%) had menarche at 14–15 years. The age at marriage for most (n = 78, 64.46%) was 15–20 years. Majority of women (n = 94, 77.68%) were sexually inactive. The reproductive and menstrual characteristics are shown in Table 2.
Table 2.
Reproductive and menstrual characteristics
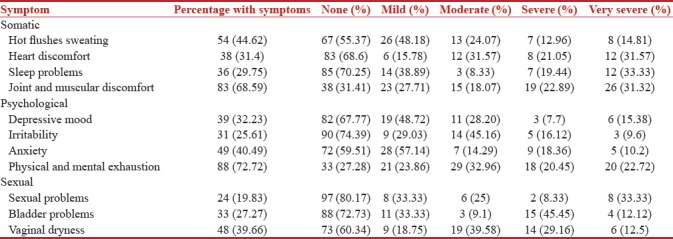
The most common symptom was mental and physical exhaustion which was reported by 88 (72%) women, followed by joint and muscular discomfort which was reported by 83 (68.59%). Hot flushes were reported by 54 (44.62%) of respondents. Majority of women reported mild-to-moderate symptoms [Table 3].
Table 3.
Menopausal symptoms and severity according to menopausal rating scale
When stratified by age, the predominant symptoms experienced by women varied [Figure 2].
Figure 2.
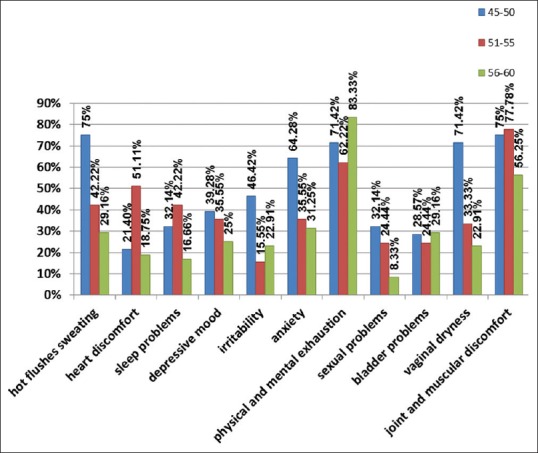
Menopausal symptoms stratified by age
Most women in the age group of 45–50 years had hot flushes (n = 21, 75%) as compared to the other two age groups. In the age group of 51–55 years, joint and muscular discomfort was the predominant symptom (n = 35, 77.78%). Physical and mental exhaustion was the symptom reported by women of age 56–60 years.
The internal consistency coefficient (Cronbach's alpha) of the MRS was calculated to be 0.894.
DISCUSSION
The present study assessed the frequency and severity of menopausal symptoms according to MRS. The prevalence of menopausal symptoms was high, but the severity of these symptoms was mild to moderate. This finding is in agreement with the survey by Nisar et al. where most women reported mild symptoms.[7]
In our study, the most common reported symptoms were mental and physical exhaustion (72%) and joint and muscular discomfort (68.59%). This is in contrast to the studies done in Nepal and Singapore on multicultural ethnicities where a host of symptoms were enumerated.[8,9,10] This may also be due to the use of the standard instrument. The findings were in agreement with a survey in rural Sindh,[6] this may be attributed to the fact that the tertiary care has a huge catchment area and receives patients from interior Sindh as well.
The majority of women in our study had a predominantly sedentary lifestyle. The lifestyle adopted by women of increasing age can also be a reason of this complaint. Furthermore, the nutritional status of the woman affects bone health.[11] Our tertiary care is a public sector hospital frequented by women of low socioeconomic status, and it is usually not possible for these women to afford quality nutrition.
The predominant symptom reported was different in different age groups. The women of age 45–50 years reported hot flushes as the most common symptom. This finding is supported by other studies and is in contrast to the finding reported by Nisar et al.[7] The small sample size of the study may be a reason. The women included in the study were mostly illiterate, and it is quite possible that the educational status of these women affected their reporting of symptoms. Educational status has been shown to affect the perception of menopausal symptoms.[12]
Another interesting finding is the low frequency of vaginal dryness and other urogenital problems. It is considered a societal norm in this part of the world to become less sexually active toward old age.[13] In our study, only 22.2% women were sexually active, and among those only 19.83% reported sexual problems. Vaginal dryness was reported by 39% of women. Of these 39% who reported vaginal dryness most (71.42%) were of age 45–50 years. Thus, our findings are consistent with previous studies.[14,15,16]
Menopause is a period of change and brings just that to a woman's life, change. If she is well prepared, she can cope better and access health-care facilities where she can receive advice on lifestyle modification and supplements that can halt or slow progression of symptoms. This can then allow a smoother transition into old age.
Women should be educated through awareness programs so that they can get proper medical attention. Health professionals should also assess the symptoms with a standard tool. Regular screening of such women can make a huge difference, and their quality of life can be improved.
Our study has a small sample size, and therefore, the results cannot be generalized to all population. Further larger multicenter studies are needed to generate an evidence base for the country.
CONCLUSIONS
The prevalence of menopausal symptoms is high, and a health policy needs to be generated for the region.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.World Health Organization (WHO) Scientific Group. Research on the Menopause in the 1990: Report of a World Health Organization Scientific Group: World Health Organization Geneva. 1996 [PubMed] [Google Scholar]
- 2.Ahsan M, Mallick AK. The effect of soy isoflavones on the menopause rating scale scoring in perimenopausal and postmenopausal women: A Pilot study. J Clin Diagn Res. 2017;11:FC13–6. doi: 10.7860/JCDR/2017/26034.10654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Unni J. Third consensus meeting of Indian menopause society (2008): A summary. J Midlife Health. 2010;1:43–7. doi: 10.4103/0976-7800.66987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nisar N, Sohoo NA, Sikandar R. Age and symptoms at natural menopause: A cross-sectional survey of rural women in Sindh Pakistan. J Ayub Med Coll Abbottabad. 2012;24:90–4. [PubMed] [Google Scholar]
- 5.Malik HS. Knowledge and attitude towards menopause and hormone replacement therapy (HRT) among postmenopausal women. J Pak Med Assoc. 2008;58:164–7. [PubMed] [Google Scholar]
- 6.Heinemann LA, Potthoff P, Schneider HP. International versions of the menopause rating scale (MRS) Health Qual Life Outcomes. 2003;1:28. doi: 10.1186/1477-7525-1-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nisar N, Sikandar R, Sohoo NA. Menopausal symptoms: Prevalence, severity and correlation with sociodemographic and reproductive characteristics. A cross sectional community based survey from rural Sindh Pakistan. J Pak Med Assoc. 2015;65:409–13. [PubMed] [Google Scholar]
- 8.Lim HK, Mackey S. The menopause transition experiences of Chinese Singaporean women: An exploratory qualitative study. J Nurs Res. 2012;20:81–9. doi: 10.1097/jnr.0b013e318254eb25. [DOI] [PubMed] [Google Scholar]
- 9.Loh FH, Khin LW, Saw SM, Lee JJ, Gu K. The age of menopause and the menopause transition in a multiracial population: A nation-wide Singapore study. Maturitas. 2005;52:169–80. doi: 10.1016/j.maturitas.2004.11.004. [DOI] [PubMed] [Google Scholar]
- 10.Gupta S, Acharya K, Srivastav P, Gurung PK, Gupta N. An overview of menopausal symptoms in A district hospital of Nepal. JNMA J Nepal Med Assoc. 2016;55:93–6. [PubMed] [Google Scholar]
- 11.Bendayan R, Kuh D, Cooper R, Muthuri S, Muniz-Terrera G, Adams J, et al. Associations of childhood and adulthood cognition with bone mineral density in later adulthood: A Population-based longitudinal study. Front Aging Neurosci. 2017;9:241. doi: 10.3389/fnagi.2017.00241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tian L, Yang R, Wei L, Liu J, Yang Y, Shao F, et al. Prevalence of osteoporosis and related lifestyle and metabolic factors of postmenopausal women and elderly men: A cross-sectional study in Gansu Province, Northwestern Of China. Medicine (Baltimore) 2017;96:e8294. doi: 10.1097/MD.0000000000008294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Omu AE, al-Qattan N. Effects of hormone replacement therapy on sexuality in postmenopausal women in a Mideast country. J Obstet Gynaecol Res. 1997;23:157–64. doi: 10.1111/j.1447-0756.1997.tb00825.x. [DOI] [PubMed] [Google Scholar]
- 14.Burri A, Hilpert P, Spector T. Longitudinal evaluation of sexual function in a cohort of pre- and postmenopausal women. J Sex Med. 2015;12:1427–35. doi: 10.1111/jsm.12893. [DOI] [PubMed] [Google Scholar]
- 15.Nappi RE, Lachowsky M. Menopause and sexuality: Prevalence of symptoms and impact on quality of life. Maturitas. 2009;63:138–41. doi: 10.1016/j.maturitas.2009.03.021. [DOI] [PubMed] [Google Scholar]
- 16.Kling JM, Manson JE, Naughton MJ, Temkit M, Sullivan SD, Gower EW, et al. Association of sleep disturbance and sexual function in postmenopausal women. Menopause. 2017;24:604–12. doi: 10.1097/GME.0000000000000824. [DOI] [PMC free article] [PubMed] [Google Scholar]