

Abstract
Background:
Tobacco is the significant cause of preventable death worldwide. The prevalence of smoking in India is 13.3%. Among the chemical constituents in the cigarette, nicotine is the one most often associated with dependence resulting in increased consumption of them. Studies have proven the dose-dependent relationship of cigarette smoking with lung and oropharyngeal cancer. Hence, assessment of nicotine dependence among the smokers is essential as it influences the tailor-made intervention.
Objectives:
The objectives of this study were to assess the nicotine dependence and exhaled carbon monoxide (CO) levels among the smokers in Bengaluru.
Materials and Methods:
A cross-sectional survey was conducted among 396 smokers selected using probability proportional to size sampling technique. Fagerstrom Test for Nicotine Dependence was used to assess the levels of nicotine dependence. Exhaled CO levels were measured using the Smokerlyzer to indicate the nicotine dependence.
Results:
About 23.7% of the participants had the very low dependence on nicotine. Nearly 26% and 22.5% of the participants had the high and very high dependence on nicotine correspondingly. The number of years of smoking was found as a significant risk indicator for nicotine dependence. Exhaled CO levels were significantly correlated with the nicotine dependence (P = 0.000) indicating it as a marker for nicotine dependence.
Conclusion:
The high nicotine dependence among the participants warrants effective public health policies to prevent tobacco-related diseases. Considering the risk indicator, the number of years of smoking, smoking cessation programs should target the participants with the habit of continuous smoking with tailor-made interventions to prevent the relapse among them.
Keywords: Carbon monoxide levels, cigarette smokers, Fagerstrom Test Nicotine Dependence, risk indicators
INTRODUCTION
Tobacco Control Policy India Project Report revealed about 275 million tobacco users in India. Tobacco use is responsible for nearly half of all cancers among males and one-quarter of all cancers among females and also for cardiovascular and respiratory diseases. Unless and until urgent action is taken, by 2020, tobacco consumption could cause more than 1.5 million deaths in India annually.[1]
The prevalence of smoking in India is 13.3%.[2] Bidi is the most popular form of smoking tobacco used in India, especially in rural areas, and the cigarette is the second-most popular form of smoking tobacco, mainly used in urban areas.[3]
Although the cigarette smoke has many harmful chemicals such as nicotine, cotinine, tar, hydrogen cyanide, tobacco-specific nitrosamines, carbon monoxide (CO), and polycyclic aromatic hydrocarbons, nicotine is the one most often associated with dependence.
The nicotine in the cigarette is psychoactive and cause neuroadaptation leading to dependence and in turn increased consumption of them.[4] Epidemiological studies have proven the dose-dependent relationship of cigarette and bidi smoking with the occurrence of oropharyngeal and lung cancer.[5]
The ability of a smoker to succeed in quitting smoking depends on the balance between the individual's motivation to quit smoking and his level of dependence on cigarettes. For the smoking cessation programs to be effective, the motivation of the smokers is indispensable. Assessment of nicotine dependence among the smokers is imperative, as it influences the choice of intervention.[6]
The chemicals from the cigarettes smoke are inhaled, absorbed, and distributed to various organ systems ensuring harmful effects. Specific biochemical markers such as nicotine, cotinine, or thiocyanate levels in plasma or urine can be used to assess the smoking habit. The blood tests are invasive and expensive, and neither the blood test nor the urine test provides the immediate assessment. On the other hand, several studies have revealed measurement of exhaled CO levels as the useful and easy tool for assessing the habit of smoking, as it is noninvasive, cheap, the results are immediate and can be used in wide variety of settings.[7,8]
Studies conducted to determine exhaled CO levels among the smokers to indicate nicotine dependence had given conflicting results.[9,10]
Fagerstrom Test for Nicotine Dependence (FTND) is widely used to assess the nicotine dependence among the smokers on different population groups globally.[11] Although studies were conducted to assess the nicotine dependence using FTND among Indian population, previous studies focussed on polydrug users and psychiatric patients.[12,13] Very few studies were done in the field setting to assess nicotine dependence.[14,15] Furthermore, about the internal consistency reliability of the FTND, previous studies had given inconsistent results.[13,14]
Hence, a study with the objective of assessing the internal consistency reliability of the FTND, nicotine dependence using FTND, estimation of risk indicators for nicotine dependence, and measuring exhaled CO levels to indicate nicotine dependence among the smokers in Bengaluru city was conducted.
MATERIALS AND METHODS
The ethical clearance for the present study was obtained from the Institutional Ethics Committee of a Dental College in Bengaluru. This cross-sectional survey was conducted for 4 months (May 2012 to August 2012) among current smokers aged 18 years and above who had smoked at least one cigarette per day for the last 1 year. Participants were enquired about the history of respiratory illness and those with respiratory illness were excluded from the study as the exhaled CO levels would be high in them due to oxidative stress.[16]
The study tools comprised of a questionnaire for sociodemographic details and smoking characteristics and FTND questionnaire to assess the nicotine dependence. The COmpact Smokerlyzer (Bedfont Scientific Ltd., Station Road, Harrietsham, Maidstone, Kent, ME17 1JA, England.), a portable CO monitor was used to measure the exhaled CO levels among the study participants.
A pilot study was conducted among the 30 participants using the convenient sampling technique to check for the feasibility and practicality of study tools and to estimate the sample size for the main study. The proportion of the participants with very low dependence to nicotine obtained from the pilot study was 37.5%. Sample size estimated for 95% confidence level, and 5% precision was 360. Anticipating a nonresponse rate of 10%, the sample size was rounded to 400.
The probability proportional to size sampling technique was used for the selection of study participants. The Bruhat Bengaluru Mahanagara Palike (BBMP) has divided Bengaluru city into eight zones and 198 wards. The total population in each zone was obtained through the BBMP website, and the estimated number of participants was divided proportionately. Simple random sampling technique was used to select the wards.
For selecting the study participants, the central bus depot in the selected wards was chosen as the starting point for uniformity and all the areas in the wards were covered. Participants were selected from the households, tea and coffee shops, and parks. On confirming their residential status, those who met our inclusion and exclusion criteria were briefed about the purpose and procedures of the study. Among those who agreed and gave informed consent were included in the study.
The data were analyzed using Statistical Package for the Social Sciences version 16 (SPSS Inc, Chicago, Illinois, United States).
The variables with significant correlation in the Spearman's test were fitted to binary logistic regression model to estimate the risk indicators for nicotine dependence.
RESULTS
A total of 425 participants were enrolled in the study and 29 participants did not respond. Data were analyzed for 396 participants.
Concerning the internal consistency reliability of the FTND in the study population, the Cronbach's alpha value obtained was 0.64.
In the present study, 23.7%, 15.4%, and 12.4% of the participants had very low, low, and medium dependence to nicotine correspondingly. Nearly 26% and 22.5% of the participants had the high and very high dependence on nicotine correspondingly.
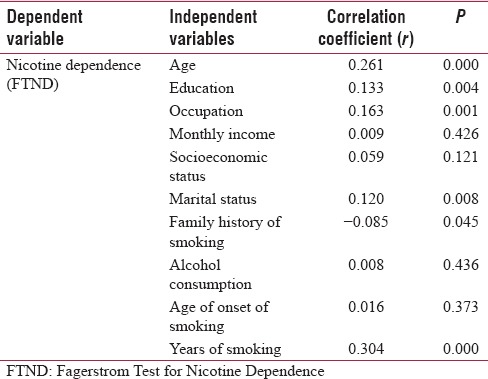
Table 1 represents the correlation between sociodemographic characteristics, smoking characteristics, and nicotine dependence where the variables age, education, occupation, marital status of the study participants, and years of smoking were significantly correlated with the nicotine dependence.
Table 1.
Correlation between the nicotine dependence and sociodemographic and smoking characteristics of the study subjects (Spearman’s Rank Correlation Test)
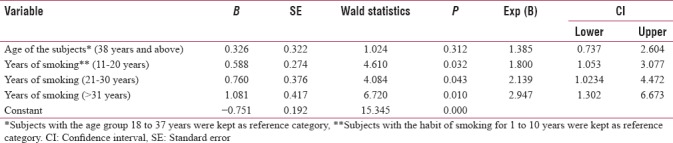
The risk indicator for nicotine dependence through binary logistic regression analysis is presented in Table 2 where the number of years of smoking was found as a significant risk indicator.
Table 2.
Risk indicators for nicotine dependence obtained through the binary logistic regression analysis
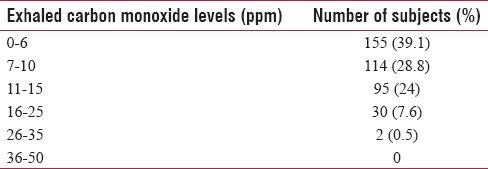
The exhaled CO levels among the study participants are given in Table 3.
Table 3.
Exhaled carbon monoxide levels among the study subjects (n=396)
The correlation between the exhaled CO levels and nicotine dependence was found to be significant (P = 0.000) and (r = 0.374).
DISCUSSION
Nicotine dependence, as a consequence of neuroadaptation by nicotine in the cigarettes, results in increased consumption of them. Studies have proven the dose-dependent relationship of cigarette consumption with oropharyngeal cancer. Therefore, assessment of nicotine dependence among smokers is necessary as it influences the tailor-made intervention.
Hence, the present study was conducted with the objective of assessing the nicotine dependence using FTND and measuring exhaled CO levels among the smokers using the Smokerlyzer.
Concerning the internal consistency reliability of FTND, the Cronbach's alpha value of 0.64 revealed moderate internal consistency reliability when compared with the previous study in the Indian population.[13]
The proportion of participants with high and very high dependence on nicotine in the present study was 26% and 22.5%, respectively. It was higher than the study conducted to estimate tobacco dependence on the population level in Italy where the proportion of participants who had a high and very high dependence on nicotine was about 13.8% and 3.8% correspondingly.[17] The high and very high dependence on nicotine among the study participants could be because tobacco consumption is a part of the socio-cultural milieu among various communities in India. Furthermore, India being the second major consumer and third leading producer of tobacco in the world and lack of firm political will makes the tobacco products readily available for consumption.
The number of years of cigarette smoking was significantly correlated with the nicotine dependence (P = 0.000 and r = 0.30). In the logistic regression analysis, when compared to the participants smoking for 1 to 10 years, the participants who were smoking for 11 to 20 years, 21 to 30 years and more had the high dependence on nicotine. As the person smokes for more the number of years, chronic exposure to nicotine occurs in the nicotinic acetylcholine receptors with resultant neuroadaptation to nicotine, and consecutively the participants tend to smoke more.
Several studies have revealed the variables age and age of onset of smoking as risk indicators for nicotine dependence.[18] Age of onset of smoking is important as the persons start smoking at the younger age, sensitization of receptors in the brain to nicotine occurs leading to the craving for cigarettes. However, in the present study, the age of onset of smoking was not significantly correlated with the nicotine dependence (P = 0.37).
The age of the study participants was significantly correlated with the nicotine dependence (P = 0.000), but it was not a significant risk indicator for nicotine dependence in the regression model (P = 0.31).
The variables education, occupation, and marital status of the study participants were negligibly correlated with the nicotine dependence. Conversely, in a study conducted to assess the socioeconomic variations on nicotine dependence, self-efficacy, and intention to quit, lower level of education was associated with higher levels of nicotine dependence, low self-efficacy, and no intention to quit.[19]
CO level is considered to be an immediate and noninvasive biochemical measure to validate the smoking status. In the present study, CO level was measured among the participants to verify the self-reported smoking status and to determine whether CO level correlates with the nicotine dependence as it indirectly reflects the nicotine seeking and dependence. The exhaled CO levels among the participants depend on the number of cigarettes smoked, number and depth of the puffs the participants inhale from the cigarettes.
Concerning CO levels in the present study, 39.1% and 28.8% of the participants had CO levels ranging from 0–6 ppm to 7–10 ppm correspondingly. It could be due to the lighter and less the number of puffs by the study participants and also might be due to faster elimination rate of CO among the participants. In the present study, CO level was significantly correlated with the nicotine dependence (P = 0.000) and (r = 0.37). In a similar study among Malaysian smokers, the exhaled CO levels were significantly correlated with the nicotine dependence.[9] Hence, exhaled CO levels can be used to indicate nicotine dependence among the smokers.
Limitations
The probable limitation of the study could be no female representation. Since the study was done in the field setting, we had not encountered any female smokers during the study.
The other limitation could be the interview with the study participants, as there may be chances for overreporting or underreporting.
The exhaled CO levels were measured using the COmpact Smokerlyzer, with levels calibrated as 0–6 ppm, 7–10 ppm, 11–15 ppm, 16–25 ppm, 26–35 ppm, and 36–50 ppm. Hence, we were not able to calculate the exact cut-off level of CO for correlating with the nicotine dependence.
CONCLUSION
The study tools were sensitive in the field setting which helped to identify the participants with different levels of nicotine dependence and in measuring exhaled CO levels. FTND could be used by the public health professionals in the outreach programs to assess the nicotine dependence for referrals and appropriate interventions. The exhaled CO levels can be used to educate the patients regarding the consequences of smoking in the outreach programs and during smoking cessation programs.
Recommendations
The results of the study can be shared with the policymakers, nongovernmental organizations, and voluntary organizations to initiate appropriate interventions accordingly at the micro, meso, and the macro level.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.TCP India Project Report. Findings from the Wave 1 Survey (2010-2011): University of Waterloo, Ontario. Canada, Navi Mumbai, India: Healis-Sekhsaria Institute for Public Health; 2013. The International Tobacco Control Policy Evaluation Project. [Google Scholar]
- 2.Ng M, Freeman MK, Fleming TD, Robinson M, Dwyer-Lindgren L, Thomson B, et al. Smoking prevalence and cigarette consumption in 187 countries, 1980-2012. JAMA. 2014;311:183–92. doi: 10.1001/jama.2013.284692. [DOI] [PubMed] [Google Scholar]
- 3.Global Adult Tobacco Survey, GATS India 2009-2010. New Delhi: Ministry of Health and Family Welfare, Government of India; 2010. Ministry of Health and Family Welfare, Government of India. [Google Scholar]
- 4.World Health Organization. Neuro Science of Psycho Active Substance Use and Dependence. Geneva: World Health Organization; 2004. [Google Scholar]
- 5.Pednekar MS, Gupta PC, Yeole BB, Hébert JR. Association of tobacco habits, including bidi smoking, with overall and site-specific cancer incidence: Results from the Mumbai cohort study. Cancer Causes Control. 2011;22:859–68. doi: 10.1007/s10552-011-9756-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.West R. Assessment of dependence and motivation to stop smoking. BMJ. 2004;328:338–9. doi: 10.1136/bmj.328.7435.338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Low EC, Ong MC, Tan M. Breath carbon monoxide as an indication of smoking habit in the military setting. Singapore Med J. 2004;45:578–82. [PubMed] [Google Scholar]
- 8.Deveci SE, Deveci F, Açik Y, Ozan AT. The measurement of exhaled carbon monoxide in healthy smokers and non-smokers. Respir Med. 2004;98:551–6. doi: 10.1016/j.rmed.2003.11.018. [DOI] [PubMed] [Google Scholar]
- 9.Guan NC, Ann AY. Exhaled carbon monoxide levels among Malaysian male smokers with nicotine dependence. Southeast Asian J Trop Med Public Health. 2012;43:212–8. [PubMed] [Google Scholar]
- 10.Kapusta ND, Pietschnig J, Plener PL, Blüml V, Lesch OM, Walter H, et al. Does breath carbon monoxide measure nicotine dependence? J Addict Dis. 2010;29:493–9. doi: 10.1080/10550887.2010.509280. [DOI] [PubMed] [Google Scholar]
- 11.Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The Fagerström test for nicotine dependence: A revision of the Fagerström tolerance questionnaire. Br J Addict. 1991;86:1119–27. doi: 10.1111/j.1360-0443.1991.tb01879.x. [DOI] [PubMed] [Google Scholar]
- 12.Chandra PS, Carey MP, Carey KB, Jairam KR, Girish NS, Rudresh HP, et al. Prevalence and correlates of tobacco use and nicotine dependence among psychiatric patients in India. Addict Behav. 2005;30:1290–9. doi: 10.1016/j.addbeh.2005.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jhanjee S, Sethi H. The Fagerström test for nicotine dependence in an Indian sample of daily smokers with poly drug use. Nicotine Tob Res. 2010;12:1162–6. doi: 10.1093/ntr/ntq148. [DOI] [PubMed] [Google Scholar]
- 14.Jayakrishnan R, Mathew A, Lekshmi K, Sebastian P, Finne P, Uutela A, et al. Assessment of nicotine dependence among smokers in a selected rural population in Kerala, India. Asian Pac J Cancer Prev. 2012;13:2663–7. doi: 10.7314/apjcp.2012.13.6.2663. [DOI] [PubMed] [Google Scholar]
- 15.Manimunda SP, Benegal V, Sugunan AP, Jeemon P, Balakrishna N, Thennarusu K, et al. Tobacco use and nicotine dependency in a cross-sectional representative sample of 18,018 individuals in Andaman and Nicobar Islands, India. BMC Public Health. 2012;12:515. doi: 10.1186/1471-2458-12-515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zhang J, Yao X, Yu R, Bai J, Sun Y, Huang M, et al. Exhaled carbon monoxide in asthmatics: A meta-analysis. Respir Res. 2010;11:50. doi: 10.1186/1465-9921-11-50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gallus S, Pacifici R, Colombo P, La Vecchia C, Garattini S, Apolone G, et al. Tobacco dependence in the general population in Italy. Ann Oncol. 2005;16:703–6. doi: 10.1093/annonc/mdi153. [DOI] [PubMed] [Google Scholar]
- 18.Roberts B, Gilmore A, Stickley A, Kizilova K, Prohoda V, Rotman D, et al. Prevalence and psychosocial determinants of nicotine dependence in nine countries of the former soviet union. Nicotine Tob Res. 2013;15:271–6. doi: 10.1093/ntr/nts100. [DOI] [PubMed] [Google Scholar]
- 19.Siahpush M, McNeill A, Borland R, Fong GT. Socioeconomic variations in nicotine dependence, self-efficacy, and intention to quit across four countries: Findings from the international tobacco control (ITC) four country survey. Tob Control. 2006;15(Suppl 3):iii71–5. doi: 10.1136/tc.2004.008763. [DOI] [PMC free article] [PubMed] [Google Scholar]