

INTRODUCTION
Graft-versus-host-disease (GVHD) is a multisystem disease that can occur after blood and marrow or solid organ transplantation. Transplanted immune cells (graft) recognize cells or tissues from the transplant recipient (host) as foreign and initiate an immune reaction manifesting in multiple organ systems, often including the skin. GVHD following solid organ transplantation (solid organ transplantation-associated GVHD; SOT GVHD) may present in one of two forms1. The more common form involves an antibody-mediated reaction against the recipient’s red blood cells, resulting in a mild and transient hemolytic anemia. The second form is driven by cellular immunity and may affect the recipient’s skin, gastrointestinal tract, liver, and/or bone marrow1. Known risk factors for developing SOT GVHD include: African American race, HLA mismatch, and cytomegalovirus infection2, as well as an underlying tumor diagnosis or neoadjuvant chemotherapy administered before the transplant3. While 3 case reports from the literature have shown that aggressive immunosuppression and plasmapheresis can be successful in treating SOT GVHD, there still exist challenges to treatment4–6.
Though patients with SOT GVHD may experience cutaneous involvement, it has been our experience that the associated eruption is non-specific and may mimic more common entities, such as viral exanthema or drug reaction. Lack of its recognition may lead to a delay in diagnosis and possibly worsened outcomes. We aimed to perform a systematic review on available relevant literature to better understand this rare but potentially serious complication of solid organ transplantation, with an emphasis on its dermatologic manifestations.
METHODS
Literature search
With the assistance of a Masters level medical librarian (A.F.), we performed a systematic review of existing English-language literature on patients who demonstrated dermatologic manifestations after SOT GVHD. We searched the following databases: MEDLINE (1946–2016), Embase (1988–2016), Web of Science (1975–2016), and Scopus (1823–2016). Studies published online, published in print, and in press from all years were considered. All search results with titles and abstracts written in English were eligible for inclusion. Studies were excluded based on the title, abstract, or both if there was no clear indication as to whether they documented dermatologic manifestations of graft-versus-host-disease after solid organ transplantation. Pediatric SOT GVHD cases were excluded. Due to the rare nature of SOT GVHD, case reports were included for review.
Data extraction
The following parameters were documented: first author; year of publication; number of cases reported; dermatologic features of SOT GVHD; skin symptoms; when skin symptoms first appeared after transplant; methods used to determine the diagnosis of SOT GVHD; biopsy results; organ involvement and complications; treatment regimen; patient outcome.
RESULTS
Study characteristics
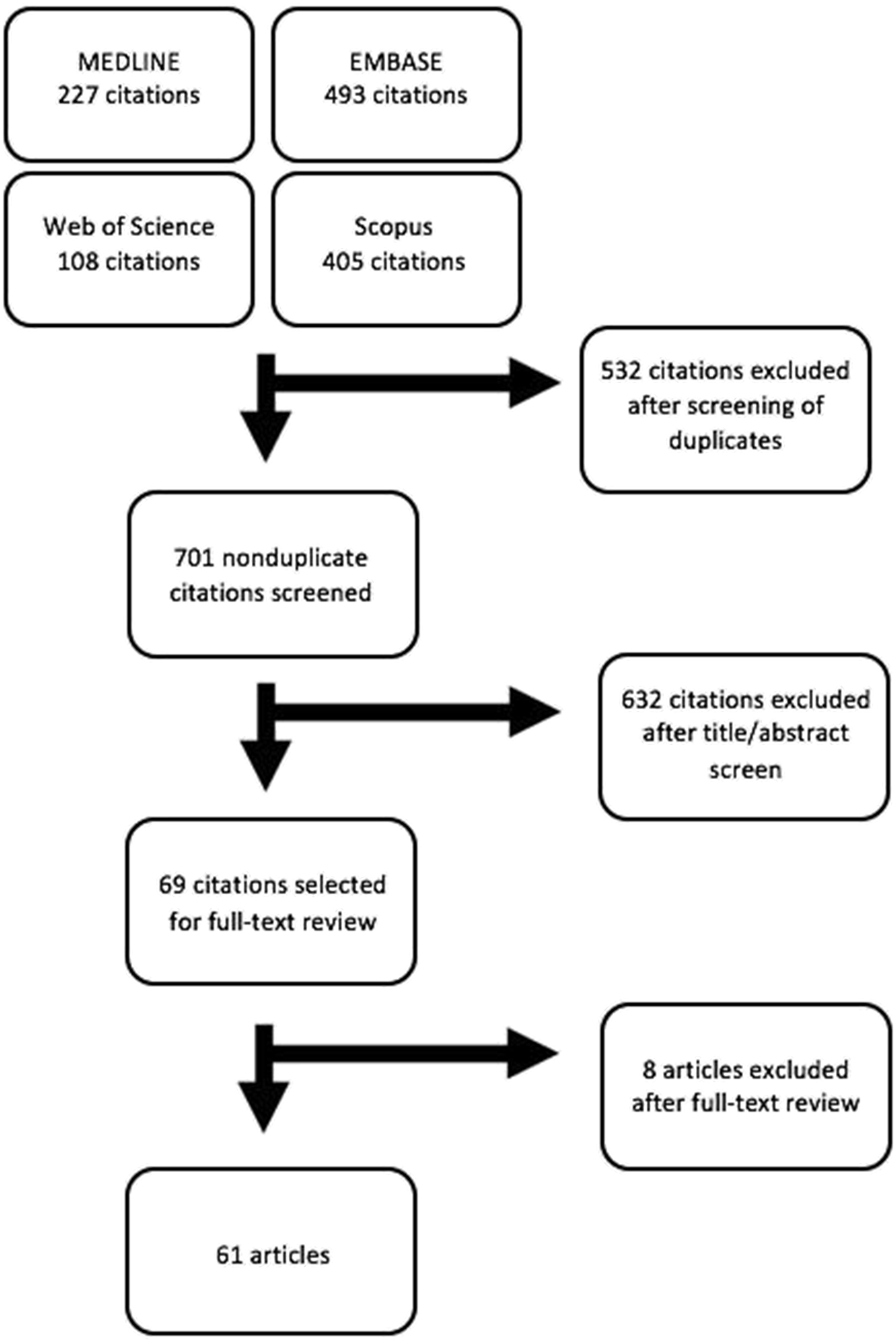
The initial literature search yielded a total of 1233 articles. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram is presented in Fig 1. In 61 articles published between 1991 and 2016, there were 115 patients with SOT GVHD reported. Of these patients, a total of 126 organs were transplanted, as some patients received multiple organs4–65. SOT GVHD was most common after liver transplantation (n=81, 64.3%). A summary of data from existing literature can be found in Table 1.
Table 1.
Summary of data from systematic literature review
| Total number of studies | 61 |
| Total number of cases | 115 |
| Organs transplanted | 126 |
| Liver | 81/126(64.3%) |
| Pancreas | 13/126(10.3%) |
| Lung | 8/126 (6.3%) |
| Kidney | 13/126(10.3%) |
| Heart | 5/126 (3.9%) |
| Intestinal | 6/126 (4.8%) |
| Dermatologic manifestations | 101/115 = 87.8% |
| Average POD of appearance of skin manifestations | 48.3 n=92 (range: 3–243) |
| Pruritic | 5/101 (4.9%) |
| Morbilliform | 2/101 (1.9%) |
| Confluent | 6/101 (5.9%) |
| Desquamation | 4/101 (3.9%) |
| Complications of SOT GVHD | |
| Total number of patients who died | 70/97(72.2%) |
| Total number of patients who recovered | 27/97 (27.8%) |
| Average POD of death | 99.2 n=23 |
| Common causes of death | |
| Infection | 10 |
| Hemorrhage | 5 |
| Sepsis | 28 |
| Multi-organ failure | 14 |
| Acute respiratory distress | 2 |
*POD = Post-operative day
Dermatologic manifestations
Of the 92 patients for whom the duration between transplantation and development of skin eruption was recorded, dermatologic manifestations of SOT GVHD developed an average of 48.3 days (range: 3–24348,60) after transplant, which is earlier than the 63 days observed in our retrospective review of patients (n=9) at the Mayo Clinic (unpublished data). While dermatologic findings were variable, the most frequent description was that of a maculopapular exanthem [28 of 101 (27.7%) patients], with 2 (1.9%) also being described as morbilliform11,23. Confluent erythema and desquamation were observed in 6 (5.9%)13,17,26,44,46,57 and 4 (3.9%)26,50,51,63 patients, respectively. In one patient, the dermatologic symptoms initially began as a maculopapular eruption that progressed to one resembling toxic epidermal necrolysis60. Of 101 patients, dermatologic findings involved the extremities in 16 (15.8%) , the trunk in 14 (13.9%) , and the face in 9 (8.9%). Detailed dermatologic descriptions were not available in the remaining relevant articles.
Diagnosis of SOT GVHD
When GVHD was suspected, skin biopsies, chimerism studies and FISH were performed in almost all cases reported in the literature. Skin biopsies were helpful in confirming the clinical suspicion of SOT GVHD, as they often revealed vacuolar degeneration, necrotic keratinocytes, and satellite cell necrosis, microscopic features that are characteristic in skin biopsies of patients with hematopoietic cell transplantation-related GVHD. In one instance, when biopsy of the bone marrow failed to show chimerism, skin biopsy results were used to confirm the diagnosis of SOT GVHD5. Moreover, in a case report by Meves et al., FISH performed on skin biopsy specimens helped confirm the diagnosis of GVHD in sex-mismatched patients63. In cases in which a PCR-based chimerism assay failed to reveal donor DNA in peripheral blood, FISH performed on skin biopsy specimens revealed a significant number of donor lymphocytes that helped solidify the diagnosis. HLA typing was performed in peripheral blood lymphocytes in 6 cases9,42,43,55,60,66. In one study, donor lymphocytes were marked by immunohistochemical methods on skin biopsy specimens as well56. HLA typing was performed by serologic techniques to test for specific donor HLA antigens in 3 cases29,51,56. For instance, in a study conducted by Smith et al., when GVHD was suspected, the patient was re-typed for HLA-A and HLA-B antigens, which demonstrated a mixture of the patient and donor HLA types with a stronger reaction being the donor’s HLA type51. HLA typing was particularly helpful in detecting the donor HLA phenotype when skin biopsy showed no signs of GVHD65.
Complications of SOT GVHD
The triad of fever, diarrhea, and pancytopenia was documented in 11 of 115 (9.6%) patients who went on to be diagnosed with SOT GVHD. Sepsis and multi-organ failure were the two most common causes of death. For the 97 patients for whom clinical outcome could be discerned from the literature, 70 (72.2%) died. Of the 23 patients for whom the time interval between transplantation and death was reported, the time after transplant to death was on average 99.2 days. Of these patients, the average time to death from the appearance of a rash was 51.7 days.
DISCUSSION
Graft-versus-host disease is a potentially lethal complication of solid organ transplantation. While several case reports and series have been published previously, we are not aware of a systematic review of the literature on SOT GVHD, particularly with regards to the dermatologic manifestations. Based on our findings, we can conclude that the dermatologic manifestations of SOT GVHD can develop within a few days to several months after transplant. The dermatologic presentation can also be varied, although it does seem to share clinical and microscopic features with hematopoietic cell transplantation-associated GVHD. Reported cases were associated with a high mortality rate.
Importantly, this literature review indicates that the dermatologic manifestations of SOT GVHD can be non-specific. Thus, particularly given the seriousness of the disease, it is essential that the consulting dermatologist have a high index of suspicion for this rare diagnosis and pursue confirmatory tests, such as a skin biopsy or other ancillary tests.
Our study demonstrates the importance of combining clinical and laboratory variables in predicting the likelihood of this disease. For instance, evidence of bone marrow or gastrointestinal tract involvement accompanying the development of a new skin eruption in the post-transplantation period may be suggestive of SOT GVHD. Though the triad of fever, diarrhea and pancytopenia was relatively infrequently observed in this population, this constellation of findings may be specific for SOT GVHD. Further studies are required to determine the specificity of these clinical features.
Currently available tests to confirm the diagnosis of SOT GVHD are not entirely sensitive. In the setting of hematopoietic cell transplantation, peripheral blood chimerism assays with only 5% sensitivity are required detect recipient bone marrow cells or graft failures. However, this sensitivity is inadequate to sufficiently exclude chimerism with a negative test in the setting of suspected SOT GVHD. While FISH can be helpful, its use is limited by the fact that it can only be applied when patients receive a transplant from a patient of the opposite sex.. We encourage future efforts to develop a more sensitive assay for chimerism in the setting of SOT GVHD.
Limitations to this systematic review include incomplete or general dermatologic descriptions in reported cases, as well as potential publication bias favoring the most fulminant and/or fatal cases.
CONCLUSION
SOT GVHD is a potentially fatal complication of solid organ transplantation that often presents with a non-specific skin eruption. Early recognition of this entity by the dermatologist, with supportive evidence from skin biopsy and possibly other ancillary tests, such as FISH or PCR-based chimerism studies, may decrease delay in diagnosis and allow for prompt initiation of appropriate treatment.
Supplementary Material
Fig 1. PRISMA flow diagram of literature search and study selection for systematic review of SOT GVHD.
{kind=link}
CAPSULE SUMMARY.
Dermatologic manifestations of graft-versus-host disease after solid organ transplantation (SOT GVHD) are not well-known.
Skin eruptionappears early on and has varied clinical presentations.
In patients who develop dermatologic signs following solid-organ transplantation, we advise dermatologists to have a high index of suspicion for this rare but potentially fatal entity.
Acknowledgement:
We thank Dr. David S. Viswanatha for sharing with us his expertise on FISH and chimerism testing for GVHD.
Funding sources:
None.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
IRB approval status: Not required.
Conflicts of interest disclosure:
None declared.
REFERENCES
- 1.Gulbache H, Brown C, Wicks M, Segall M, Jessurun J. Graft-vs-Host Disease After Solid Organ Transplant. Am J Clin Pathol. 2003;119(4):568–573. [DOI] [PubMed] [Google Scholar]
- 2.Sharma A, Armstrong AE, Posner MP, et al. Graft-versus-host disease after solid organ transplantation: a single center experience and review of literature. Ann Transpl. 2012;17(4):133–139. [DOI] [PubMed] [Google Scholar]
- 3.Cromvik J, Varkey J, Herlenius G, Johansson J-E, Wennerås C. Graft-versus-host Disease After Intestinal or Multivisceral Transplantation: A Scandinavian Single-center Experience. Transplant Proc. 2016;48(1):185–190. [DOI] [PubMed] [Google Scholar]
- 4.Rossi AP, Bone BA, Edwards AR, et al. Graft-versus-host disease after simultaneous pancreas-kidney transplantation: a case report and review of the literature. Am J Transpl. 2014;14(11):2651–2656. [DOI] [PubMed] [Google Scholar]
- 5.Guy S, Potluri A, Xiao G, et al. Successful treatment of acute severe graft-versus-host-disease in a pancreas-after-kidney transplant recipient: Case report. Transplant Proc. 2014;46(7):2446–2449. [DOI] [PubMed] [Google Scholar]
- 6.Zacharias N, Gallichio MH, Conti DJ. Graft-versus-Host Disease after Living-Unrelated Kidney Transplantation. Case Rep Transplant. 2014;2014:971426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Asari S, Matsumoto I, Toyama H, et al. Acute graft-versus-host disease following simultaneous pancreas-kidney transplantation: report of a case. Surg Today. 2015;45(12):1567–1571. [DOI] [PubMed] [Google Scholar]
- 8.Elsiesy H, Ibrahim A, Selim K, et al. Graft-versus-Host Disease after Liver Transplantation: A Single-Center Case Series. Ann Transplant. 2015;20:397–401. [DOI] [PubMed] [Google Scholar]
- 9.Schmuth M, Vogel W, Weinlich G, Margreiter R, Fritsch P, Sepp N. Cutaneous lesions as the presenting sign of acute graft-versus-host disease following liver transplantation. Br J Dermatol. 1999;141(5):901–904. [DOI] [PubMed] [Google Scholar]
- 10.Kohler S, Pascher A, Junge G, et al. Graft versus host disease after liver transplantation - a single center experience and review of literature. Transpl Int. 2008;21(5):441–451. [DOI] [PubMed] [Google Scholar]
- 11.Jeanmonod P, Hubbuch M, Grunhage F, et al. Graft-versus-host disease or toxic epidermal necrolysis: diagnostic dilemma after liver transplantation. Transpl Infect Dis. 2012;14(4):422–426. [DOI] [PubMed] [Google Scholar]
- 12.Weinstein A, Dexter D, KuKuruga DL, Philosophe B, Hess J, Klassen D. Acute graft-versus-host disease in pancreas transplantation: a comparison of two case presentations and a review of the literature. Transplantation. 2006;82(1):127–131. [DOI] [PubMed] [Google Scholar]
- 13.Moody MN, Kazakevich N, Smith JR, et al. Sweat the small stuff: the importance of clinical-pathologic correlation in cutaneous GVHD following orthotopic liver transplant. Arch Dermatol. 2011;147(11):1345–1346. [DOI] [PubMed] [Google Scholar]
- 14.Chang JW, Sageshima J, Ciancio G, et al. Successful treatment for graft-versus-host disease after pancreas transplantation. Clin Transplant. 2014;28(2):217–222. [DOI] [PubMed] [Google Scholar]
- 15.Assi MA, Pulido JS, Peters SG, McCannel CA, Razonable RR. Graft-vs.-host disease in lung and other solid organ transplant recipients. Clin Transplant. 2007;21(1):1–6. [DOI] [PubMed] [Google Scholar]
- 16.Gao PJ, Leng XS, Wang D, et al. Graft versus host disease after liver transplantation: a case report. Front Med China. 2010;4(4):469–472. [DOI] [PubMed] [Google Scholar]
- 17.Sudhindran S, Taylor A, Delriviere L, et al. Treatment of graft-versus-host disease after liver transplantation with basiliximab followed by bowel resection. Am J Transplant. 2003;3(8):1024–1029. [DOI] [PubMed] [Google Scholar]
- 18.Gulbahce HE, Brown CA, Wick M, Segall M, Jessurun J. Graft-vs-host disease after solid organ transplant. Am J Clin Pathol. 2003;119(4):568–573. [DOI] [PubMed] [Google Scholar]
- 19.Smith DM, Agura E, Netto G, et al. Liver transplant-associated graft-versus-host disease. Transplantation. 2003;75(1):118–126. [DOI] [PubMed] [Google Scholar]
- 20.Roberts JP, Ascher NL, Lake J, et al. Graft vs. host disease after liver transplantation in humans: a report of four cases. Hepatology. 1991;14(2):274–281. [PubMed] [Google Scholar]
- 21.Redondo P, Espana A, Herrero JI, et al. Graft-versus-host disease after liver transplantation. J Am Acad Dermatol. 1993;29(2 Pt 2): 314–317. [DOI] [PubMed] [Google Scholar]
- 22.Elfeki MA, Genco P V, Pungpapong S, Nakhleh RE, Nguyen JH, Harnois DM. Abatacept use in graft-versus-host disease after orthotopic liver transplantation: a case report. Transplant Proc. 2014;46(7):2422–2425. [DOI] [PubMed] [Google Scholar]
- 23.Stotler CJ, Eghtesad B, Hsi E, Silver B. Rapid resolution of GVHD after orthotopic liver transplantation in a patient treated with alefacept. Blood. 2009;113(21):5365–5366. [DOI] [PubMed] [Google Scholar]
- 24.Cho EH, Suh KS, Yang SH, et al. Acute graft versus host disease following living donor liver transplantation: first Korean report. Hepatogastroenterology. 2007;54(79):2120–2122. [PubMed] [Google Scholar]
- 25.Merhav HJ, Landau M, Gat A, et al. Graft versus host disease in a liver transplant patient with hepatitis B and hepatocellular carcinoma. Transplant Proc. 1999;31(4):1890–1991. [DOI] [PubMed] [Google Scholar]
- 26.Sun B, Zhao C, Xia Y, et al. Late onset of severe graft-versus-host disease following liver transplantation. Transpl Immunol. 2006;16(3–4):250–253. [DOI] [PubMed] [Google Scholar]
- 27.Guo ZY, He XS, Wu LW, et al. Graft-verse-host disease after liver transplantation: A report of two cases and review of literature. World J Gastroenterol. 2008;14(6):974–979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Qiu W, Lv GY, Jiang C, et al. Successful salvage treatment of acute graft-versus-host disease after liver transplantation by withdrawal of immunosuppression: a case report. Korean J Hepatobiliarypancreatic Surg. 2016;20(1):38–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kanehira K, Riegert-Johnson DL, Chen D, Gibson LE, Grinnell SD, Velgaleti G V. FISH diagnosis of acute graft-versus-host disease following living-related liver transplant. J Mol Diagnostics. 2009;11(4):355–358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Nemoto T, Kubota K, Kita J, et al. Unusual onset of chronic graft-versus-host disease after adult living-related liver transplantation from a homozygous donor. Transplantation. 2003;75(5):733–736. [DOI] [PubMed] [Google Scholar]
- 31.Smith DM, Agura ED, Ausloos K, Ring WS, Domiati-Saad R, Klintmalm GB. Graft-vs-host disease as a complication of lung transplantation. J Hear Lung Transplant. 2006;25(9):1175–1177. [DOI] [PubMed] [Google Scholar]
- 32.Mazariegos G V, Abu-Elmagd K, Jaffe R, et al. Graft versus host disease in intestinal transplantation. Am J Transplant. 2004;4(9):1459–1465. [DOI] [PubMed] [Google Scholar]
- 33.Pageaux GP, Perrigault PF, Fabre JM, et al. Lethal acute graft-versus-host disease in a liver transplant recipient: relations with cell migration and chimerism. Clin Transplant. 1995;9(1):65–69. [PubMed] [Google Scholar]
- 34.Cheung CYM, Leung AYH, Chan SC, Trendell-Smith NJ, So CC, Kwong YL. Fatal graft-versus-host disease after unrelated cadaveric liver transplantation due to donor/recipient human leucocyte antigen matching. Intern Med J. 2014;44(4):425–426. [DOI] [PubMed] [Google Scholar]
- 35.Kang WH, Hwang S, Song GW, et al. Acute Graft-vs-Host Disease After Liver Transplantation: Experience at a High-volume Liver Transplantation Center in Korea. Transplant Proc. 2016;48(10):3368–3372. [DOI] [PubMed] [Google Scholar]
- 36.Corbi MR, Sanchez Conejo-Mir J, Linares M, Jimenez G, Artola JL, Navarrete M. Graft-versus-host disease after liver transplantation. [Spanish]. Med Cutan Ibero Lat Am. 1996;24(5):251–254. [Google Scholar]
- 37.Kuball J, Theobald M, Ferreira EA, et al. Control of organ transplant-associated graft-versus-host disease by activated host lymphocyte infusions. Transplantation. 2004;78(12):1774–1779. [DOI] [PubMed] [Google Scholar]
- 38.Rogulj IM, Deeg J, Lee SJ. Acute graft versus host disease after orthotopic liver transplantation. J Hematol Oncol. 2012;5:50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Soejima Y, Shimada M, Suehiro T, et al. Graft-versus-host disease following living donor liver transplantation. Liver Transplant. 2004;10(3):460–464. [DOI] [PubMed] [Google Scholar]
- 40.Zeidan AM, Wozney JL, Torbenson M, Krok K, Bolaños-Meade J. Successful treatment of severe refractory hepatic graft-versus-host disease by cadaveric liver transplant. Leuk Lymphoma. 2013;54(12):2756–2759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Yu YD, Kim DS, Ha N, et al. Fatal Graft-Versus-Host Disease Following Adult-To-Adult Living Donor Liver Transplantation From an HLA Nonhomozygous Donor. Prog Transplant. 2016;23:23. [DOI] [PubMed] [Google Scholar]
- 42.Liang TB, Tang XF, Zheng SS, et al. [Graft versus host disease after liver transplantation: a report of 3 cases]. Chung-Hua i Hsueh Tsa Chih [Chinese Med Journal]. 2004;84(10):826–829. [PubMed] [Google Scholar]
- 43.Agura E, Smith DM, Netto G, et al. Fatal graft-versus-host disease associated with solid-organ transplantation. Blood. 2000;96(11 PART II).10607691 [Google Scholar]
- 44.Whalen JG, Jukic DM, English 3rd JC. Rash and pancytopenia as initial manifestations of acute graft-versus-host disease after liver transplantation. J Am Acad Dermatol. 2005;52(5):908–912. [DOI] [PubMed] [Google Scholar]
- 45.Blank G, Li J, Kratt T, Handgretinger R, Konigsrainer A, Nadalin S. Treatment of liver transplant graft-versus-host disease with antibodies against tumor necrosis factor-alpha. Exp Clin Transplant Off J Middle East Soc Organ Transplant. 2013;11(1):68–71. [DOI] [PubMed] [Google Scholar]
- 46.Wang B, Lu Y, Yu L, Liu C, Wu Z, Liu X. Diagnosis and treatment for graft-versus-host disease after liver transplantation: two case reports. Transplant Proc. 2007;39(5):1696–1698. [DOI] [PubMed] [Google Scholar]
- 47.Kato T, Yazawa K, Madono K, Saito J, Hosomi M, Itoh K. Acute graft-versus-host-disease in kidney transplantation: case report and review of literature. Transplant Proc. 2009;41(9):3949–3952. [DOI] [PubMed] [Google Scholar]
- 48.Pollack MS, Speeg K V, Callander NS, et al. Severe, late-onset graft-versus-host disease in a liver transplant recipient documented by chimerism analysis. Hum Immunol. 2005;66(1):28–31. [DOI] [PubMed] [Google Scholar]
- 49.Weng FL, Pancoska C, Patel AM. Fatal graft-versus-host disease presenting as fever of unknown origin in a pancreas-after-kidney transplant recipient. Am J Transplant. 2008;8(4):881–883. [DOI] [PubMed] [Google Scholar]
- 50.Thin L, Macquillan G, Adams L, et al. Acute graft-versus-host disease after liver transplant: novel use of etanercept and the role of tumor necrosis factor alpha inhibitors. Liver Transplant. 2009;15(4):421–426. [DOI] [PubMed] [Google Scholar]
- 51.Smith DM, Agura ED, Levy MF, Melton LB, Domiati-Saad R, Klintmalm G. Graft vs host disease following kidney transplantation using an “0 HLA antigen mismatched” donor. Nephrol Dial Transplant. 2006;21(9):2656–2659. [DOI] [PubMed] [Google Scholar]
- 52.Walling HW, Voigt MD, Stone MS. Lichenoid graft vs. host disease following liver transplantation. J Cutan Pathol. 2004;31(2):179–184. [DOI] [PubMed] [Google Scholar]
- 53.Luckraz H, Zagolin M, McNeil K, Wallwork J. Graft-versus-host disease in lung transplantation: 4 Case reports and literature review. J Hear Lung Transplant. 2003;22(6):691–697. [DOI] [PubMed] [Google Scholar]
- 54.Zhang C, Yang G, Ling Y, Chen G, Zhou T. Graft versus host disease following liver transplantation: A case report. Exp Ther Med. 2014;8(4):1164–1166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Collins RH Jr, Cooper B, Nikaein A, Klintmalm G, Fay JW. Graft-versus-host disease in a liver transplant recipient. Ann Intern Med. 1992;116(5):391–392. [DOI] [PubMed] [Google Scholar]
- 56.Lehner F, Becker T, Sybrecht L, et al. Successful outcome of acute graft-versus-host disease in a liver allograft recipient by withdrawal of immunosuppression. Transplantation. 2002;73(2):307–310. [DOI] [PubMed] [Google Scholar]
- 57.Lu Y, Wu LQ, Zhang BY, Cao JY. Graft-Versus-Host Disease After Liver Transplantation: Successful Treatment of a Case. Transplant Proc. 2008;40(10):3784–3786. [DOI] [PubMed] [Google Scholar]
- 58.Yilmaz M, Ozdemir F, Akbulut S, et al. Chronic graft-versus-host disease after liver transplantation: a case report. Transplant Proc. 2012;44(6):1751–1753. [DOI] [PubMed] [Google Scholar]
- 59.Perez Saborido B, Asensio Diaz E, Barrera Rebollo A, et al. Graft versus host disease as a complication after liver transplantation: A rare but serious association. Rev Esp Enfermedades Dig. 2015;5:5. [PubMed] [Google Scholar]
- 60.Pfitzmann R, Hummel M, Grauhan O, et al. Acute graft-versus-host disease after human heart-lung transplantation: A case report. J Thorac Cardiovasc Surg. 1997;114(2):285–287. [DOI] [PubMed] [Google Scholar]
- 61.Fossi A, Voltolini L, Filippi R, et al. Severe Acute Graft Versus Host Disease After Lung Transplant: Report of a Case Successfully Treated With High Dose Corticosteroids. J Hear Lung Transplant. 2009;28(5):508–510. [DOI] [PubMed] [Google Scholar]
- 62.Auerbach JS, Schott CK. Solid-Organ Graft-Versus-Host Disease After Liver Transplant: A Case Report. Crit Care Nurse. 2016;36(3):e7–e11. [DOI] [PubMed] [Google Scholar]
- 63.Meves A, el-Azhary RA, Talwalkar JA, et al. Acute graft-versus-host disease after liver transplantation diagnosed by fluorescent in situ hybridization testing of skin biopsy specimens. J Am Acad Dermatol. 2006;55(4):642–646. [DOI] [PubMed] [Google Scholar]
- 64.Kimball P, Ham J, Eisenberg M, et al. Lethal graft-versus-host disease after simultaneous kidney-pancreas transplantation. Transplantation. 1997;63(11):1685–1688. [DOI] [PubMed] [Google Scholar]
- 65.Neumann U, Knoop M, Langrehr JM, et al. [Graft-vs.-host reaction: a severe complication after orthotopic liver transplantation]. Zentralbl Chir. 1995;120(6):478–481. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fig 1. PRISMA flow diagram of literature search and study selection for systematic review of SOT GVHD.