

Abstract
Background:
Alcohol outlet density has been associated with increased pedestrian injury risk. It is unclear whether this is because alcohol outlets are located in dense retail areas with heavy pedestrian traffic or whether alcohol outlets contribute a unique neighborhood risk. We aimed to compare the pedestrian injury rate around alcohol outlets to the rate around other, similar retail outlets that do not sell alcohol.
Methods:
A spatial analysis was conducted on census block groups in Baltimore City. Data included pedestrian injury EMS records from January 1, 2014, to April 15, 2015 (n=848); locations of alcohol outlets licensed for off-premise (n=726) and on-premise consumption (n=531); and corner (n=398) and convenience stores (n=192) that do not sell alcohol. Negative binomial regression was used to determine the relationship between retail outlet count and pedestrian injuries, controlling for key confounding variables. Spatial autocorrelation was also assessed and variable selection adjusted accordingly.
Results:
Each additional off-premise alcohol outlet was associated with a 12.3% increase in the rate of neighborhood pedestrian injury when controlling for convenience and corner stores and other confounders (IRR=1.123, 95%CI=(1.065, 1.184), p<0.001). The attributable risk was 4.9% (95% CI=(0.3%,8.9%)) or 41 additional injuries. On-premise alcohol outlets were not significant predictors of neighborhood pedestrian injury rate in multivariable models (IRR=0.972, 95%CI=(0.940, 1.004), p=0.194).
Conclusion:
Off-premise alcohol outlets are associated with pedestrian injury rate, even when controlling for other types of retail outlets. Findings reinforce the importance of alcohol outlets in understanding neighborhood pedestrian injury risk and may provide evidence for informing policy on liquor store licensing, zoning, and enforcement.
Keywords: alcohol outlets, alcohol availability, pedestrian injury, spatial analysis, neighborhood
INTRODUCTION
Pedestrian injuries have steadily increased over the last decade in the United States, with 5,376 killed and 70,000 injured in 2015 alone; pedestrian fatality increased by 25% from 2010 to 2015 (National Center for Statistics and Analysis, 2017). Neighborhood presence of alcohol outlets has been associated with increased risk for pedestrian-involved motor vehicle crashes in several studies, for both alcohol-involved crashes (DiMaggio et al., 2016; Escobedo and Ortiz, 2002; LaScala et al., 2001; Treno et al., 2007) and all pedestrian injuries in general (Nesoff et al., 2018; Schuurman et al., 2009). However, it is unclear whether this is because alcohol outlets are located in dense retail areas with heavy pedestrian and motor vehicle traffic or whether alcohol outlets contribute a unique neighborhood injury risk.
The location of alcohol outlets alongside other commercial destinations may account for the increased risk for pedestrian injury in these neighborhoods. The convergence of people and vehicles at popular destinations such as workplaces, restaurants, bars, and recreation and entertainment venues may provide more opportunities for pedestrians and vehicles to interact, increasing crash risk (Dai et al., 2010). At the same time, several studies have shown that densely-populated urban areas characterized by mixed residential and commercial land use experience fewer motor vehicle crashes, particularly when traffic safety infrastructure is in place (Ewing and Dumbaugh, 2009; Miranda-Moreno et al., 2011). To our knowledge, the risk for motor vehicle crashes around alcohol outlets compared to other, similar commercial establishments has not been studied.
There is evidence that alcohol outlets contribute a unique community risk factor for injury above and beyond that associated with densely-populated retail areas (Grubesic et al., 2013; Tabb et al., 2016). A study comparing violent injury around liquor stores to that around small grocery and convenience stores found that, although violent injury was associated with both types of retail locations, liquor stores were more strongly associated with violent injury; this association remained strong for longer distances away from liquor stores compared to other retail locations, even when controlling for a variety of neighborhood factors (Furr-Holden et al., 2016). A longitudinal study of nine U.S. cities found that alcohol outlets were associated with greater violent injury, while food establishments such as cafés and coffee shops were protective of violent injury (Wo, 2016).
Furthermore, the type of alcohol outlet may impact neighborhood injury risk differently. Alcohol outlets licensed to sell alcohol for off-premise consumption are more strongly associated with drinking problems, crime, and violence compared to outlets licensed for on-premise consumption only (Branas et al., 2011; Furr-Holden et al., 2016; Han et al., 2016; Schonlau et al., 2008). Off-premise settings include grocery and convenience stores, as well as liquor and package stores and taverns that sell liquor, beer, and wine; on-premise settings include restaurants, bars, hotels, and ballparks (Campbell et al., 2009; Milam et al., 2014). Unlike on-premise outlets, off-premise alcohol outlets can sell alcoholic beverages in large quantities that are distributed to patrons who are unmonitored by servers and often left to drink in nearby, uncontrolled environments such as motor vehicles, liquor store parking lots, or street corners (Branas et al., 2009; LaVeist and Wallace, 2000). Consequently, off-premise outlets are often surrounded by signs of alcohol consumption, such as empty or broken bottles, loiterers, and publicly intoxicated patrons (Cunradi, 2010; Scribner et al., 2007). The aggregation of these deleterious social and physical conditions around alcohol outlets are often viewed as troublesome and potentially threatening by residents and visitors, who may drive or cross the street unsafely to avoid this undesirable activity (Garvin et al., 2013; Theall et al., 2009).
The purpose of this study was to compare the pedestrian injury rate around alcohol outlets to the rate around other, similar retail outlets that do not sell alcohol. We hypothesize that alcohol outlets contribute a unique risk factor for nearby neighborhood pedestrian injury risk. We also compare the pedestrian injury rate around alcohol outlets licensed for on- and off-premise consumption. Consistent with prior research, we hypothesize that off-premise alcohol outlets will be more strongly associated with neighborhood risk for pedestrian injury than on-premise outlets.
MATERIALS AND METHODS
This research was approved by the Institutional Review Board at the Johns Hopkins Bloomberg School of Public Health.
Data Sources
Pedestrian injury data were gathered through emergency medical services (EMS) records collected from January 1, 2014, to April 15, 2015 (n=848). The Baltimore City Fire Department (BCFD) operates the City’s EMS system; as Baltimore City is served by a single EMS system, these data are representative of all EMS calls for pedestrian injuries. Paramedics on the scene confirmed that the injury was caused by a motor vehicle crash. Drug and alcohol use indicators were recorded for only 23% (n=194) of injured pedestrians by EMS staff; positive indicators were present in 6.3% (n=53). Consequently, we were unable to stratify by intoxication status. However, a study of motor vehicle crash victims admitted to a Level-1 trauma center in Baltimore City found that approximately 27% of pedestrians tested positive for alcohol use (Walsh et al., 2005). We, therefore, assume that a majority of pedestrians included in this study were sober at the time of the crash.
Locations of alcohol outlets in 2014 were obtained through the Board of Liquor License Commissioners for Baltimore City. The 12 liquor license types administered by the Board (n=1,264) were classified into on-premise and off-premise alcohol outlets (Jennings et al., 2014). Outlets licensed for on-premise consumption included restaurants, hotels/motels, entertainment venues, and non-profit private clubs (n=531). Off-premise alcohol outlets included all LA/LA2 (n=243) license class locations, liquor stores open six days a week from 9 a.m. to midnight (no Sunday sales) that do not allow on-premise consumption. Off-premise locations also included all LBD7 (n=450) license class locations, bars/taverns allowed to open every day from 6 a.m. to 2 a.m., providing on-premise consumption. LBD7s also sell packaged goods for off-premise consumption, depending on the owner’s discretion. LBD7s are expected to devote at least half of their sales and floor space to on-site consumption; however, this stipulation was only recently incorporated into the zoning code, and there is little oversight to enforce this ruling (Baltimore City Department of Planning, 2009). LBD7s are also the only license class allowable in certain restrictively-zoned residential neighborhoods as LA/LA2 license types were considered inappropriate for residential zones when the City passed its last residential zoning code in 1971 (Friedman, 2015). Stores licensed to sell only wine and beer (i.e., WA license type) exclusively for off-premise consumption (n=33), open six days a week from 6 a.m. to midnight, were also coded as off-premise outlets.
Corner Stores and Convenience Stores.
The addresses and facility names of all 807 food stores from 2013 were obtained from the Baltimore City Health Department; all sell food intended for off-premise consumption. The food stores were classified into seven categories using the schema developed by The Johns Hopkins Center for Livable Future (Haering and Franco, 2010). We chose small food stores—namely, convenience and corner stores—as appropriate comparisons to alcohol outlets.
Corner stores (n=307) are independently-owned and managed, lacking national franchise affiliation. They have a limited supply network, do not have name recognition outside their neighborhood, and have fewer than five cashiers. Behind-the-glass stores (n=127) are a subtype of corner stores. Access to goods is limited by a Plexiglass safety barrier, separating the customers on one side and the cashiers and merchandise on the other. Behind-the-glass stores have the lowest availability of healthy foods in Baltimore as measured by the Healthy Food Availability Index ratings and are located in some of Baltimore’s poorest neighborhoods (Casagrande et al., 2011). After excluding food stores that were also liquor stores, there were 398 corner (n = 284) and behind-the-glass stores (n = 114). These were combined into a single category are referred to “corner stores.”
Convenience stores (n=194) are franchises of nationally or regionally recognized stores, but are much smaller than supermarkets and by definition have fewer than five cashiers. They generally have long hours of operation, well-established distribution systems, and name recognition beyond their immediate area (e.g., 7-eleven, Royal Farms). While the stores’ different locations are homogeneous in appearance, their offerings may vary greatly based on the socioeconomic and racial composition of neighborhoods where they are located. Two convenience stores were excluded because they also sold liquor, beer, and wine (n=192).
Vacant lots:
Addresses for all vacant lots in 2015 were compiled by the Baltimore City Housing Authority (City of Baltimore, n.d.). Digital parcel maps of all lots were available through the Maryland State Department of Planning (Maryland Department of Planning, n.d.). Vacant lots are an important indicator of neighborhood disorder and have significant effects on community health and safety (Branas et al., 2012). A qualitative study of vacant lots’ impact on community well-being found that vacant lots overshadowed positive aspects of the community, eroding community cohesion, attracting crime, and increasing residents’ fear and anxiety (Garvin et al., 2013). To calculate percent of vacant lots per census block group, we aggregated the count of lots that were vacant and the count of all lot parcels to each census block group. We then divided the number of lots that were vacant by the total number of lot parcels in the corresponding block group to calculate the percent of vacant lots in each block group.
Traffic volume:
Traffic volume is an important predictor of pedestrian injury (Lassarre et al., 2007; Morency et al., 2012). Average Daily Traffic Volume for 2013—the most recent year of data availability—was collected by the Maryland State Highway Administration’s Traffic Monitoring System (Maryland State Highway Administration, n.d.). Traffic counts are recorded at a specific point on the roadway referred to as a “count station” but extrapolated to represent the entire segment or section of roadway by a linear referencing system integration process. This data is then mapped for use as a segment file. The traffic count extrapolation process is handled internally by the Maryland State Highway Administration using a linear referencing system (LRS). LRS is based on county, route, and milepoint and uses a distance-based measure system, measured in 1/1000ths of a mile along a route, beginning and ending at jurisdictional boundaries (State of Maryland, n.d.). More information on Maryland’s LRS can be found at Maryland’s Mapping and GIS Data Portal (n.d.). There are 752 count stations in Baltimore City; 168 (22.3%) count stations located on highways were excluded to create a measure of residential traffic volume. For this analysis, we used the spatial lag of traffic flow. We used the join function in ArcGIS 10.4 to join segment data to each census block group to calculate an average of Annual Average Daily Traffic (AADT) values for each census block group. AADT represents a typical traffic volume count any time or day of the year at a count station, including weekends. Traffic on one road is spatially autocorrelated with traffic on adjoining roads because traffic flows through adjoining roadways; likewise, traffic in a census block group is spatially autocorrelated with traffic in the adjoining block groups. The spatial lag accounts for traffic volume in the adjoining census block groups, creating a weighted average of traffic volume over the local area; it does not take into account block groups that may be geographically close but are separated by bodies of water. This smooths census block group traffic volume and allows for a more effective estimation of average traffic volume in each census block group (Bivand et al., 2013). Traffic volume was measured in units of 1,000 vehicles to better facilitate interpretation of coefficients.
Walk Score for Baltimore neighborhoods were obtained from Live Baltimore and served as a proxy measure for pedestrian volume as higher Walk Scores are correlated with higher volumes of pedestrians (Live Baltimore, 2018; Mooney et al., 2016). A high walkability score (on a scale of 0 to 100) signifies that daily errands can be easily performed on foot, while lower scores indicate a neighborhood’s automobile dependence.
Demographic variables for each census block group in Baltimore City (n=653), including population totals and median household income, were taken from 2014 Census estimates (U.S. Census Bureau, n.d.). Increased population density and median household income have been associated with reduced pedestrian injury risk in previous research (Clifton et al., 2009; Ewing and Dumbaugh, 2009; Mohamed et al., 2013; Morency et al., 2012). Population density was calculated by taking the total population of each census block group and dividing by the area of the census block group in square miles.
Data Analyses
Statistical Analysis.
Locations of pedestrian injuries, alcohol outlets, and food stores were geocoded and mapped using ArcGIS 10.4. BCFD provided either street addresses or intersections to which an ambulance was sent for an injured pedestrian, and this location was geographically coded to latitude and longitude points. Alcohol and food outlets were geographically coded to latitude and longitude points using street addresses. All injury and outlet locations were successfully coded in this manner and then aggregated to the census block group level. The outcomes of interest were count of each type of retail outlet per census block group. We performed negative binomial regression in R 3.3, analyzing the counts of pedestrian injuries per block group, while adding each control variable in a stepwise fashion. Negative binomial regression derives as an alternative to Poisson regression (the preferred distribution for analyzing count data) that accommodates over-dispersion. Initially, we estimated four separate models comparing the relationship between pedestrian injury and off-premise alcohol outlets (model 1), on-premise alcohol outlets (model 2), corner stores (model 3) and convenience stores (model 4). Each model controlled for population density, percent of vacant lots, traffic volume lag, median household income, and Walk Score. To test if alcohol outlet type differently impacted neighborhood pedestrian injury rate, we calculated a model with all alcohol outlets (alcohol model 1) and then stratified by outlet type (alcohol model 2). We then included all alcohol and food outlet types in the model to assess if food outlets attenuated the relationship between alcohol outlets and pedestrian injury (full model). For each model, we calculated Residual Moran’s I (RMI) to assess residual spatial variation not accounted for by the model’s covariates using a queen adjacency spatial weights matrix (Waller and Gotway, 2004) and Akaike’s Information Criterion (AIC) to assess model fit and parsimony.
To calculate the neighborhood pedestrian injury risk attributable to the presence of alcohol outlets and food stores, we compared population count per block group to injured pedestrian count using the attribrisk package in R (Schenck et al., 2014). We calculated the baseline injury risk assuming no alcohol outlets or food stores in Baltimore City but controlling for population density, percent of vacant lots, traffic volume lag, median household income, and Walk Score. We next included either alcohol outlets or food stores and compared the baseline pedestrian injury risk to the outlet-included injury risk.
Missing Data.
Walk Scores were only available for certain neighborhoods, with n=33 (11.9%) neighborhoods missing Walk Scores; Baltimore’s neighborhood boundaries also do not align with block group borders. We performed ordinary kriging to estimate a city-wide map of Walk Score values (Waller and Gotway, 2004). Using a planimetric map of all Baltimore City streets, we assigned a kriged Walk Score value to each street centroid. We then aggregated the centroid values to the block group level to calculate the average estimated Walk Score for each block group.
Sensitivity Analysis.
The downtown neighborhood block group was an outlier for injury, alcohol, and food outlet counts. For example, it contained 40 injured pedestrians and 32 off-premise alcohol outlets; in comparison, the next highest block group contained 13 injuries and 10 off-premise outlets (Figure 1). To assess potential biases associated with clustering, we excluded the downtown block group to check that the injury-outlet relationship was not driven by the excessive number of alcohol or food outlets and injuries in this block group. As we did not have access to the locations of alcohol and food outlets for the counties surrounding Baltimore City, we were unable to test the effects of proximal alcohol and food outlets on our models. We performed a sensitivity analysis by excluding all census block groups bordering the surrounding counties (n=62) and reran our models.
Figure 1.
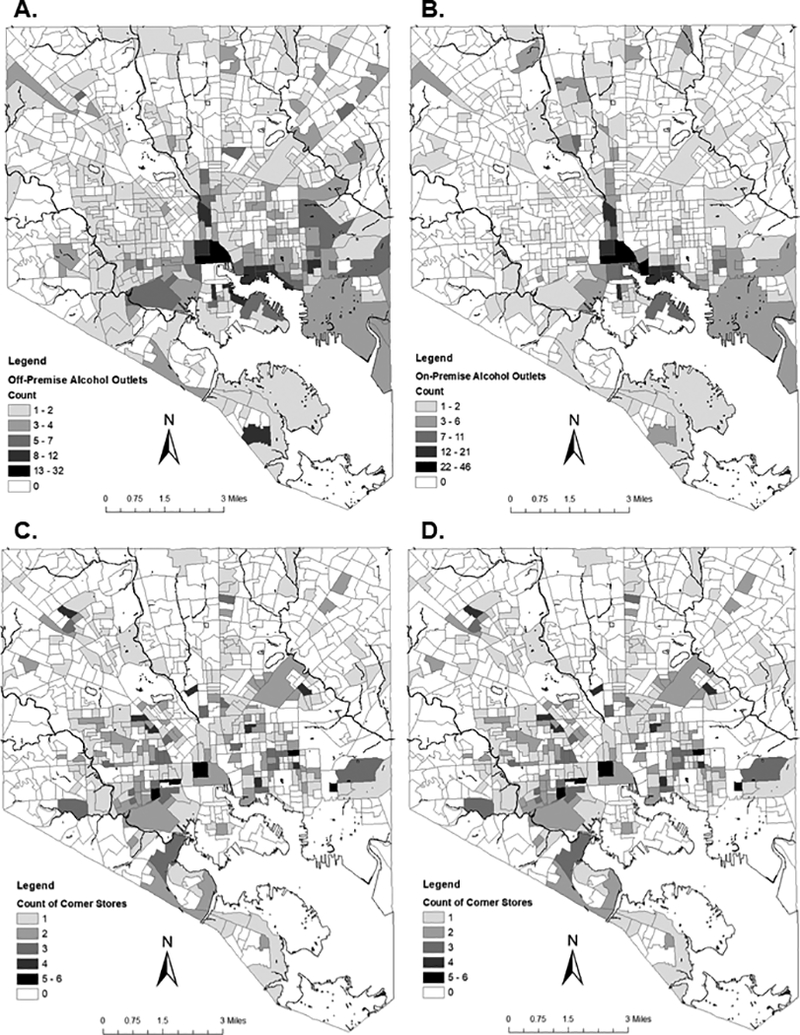
Maps of the distribution of alcohol outlets and small food stores in Baltimore City
Maps A and B: Count of off-premise alcohol outlets and on-premise alcohol outlets in 2014 by census block group (Dara Source: Baltimore City Board of Liquor License Commissioners)
Maps C and D: Count of corner stores and convenience stores in 2013 by census block group (Data Source: Baltimore City Health Department)
Recent guidelines issued by the CDC have urged researchers to implement specific methodological protocols when investigating alcohol outlet density (Centers for Disease Control and Prevention, 2017). Investigating counts of alcohol outlets aggregated to a particular geographic area is still a useful tool, particularly when investigating harms associated with alcohol outlets beyond those attributable to alcohol availability and consumption (Nesoff et al., 2018). In Baltimore City, where new policy will be implemented to limit the number of alcohol outlets that can be physically located near each other (City of Baltimore, 2017), understanding the count of alcohol outlets in a neighborhood may be a useful tool for making policy recommendations and identifying communities most burdened by alcohol outlets and associated harms. However, in support of the CDC guidelines, we have included a sensitivity analysis implementing one of these methods: We divided the count of all types of alcohol and food outlets and injuries by the area of the associated census block group in square miles and reran our full model accordingly.
RESULTS
Table 1 shows the distribution of selected characteristics across block groups. There was an average of 1.30 (sd=2.36) pedestrian injuries per block group. The count of pedestrian injuries across block groups ranged from 0 to 40, with 46% of block groups (n=301) reporting no pedestrian injuries. The highest pedestrian injury count was reported in the downtown neighborhood with 40 injuries, followed by the adjoining block group with 13 injuries (Figure 1). The downtown block group also reported the highest count of alcohol outlets with 32 off-premise outlets and 46 on-premise outlets. The downtown block group also had the highest number of convenience stores with 10; however, downtown only had 2 corner stores. Over half (n=347) of block groups did not contain an off-premise alcohol outlet, while 75% (n=490) did not contain an on-premise outlet; on average, there were 1.11 (sd=2.13) off-premise alcohol outlets and 0.81 (sd=3.10) on-premise outlets per block group. Similarly, 63% (n=411) of block groups did not contain a corner store and 81% (n=533) did not contain a convenience store, with an average of 0.61 (sd=0.99) corner stores and 0.29 (0.80) convenience stores per block group.
Table 1.
Description of selected characteristics by census block group, Baltimore City, 2014 (n=653)
| Variable by Block Group | N | Min. | Max. | Mean | SD |
|---|---|---|---|---|---|
| Pedestrian Injury count | 848 | 0 | 40 | 1.30 | 2.36 |
| Alcohol Outlet count | 1,264 | 0 | 82 | 1.94 | 4.97 |
| Outlets for off-premise consumption | 726 | 0 | 32 | 1.11 | 2.13 |
| Outlets for on-premise consumption | 530 | 0 | 46 | 0.81 | 3.10 |
| Corner Stores | 398 | 0 | 6 | 0.61 | 0.99 |
| Convenience Stores | 192 | 0 | 10 | 0.29 | 0.80 |
| Population density (per square mile in 1,000 residents) | -- | 0 | 95.16 | 13.72 | 9.94 |
| Percent of all lots that are vacant (%) | -- | 0 | 49.53 | 7.02 | 9.65 |
| Median Household income (in $1,000s) | -- | 0 | 224.43 | 44.81 | 27.72 |
| Mean daily traffic volume (in 1,000 vehicles) | -- | 0.07 | 33.34 | 9.71 | 5.13 |
| Walk Score | -- | 26.35 | 97.03 | 69.16 | 14.89 |
All types of alcohol outlets and food outlets were significant predictors of neighborhood pedestrian injury rate in univariable analysis (p<0.001) (Table 2). In multivariable analysis that controlled for population density, percent of vacant lots, traffic volume lag, median household income, and Walk Score, off-premise (Table 2, model 1) and on-premise outlets (Table 2, model 2) were both significant predictors of neighborhood pedestrian injury rate(p<0.001), with off-premise outlets showing a stronger effect size compared to on-premise outlets (IRR=1.143, 95% CI=(1.100, 1.192) vs. IRR=1.055, 95%CI=(1.033, 1.081)). Model 2 had significant unexplained spatial variation (RMI=0.0578, p=0.0034) while model 1 did not (RMI=0.0211, p=0.15); model 2 also had worse fit compared to model 1 (AICs=1921 and 1897, respectively). Corner stores also had a strong effect size (IRR=1.214, 95% CI=(1.112, 1.327), p<0.001) but significant unexplained spatial variation (RMI=0.0582, p=0.0028) and poor model fit compared to both alcohol outlet types (AIC=1930). Convenience stores had the strongest effect size (IRR=1.349, 95%CI=(1.243, 1.475)); residual unexplained variation was marginally insignificant (RMI=0.0326, p=0.0595) and model fit was slightly worse than model 1 (AIC=1900).
Table 2.
Univariable and multivariable results for spatial modeling (n=653)
| Variable | Unadjusted IRR (p) |
Model 1* IRR (p) |
Model 2* IRR (p) |
Model 3* IRR (p) |
Model 4* IRR (p) |
Alcohol model 1* IRR (p) |
Alcohol model 2* IRR (p) |
Full Model* IRR (p) |
|---|---|---|---|---|---|---|---|---|
| All alcohol outlets | 1.072 (<0.001) | 1.046 (<0.001) | ||||||
| Off-premise alcohol outlets | 1.213 (<0.001) | 1.143 (<0.001) | 1.168 (<0.001) | 1.123 (<0.001) | ||||
| On-premise alcohol outlets | 1.084 (<0.001) | 1.055 (<0.001) | 0.978 (0.281) | 0.972 (0.194) | ||||
| Corner Stores | 1.375 (<0.001) | 1.214 (<0.001) | 1.080 (0.124) | |||||
| Convenience Stores | 1.427 (<0.001) | 1.349 (<0.001) | 1.213 (0.002) | |||||
| Population density | 0.985 (0.0122) | 0.979 (<0.001) | 0.975 (<0.001) | 0.966 (<0.001) | 0.981 (0.001) | 0.977 (<0.001) | 0.979 (<0.001) | 0.981 (0.002) |
| Vacant lots | 1.020 (<0.001) | 1.016 (<0.001) | 1.017 (<0.001) | 1.009 (0.133) | 1.020 (<0.001) | 1.017 (<0.001) | 1.015 (0.007) | 1.016 (0.006) |
| Median household income | 0.992 (<0.001) | 0.992 (<0.001) | 0.992 (<0.001) | 0.994 (0.004) | 0.994 (0.003) | 0.992 (<0.001) | 0.992 (<0.001) | 0.993 (0.002) |
| Traffic volume (time lagged) | 1.100 (<0.001) | 1.076 (<0.001) | 1.074 (<0.001) | 1.080 (<0.001) | 1.069 (<0.001) | 1.073 (<0.001) | 1.077 (<0.001) | 1.071 (<0.001) |
| Walk Score | 1.028 (<0.001) | 1.018 (<0.001) | 1.022 (<0.001) | 1.027 (<0.001) | 1.024 (<0.001) | 1.020 (<0.001) | 1.023 (<0.001) | 1.019 (<0.001) |
Note: From negative binomial regression
Adjusted for other covariates in the column
In the alcohol-only models (Table 2), each unit increase in the number of alcohol outlets was associated with a 4.6% increase in neighborhood pedestrian injury rate (IRR=1.046, 95%CI=(1.030, 1.065), p<0.001). When we stratified by alcohol outlet type (alcohol model 2), off-premise alcohol outlets attenuated the relationship between on-premise alcohol outlets and pedestrian injury. On-premise outlets became protective of pedestrian injury (IRR=0.978, 95% CI=(0.946, 1.010)), but this relationship was not significant (p=0.281). Compared to model 1, the strength of the association between off-premise alcohol outlets and pedestrian injury rate increased (IRR=1.168, 95%CI=(1.111, 1.230), p<0.001).
In the full model (Table 2), off-premise alcohol outlets (IRR=1.123, 95%CI=(1.065, 1.184), p<0.001) and convenience stores (IRR=1.213, 95%CI=(1.099, 1.342), p=0.002) remained significant, with convenience stores reporting the largest effect size but off-premise alcohol outlets reporting the smallest p-value. On-premise outlets (IRR=0.972, 95%CI=(0.940, 1.004), p=0.194) and corner stores (IRR=1.080, 95%CI=(0.992, 1.177), p=0.124) were not significant predictors in the full model. This model reported no significant residual spatial variation (RMI=0.0008, p=0.458) and stronger model fit compared to the 4 individual predictor models (AIC=1888).
Corner stores showed possible multicollinearity with vacant lots in the multivariable model (Table 2, model 3) as the effect size of vacant lots was attenuated (IRR=1.009, 95% CI=(0.999, 1.019), p=0.133). Corner stores were correlated with percent of vacant lots (r=0.33, p<0.0001) However, variance inflation factors for this model were below 2, and vacant lots was not attenuated in the full model (IRR=1.016, 95% CI=(1.006, 1.025), p=0.006) while corner stores were insignificant. This indicates that corner stores may be a proxy measure for neighborhood disorder.
In the simulated case-control study for the full model, the pedestrian injury risk attributable to off-premise alcohol outlets was 4.9% (95% CI=(0.3, 8.9)) or 41 extra injuries over baseline. The risk attributable to convenience stores was 7.2% (95%CI=(4.1, 10.1)) or 61 extra injuries. As on-premise outlets and corner stores were not significant, their attributable risk was not calculated.
As part of sensitivity analyses, the removal of the downtown block group was found to strengthen the association between pedestrian injury rate and off-premise alcohol outlets (IRR=1.142, p<0.001) and convenience stores (IRR=1.245, p<0.001); model fit also improved (AIC=1869). However, RMI became marginally significant (RMI=0.0355, p=0.0458), indicating potential spatial variation unexplained by the covariates. On-premise alcohol outlets (IRR=0.981, p=0.383) and corner stores (IRR=1.065, p=0.228) remained insignificant. After removing all census block groups which bordered the counties contiguous to Baltimore City, we found alcohol outlets remained significantly associated with pedestrian injury rate (IRR=1.121, p<0.001) but convenience stores were no longer significant (IRR=1.122, p=0.095); on-premise alcohol outlets (IRR=0.975, p=0.24) and corner stores (IRR=1.085, p=0.097) remained insignificant. Further, the sensitivity analysis dividing all counts by census block group area found that off-premise alcohol outlets remained significantly associated with pedestrian injury rate (IRR=1.007, p=0.027) but convenience stores (IRR=1.017, p=0.125), on-premise alcohol outlets (IRR=0.99, p=0.62 ), and corner stores (IRR=1.006, p=0.13 ) were not significant.
DISCUSSION
The objective of this study was to compare pedestrian injury rate around alcohol outlets to the rate around other, similar retail outlets that do not sell alcohol. Off-premise alcohol outlets were significant predictors of neighborhood pedestrian injury risk when controlling for a variety of neighborhood factors, including other types of retail establishments such as convenience stores and corner stores. Each increase in the number of off-premise alcohol outlets was associated with a 12.3% increase in the neighborhood rate of pedestrian injuries in the full model. In the simulated case-control study, 4.9% of injuries could be attributed to neighborhood presence of off-premise alcohol outlets, when controlling for neighborhood features and convenience stores.
Off-premise alcohol outlets showed a strong association with neighborhood injury rate. Models with off-premise alcohol outlets also had no significant unexplained spatial variation, indicating that off-premise alcohol outlets are a potentially important predictor of neighborhood pedestrian injury rate. If the location of alcohol outlets in areas of dense retail opportunity had explained the association between alcohol outlets and injuries, then we would have expected this relationship to become nonsignificant when controlling for food outlets. In contrast, we found that one or both types of food outlets became nonsignificant when controlling for off-premise alcohol outlets depending on the method of analysis used or when controlling for edge effects. It is unclear why convenience stores were significantly associated with pedestrian injury rate in the count models and corner stores were not. Corner stores and off-premise alcohol outlets are both located in more resource-deprived areas and neighborhoods with higher rates of crime and disorder, while convenience stores tend to be located in wealthier areas (Furr-Holden et al., 2016; LaVeist and Wallace, 2000; Morland et al., 2002). Convenience stores are also larger than corner stores and tend to be located at busy intersections; their size and location may attract more pedestrian traffic than corner stores, but these factors have not been studied previously. Understanding the mechanisms by which various retail establishments differentially impact pedestrian injury risk is a potentially important area for future inquiry.
We also compared pedestrian injury rate around alcohol outlets licensed for on- and off-premise consumption. Similar to studies of violent injury (Furr-Holden et al., 2016), off-premise alcohol outlets were more strongly associated with neighborhood pedestrian injury rate than on-premise outlets. When both types of alcohol outlets were present in the model, we found that on-premise outlets were not significant predictors of pedestrian injury rate. Previous studies of pedestrian injury have combined alcohol outlet types (DiMaggio et al., 2016; Treno et al., 2007), which may limit the ability to understand the specific impact of these neighborhood features on pedestrian injury rate. Stratifying by alcohol outlet type may also help researchers detect the mechanisms by which alcohol outlets contribute to neighborhood injury risk. Nesoff and colleagues (2018) propose a conceptual model detailing the structural/environmental factors, interpersonal relationships, and individual cognitive and biological events which may differently influence pedestrian and driver behavior around on- and off-premise alcohol outlets. Future inquiry will further explore the different roles of off- and on-premise outlets in pedestrian injury risk.
Limitations
This study is cross-sectional and, therefore, does not allow for discussion of changes in the injury risk environment over time. We were unable to consistently identify alcohol- or drug-involved pedestrian crashes as these indicators were rarely recorded by EMS staff. It is possible that intoxication confounds the relationship between neighborhood pedestrian injury risk and retail outlet type; this association will be further investigated in future studies. Neighborhoods with more alcohol outlets may be visited by people looking to purchase or consume alcohol, and this alcohol-related traffic may account for some of the injury risk in areas where alcohol outlets are located (Gruenewald, 2007; Pollack et al., 2005). As we did not have access to the pedestrians’ residential addresses, non-residents may be included. However, previous studies have shown that the majority of pedestrians are struck within a mile of their home (Anderson et al., 2012; Haas et al., 2015), suggesting that injured pedestrians are representative of the neighborhoods in which they are struck. While the use of delineated geographic units has utility when discussing the burden of alcohol outlets and associated harms in a specific neighborhood, these methods are not without limitations. The boundaries of administrative geographic units such as census block groups have been delineated for purposes other than the specific relationships under study and, consequently, may be non-uniform in shape, poorly correspond to the lived experiences of residents, or impose neighborhood scale that is inappropriate for the subjects being studied (Branas et al., 2009). Furthermore, alcohol outlets are assumed to be dispersed evenly throughout each geographic unit; clustering of alcohol outlets within a geographic unit may attract drinkers, potentially impacting the association between outlets and injuries. Future studies will explore the relationship between alcohol outlets and pedestrian injury using spatial interaction methods.
Conclusions
Off-premise alcohol outlets are associated with pedestrian injury rate, even when controlling for other retail locations. This study provides new information in disentangling the mechanisms by which the neighborhood environment around alcohol outlets and other retail establishments influence pedestrian injury risk. Findings reinforce the unique importance of alcohol outlets in understanding neighborhood pedestrian injury risk and may provide evidence for informing policy on liquor store licensing, zoning, and enforcement.
ACKNOWLEDGEMENTS
This work was supported by the National Institute on Alcohol Abuse and Alcoholism (Grant Numbers F31AA023716 and R01AA024941) and the National Institute on Drug Abuse (Grant Numbers T32DA031099 and R34DA034314). Food outlet data were provided by the Johns Hopkins Center for Livable Future. The authors thank Alex Freed and Brian Weir for their help in preparing this manuscript.
REFERENCES
- Anderson CL, Dominguez KM, Hoang T V, Rowther AA, Carroll MC, Lotfipour S, Hoonpongsimanont W, Chakravarthy B (2012) An Analysis of Distance from Collision Site to Pedestrian Residence in Pedestrian versus Automobile Collisions Presenting to a Level 1 Trauma Center. Ann Adv Automot Med 56:31–6. [PMC free article] [PubMed] [Google Scholar]
- Baltimore City Department of Planning (2009) Alcohol Outlet Density Reduction in Baltimore City: Summary. Available at: http://www.rewritebaltimore.org/pdf/AlcoholOutletDensityReduction.pdf
- Bivand RS, Pebesma E, Gomez-Rubio V (2013) Applied Spatial Data Analysis with R, 2nd ed. New York, Springer. [Google Scholar]
- Branas CC, Elliott MR, Richmond TS, Culhane DP, Wiebe DJ (2009) Alcohol consumption, alcohol outlets, and the risk of being assaulted with a gun. Alcohol Clin Exp Res 33:906–915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Branas CC, Richmond TS, Ten Have TR, Wiebe DJ (2011) Acute alcohol consumption, alcohol outlets, and gun suicide. Subst Use Misuse 46:1592–1603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Branas CC, Rubin D, Guo W (2012) Vacant properties and violence in neighborhoods. ISRN Public Health 1–9. [DOI] [PMC free article] [PubMed]
- Campbell CA, Hahn R, Elder R, Brewer R, Chattopadhyay S, Fielding J, Naimi TS, Toomey T, Lawrence B, Middleton JC (2009) The effectiveness of limiting alcohol outlet density as a means of reducing excessive alcohol consumption and alcohol-related harms. Am J Prev Med 37:556–69. [DOI] [PubMed] [Google Scholar]
- Casagrande SS, Franco M, Gittelsohn J, Zonderman AB, Evans MK, Fanelli Kuczmarski M, Gary-Webb TL (2011) Healthy food availability and the association with BMI in Baltimore, Maryland. Public Health Nutr 14:1001–1007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (2017) Guide for Measuring Alcohol Outlet Density. Available at: https://www.cdc.gov/alcohol/pdfs/CDC-Guide-for-Measuring-Alcohol-Outlet-Density.pdf
- City of Baltimore (2017) Council Bill 12–0152. §14–336.
- City of Baltimore (n.d.) Open Baltimore. Available at: https://data.baltimorecity.gov/
- Clifton KJ, Burnier C V., Akar G (2009) Severity of injury resulting from pedestrian–vehicle crashes: What can we learn from examining the built environment? Transp Res Part D 14:425–436. [Google Scholar]
- Cunradi CB (2010) Neighborhoods, alcohol outlets and intimate partner violence: addressing research gaps in explanatory mechanisms. Int J Environ Res Public Health 7:799–813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dai D, Taquechel E, Steward J, Strasser S (2010) The impact of built environment on pedestrian crashes and the identification of crash clusters on an urban university campus. West J Emerg Med 11:294–301. [PMC free article] [PubMed] [Google Scholar]
- DiMaggio C, Mooney S, Frangos S, Wall S (2016) Spatial analysis of the association of alcohol outlets and alcohol-related pedestrian/bicyclist injuries in New York City. Inj Epidemiol 3:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Escobedo LG, Ortiz M (2002) The relationship between liquor outlet density and injury and violence in New Mexico. Accid Anal Prev 34:689–694. [DOI] [PubMed] [Google Scholar]
- Ewing R, Dumbaugh E (2009) The Built Environment and Traffic Safety: A Review of Empirical Evidence. J Plan Lit 23:347–367. [Google Scholar]
- Friedman G (2015) Alcohol Outlet Density Reduction: Setting the Record Straight. Citizens Plan Hous Adm. Available at: http://www.cphabaltimore.org/2015/09/alcohol-outlet-density-reduction-setting-the-record-straight/
- Furr-Holden CDM, Milam AJ, Nesoff ED, Johnson RM, Fakunle DO, Jennings JM, Thorpe RJ (2016) Not in My Back Yard: A Comparative Analysis of Crime Around Publicly Funded Drug Treatment Centers, Liquor Stores, Convenience Stores, and Corner Stores in One Mid-Atlantic City. J Stud Alcohol Drugs 77:17–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garvin E, Branas C, Keddem S, Sellman J, Cannuscio C (2013) More than just an eyesore: local insights and solutions on vacant land and urban health. J Urban Heal 90:412–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grubesic TH, Pridemore WA, Williams DA, Philip-Tabb L (2013) Alcohol Outlet Density and Violence: The Role of Risky Retailers and Alcohol-Related Expenditures. Alcohol Alcohol 48:613–619. [DOI] [PubMed] [Google Scholar]
- Gruenewald PJ (2007) The spatial ecology of alcohol problems: niche theory and assortative drinking. Addiction 102:870–8. [DOI] [PubMed] [Google Scholar]
- Haas B, Doumouras AG, Gomez D, de Mestral C, Boyes DM, Morrison L, Nathens AB (2015) Close to home: an analysis of the relationship between location of residence and location of injury. J Trauma Acute Care Surg 78:860–865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haering S, Franco M (2010) The Baltimore City Food Environment. Baltimore, Maryland, Center for a Livable Future. [Google Scholar]
- Han S, Branas CC, MacDonald JM (2016) The Effect of a Sunday Liquor-Sales Ban Repeal on Crime: A Triple-Difference Analysis. Alcohol Clin Exp Res 40:1111–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jennings JM, Milam AJ, Greiner A, Furr-Holden CDM, Curriero FC, Thornton RJ (2014) Neighborhood alcohol outlets and the association with violent crime in one mid-Atlantic City: the implications for zoning policy. J Urban Heal 91:62–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LaScala EA, Johnson FW, Gruenewald PJ (2001) Neighborhood Characteristics of Alcohol-Related Pedestrian Injury Collisions: A Geostatistical Analysis. Prev Sci 2:123–134. [DOI] [PubMed] [Google Scholar]
- Lassarre S, Papadimitriou E, Yannis G, Golias J (2007) Measuring accident risk exposure for pedestrians in different micro-environments. Accid Anal Prev 39:1226–1238. [DOI] [PubMed] [Google Scholar]
- LaVeist TA, Wallace JM (2000) Health risk and inequitable distribution of liquor stores in African American neighborhood. Soc Sci Med 51:613–617. [DOI] [PubMed] [Google Scholar]
- Live Baltimore (2018) Discover Baltimore City Neighborhoods. Available at: https://livebaltimore.com/neighborhoods/
- Maryland Department of Planning (n.d.) MdPropertyView. Available at: http://planning.maryland.gov/OurProducts/downloadFiles.shtml
- Maryland State Highway Administration (n.d.) GIS Traffic Count Data. Traffic Monit Syst. Available at: http://www.roads.maryland.gov/Index.aspx?PageId=251 Accessed June 24, 2016.
- Milam AJ, Furr-Holden CD, Cooley-Strickland MC, Bradshaw CP, Leaf PJ (2014) Risk for exposure to alcohol, tobacco, and other drugs on the route to and from school: the role of alcohol outlets. Prev Sci 15:12–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miranda-Moreno LF, Morency P, El-Geneidy AM (2011) The link between built environment, pedestrian activity and pedestrian-vehicle collision occurrence at signalized intersections. Accid Anal Prev 43:1624–34. [DOI] [PubMed] [Google Scholar]
- Mohamed MG, Saunier N, Miranda-Moreno LF, Ukkusuri S V (2013) A clustering regression approach: A comprehensive injury severity analysis of pedestrian-vehicle crashes in New York, US and Montreal, Canada. Saf Sci 54:27–37. [Google Scholar]
- Mooney SJ, DiMaggio CJ, Lovasi GS, Neckerman KM, Bader MDM, Teitler JO, Sheehan DM, Jack DW, Rundle AG (2016) Use of Google Street View to Assess Environmental Contributions to Pedestrian Injury. Am J Public Health 106:462–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morency P, Gauvin L, Plante C, Fournier M, Morency C (2012) Neighborhood Social Inequalities in Road Traffic Injuries: The Influence of Traffic Volume and Road Design. Am J Public Health 102:1112–1119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morland K, Wing S, Diez Roux A, Poole C (2002) Neighborhood characteristics associated with the location of food stores and food service places. Am J Prev Med 22:23–29. [DOI] [PubMed] [Google Scholar]
- National Center for Statistics and Analysis (2017) Pedestrians: 2015 Data (Traffic Safety Facts. Report No. DOT HS 812 375), U.S. Department of Transportation. Washington, D.C., National Highway Traffic Safety Administration. [Google Scholar]
- Nesoff ED, Milam AJ, Pollack KM, Curriero FC, Bowie J V, Knowlton AR, Gielen AC, Furr-Holden DM (2018) Neighbourhood alcohol environment and injury risk: a spatial analysis of pedestrian injury in Baltimore City. Inj Prev. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollack CE, Cubbin C, Ahn D, Winkleby M (2005) Neighbourhood deprivation and alcohol consumption: does the availability of alcohol play a role? Int J Epidemiol 34:772–80. [DOI] [PubMed] [Google Scholar]
- Schenck L, Atkinson E, Crowson C, Therneau T (2014) attribRisk: Estimates population attributable risk and confidence intervals R package version 0.1. [Google Scholar]
- Schonlau M, Scribner R, Farley TA, Theall KP, Bluthenthal RN, Scott M, Cohen DA (2008) Alcohol outlet density and alcohol consumption in Los Angeles County and Southern Louisiana. Geospat Health 3:91–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schuurman N, Cinnamon J, Crooks VA, Hameed SM (2009) Pedestrian injury and the built environment: an environmental scan of hotspots. BMC Public Health 9:233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scribner R, Theall KP, Ghosh-Dastidar B, Mason K, Cohen D, Simonsen N (2007) Determinants of Social Capital Indicators at the Neighborhood Level: A Longitudinal Analysis of Loss of Off-Sale Alcohol Outlets and Voting. J Stud Alcohol Drugs 68:934–943. [DOI] [PubMed] [Google Scholar]
- State of Maryland (n.d.) One Maryland One Centerline (OMOC) Linear Referencing. MD iMap. Available at: http://imap.maryland.gov/Pages/road-centerlines-linear-referencing.aspx
- Tabb LP, Ballester L, Grubesic TH (2016) The spatio-temporal relationship between alcohol outlets and violence before and after privatization: A natural experiment, Seattle, Wa 2010–2013. Spat Spatiotemporal Epidemiol 19:115–124. [DOI] [PubMed] [Google Scholar]
- Theall KP, Scribner R, Cohen D, Bluthenthal RN, Schonlau M, Farley TA (2009) Social capital and the neighborhood alcohol environment. Health Place 15:323–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Treno AJ, Johnson FW, Remer LG, Gruenewald PJ (2007) The impact of outlet densities on alcohol-related crashes: a spatial panel approach. Accid Anal Prev 39:894–901. [DOI] [PubMed] [Google Scholar]
- U.S. Census Bureau (n.d.) State and County Quick Facts: Baltimore City. Available at: http://quickfacts.census.gov/qfd/states/24/24510.html
- Waller LA, Gotway CA (2004) Applied Spatial Statistics for Public Health Data. Hoboken, NJ, Wiley. [Google Scholar]
- Walsh JM, Flegel R, Atkins R, Cangianelli LA, Cooper C, Welsh C, Kerns TJ (2005) Drug and alcohol use among drivers admitted to a Level-1 trauma center. Accid Anal Prev 37:894–901. [DOI] [PubMed] [Google Scholar]
- Wo JC (2016) Community Context of Crime: A Longitudinal Examination of the Effects of Local Institutions on Neighborhood Crime. Crime Delinq 62:1286–1312. [Google Scholar]