

Abstract
Background:
Objective in root canal preparation is to develop a shape that tapers from apical to coronal, maintaining the original canal shape. With advent of instruments manufactured from nickel-titanium (NiTi) alloys, there was a significant improvement of quality of root canal shaping, with predictable results and less iatrogenic damage.
Aim:
The aim of the study was to evaluate the canal centric ability and apical transportation in apical region of newer NiTi file system in root canal using cone-beam computed tomography (CBCT) on extracted molars.
Materials and Methods:
Root canal of thirty extracted human permanent teeth with mature root apices with 20°–40° of curvature were collected and divided into three groups after initial bio-mechanical preparation: Group 1: canal prepared using ProTaperNext (PTN) file system; Group 2: canal prepared using Mani silk system; and Group 3: canal prepared using V-taper file system. All samples were scanned before and after biomechanical preparation using CBCT. The data collected were evaluated using the Kruskal–Wallis analysis of variance test and Mann–Whitney U-test.
Results:
It was observed that in apical region Group I (PTN) showed significantly lower mean apical transportation and canal centric ability as compared to Group II (Mani Silk) and Group III (V-taper).
Conclusion:
It was concluded that PTN rotary system has no canal transportation and maintained centric ability in comparison to Mani and V-taper rotary file system in apical region of curved root canal.
Keywords: Apical transportation, cone-beam computed tomography, centric ability, nickel-titanium rotary files
Introduction
Since the beginning of modern-day endodontics, there have been numerous concepts, strategies, and techniques for preparing root canals and one of the objectives in root canal preparation is to develop a shape that tapers from apical to coronal, maintaining the original canal shape.[1]
In spite of the design of the file, the number of instruments required and the surprising multitude of techniques advocated, endodontic treatment has typically been approached with optimism for probable success especially in curved root canals. During shaping of curved root canals, several procedural errors can occur including apical transportation, zips, ledges, root perforations, loss of working length, straightening of root canals, or deviation from original path.[2] During enlargement of curved root canal, the use of progressively greater diameter files decreases the angle of curvature, owing to the tendency to move toward the outer wall of the root canal, leading to a noninstrumented inner dentine wall in the apical third which may entail a worse prognosis for treatment.[3,4] The breakthrough in clinical endodontics progressed from utilizing a long series of stainless-steel (SS) hand files and several rotary gates-glidden drills to the integration of nickel-titanium (NiTi) files for shaping canals.
Since inception in 1993 more than 30 current NiTi instrument systems in the market are classified according to their design, shaping characteristics, breakage potential, and clinical performance from generation 1st to generation 5th.[5] The ability to remain centered in root canal system is the most important feature of NiTi instrument as compared to SS instrument. A lower modulus of elasticity allows NiTi files to be placed in curved root canals with less lateral force exerted against the root canal walls.[6] Yet along with this advantage, NiTi also has a straightening tendency, especially in instruments with greater taper and tip.[7]
Centric ability is the ability of an instrument to remain centered in the canal, thus preserving the canal anatomy.[8] Transportation is defined within The Glossary of Endodontic Terms as removal of the root canal dentin on the outer wall of the curve within the apical half of the canal as a result of the tendency of instruments to regain their original straight shape during canal preparation.[9]
Centering ability and transportation of different rotary NiTi files have been compared by different methods. Cone-beam computed tomography (CBCT) imaging provides three-dimensional evaluation without destructing the tooth, is a noninvasive technique for analysis of canal geometry and efficiency of shaping techniques.[10] Using CBCT, it becomes possible to compare the anatomic structure of root canal before and after root canal preparation.
Investigations of the shaping effect of these new NiTi systems with different design features and kinematics are important for understanding how the differences affect their performance. To the best of our knowledge, no other studies have compared the centric ability and apical transportation of these new NiTi systems. Hence, the present study was conducted to compare the centric ability, and apical transportation of three different newer rotary NiTi file system, i.e., Protaper Next (PTN) Densply, Silk from Mani and V taper from SS White in curved root canal.
Materials and Methods
Thirty human permanent mandibular 1st and 2nd molars extracted due to compromised periodontal condition were stored in a 2% thymol solution until use.[7] The teeth with mature apices, curved canals (20°–40° of curvature) were selected. Canal curvature was determined by using Schneider's method.[11] Teeth with immature apices, root resorption, calcified canals, fractured teeth, and teeth with curvature above 40° were excluded from the study.
The Institutional Ethical Committee approval was granted, and the study was commenced on August 2016 and continued for 2 months in Kota, India.
The crown of each selected tooth was removed at the level of the cementum enamel junction using a diamond disc to obtain a root canal measuring 12 mm in length of mesiobuccal canal and the specimens were embedded in acrilic resin employing an endodontic cube [Figure 1a].[7]
Figure 1.
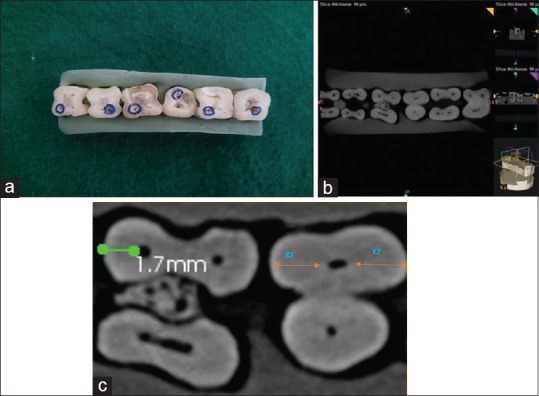
(a) Specimens embedded in acrylic resin. (b) Prepreparation. (c) Postpreparation
Preinstrumentation images were taken by CBCT machine (Alphard VEGA, Asahi Roentgen Ind., Kyoto, Japan) with following settings: 80 kV, 4 mA, and 51 mm × 51 mm field of view and 0.1/voxel (mm) size. All teeth were scanned with their roots being perpendicular to the beam of a CBCT device starting from the apical end of the root [Figure 1b].
A glide path was performed through a size 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland). The working length was determined by subtracting 1 mm from the length at which the file tip extruded apically. RC Help (Prime Dental Products Pvt. Ltd.) was used in all canal preparations, and the root canal was irrigated with 2 ml 2.5% sodium hypochlorite solution after each instrumentation. These 30 mesiobuccal roots were divided into three groups after initial biomechanical preparation till 20# K-file:
Group 1 - The canals were prepared using PTN Densply file system with the sequence ProTaper Universal SX, PTN X1, and X2 at a rotational speed of 350 rpm along with torque values of 200 g/cm
Group 2 - The canals were prepared using Mani Silk file system with 0.08/25 (Orifice opener [OO]). After orifice shaping, the 0.06/20 file is inserted to resistance followed by the 0.06/25 file at the rotational speed of 500 rpm with a torque value of 300 g/cm
Group 3 - The canals were prepared using V Taper SS White file system with the sequence 25 (V08), 30 (V10) for coronal shaping and for apical shaping sequence 30 (V10), 25 (V08) files was used at the rotational speed of 250 rpm with a torque value of 455 g/cm.
After canal shaping, postinstrumentation CBCT scans were performed with similar values and position as preinstrumentation scans [Figure 1c].
Pre-and post-operative CBCT scans were superimposed, and the transportation in the mesiodistal direction was calculated. The horizontal sections were used, and the dimensions were measured by calculating the shortest distance from the periphery of the uninstrumented canal to the periphery of the tooth in both mesial and distal directions and then compared with the values measured from the prepared canals. The canal centering ratio at each level was calculated using the formula:[10]
Centric ability = (X1−X2)/(Y1−Y2) or (Y1−Y2)/(X1−X2)
Transportation at each level was calculated using the formula:[10]
Transportation = (X1−X2) − (Y1−Y2)
X1 represented the shortest mesial distances from the outside of the curved root to the periphery of the un-instrumented canal.
X2 represented the shortest mesial distances from the outside of the curved root to the periphery of the instrumented canal.
Y1 represented the shortest distal distances from the outside of the curved root to the periphery of the un-instrumented canal.
Y2 represented the shortest distal distances from the outside of the curved root to the periphery of the instrumented canal.
Changes in centering ratio and canal transportation data were analyzed using the Kruskal–Wallis analysis of variance test and pairwise comparison was done by Mann–Whitney U-test. The significance level was set at P = 0.05. Statistical analysis was performed with SPSS statistics version 20.0 (SPSS Inc., Chicago, IL, USA).
Result
Mean and standard deviation values of canal centering ratio and canal transportation in apical region for three groups [Tables 1 and 2].
Table 1.
Canal transportation and centric ability ratio of curved canals in apical region
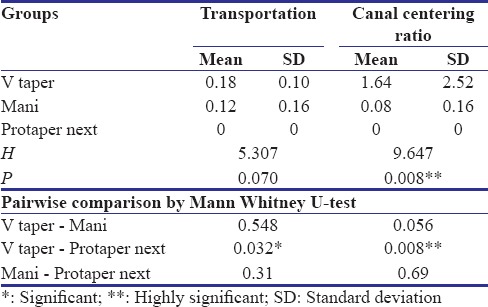
Table 2.
Graphical comparison of three groups
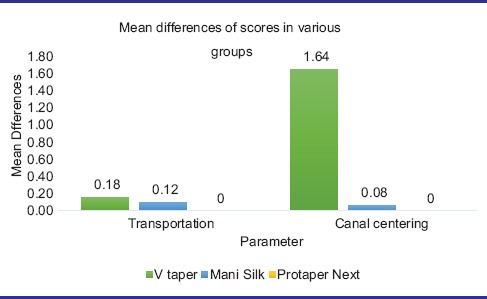
The mean canal centric ability and apical transportation for PTN file group show statistically significant difference when compared with Mani Silk and V-taper file system.
The pair-wise correlation was assessed using Mann-Whitney test in which a significant correlation was observed between V-taper and PTN (P < 0.05) and a nonsignificant correlation was observed with V-taper and Mani and Mani and PTN (P > 0.05).
The PTN showed optimal centering ability and no canal transportation as compared to Silk Mani and V Taper. In pairwise comparison, V Taper– PTN combination is highly significant.
Discussion
Successful endodontic treatment includes proper root canal shaping and effective debridement of the root canal system. The purpose of mechanical instrumentation is to remove the infected soft and hard tissues from the root canal and to create a sufficient taper for the subsequent placement of root filling materials.[12] Maintenance of the original root canal shape is an important goal in root canal preparation and fundamental aspect of endodontic therapy.[7] Regardless of the instrumentation technique, cleaning and shaping procedures invariably lead to dentine removal from the canal walls. However, excessive dentine removal in a single direction within the canal rather than in all directions equidistantly from the main tooth axis causes what is known as “canal transportation.”[13] The occurrence of up to 0.15 mm of root canal transportation has been considered to be acceptable whereas the canal transportation above 0.30 mm may have negative impact on apical seal after obturation of canal.[2] The ability of an instrument to remain centered is essential to provide a correct enlargement and is called the canal centering ability of instrument.
In this study, an evaluation on the effects of three newly developed file systems that have different designs, metallurgies, manufacturing process on the parameters of centering ratio and canal transportation using CBCT imaging was performed.
PTN consists of five files (X1, X2, X3, X4, and X5) with color-coded identification ring of yellow, red, blue, double black, and double yellow on their handles, respectively.[14] PTN files to be used in sequence:
PU SX followed by X1 (17/0.04) and X2 (25/0.06). The X1 and X2 are the shaping and finishing files and X3, X4, and X5 are optional.[15] Both X1 and X2 file system utilizes both an increasing and decreasing percentage tapered design on a single file. This design feature serves to minimize the contact between a file and dentin, which reduces dangerous taper lock and the screw effect while increasing efficiency.[14] Incorporating M-Wire into the mechanical design of PTN improves the resistance to cyclic fatigue, decreases the potential for broken instruments, and increase flexibility. The PTN files produce a unique asymmetrical rotary motion because of which only two edges are in contact with the canal wall at time, leading to an efficient canal preparation.[16] The cross-section is rectangular (off-set) except apical 3 mm which has square cross-section with radial land and noncutting tip. The rotation of the off-centered cross section creates an enlarged space for debris removal, optimizes the canal tracking, and reduces binding. The shaft size of the PTN is small. Therefore, providing better access to the posterior teeth. This is recommended at 350 rpm with a torque of 2.5 N/cm.[15] Clinically, PTN provides three significant advantages (a) Reduced engagement due to swaggering effect which limits undesirable taper lock (b) Affords more cross-sectional space for enhanced cutting, loading, and augering debris and (c) Allows files to cut a bigger envelope of motion compared to a similarly-sized file with a symmetrical mass and axis of rotation.[16]
Mani Silk is packaged into simple pack configuration containing a 0.08/25 OO, 0.06/25, and 0.06/30 instruments (for relatively straight canals). Standard pack configuration containing a 0.08/25 OO, 0.06/20, and 0.06/25 instruments (for moderate curvature). Complex anatomy pack configuration containing a 0.08/25 OO, 0.04/20, and 0.04/25 instruments (For moderate-to-severe curvature). All pack configurations and individual sizes are available in 21 and 25 mm.[17] NiTi alloy of martensitic type makes the file more flexible to accommodate the stress. They are rotated at 500 rpm and 300 g/cm. Files are heat treated from D1 to D10 of the cutting flutes providing increased fracture resistance and flexibility. The cross-section is teardrop shaped. This design channels debris out of the canal efficiently and centers the file while minimizing transportation. This teardrop cross-section also decreases the “screwing-in” effect and simultaneously improves tactile sensation. The Mani Silk files have a constant taper throughout the file length with noncutting tip.[17]
The V-taper rotary system is a series of three variable taper NiTi rotary files that permits deeper apical shape patented with fewer instruments 30 (V10), 25 (V08), and optionally 20 (V06) and is used with crown-down technique. For higher performance modified NiTi alloy Endonol specially formulated in this file system reduces the risk of breakage. V-taper rotary files feature a parabolic cross-section design that attributes of being a highly efficient and flexible instrument while being extremely safe and resistant to fracture with variable pitch, neutral rake angle, no radial land, and noncutting tip.
In previous studies, two experimental models were usually preferred: Simulated canals versus extracted teeth. Using extracted teeth has an advantage over resin blocks because they provide conditions closer to clinical situations.[4] Even the hardness and abrasion behavior of acrylic resin and root dentin are not identical,[18] and the heat generated may soften the resin material.[19] Therefore, we used extracted teeth in this study to compare different file systems.
In this study, to measure canal curvature Schneider's method was used. According to this technique, the angle is obtained by two straight lines. The first line is parallel to the long axis of the root canal and the second line passes through the apical foramen until intersectioning with the first line at the point where the curvature starts.[11] In this study, canal curvature (20°–40°) were included in this study.
Several methods have been used to evaluate the quality of root canal preparations, such as serial sectioning and microscopic evaluation, simulated canals, true tooth training replicas radiographic evaluation and CBCT[20] serial sectioning technique and optical microscopy have been used to evaluate the final shape of root canal preparations. However, when using these methods, part of the specimen structure is lost because there is a need to cut the tooth before the postoperative evaluation.[21] More complex simulated canals, True Tooth training replicas have been introduced recently.[22] These models have five difficulty scales that many factors (i.e., pulp chamber size, canal curvature, apical branching, etc.) determine their difficulty, but these models also have drawbacks such as different hardness of dentin. Radiographic evaluation only allows for two-dimensional evaluation of the root canal[23] CT allows a noninvasive and reproducible three dimensional evaluation of external and internal morphology of the tooth with little radiation. Although the cost is more, we used CBCT in this study as it leads to increased precision, resolution, and the time of exposure of radiation is less.
Ideal canal preparation requires negligible canal transportation with optimally centered preparations. The present study had observed that PTN maintained canal centric curvature and caused no apical transportation when compared with Mani silk file and V-taper file system.
This may be due to PTN modified tip design and a brushing motion, away from external root concavities, to facilitate flute unloading and apical file progression[24] which leads to more centered preparation and its M-wire alloy property which increases flexibility[16] and a reducing taper of PTN file in coronal portion leads to more flexibility in the apical region[25] which causes less apical transportation. Even the apical 3 mm of the PTN instrument has square cross-section which gives more core strength in narrow apical part.[26] This is in correlation with the study conducted by Dhingra et al.,[15] who concluded that PTN exhibited more centered preparation with negligible transportation.
Shenoi et al.[25] concluded that PTN and V-taper showed no significant transportation in apical region and V-taper showed better centering ability than PTN and Hyflex. He attributed this to reduced shaft diameter and less cross-section area of V-taper file. However, this is in contrast to our study where V-taper showed maximum centric ability and canal transportation which may be due to more taper of 25(V08) file used as compared to PTN (25/0.06) and Mani Silk (20/0.06) file system. As more taper of the file leads to increase in canal transportation in the apical region which is in accordance with the study conducted by López et al.,[27] who found that there was increase in the tendency for the canal transportation as the diameter of the file increases.
Wu et al.[28] have shown that PTN caused the least transportation at apical section in severely curved canals and had better shaping ability than Protaper universal and Wave-one. He attributed this to the progressive taper of PTN which makes it more flexible at the apical section and even the microstructure of Ni-Ti alloy of PTN file mostly consisted of martensite phase which displays flexibility and ductility.
In the present study, Mani Silk showed more canal transportation and less centric ability than PTN. It may be due to the constant taper of the Mani Silk rotary file system. A constant increase in taper adds more material to the overall body, leading to an increase in stiffness. Kunert et al.[29] and Gundappa et al.[8] suggested that taper is one of the main factors responsible for canal transportation.
Conclusion
The study concluded that PTN (Dentsply Maillefer, Ballaigues, Switzerland) rotary system has optimal centric ability and no canal transportation in comparison to Mani and V-taper rotary file system. It is one of the few rotary systems that provide quick and safe endodontic preparation. With the limitation of low sample size, all the file system used in the present study showed optimal centric ability and acceptable apical transportation. Hence, further studies with larger sample size are needed to get the more accurate data.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Gergi R, Rjeily JA, Sader J, Naaman A. Comparison of canal transportation and centering ability of twisted files, Pathfile-ProTaper system, and stainless steel hand K-files by using computed tomography. J Endod. 2010;36:904–7. doi: 10.1016/j.joen.2009.12.038. [DOI] [PubMed] [Google Scholar]
- 2.Peters OA. Current challenges and concepts in the preparation of root canal systems: A review. J Endod. 2004;30:559–67. doi: 10.1097/01.don.0000129039.59003.9d. [DOI] [PubMed] [Google Scholar]
- 3.Greene KJ, Krell KV. Clinical factors associated with ledged canals in maxillary and mandibular molars. Oral Surg Oral Med Oral Pathol. 1990;70:490–7. doi: 10.1016/0030-4220(90)90217-g. [DOI] [PubMed] [Google Scholar]
- 4.Schäfer E, Vlassis M. Comparative investigation of two rotary nickel-titanium instruments: ProTaper versus RaCe. Part 1. Shaping ability in simulated curved canals. Int Endod J. 2004;37:229–38. doi: 10.1111/j.0143-2885.2004.00786.x. [DOI] [PubMed] [Google Scholar]
- 5.Serene TP, Adams JD, Saxena A. Nickel-Titanium Instruments: Applications in Endodontics. St. Louis: Ishiaku EuroAmerica; 1995. [Google Scholar]
- 6.Gambill JM, Alder M, del Rio CE. Comparison of nickel-titanium and stainless steel hand-file instrumentation using computed tomography. J Endod. 1996;22:369–75. doi: 10.1016/S0099-2399(96)80221-4. [DOI] [PubMed] [Google Scholar]
- 7.Uroz-Torres D, González-Rodríguez MP, Ferrer-Luque CM. Shaping ability of mtwo and twisted file rotary systems in curved root canals. J Clin Exp Dent. 2012;4:275–80. [Google Scholar]
- 8.Gundappa M, Bansal R, Khoriya S, Mohan R. Root canal centering ability of rotary cutting nickel titanium instruments: A meta-analysis. J Conserv Dent. 2014;17:504–9. doi: 10.4103/0972-0707.144567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Transportation. Chicago: American Association of Endodontists; 2003. American Association of Endodontists. Glossary of endodontic terms. [Google Scholar]
- 10.Gluskin AH, Brown DC, Buchanan LS. A reconstructed computerized tomographic comparison of Ni-Ti rotary GT files versus traditional instruments in canals shaped by novice operators. Int Endod J. 2001;34:476–84. doi: 10.1046/j.1365-2591.2001.00422.x. [DOI] [PubMed] [Google Scholar]
- 11.Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971;32:271–5. doi: 10.1016/0030-4220(71)90230-1. [DOI] [PubMed] [Google Scholar]
- 12.Stern S, Patel S, Foschi F, Sherriff M, Mannocci F. Changes in centring and shaping ability using three nickel-Titanium instrumentation techniques analysed by micro-computed tomography (μCT) Int Endod J. 2012;45:514–23. doi: 10.1111/j.1365-2591.2011.02004.x. [DOI] [PubMed] [Google Scholar]
- 13.Nagaraja S, Sreenivasa Murthy BV. CT evaluation of canal preparation using rotary and hand Ni-Ti instruments: An in vitro study. J Conserv Dent. 2010;13:16–22. doi: 10.4103/0972-0707.62636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ruddle CJ, Machtou P, West JD. The shaping movement: Fifth-generation technology. Dent Today. 2013;32:94, 96–9. [PubMed] [Google Scholar]
- 15.Dhingra A, Banerjee S, Aggarwal N, Yadav V. Canal shaping with ProTaper next: An ex vivo study. Int J Sci Study. 2014;2:1–4. [Google Scholar]
- 16.Chandrasekhar P, Shetty RU, Adlakha T, Shende S, Podar R. A comparison of two NiTi rotary systems, protaper next and silk for root canal cleaning ability (An in vitro study) Indian J Conserv Endod. 2016;1:22–4. [Google Scholar]
- 17.Mounce R. Mani Silk: A new and novel means of predictable canal shaping. Endod Prac. 2015 [Google Scholar]
- 18.Paqué F, Musch U, Hülsmann M. Comparison of root canal preparation using RaCe and ProTaper rotary Ni-Ti instruments. Int Endod J. 2005;38:8–16. doi: 10.1111/j.1365-2591.2004.00889.x. [DOI] [PubMed] [Google Scholar]
- 19.Kum KY, Spängberg L, Cha BY, Il-Young J, Msd, Seung-Jong L, et al. Shaping ability of three ProFile rotary instrumentation techniques in simulated resin root canals. J Endod. 2000;26:719–23. doi: 10.1097/00004770-200012000-00013. [DOI] [PubMed] [Google Scholar]
- 20.Özer SY. Comparison of root canal transportation induced by three rotary systems with noncutting tips using computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111:244–50. doi: 10.1016/j.tripleo.2010.08.017. [DOI] [PubMed] [Google Scholar]
- 21.Kfir A, Tsesis I, Yakirevich E, Matalon S, Abramovitz I. The efficacy of five techniques for removing root filling material: Microscopic versus radiographic evaluation. Int Endod J. 2012;45:35–41. doi: 10.1111/j.1365-2591.2011.01944.x. [DOI] [PubMed] [Google Scholar]
- 22.Aminsobhani M, Ghorbanzadeh A, Dehghan S, Niasar AN, Kharazifard MJ. A comparison of canal preparations by Mtwo and RaCe rotary files using full sequence versus one rotary file techniques; a cone-beam computed tomography analysis. Saudi Endod J. 2014;4:70–6. [Google Scholar]
- 23.Backman CA, Oswald RJ, Pitts DL. A radiographic comparison of two root canal instrumentation techniques. J Endod. 1992;18:19–24. doi: 10.1016/S0099-2399(06)81137-4. [DOI] [PubMed] [Google Scholar]
- 24.Vyver P. Creating a glide path for rotary NiTi instruments: Part one. Int Dent J. 2010;13:6–10. [Google Scholar]
- 25.Shenoi PR, Luniya DA, Badole GP, Makade CS, Kubde R, Khode RT. Comparative evaluation of shaping ability of V-taper 2H, ProTaper next, and HyFlex CM in curved canals using cone-beam computed tomography: An in vitro study. Indian J Dent Res. 2017;28:181–6. doi: 10.4103/ijdr.IJDR_34_16. [DOI] [PubMed] [Google Scholar]
- 26.Vander Vyver PJ, Scianamblo MJ. Clinical guidelines for the use of Protaper Next instruments- part 1. Dent Trib Asia Pac Ed. 2014;10:12–6. [Google Scholar]
- 27.López FU, Fachin EV, Camargo Fontanella VR, Barletta FB, Só MV, Grecca FS, et al. Apical transportation: A comparative evaluation of three root canal instrumentation techniques with three different apical diameters. J Endod. 2008;34:1545–8. doi: 10.1016/j.joen.2008.07.027. [DOI] [PubMed] [Google Scholar]
- 28.Wu H, Peng C, Bai Y, Hu X, Wang L, Li C, et al. Shaping ability of ProTaper universal, WaveOne and ProTaper next in simulated L-shaped and S-shaped root canals. BMC Oral Health. 2015;15:27. doi: 10.1186/s12903-015-0012-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Kunert GG, Camargo Fontanella VR, de Moura AA, Barletta FB. Analysis of apical root transportation associated with ProTaper universal F3 and F4 instruments by using digital subtraction radiography. J Endod. 2010;36:1052–5. doi: 10.1016/j.joen.2010.02.004. [DOI] [PubMed] [Google Scholar]