

Abstract
Morquio patients, in many cases, present with severe tracheal narrowing and restrictive lung problems making them susceptible to high mortality arising from sleep apnea and related complications. Tracheal obstruction with growth imbalance, short neck, adeno and tonsillar hypertrophy, large mandible, and/or pectus carinatum also contributes to the challenges in managing the airway with intubation and extubation due to factors intrinsic to Morquio syndrome. Taken together, these issues lead to serious respiratory distress and life-threatening complications during anesthetic procedures. Furthermore, patients with Morquio syndrome frequently cannot perform standard pulmonary function tests as a result of their distinctive skeletal dysplasia and chest deformity, thus making diagnosis of incipient pulmonary disease difficult. In many cases, conventional spirometry is too difficult for patients to complete, deriving from issues with cooperation or clinical circumstance. Therefore, it is an unmet challenge to assess pulmonary insufficiency with standard pulmonary function test (PFT) with minimal effort. Non-invasive PFT such as respiratory inductance plethysmography, impulse oscillometry system, and pneumotachography were described in Morquio patients as compared with spirometry. Findings from our previous study indicate that these non-invasive tests are a reliable approach to evaluate lung function in a larger range of patients, and provide valuable clinical information otherwise unobtainable from invasive tests. In conclusion, the present study describes the utility of non-invasive (PFT) to accommodate a broad range of patients including intolerance to effort-dependent PFT.
Keywords: Non-invasive pulmonary function test, Morquio syndrome, Impulse oscillometry system, Pneumotachography, Respiratory inductance plethysmography
Introduction
Morquio syndrome (Mucopolysaccharidosis IV, MPS IV) is classified into two different autosomal recessive disorders, Morquio syndrome A (MPS IVA) and Morquio syndrome B (MPS IVB), caused by a deficiency of N-acetylgalactosamine-6-sulfate sulfatase (GALNS) or β-galactosidase (GLB1), respectively1–4. Both enzymes are required for the catabolism of glycosaminoglycan(s) (GAGs): chondroitin-6-sulfate (C6S) and keratan sulfate (KS) for Morquio syndrome A and KS only for Morquio syndrome B1.
Morquio syndrome is characterized by skeletal dysplasia with short stature, spinal cord compression, pectus carinatum, kyphoscoliosis, genu valgum, and pulmonary complications caused by the constant, progressive accumulation of GAG(s) in the lysosomes of bones, cartilage, ligaments, and the extracellular matrix (ECM) (Figure 1)1,5–8.
Figure 1. A 3-year-old patient with severe Morquio Syndrome.
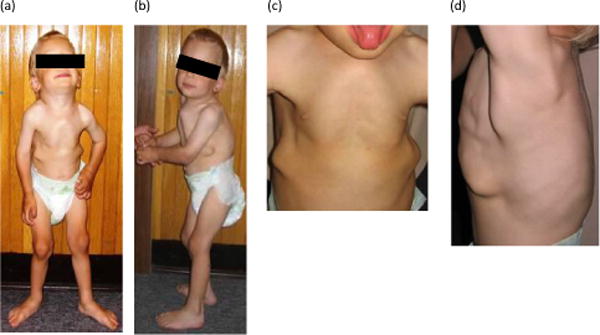
The continuous and progressive buildup of GAGs in the lysosomes of cartilage, ligaments, ECM, and bone, leads to the many clinical manifestations associated with Morquio syndrome8. (a) Genu valgum is exhibited in the knees. (b) Pectus carinatum is visible in the chest and kyphoscoliosis can be seen from the curvature of the spine. (c) A closer examinaton of the chest reveals prominent bone deformity and an additional view of pectus carinatum. (d) Bone deformity and kyphoscoliosis can also be seen from a side view of the patient.
Modified from: Educational CD for Morquio and permitted by Carol Ann Foundation
In patients with a severe phenotype of Morquio syndrome A, spinal cord compression, airway compromise, and later valvular heart disease are the leading causes of morbidity and mortality, attributing to the shortened lifespan of individuals, who often do not survive past their twenties if untreated5.
GAGs are an important component of the extracellular matrix (ECM), which plays a substantial role in the behavior of the lung parenchyma. In the ECM of the lung, GAGs are shown to maintain structure and function, influence tissue repair and remodeling, regulate hydration and water homeostasis, and modulate inflammatory response9. Accumulation of GAGs causes narrowing of the upper airway and leads to progressive cellular, multisystem damage, and successive organ failure or even death8,10–13. GAG deposits are associated with many respiratory manifestations with airway obstruction as the most prominent feature7,8,12.
Proteoglycans (PGs), which are formed by the covalent attachment of GAGs to a protein core, are a major component of the ECM in the lungs9. PGs are implicated in the maintenance of tissues, tissue regulation of water balance, and influencing cell migration14. The balance of the synthesis and degradation of ECM components largely determines the structural integrity of the pulmonary interstitium9. Due to thoracic cage abnormalities, patients with Morquio syndrome often develop restrictive lung profiles11. Respiratory manifestations including narrowing airway in Morquio patients contribute to high mortality rates13 and a high risk during anesthesia5,8,15.
High prevalence of restrictive lung disease and airway obstruction in conjunction with other cardiovascular issues frequently complicates anesthetic procedures5,11,15.
GAG accumulation along the upper airway causes tongue enlargement, adenoidal, tonsillar, and vocal cord hypertrophy, large mandible, short neck, imbalance of growth between spine, rib, and trachea, and consequent bulging and twisted trachea5,12 (Figure 2). This anatomical issue causes difficult airway, making endotracheal intubation/extubation challenging or impossible5,16,17. Typical complications associated with anesthesia include failure to intubate or extubate, cardiac arrest, and possible emergency tracheostomy11,17,18. If severe airway obstruction occurs in a patient with advanced clinical manifestations, hypoxemia, cardiac arrest, and/or obstructive pulmonary edema will be induced in a high probability in intubation or extubation11,17. Profound oxygen desaturation often requires an emergency tracheostomy, a procedure that is difficult in MPS patients due to a short neck, the deep position of the trachea within the neck, and thickened soft tissues11. In patients with Morquio syndrome, respiratory function tests are challenging to perform due to their small body size, skeletal dysplasia, and ambulatory status1. Conventional spirometry assesses static and dynamic volume measurements; however, it relies heavily on the cooperation between the subject and the examiner. Spirometry also cannot be performed on young patients under 5 years old, those who are wheel-chair bound, and post-operative patients suffering from severe muscle weakness1,19, leading to limitation of population available. Rapid, feasible, and accurate non-invasive pulmonary functions tests (PFTs) have been developed to examine tidal breathing in patients unable to cooperate fully as a result of age or clinical circumstance1. These non-invasive PFTs include respiratory inductance plethysmography (RIP), impulse oscillometry (IOS), and pneumotachography (PNT), all of which have been abundantly performed in pediatric populations1.
Figure 2. Airway pathophysiology of Morquio A.
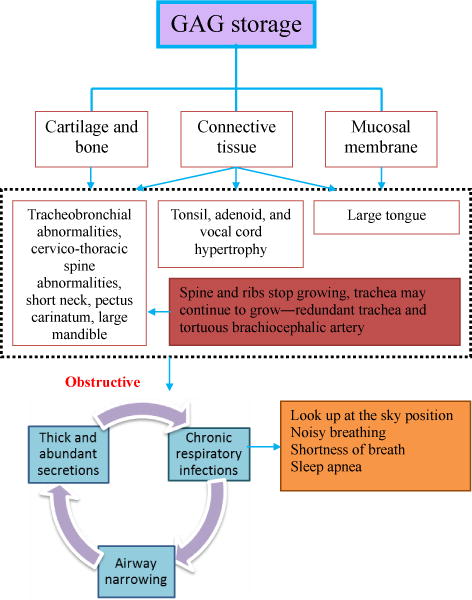
The airway pathophysiology of Morquio A shows the progressive nature of the disease and the presence of severe cycles. Accumulated GAGs alter connective tissue and cartilage, which alters the acquirement of bone mass and disturbs the microarchitecture of cartilage8. Respiratory problems exhibited by Morquio A patients include restrictive and obstructive sequences8. Thoracic cage abnormalities contribute to the restrictive lung, while obstructive lung disease is caused by tracheobronchial anomalies, cervicothoracic spine abnormalities, tortuous brachiocephalic artery, short neck, and a large tongue and mandible, as well as adenoidal, tonsillar, and vocal cord hypertrophy from GAG accumulation. Additionally, Morquio A patients display small nasal passages from thickened mucus membranes and abundant secretions. Chronic upper respiratory infectons further decline the previously diminished airway lumen (8). The look up to the sky positon, sleep apnea, noisy breathing, and shortness of breath are seen in patients with severe obstruction and lead to sudden death as well as difficulties during anesthetic procedures.
Modified from: Educational CD for Morquio and permitted by Carol Ann Foundation
As compared to conventional spirometry, non-invasive PFTs accommodate a broader spectrum of patients, including pediatric, wheel-chair bound, and minimally cooperative patients1,20. In this review article, we have described non-invasive PFTs in patients with Morquio syndrome, compared with invasive tests.
Material and Methods
Invasive PFT
Spirometry
Spirometry (i.e., Medgraphics Ultima PF; BreezeSuite Software; and PreVent Flow Sensor; St. Paul, MN) remains the most common method for assessing pulmonary function19. It is often used when a patient is suspected of having restrictive or obstructive lung disease and can be beneficial in determining the degree of improvement or advancement of respiratory disorders21. However, spirometry requires forceful expiratory and inspiratory maneuvers in which patient cooperation is essential19. Thus, the test is difficult to perform in young and elderly patients, as well as those with physical or cognitive restraints19. The spirometer measures breathing volumes per unit time and allows many physiological measurements to be obtained, with the forced expiratory spirogram as the most useful21. The spirogram reports measurements such as forced vital capacity (FVC), volume expired in the first second (FEV1), and maximum mid-expiratory flow rate (MMEF or FEF25-75%)21. Contrary to using impulse oscillometry system (IOS), it has been shown that the mid-expiratory flow rate does not provide a clear indication of peripheral airway disease20.
To obtain an accurate spirogram, the patient must be seated or standing comfortably with a nose clip applied21. The patient will then inhale as much as possible and when told to do so, exhale as hard and quickly as can be achieved. Three spirometric tracings should be attained, and the greatest FVC measurements are recorded. The spirogram can be interpreted based upon deviations from predicted values established by age, sex, and height21. This interpretation becomes difficult in patients with abnormal height (above or below), such as achondroplasia and other skeletal dysplasias, because minimal reference data exists22.
There are many different types of spirometers including the water-sealed bell, waterless (bellows or rolling seal), and electronic. While the water-sealed bell is the simplest type of spirometer, waterless and electronic spirometers are more convenient and portable; however, they may be less precise21. Due to its large size, the water-sealed bell is used for research purposes, and although it is highly accurate, its performance becomes diminished during FVC breathing because of the inertia of the moving parts23. On the other hand, conventional spirometry often involves the use of a pneumotachographer; however, the associated mouthpiece may modify typical breathing patterns24.
While spirometry can provide a rapid and accurate indication of the presence of lung disease, attention to technique is essential for precise measurements, and additional PFTs are usually required for more detailed assessment21. In a recent study, it was demonstrated that when undergoing spirometry, the predicted forced expiratory volume total (%FEVTOT) in Morquio patients appeared normal until 10 years of age, in which it decreased with age1. It was also found that the higher BMIs in Morquio patients harmfully impact respiratory function. However, in a study done by Morcap, only 66.3% of patients were shown to be compliant with spirometry (FVC), and in our study, only 77.3% of Morquio patients could manage spirometry1.
Non-invasive PFT
a. Respiratory Inductance Plethysmography (RIP)
RIP (Sensormedics, Yorba Linda, CA) is a noninvasive method used to determine the timing and capacity of respiration through analysis of thoracoabdominal movement, concluding the extent to which abdomen and chest excursions are out of phase1,25,26. Developed for use during quiet breathing, RIP measures tidal ventilation and can be operated during everyday activities, including walking24. Inductance coils with bands are positioned to fit comfortably around the ribcage and the addomen1,25,26. RIP measures the current produced by the magnetic field in the coils, which become altered by the volume change of the ribcage or abdomen during ventilation (Figure 3)24–26. The sum of the individual ribcage and abdomen alterations makes up the tidal volume at the opening of the airway26. The RIP technique may be employed using either the uncalibrated or calibrated method25. Uncalibrated RIP provides a measure of phase and thoracoabdominal asynchrony (TAA), requiring the use of a face mask, such as a pneumotachometer, for accurate measurement of ventilation changes1,25. It has been shown in previous studies that chest and abdominal movements can be out of phase perturbing to airway hindrance and other respiratory or lung irregularities1. The calibrated RIP technique does not entail the use of a mouthpiece or face mask; however, fully quantitative calibration involves measurements to be taken using a face mask26. Without the use of a mask or mouthpiece, more accurate readings of respiration patterns can be assessed24. As RIP measures breathing activity without attaching at the airway aperture, it is a particularly useful technique for infants and can be used both postoperatively and in the intensive care unit for further respiratory examination25.
Figure 3. Thoracoabdominal Motion Analysis.
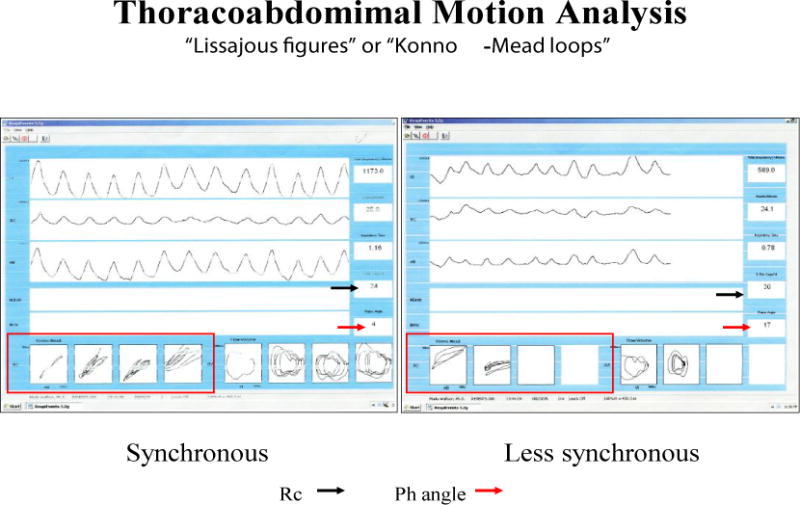
Respiratory Inductance Plethysmography (RIP) tracings demonstrating thoracoabdominal motion during synchronous (phase angle = 4 degrees) and less synchronous (phase angle =17 degrees) breathing. The Lissajous figures (Konno-Mead Loops; red outlines) show the phase shift and the red arrow indicates the phase angle between the rib cage and abdominal compartments.
b. Impulse Oscillometry System (IOS)
Developed by Dubois in 1956, IOS derives from the forced oscillation technique (FOT) and determines the extent of lung disorders19,20,27. IOS (E. Jaeger, Höchberg, Germany) supplies measurements of resistance from the central and peripheral airways, as well as reactance, which is the ability of the air column to move, through the utilization of soundwaves that are superimposed on breathing pattern1,20. Through employing an impulse comprising of different frequencies that pass into the lungs, pressure and air flow changes are induced and measured at the mouthpiece20. Patients undergo testing while sitting, with the head in a neutral position, a nose clip in use, and cheeks supported by the examiner (Figure 4)1,20,27. Due to its rapid, point-of-care and noninvasive nature, IOS requires less cooperation from patients than does conventional spirometry20,27. One of its advantages is that it can be used to detect respiratory anomalies in skeletal dysplasia patients who are young, as well as those unable to perform traditional pulmonary function tests27. It has also been found that IOS may be more predictive than spirometry, especially in determining peripheral airway disease, as it can recognize early deviations in the function of the lung and can further distinguish between small and large airway hindrance19,20.
Figure 4. Impulse Oscillometry System Overview.
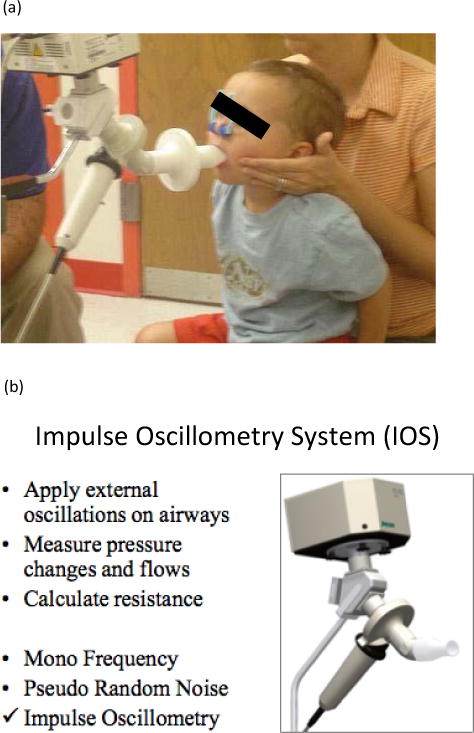
(a) IOS operaton with a patient. (b) Schematc of the Impulse Oscillometry System, IOS (Jaegger, Inc.) showing system components.
c. Pneumotachography (PNT)
First presented by Fleisch in 1925, PNT measures the movement of gas that occurs during respiration. While this method has only recently become more largely acknowledged23, its ability to be performed during anesthesia and respiratory treatment convey its many advantages28. Most importantly, this test has proven to be useful in patients who are noncooperative or unable to stand for spirometric procedures, such as the very young and old29. Due to its sensitivity, PNT quickly and accurately measures air flow and volume and is based on Poiseuille’s Law, which states that volumetric flow rate is directly proportional to the pressure gradient generated. Thus, the pneumotachograph must consider changes in temperature, pressure, humidity, and composition of respiratory gases for accurate measurements, which can be accomplished with calibration23,28. As shown in Figure 5, air flow, end tidal CO2, and oximetry measurements can be obtained by an integrated pneumotach (PNT) system such as the CO2SMO (Novametrix Medical Systems, Wallingford, CT) for simultaneous, real time measurements.
Figure 5. CO2SMO Respiratory Profle Monitor.
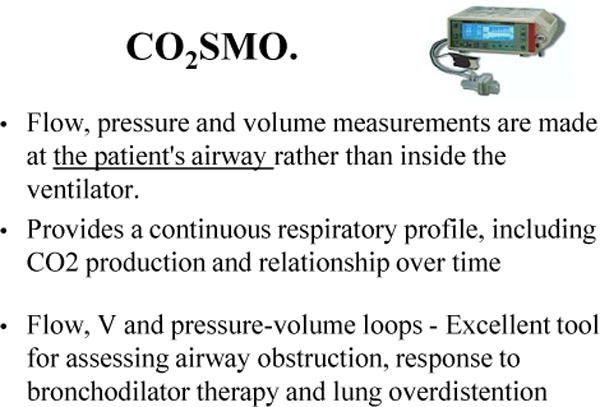
Integrated pneumotach (PNT) System including end tidal CO2 and pulse oximetry sensors for monitoring simultaneous, real time measurements of flow, tidal volume, end tidal CO2 and oxygen saturation.
A differential manometer or pressure transducer measures the pressure gradient on both sides of the resistive element23,29. This difference in pressure across the resistance is kept at a small amount to prevent the resistance from significantly affecting the flow of gas23. Pneumotachography via a face mask is non-invasively placed over the nose and mouth to record measurements over time, and the mask is checked for leaks1. The patient must have a leak-free connection to the device to ensure that flow and volume is measured by direct means. Since a change in breathing pattern alters volume and air flow, an accurate representation of these parameters requires measurements to be taken over a designated period, typically 10 uniform breaths23. The pneumatograph frequently uses two different head types. The resistance of the Fleisch head comprises a bundle of parallel tubes, in which the pressure drop may be elevated by decreasing the diameter of the tubes. Heating the coil around this apparatus prevents condensation from moist gases and compensates for temperature differences between inspiratory and expiratory gas temperatures. The Silverman-Lilly head can attain laminar flow over a wide range due to its trumpet-like shape. The resistive element is provided by a metal screen, and a V-shaped incision in the screen avoids condensation. If the size of the head is too big, a large dead space and small pressure signal may occur23. A large dead space allows both inspired and expired gases to pass through the patient’s airways while a properly sized pneumotachograph head minimally affects lung function, and is thus well endured by patients with low breathing capacity, such as infants28.
Results
In a recent study all of the Morquio patients could perform RIP1. Measures of phase angle, and percent rib cage (%RC) were taken, and when compared with healthy values, were found to be within normal limits (Figure 6); however, when these limits are out of range, it indicates dysfunction of the chest wall and lungs1. RIP also indicated that if stature is corrected, skeletal dysplasia, a characteristic of Morquio syndrome, has minimal impact on declining respiratory function with age, shown by higher values of peripheral resistance in younger patients1.
Figure 6. RIP summary.
22 patients were analyzed. Phase angle and %Rib cage demonstrated normal breathing synchrony. No normative data exist for patients with small stature and skeletal dysplasia. Modified from: Kubaski et al., 2015.
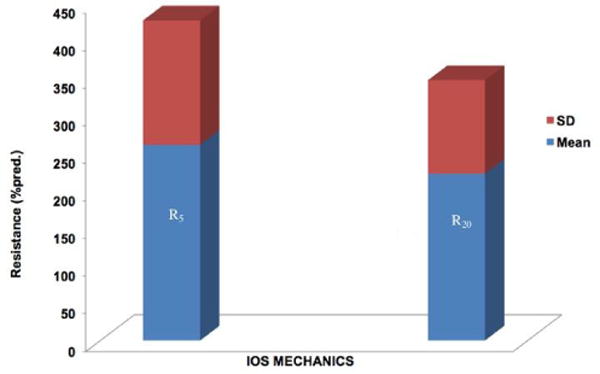
In the same study, 81.8% of Morquio patients could undergo IOS1. A measurement of IOS resistance revealed that peripheral and central airway resistance is not in relation to age; however, some values were higher than predicted as compared to normal values from patients with average stature (Figure 7). However, there was an appropriate correlation between IOS resistance and vital capacity (lung volumes) in these Morquio patients; thus, those patients with smaller lung volumes had higher resistance values1.
Figure 7. Summarized IOS results.
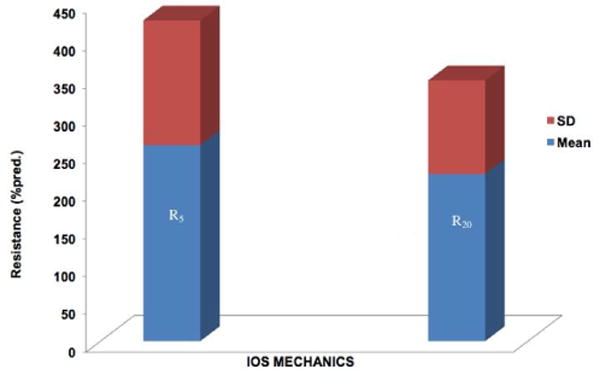
18 Patients were evaluated. Normal range: less than 200%. Higher resistances were seen in younger patients.
Modified from: Kubaski et al., 2015.
Similar to RIP, all of the Morquio patients were compliant with PNT1. It was found that the air flow, end tidal CO2, and oximetry measurements from PNT were normal when compared with age and gender matched controls1. As shown all Morquio patients do not always exhibit restrictive and obstructive lung disease, as patients can have small but properly functioning lungs.
Discussion
Morquio patients exhibit a shortened lifespan due to spinal cord impediments, respiratory complications or heart valve disease, leading to high anesthetic risk in patients with Morquio syndrome5,17. Multiple surgical procedures involving anesthesia are often required for the management of Morquio syndrome; however, surgical intervention may lead to severe stress including serious respiratory distress or arrest, cardiac arrest, or even death or paralysis11. Tracheal obstruction is often recognized as part of the natural progression of Morquio syndrome or may even go unrecognized until complications arise in the form of life-threatening sleep apnea or during anesthetic procedures5,17. While a tracheostomy is often performed to save difficult airway, to maintain it in a Morquio patient proves difficult due to their short neck, tortuous trachea, inability to hyperextend the neck, and fixed cervical vertebrae5. Therefore, the new tracheal reconstructive surgery has been successfully performed in several patients, resulting in the recovery of respiratory function5,8,30. Conventional PFT, such as spirometry, can be used to detect respiratory dysfunction preoperatively; however, these tests are often hard to interpret because the available reference data does not apply to MPS patients who exhibit short stature and skeletal dysplasia11. Furthermore, invasive pulmonary function testing can be complicated with issues of cooperation in young patients or those with physical limitations. While spirometry proves beneficial in identifying lung disease1, and is the most common method for evaluating lung function, its forced expiratory maneuvers are often difficult for patients to perform19. Thus, PFTs have been modified to accommodate a larger range of patients including infants and patients with skeletal dysplasia and asthma31. These non-invasive PFTs would offer a new method for the evaluation of lung function in Morquio patients, in which many cases would otherwise be challenging to assess1. RIP has the benefit of being noninvasive and requires no patient cooperation31, making it an appropriate test for infants and post-operative patients25. Moreover, the American Thoracic Society (ATS) affirms that the TAA measurements provided by RIP prove to be promising for evaluating lung function in infants31. Recently, our hospital has published results with a new portable, point-of-care RIP system that utilizes a specifically programmed iPad application to provide immediate RIP parameters to caregivers32. Similarly, IOS requires little cooperation, and its ability to detect slight changes in airway function allows for early diagnosis and monitoring of airway diseases20. Furthermore, not only does IOS offer additional information regarding total respiratory system resistance, but studies have also shown its implications in identifying airway impediments, chest wall anomalies, lung compliance conditions, as well as chronic obstructive pulmonary disease and asthma assessments1. As one of the more recently acknowledged non-invasive PFTs, PNT is well tolerated by infants and patients with physical limitations. In addition, PNT proves to be beneficial for non-cooperative patients and those incapable of performing spirometry29, as it can be implemented during anesthesia and respiratory treatment28. The suggested non-invasive PFTs would supply both physicians and the Morquio community with important information used to analyze clinical conditions, as well as monitoring treatment progress. These tests would be able to be administered to patients with other types of MPS and skeletal dysplasia, thus incorporating a wider spectrum of patients than invasive PFTs1.
However, by validating these non-invasive PFTs with conventional spirometry and vital signs, valuable clinical data was provided to indicate the pulmonary status of Morquio patients. While the study was successful in testing patients ranging from 3 to 40 years old, a larger spectrum of phenotypes (mild to severe) with various stages of Morquio syndrome must be studied to strengthen these results1. Spirometry can be beneficial in determining the extent or progression of lung disease21; although, as demonstrated by our study, it may not be a suitable test for some patients1.
Conclusion
Morquio patients exhibit worsening tracheal obstruction with age due to accumulation of GAGs and successive imbalance of growth of the bones and cartilage organs. Many patients require surgical intervention to alleviate the clinical manifestations associated with Morquio Syndrome, in which life-threatening complications arise during anesthesia5. Our findings suggest that respiratory inductance plethysmography (RIP), impulse oscillometry system (IOS), and pneumotachography (PNT), are feasible, non-invasive methods for distinguishing and monitoring respiratory dysfunction in patients who cannot perform invasive pulmonary function testing1. Tracheal obstruction proves a greater risk to Morquio patients than other clinical factors associated with the disease, thus prompt recognition and intervention could be life-saving measures5.
Acknowledgments
T.H.S. and S.T. were supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of NIH under grant number P30GM114736. This work was supported by grants from the Austrian MPS Society and International Morquio Organization (Carol Ann Foundation). F.K. was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico from Brazil (CNPq) and INAGEMP. The content of the article has not been influenced by the sponsors.
Abbreviations
- %FEVTOT
predicted forced expiratory volume total
- ATS
American Thoracic Society
- C6S
chondroitin-6-sulfate
- CO2
carbon dioxide
- ECM
extracellular matrix
- FEV1
volume expired in the first second
- FOT
forced oscillation technique
- FVC
forced vital capacity
- GAGs
glycosaminoglycans
- GALNS
N-acetylgalactosamine-6-sulfate sulfatase
- GLB1
β-galactosidase
- IOS
impulse oscillometry
- KS
keratan sulfate
- MMEF
maximum mid-expiratory flow rate
- MPS IV
Mucopolysaccharidosis IV
- MPS
Mucopolysaccharidosis
- PFT
pulmonary functions tests
- PGs
proteoglycans
- PNT
pneumotachography
- RIP
respiratory inductance plethysmography
- TAA
thoracoabdominal asynchrony
Footnotes
Disclosures
All the authors contributed to this review paper and have no conflict of interest with any other part.
References
- 1.Kubaski F, Tomatsu S, Patel P, et al. Non-invasive pulmonary function test on Morquio patients. Mol Genet Metab. 2015 Aug;115(4):186–192. doi: 10.1016/j.ymgme.2015.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Neufeld E, Muenzer J. The Mucopolysaccharidoses. 8th. New York: McGraw-Hill; 2001. [Google Scholar]
- 3.Morquio L. Sur une forme de dystrophie osseuse familial. Arch Méd Enfants Paris. 1929;32:129–135. [Google Scholar]
- 4.Brailsford JF. Chondro-osteo-dystrophy roentgenopgraphic & clinical features of a child with dislocation of vertebrae. The American Journal of Surgery. 1929;7:404–410. [Google Scholar]
- 5.Tomatsu S, Averill LW, Sawamoto K, et al. Obstructive airway in Morquio A syndrome the past the present and the future. Mol Genet Metab. 2016 Feb;117(2):150–156. doi: 10.1016/j.ymgme.2015.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yasuda E, Fushimi K, Suzuki Y, et al. Pathogenesis of Morquio A syndrome an autopsied case reveals systemic storage disorder. Mol Genet Metab. 2013 Jul;109(3):301–311. doi: 10.1016/j.ymgme.2013.04.009. [DOI] [PubMed] [Google Scholar]
- 7.Khan S, Alméciga-Díaz CJ, Sawamoto K, et al. Mucopolysaccharidosis IVA and glycosaminoglycans. Mol Genet Metab. 2016 Nov 29; doi: 10.1016/j.ymgme.2016.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pizarro C, Davies RR, Theroux M, et al. Surgical Reconstruction for Severe Tracheal Obstruction in Morquio A Syndrome. Ann Thorac Surg. 2016 Oct;102(4):329. doi: 10.1016/j.athoracsur.2016.02.113. [DOI] [PubMed] [Google Scholar]
- 9.Souza-Fernandes AB, Pelosi P, Rocco PRM. Bench to bedside review the role of glycosaminoglycans in respiratory disease. Crit Care. 2006;10(6):237. doi: 10.1186/cc5069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yasuda E, Mackenzie W, Ruhnke K, et al. Long-term follow-up of post hematopoietic stem cell transplantation for Hurler syndrome clinical biochemical and pathological improvements. Mol Genet Metab Rep. 2015 Mar;2:65–76. doi: 10.1016/j.ymgmr.2014.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Walker R, Belani KG, Braunlin EA, et al. Anaesthesia and airway management in mucopolysaccharidosis. J Inherit Metab Dis. 2013 Mar;36(2):211–219. doi: 10.1007/s10545-012-9563-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Muhlebach MS, Wooten W, Muenzer J. Respiratory Manifestations in Mucopolysaccharidoses. Paediatric Respiratory Reviews. 2011 Jun;12(2):133–138. doi: 10.1016/j.prrv.2010.10.005. [DOI] [PubMed] [Google Scholar]
- 13.Lavery C, Hendriksz C. Mortality in patients with morquio syndrome a. JIMD Rep. 2015;15:59–66. doi: 10.1007/8904_2014_298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.de Medeiros Matsushita M, da Silva Luiz, Ferraz Fernando, et al. Airway proteoglycans are differentially altered in fatal asthma. J Pathol. 2005 Sep;207(1):102–110. doi: 10.1002/path.1818. [DOI] [PubMed] [Google Scholar]
- 15.Yasuda E, Suzuki Y, Shimada T, et al. Activity of daily living for Morquio A syndrome. Mol Genet Metab. 2016 Jun;118(2):111–122. doi: 10.1016/j.ymgme.2016.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kadic L, Driessen JJ. General anaesthesia in an adult patient with Morquio syndrom with emphasis on airway issues. Bosn J Basic Med Sci. 2012 May;12(2):130–133. doi: 10.17305/bjbms.2012.2513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Theroux MC, Nerker T, Ditro C, et al. Anesthetic care and perioperative complications of children with Morquio syndrome. Paediatr Anaesth. 2012 Sep;22(9):901–907. doi: 10.1111/j.1460-9592.2012.03904.x. [DOI] [PubMed] [Google Scholar]
- 18.Drummond JC, Krane EJ, Tomatsu S, et al. Paraplegia after epidural-general anesthesia in a Morquio patient with moderate thoracic spinal stenosis. Can J Anaesth. 2015 Jan;62(1):45–49. doi: 10.1007/s12630-014-0247-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Brashier B, Salvi S. Measuring lung function using sound waves role of the forced oscillation technique and impulse oscillometry system. Breathe Sheff. 2015 Mar;11(1):57–65. doi: 10.1183/20734735.020514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Desiraju K, Agrawal A. Impulse oscillometry The state-of-art for lung function testing. Lung India. 2016 Jul-Aug;33(4):410–416. doi: 10.4103/0970-2113.184875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Burki NK. Spirometry and other pulmonary function tests. J Fam Pract. 1981 Jan;12(1):119–124. [PubMed] [Google Scholar]
- 22.Berkowitz ID, Raja SN, Bender KS, et al. Dwarfs pathophysiology and anesthetic implications. Anesthesiology. 1990 Oct;73(4):739–759. [PubMed] [Google Scholar]
- 23.Mandal NG. Respirometers including spirometer pneumotachograph and peak flow meter. Anaesthesia & Intensive Care Medicine. 2006;7(1):1–5. 01-01. [Google Scholar]
- 24.Retory Y, Niedzialkowski P, de Picciotto C, et al. New Respiratory Inductive Plethysmography (RIP) Method for Evaluating Ventilatory Adaptation during Mild Physical Activities. PLoS ONE. 2016;11(3):e0151983. doi: 10.1371/journal.pone.0151983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Brown K, Aun C, Jackson E, et al. Validation of respiratory inductive plethysmography using the Qualitative Diagnostic Calibration method in anaesthetized infants. Eur Respir J. 1998 Oct;12(4):935–943. doi: 10.1183/09031936.98.12040935. [DOI] [PubMed] [Google Scholar]
- 26.Poole KA, Thompson JR, Hallinan HM, et al. Respiratory inductance plethysmography in healthy infants a comparison of three calibration methods. Eur Respir J. 2000 Dec;16(6):1084–1090. doi: 10.1034/j.1399-3003.2000.16f11.x. [DOI] [PubMed] [Google Scholar]
- 27.Rodriguez ME, Mackenzie WG, Ditro C, et al. Skeletal dysplasias evaluation with impulse oscillometry and thoracoabdominal motion analysis. Pediatr Pulmonol. 2010 Jul;45(7):679–686. doi: 10.1002/ppul.21246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Grenvik A, Hedstrand U, Sjögren H. Problems in pneumotachography. Acta Anaesthesiol Scand. 1966;10(3):147–155. doi: 10.1111/j.1399-6576.1966.tb00339.x. [DOI] [PubMed] [Google Scholar]
- 29.Bouhuys A. The clinical use of pneumotachography. Acta Med Scand. 1957 Nov 15;159(2):91–103. doi: 10.1111/j.0954-6820.1957.tb00110.x. [DOI] [PubMed] [Google Scholar]
- 30.Sawamoto K, Suzuki Y, Mackenzie WG, et al. Current therapies for Morquio A syndrome and their clinical outcomes. Expert Opinion on Orphan Drugs. 2016 Sep 1;4(9):941–951. doi: 10.1080/21678707.2016.1214572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Giordano K, Rodriguez E, Green N, et al. Pulmonary function tests in emergency department pediatric patients with acute wheezing/asthma exacerbation. Pulm Med. 2012;2012:724139. doi: 10.1155/2012/724139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rahman T, Page R, Page C, et al. PneuRIPTM: A Novel Respiratory Inductance Plethysmography Monitor. ASME J Med Devices. 2017 doi: 10.1115/1.4035546. 011010-011-010-6. [DOI] [PMC free article] [PubMed] [Google Scholar]