

Abstract
Choroidal nevi are benign fundus lesions that require regular follow with documentation. Conventional color fundus photography (CFP) has traditionally been used to images these lesions. Multicolor imaging (MCI) available on Spectralis spectral domain optical coherence tomography system is increasingly been tested vis-à-vis conventional CFP in various retinal diseases. We present data of the right eye of a 59-year-old gentleman with choroidal nevus who underwent conventional CFP as well as MCI. Nevus appeared orange red on MCI and its size appeared larger than the same measured on conventional CFP. We also report infrared reflectance and near infrared autofluorescence features of choroidal nevus.
Keywords: Choroidal nevus, color fundus photography, multicolor imaging, multimodal imaging, retinal imaging
Nevus cells are result of atypical melanization of melanoblasts originating from neural crest.[1] Choroidal nevus presents as round or oval dark brown lesions on fundus.[2] Though choroidal nevi are benign lesion, they do carry malignant potential, necessitating a regular follow-up to look for any change in their size. Conventional color fundus photography (CFP) has been the modality of choice to document the size and follow-up of choroidal nevus.
Multicolor imaging (MCI) available on Spectralis spectral domain optical coherence tomography (SDOCT) platform developed by Heidelberg Engineering, Germany is a new imaging modality that provides pseudocolor coding of various fundus lesions and has been used in various retinal disorders.[2,3,4,5,6,7,8] MCI is based on confocal scanning laser ophthalmoscopy principles and uses three laser lights (blue 488 nm, green 515 nm, and infrared (IR) 820 nm) to image the retina.[4,5,6,7] Blue channel images the vitreoretinal interface and retinal surface, green channel is meant for imaging inner retinal features such as hemorrhage, hard exudates and blood vessels, and IR channel images retinal pigment epithelium and choroid. By virtue of imaging different retinal layers separately, MCI is able to provide topographic changes in retina which is not discernable on CFP. We report here the MCI features of choroidal nevus and compare it with CFP.
Case Report
A 59-year-old gentleman visited the outpatient department for routine eye examination. The best corrected visual acuity was 20/30, N6 in right eye and 20/20, N6 in left eye. Anterior segment revealed early nuclear sclerosis in right eye, while left eye was pseudophakic. Fundus of right eye revealed attached retina and normal optic disc. There was an oval patch of dark brown pigmentation at macula, abutting fovea, and extending toward superior vascular arcade in right eye [Fig. 1a]. Fundus of left eye was within normal limits. SDOCT of right eye through the area revealed hyporeflectivity beneath retinal pigment epithelium, suggestive of choroidal nevus. Overlying retinal pigment epithelium and other retinal layers were normal [Fig. 1b].
Figure 1.

(a) CFP of the right eye shows choroidal nevus as dark brown lesion near superior arcade extending up to fovea (white arrow heads). (b) SDOCT scan passing through the nevus shows hyporeflectivity in choroid (white star) and normal overlying retina. (c) MCI of the right eye shows choroidal nevus as orange red lesion (white arrow heads) owing to its high melanin content, making it amenable to be imaged by IR channel
MCI of right eye showed choroidal nevus as subretinal orange red lesion [Fig. 1c]. IR reflectance image of right eye showed hyperreflectance at the site of nevus [Fig. 2a]. Lipofuscin-based blue autofluorescence did not show choroidal nevus [Fig. 2b]. Melanin-based near infrared autofluorescence (NIR-AF) image showed nevus as hyperautofluorescent zone corresponding to CFP and MCI [Fig. 2c].
Figure 2.

(a) IR image of right eye shows hyperreflectivity at the site of choroidal nevus (yellow arrow heads). (b) Lipofuscin-based blue autofluorescence image of right eye does not show choroidal nevus. It is important to know because this is the most commonly used autofluorescence imaging in clinical practice. (c) Melanin-based NIR-AF image shows hyperautofluorescence at the site of choroidal nevus (yellow arrow heads) owing to its high melanin content
The area of choroidal nevus was measured on MCI with the help of inbuilt Heyex software on Spectralis system. The area on MCI was 3.34 mm2. To measure the area of nevus on CFP, the image was imported into Spectralis system and measured as suggested by Muftuoglu et al.[2] The area of nevus on CFP was 2.21 mm2 [Fig. 3a and b].
Figure 3.
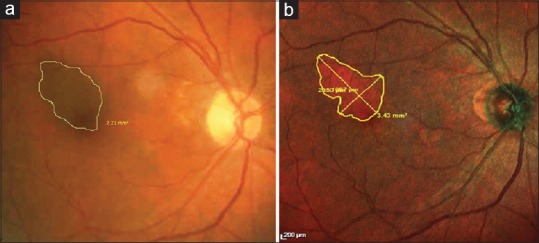
(a) Heyex software line drawing tool shows area of the choroidal nevus as measured on CFP. (b) Heyex software line drawing tool shows area of the choroidal nevus as measured on MCI
Discussion
Choroidal nevi are benign lesions of fundus. However, regular follow-up of these patients with CFP is essential due to possible risk of malignant transformation.[1] MCI is a novel imaging modality which has been found useful in various retinal disorders ranging from superficial epiretinal membrane to deeper retinal pigment epitheliitis.[3,9] Similarly, melanin-based NIR-AF has been used to image retinal conditions such as geographic atrophy and hydroxychloroquine retinal toxicity.[4,10] However, the data about MCI, IR, and NIR-AF imaging signatures of choroidal nevus are sparse in published literature.
In our case, the dark brown choroidal nevus seen on conventional CFP appeared orange red on MCI. Pigmented choroidal nevi are high in melanin content and are located beneath retinal pigment epithelium. The laser channel of multicolor technology that images deeper lesions is IR and the pseudocolor assigned to this channel is red. The pseudocolor rendering assigned to superficial blue laser is blue and inner retinal green laser is green. The orange red color of nevus originates from high melanin content and deeper location; both of which make it amenable to be imaged by the IR channel of MCI. Because of the same reason, nevus appeared hyperreflective on IR image. We also describe the NIR-AF imaging signatures of choroidal nevus, which is hitherto unreported in the literature. Being high in melanin content, pigmented choroidal nevus appeared hyperautofluorescent on NIR-AF image. It was not picked up by lipofuscin-based blue autofluorescence.
Muftuoglu et al. have reported that MCI underestimates the size of choroidal lesion by 33% when compared with CFP. However, in our case, the nevus appeared larger on MCI than on CFP. CFP is influenced by the pigmentation of the fundus.[11] Higher pigmentation of the fundus in our case due to ethnic difference from those described by Muftuoglu et al. may be a reason of smaller size of nevus on CFP compared to MCI. However, the finding of larger area of pigmented nevus on MCI needs to be further validated in a larger series to make it robust finding.
Apart from pigmented choroidal nevus, nevi which are located beyond posterior pole may not show same imaging characteristics because the currently available MCI technology does not properly image lesions beyond posterior pole. Similarly, amelanotic choroidal nevus that lack melanin should have different imaging pattern on MCI than pigmented choroidal nevus.
Conclusion
The current case reports the multimodal imaging characteristics of pigmented choroidal nevus. CFP has been the gold standard for serial follow-up of these eyes. MCI, IR, and NIR-AF imaging signatures of choroidal nevus reported here need further validation in a large case series and on multiple visits. However, our single case does reveal the hitherto unreported imaging signatures of the pigmented choroidal nevus.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Torczynski E. Choroid and suprachoroid. In: Jakobiec F, editor. Ocular anatomy, embryology, and teratology. Philadelphia: Harper & Row; 1982. [Google Scholar]
- 2.Muftuoglu IK, Gaber R, Bartsch DU, Meshi A, Goldbaum M, Freeman WR. Comparison of conventional color fundus photography and multicolor imaging in choroidal or retinal lesions. Graefes Arch Clin Exp Ophthalmol. 2018;256:643–9. doi: 10.1007/s00417-017-3884-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Roy R, Saurabh K, Thomas NR. Multicolor imaging in a case of acute retinal pigment epithelitis. Retin Cases Brief Rep. 2018 doi: 10.1097/ICB.0000000000000726. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 4.Saurabh K, Roy R, Thomas NR, Chowdhury M. Multimodal imaging characteristics of hydroxychloroquine retinopathy. Indian J Ophthalmol. 2018;66:324–7. doi: 10.4103/ijo.IJO_787_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Thomas NR, Ghosh PS, Chowdhury M, Saurabh K, Roy R. Multicolor imaging in optic disc swelling. Indian J Ophthalmol. 2017;65:1251–5. doi: 10.4103/ijo.IJO_473_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ahmad MSZ, Carrim ZI. Multicolor scanning laser imaging in diabetic retinopathy. Optom Vis Sci. 2017;94:1058–61. doi: 10.1097/OPX.0000000000001128. [DOI] [PubMed] [Google Scholar]
- 7.Saurabh K, Roy R, Chowdhury M. Efficacy of multicolor imaging in patients with asteroid hyalosis: Seeing the unseen. JAMA Ophthalmol. 2018 doi: 10.1001/jamaophthalmol.2018.0026. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Roy R, Saurabh K, Bhattacharyya S, Thomas NR, Datta K. Multimodal imaging in dominant cystoid macular dystrophy. Indian J Ophthalmol. 2017;65:865–6. doi: 10.4103/ijo.IJO_328_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kilic Muftuoglu I, Bartsch DU, Barteselli G, Gaber R, Nezgoda J, Freeman WR. Visualization of macular pucker by multicolor scanning laser imaging. Retina. 2018;3:352–8. doi: 10.1097/IAE.0000000000001525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chen FK, Khoo YJ, Tang I. Near-infrared autofluorescence imaging in geographic atrophy using spectralis single and combined wavelength modes. Asia Pac J Ophthalmol (Phila) 2015;4:334–8. doi: 10.1097/APO.0000000000000142. [DOI] [PubMed] [Google Scholar]
- 11.Bourne RA. Ethnicity and ocular imaging. Eye (Lond) 2011;25:297–300. doi: 10.1038/eye.2010.187. [DOI] [PMC free article] [PubMed] [Google Scholar]