

Abstract
Rhinoplasty is done with external and endonasal methods. One of the main stages of rhinoplasty in both external and endonasal methods is the lateral nasal osteotomy. Lateral nasal osteotomy is the main cause of edema and ecchymosis after rhinoplasty, which is annoying and unpleasant for patients. Piezosurgery is a new method that uses electronic-ultrasonic waves to perform nasal osteotomies. The aim of this study was to compare of edema and ecchymosis after lateral nasal osteotomy using piezosurgery with external osteotomy in rhinoplasty candidates. In this clinical trial, 66 experimental patients for rhinoplasty surgery were selected from Imam Reza hospital in Tabriz, Iran. After examination, the patients were randomly divided into two groups. One group of patients had lateral nasal osteotomy by using the piezosurgery technique, and the other group had a lateral osteotomy with the conventional method of external subcutaneous. On the third and 7 days after the operation, the level of edema and ecchymosis in the patients were examined as per the Gökalan questionnaire (adopted by Yucel) by two persons who were not aware of the goals of the study, and then, they evaluated and scored the questionnaire. The obtained data were analyzed by the SPSS 19 software. The highest level of edema and ecchymosis was observed 3 days after surgery in both groups. Meanwhile, the findings revealed a significant difference between the two groups in the amount of edema and ecchymosis on day 3 after surgery. Furthermore on day 7, the amount of edema and ecchymosis compared to that of the 3rd day was statistically significant for both groups. In general, in all studied groups, edema, and ecchymosis decreased in 7 days compared to 3 days and also piezosurgery is more promising and effective than osteotomy.
Keywords: Ecchymosis, edema, lateral nasal osteotomy, piezosurgery, rhinoplasty
INTRODUCTION
Osteotomy of the nasal bones is one of the most dangerous processes in rhinoplasty that is the less controllable stage of rhinoplasty. The main indications of osteotomy include the open roof deformity correction after removing the nose hump, thinning the nasal pyramid and removing the convexity or asymmetry, and straightening the nasal bones.[1,2] Lateral osteotomy applies a lot of energy to the hard and soft nose tissues and should be done with stability and without any unwanted changes. Rees and Ford approved external osteotomy method, due to reduced trauma to soft tissues, mucous, and periosteum.[3] The osteotomy of nasal bone structures results in soft tissue damage, ecchymosis, and prolonged edema after surgery. Piezosurgery is a new technique for nasal osteotomy that uses piezoelectric ultrasonic waves. Ultrasonic frequencies can induce small vibrations in the surgical blade, which leads to bone cutting.[4,5] On the other hand, the piezoelectric osteotomy is safe and prevents osteonecrosis and soft-tissue damage due to the establishment of selective, very delicate, and accurate methods.[6]
Many studies have compared the side effects, edema, and ecchymosis after surgery between these two methods; however, none of the conducted studies have arrived at a theoretical agreement regarding the superiority of either method.[7,8] In a study by Tirelli et al. in Italy in 2015, 12 patients with a typical 2-mm osteotome and 10 patients were subjected to external lateral osteotomy with piezosurgery. The results showed that within 4 days after surgery, pain, edema, and ecchymosis in the patients who underwent rhinoplasty with piezosurgery were significantly less than in the other patients. Furthermore, endoscopic examination revealed that mucosal injury was significantly lower in patients who underwent piezosurgery. However, at the end of their study, the authors acknowledged that the number of samples in the study was low and proposed other studies with more samples.[9] In the study by Ilhan et al. in Turkey in 2016, 22 patients with 4-mm standard osteotomies, and 34 patients underwent osteotomy with the piezosurgery technique. The results showed that ecchymosis was more significant in the patients who underwent conventional osteotomy in 3 and 7 days following surgery. However, from the 3rd day until the 7 days, there was reduced ecchymosis in both groups, and the level of ecchymosis reduction in the two groups was the same. Edema was significantly higher after surgery on day 3 in patients who underwent conventional osteotomy. The results of one of the examinations regarding the level of edema on day 7 showed that edema was more significant in patients who underwent conventional osteotomy, but the results of the other test examination reported that the two groups had the same value on day 7.[10] Furthermore, in a study by Koçak et al. in Turkey in 2017, 25 patients with a conventional 3-mm osteotome and 24 patients with piezosurgery were subjected to lateral internal osteotomy. The results showed that ecchymosis was higher on days 2, 4, and 7 in patients who underwent conventional osteotomy. Edema was significantly higher on day 2 after surgery in patients who underwent conventional osteotomy, but on day 4, edema had increased in patients who underwent piezosurgery and then went on reducing until day 7.[11]
According to many studies on the significance of edema and ecchymosis, the number of samples in these studies was small. Consequently, there is no definitive decision on which of the two methods mentioned above can be effective for edema and ecchymosis. This study aims to compare the significance of edema and ecchymosis after nasal osteotomy with the piezosurgery method and the external method.
MATERIALS AND METHODS
Studied subjects
In this clinical and double-blind clinical trial, 66 candidates for rhinoplasty surgery referred to Imam Reza Hospital in Tabriz (from March to November 2017) were chosen by using convenience sampling. After explaining the study, how it would be conducted, the side effects and limitations of each osteotomy method, and obtaining their informed consent, the patients were included in the study. This study was approved by the Ethics Committee of Tabriz University of Medical Sciences and assigned the code 1164, 2017, IR–TBZMED.
The inclusion criteria were the satisfaction of the patients and the absence of contraindication for rhinoplasty surgery. Furthermore, current smokers, patients with chronic rhinosinusitis, chronic diseases of the skin or rheumatology, nasal polyps, asthma, allergic rhinitis, patients with prior septoplasty or nasal beautification surgeries, ecchymosis or edema before surgery for any reason as well as the patients who did not come back for postoperative examinations were excluded.
Following their entry into the study, patients were selected according to the criteria and underwent clinical examinations. Patients with a thick skin or with a lateral bone thicker than 3 mm were excluded from the study.
Surgical procedures
All the patients were prescribed 1 g of cefazolin 1 h before surgery as well as 8 mg of Dexamethasone 30 min before surgery and 8 mg every 8 h after operation for 24 h. The same anesthesia induction was used for all the patients. Each patient was laid in the reverse Trendelenburg position. During the surgery for hydro dissection and homeostasis, the same amount of local anesthesia with epinephrine (3 carpule lidocaine with epinephrine 1% per thousand) on both sides with a 1:1 ratio with injectable normal saline were used.
The patients were randomly divided into two groups as follows: one group of patients underwent lateral nasal osteotomy by using two stab incisions by utilizing a 2-mm osteotome. The other group underwent lateral nasal osteotomy after two stab incisions with 2 mm, using the Viosurg device from NSK Company with a lateral osteotomy pen. This device includes a powerful piezoelectric platform with a functional frequency range from 25 to 29 kHz with a digital modulation (amplifier) up to 30 kHz. This device also has a cooling system with sterile solution flow per min with 0°C–60°C temperature. For both groups, if the surgical time for a patient took longer than 2 h, the patient was excluded from the study. For patients in the piezosurgery group, in addition to the blade of the device for osteotomy, another method was used for FX, and these patients were excluded from the study. The site of the stab incisions for all the patients was sutured by using nylon yarn 0–5.
One pair of internal nasal splint was prescribed for all the patients, and an external splint made of thermodynamic silicone was placed in the hump area. For all the patients, the head was kept at a 30° angle postoperation and compressed ice was applied for 15 min every h for the first 24 h, and 500 cephalexin capsules after every 8 h, 400 mg of Gelofen capsules after every 6 h up to 5 days and 8 mg of dexamethasone after every 8 h up to 24 h were prescribed for all the patients [Figure 1]. The internal splint was extracted on day 4, and the external splint was extracted on day 7 from all the patients.
Figure 1.

How to perform piezosurgery
On days 3 and 7 after surgery, the amounts of ecchymosis and edema in the patients were examined by two examiners who were not aware of the goals of the study. The amounts of ecchymosis and edema in the patients were evaluated and scaled using the Kara and Gökalan (Adopted by Yucel) scoring diagram, which is shown in Figures 2 and 3.[12,13]
Figure 2.
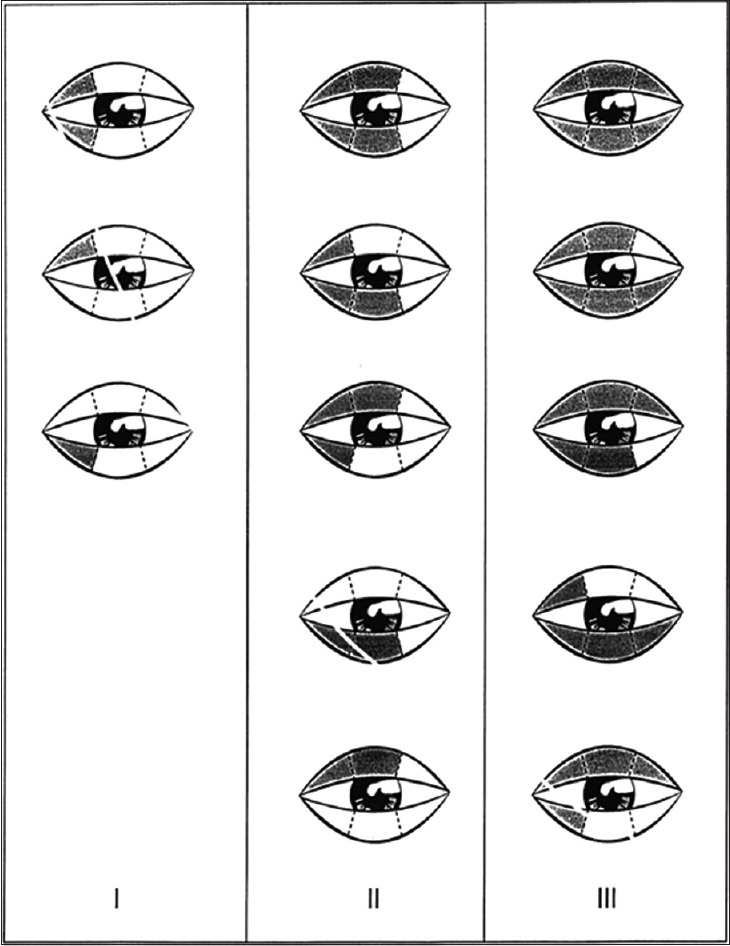
Ecchymosis: Extending the ecchymosis to one-third of the inner lower or upper eyelid = Grade 1, extending the ecchymosis to two third of the inner lower or upper eyelid = Grade 2, and extending the ecchymosis to the entire lower or upper eyelid = Grade 3
Figure 3.
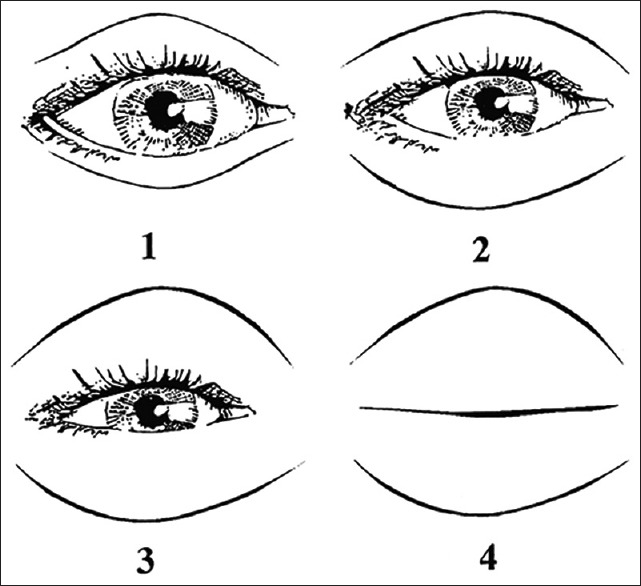
Edema: Iris is not covered by eyelid = Grade 1, part of the iris covered with eyelid = Grade 2, full iris coverage with a flap of the eyelid = Grade 3, and complete closure of the eye and swelling = Grade 4
Statistical analysis
The results of the study were reported using descriptive statistics (mean + standard deviation and frequency). To compare edema and ecchymosis on the third and 7 days after surgery, Chi-square and Friedman tests were performed with the IBM SPSS statistic software version 19 software. The comparison between the ages of the patients in the two groups was carried out according to the normal distribution of age data by using an independent t-test. In this study, a value of P < 0.05 was considered statistically significant.
RESULTS
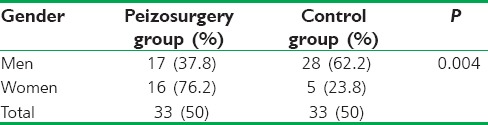
In this clinical trial, 66 patients (33 women and 33 men) with rhinoplasty referred to Imam Reza Hospital were included in the study. The comparison between the ages of the patients in the two groups according to the normal distribution of age data was carried out. The results revealed that 17 of the male patients (8.7%) and 16 of the female patients (76.2%) underwent piezosurgery, and these numbers showed that there was a significant statistical difference (P = 0.004) [Table 1].
Table 1.
Gender dispersion in the case and control groups
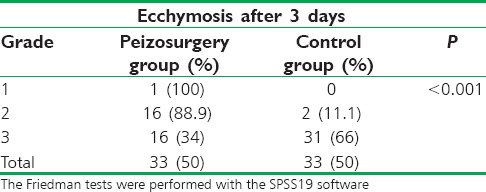
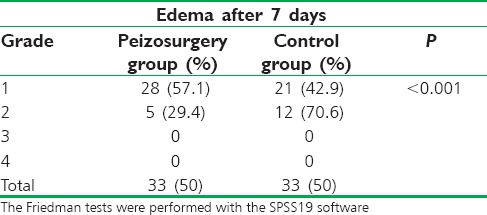
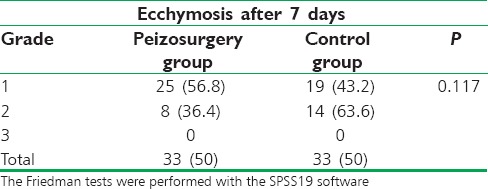
The significance of edema 3 days after surgery in both groups showed that the highest edema with Grade 4 was found with the frequency of 13 (31%) and 29 (69%) individuals, respectively. These rates decreased on day 7 after surgery and were only observed in Grades 1 and 2. Meanwhile, on day 7, the highest levels of edema were found in both groups with Grade 1, in the piezosurgery and control groups were observed 28 (57.1%) and 21 (42.9%) individuals, respectively. The significance of ecchymosis 3 days after surgery was observed with Grades 1–3, so that the highest levels in both groups were of Grade 3 with the frequency of 16 individuals (34%) and 31 individuals (66%), respectively. These rates decreased on the 7 days after surgery and were observed only with Grades 1 and 2. The highest ecchymosis amounts occurred with Grade 1 in both the piezosurgery and control groups with a frequency of 25 individuals (56.8%) and 19 individuals (43.2%), respectively.
The difference between the amount of edema in different postsurgery periods (3 and 7 days) was examined for each group by using the Friedman test. It was observed that there was a significant difference between the amount of edema on days 3 and 7.
Postsurgery, the means in both the piezosurgery and the control groups showed significant statistical differences (P < 0.001). The highest edema mean in both the groups was on the 3 days after surgery [Table 2 and Figure 4a].
Table 2.
Edema between two groups after 3 days
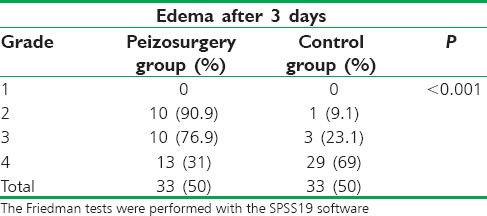
Figure 4.

The comparison of edema and ecchymosis after surgery between the piezosurgery and control groups. (a) edema 3 days; (b) edema 7 days; (c) ecchymosis 3 days; (d) ecchymosis 7 days
There was a significant statistical difference between the amount of ecchymosis on the third and 7 days after surgery in the piezosurgery group and also in the control group (P < 0.001). The maximum amount of ecchymosis in both groups was recorded in 3 days after surgery [Table 3 and Figure 4c, d].
Table 3.
Ecchymosis after 3 days between two groups
The level of edema on 3 and 7 days after surgery showed a significant statistical difference between the two groups with P < 0.001 and P = 0.049, respectively [Table 4 and Figure 4a, b].
Table 4.
Edema after 7 days between two groups
Furthermore, the amount of ecchymosis on day 3 after surgery between the two groups showed a significant difference (P > 0.001), whereas this difference was not significant on day 7 after surgery (P = 0.117) [Table 5 and Figure 4d].
Table 5.
Ecchymosis after 7 days between two group
There were no cases of skin infection and burning or abnormal nasal bleeding among the patients after surgery.
DISCUSSION
This study evaluated piezosurgery method as a low-invasive technique for lateral nasal osteotomy, which is effective in preventing short-term complications (ecchymosis and edema) in comparison to conventional osteotomy. This study was performed on a large sample size in comparison to previous studies. The ideal technique for lateral osteotomy should ensure the integrity of the nasal mucosa and the periosteal joints of the nose bone's lateral wall. The selected clinical method should be safe, accurate, and repeatable.[14]
Piezosurgery is a precise method that has minor soft-tissue damage during bone cutting, which is based on ultrasonic micro vibration. The main advantages of piezosurgery include the protection of soft tissue, optimal vision at the surgery site, reduction in blood loss, less vibration and low noise, and it can be used in the fields of maxillofacial surgery, ears, pharynx, ophthalmology, dermatology, and orthopedics. Piezosurgery is a technical modality for bone surgery, which is being increasingly used in various fields.[15] For this purpose, piezosurgery was first developed by Robiony et al.[4] Since the bone thickness along the osteotomy line is <3 mm, and also because cutting the bone to its total thickness is not necessary, piezosurgery can be an ideal tool for performing lateral osteotomies.[16]
Postsurgery edema and ecchymosis in rhinoplasty are common side effects which are mainly caused by soft-tissue injuries and damage during osteotomy, and most surgeons focus on reducing these side effects.[17]
The study aimed to compare lateral osteotomy techniques by using the piezosurgery method and by using the external percutaneous method by utilizing a 2-mm osteotomy to determine the difference between these two methods in reducing edema and ecchymosis after surgery. Considering similar studies conducted earlier, the number of cases studied and the lack of a clear result in indicating which technique was better, the present study was designed with a greater number of cases to determine which method was superior.
In a study by Sinha et al., a comparison between the incidence and severity of edema and ecchymosis in rhinoplasty determined that edema and ecchymosis were less intense in a closed rhinoplasty. The open technique for rhinoplasty was used in all our study cases, which, in contrast to our results, may lead to increased edema and ecchymosis.[16] The open technique was used in our study because it provided better access to the tip of the nose.
A study by Caglar et al. reported that an osteotomy time of <2 h reduced the incidence and morbidity.[17] This result was synchronized with our study with those who required surgery for more than 120 min were excluded from our study sample.
Researchers have determined that nasal bone thickness is very important in soft-tissue damage during osteotomy, and therefore, the tools used in osteotomy to prevent vascular damage are very important.[18] In our study, people with thick nasal bones were excluded following initial examinations to avoid disorder in the study results.
Since the thickness of the bone along the osteotomy line is <3 mm, and also because cutting the bone to its total thickness is not necessary, piezosurgery can be an ideal tool for performing lateral osteotomy by virtue of it being a less invasive technique that prevents vascular damage as well as edema and ecchymosis creations in short terms.[18]
According to our study results, the highest rate of edema and ecchymosis in both the piezosurgery and external osteotomy groups was found on day 3 after surgery. The findings showed that there was a significant statistical difference between the amount of edema and ecchymosis on the third and 7 days after surgery in the piezosurgery group as well as in the external osteotomy group so that in both groups, the values of edema and ecchymosis reduced with the passage of time.
Furthermore, the amount of edema on days 3 and 7 was statistically significant and reduced in the piezosurgery group as compared to the external osteotomy group. Compared to the conventional osteotomy group, the amount of ecchymosis in the piezosurgery group within 3 days after surgery was significantly lower, but on the 7 days, there was no statistical difference between the two groups.
A study by Taşkın et al. conducted in Turkey reported that the amount of edema in both groups was significantly higher on the 2nd day than on the 7 days. However, no significant differences were found between the piezosurgery and external osteotomy groups.[8] In our study, edema significance on day 2 was similar to that on day 7 for both groups, but the amount of edema in the piezosurgery group was significantly lower than that in the lateral osteotomy group.
In a study in 2017, Koc et al. compared piezosurgery and lateral osteotomy in rhinoplasty, and found that on day 1 after surgery, the piezosurgery group showed better results regarding edema, ecchymosis, and hemorrhage. Similarly, the results for edema and ecchymosis in the piezosurgery group were better on the 7 days.[19]
Previous studies have shown that piezosurgery reduces pain and maintains hemostasis in compared to conventional osteotomy. Yaman and Suer showed that in piezosurgery, the cavitation phenomenon helps to maintain good visibility in the operative field by dispersing a coolant fluid as an aerosol that causes the blood to essentially be washed away. Furthermore, the cavitation effect will bring about hemostasis, which results in a bloodless surgery.[20] In another study, Tirelli et al. reported significantly reduced rates of pain in patients who underwent piezosurgery as compared to the patients in the conventional osteotomy, while endoscopic studies have also determined less mucosal damage in patients who underwent piezosurgery.[9]
It is also recommended to investigation and to compare the severity of the injuries and damage in both piezosurgery and lateral osteotomy methods with novel methods such as immunohistochemistry based on the shape and facial anatomy of different individuals.
CONCLUSION
According to the results, it seems that piezosurgery is a safe and very precise technique with minimal soft-tissue damage that results in precise bone grafts and it can be considered as a superior technique for performing lateral osteotomies. According to our study results, piezosurgery can be more effective in reducing edema and ecchymosis as compared to lateral osteotomy immediately after surgery (up to 3 days). The only disadvantage of this technique, as per our opinion, is the possibility of skin burn due to the use of the device, which we tried to eliminate by using a large amount of shank on the device.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Manafi A, Eslami Shahr Babaki A, Mehrabani G, Shahlaee A, Manafi A. Can we add auricular composite graft to our rhinoplasty armamentarium? World J Plast Surg. 2013;2:33–40. [PMC free article] [PubMed] [Google Scholar]
- 2.Hassanpour SE, Heidari A, Moosavizadeh SM, Tarahomi MR, Goljanian A, Tavakoli S, et al. Comparison of aesthetic and functional outcomes of spreader graft and autospreader flap in rhinoplasty. World J Plast Surg. 2016;5:133–8. [PMC free article] [PubMed] [Google Scholar]
- 3.Motamed S, Saberi A, Niazi F, Molaei H. Complications of internal continuous and perforating external osteotomy in primary rhinoplasty. World J Plast Surg. 2017;6:164–9. [PMC free article] [PubMed] [Google Scholar]
- 4.Robiony M, Toro C, Costa F, Sembronio S, Polini F, Politi M, et al. Piezosurgery: A new method for osteotomies in rhinoplasty. J Craniofac Surg. 2007;18:1098–100. doi: 10.1097/scs.0b013e3180de6489. [DOI] [PubMed] [Google Scholar]
- 5.Vercellotti T. Piezoelectric surgery in implantology: A case report – A new piezoelectric ridge expansion technique. Int J Periodontics Restorative Dent. 2000;20:358–65. [PubMed] [Google Scholar]
- 6.Politi M, Vercellotti T, Polini F, editors. Bologna, Italy: 2002. Piezoelectric surgery: A new method of bone cutting. Preliminary experience in alveolar osteogenesis distraction. Proceedings of the 2nd International Meeting on Distraction Osteogenesis of the Facial Skeleton; p. Y28. [Google Scholar]
- 7.Chu E, Davis RE. SMAS debulking for management of the thick-skinned nose. JAMA Facial Plast Surg. 2015;17:305–6. doi: 10.1001/jamafacial.2015.0361. [DOI] [PubMed] [Google Scholar]
- 8.Taşkın Ü, Batmaz T, Erdil M, Aydın S, Yücebaş K. The comparison of edema and ecchymosis after piezoelectric and conventional osteotomy in rhinoplasty. Eur Arch Otorhinolaryngol. 2017;274:861–5. doi: 10.1007/s00405-016-4306-9. [DOI] [PubMed] [Google Scholar]
- 9.Tirelli G, Tofanelli M, Bullo F, Bianchi M, Robiony M. External osteotomy in rhinoplasty: Piezosurgery vs osteotome. Am J Otolaryngol. 2015;36:666–71. doi: 10.1016/j.amjoto.2015.05.006. [DOI] [PubMed] [Google Scholar]
- 10.Ilhan AE, Cengiz B, Caypinar Eser B. Double-blind comparison of ultrasonic and conventional osteotomy in terms of early postoperative edema and ecchymosis. Aesthet Surg J. 2016;36:390–401. doi: 10.1093/asj/sjv260. [DOI] [PubMed] [Google Scholar]
- 11.Koçak I, Doğan R, Gökler O. A comparison of piezosurgery with conventional techniques for internal osteotomy. Eur Arch Otorhinolaryngol. 2017;274:2483–91. doi: 10.1007/s00405-017-4514-y. [DOI] [PubMed] [Google Scholar]
- 12.Kara CO, Gökalan I. Effects of single-dose steroid usage on edema, ecchymosis, and intraoperative bleeding in rhinoplasty. Plast Reconstr Surg. 1999;104:2213–8. doi: 10.1097/00006534-199912000-00041. [DOI] [PubMed] [Google Scholar]
- 13.Yücel OT. Which type of osteotomy for edema and ecchymosis: External or internal? Ann Plast Surg. 2005;55:587–90. doi: 10.1097/01.sap.0000185396.94875.4a. [DOI] [PubMed] [Google Scholar]
- 14.Kienstra MA, Sherris DA, Kern EB. Osteotomy and pyramid modification in the Joseph and Cottle rhinoplasty. Facial Plast Surg Clin North Am. 1999;7:279–94. [Google Scholar]
- 15.PavlÍková G, Foltán R, Horká M, Hanzelka T, Borunská H, Sedý J, et al. Piezosurgery in oral and maxillofacial surgery. Int J Oral Maxillofac Surg. 2011;40:451–7. doi: 10.1016/j.ijom.2010.11.013. [DOI] [PubMed] [Google Scholar]
- 16.Sinha V, Gupta D, More Y, Prajapati B, Kedia BK, Singh SN, et al. External vs. Internal osteotomy in rhinoplasty. Indian J Otolaryngol Head Neck Surg. 2007;59:9–12. doi: 10.1007/s12070-007-0002-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Caglar E, Celebi S, Topak M, Develioglu NO, Yalcin E, Kulekci M, et al. How can periorbital oedema and ecchymose be reduced in rhinoplasty? Eur Arch Otorhinolaryngol. 2016;273:2549–54. doi: 10.1007/s00405-016-3907-7. [DOI] [PubMed] [Google Scholar]
- 18.Kuran I, Ozcan H, Usta A, Bas L. Comparison of four different types of osteotomes for lateral osteotomy: A cadaver study. Aesthetic Plast Surg. 1996;20:323–6. doi: 10.1007/BF00228464. [DOI] [PubMed] [Google Scholar]
- 19.Koc B, Koc EA, Erbek S. Comparison of clinical outcomes using a piezosurgery device vs. A conventional osteotome for lateral osteotomy in rhinoplasty. Ear Nose Throat J. 2017;96:318–26. doi: 10.1177/014556131709600819. [DOI] [PubMed] [Google Scholar]
- 20.Yaman Z, Suer B. Piezoelectric surgery in oral and maxillofacial surgery. Ann Oral Maxillofac Surg. 2013;1:5. doi: 10.1016/j.ijom.2013.05.003. [DOI] [PubMed] [Google Scholar]