

Abstract
Objectives
Type D personality is associated with psychological and physical ill‐health. However, there has been limited investigation of the role of Type D personality in interventions designed to enhance well‐being. This study investigated associations between Type D personality and the efficacy of positive emotional writing for reducing stress, anxiety, and physical symptoms.
Design
A between‐subjects longitudinal design was employed.
Method
Participants (N = 71, M age = 28.2, SD age = 12.4) completed self‐report measures of Type D personality, physical symptoms, perceived stress, and trait anxiety, before completing either (1) positive emotional writing or (2) a non‐emotive control writing task, for 20 min per day over three consecutive days. State anxiety was measured immediately before and after each writing session, and self‐report questionnaires were again administered 4 weeks post‐writing.
Results
Participants in the positive emotional writing condition showed significantly greater reductions in (1) state anxiety and (2) both trait anxiety and perceived stress over the 4‐week follow‐up period, compared to the control group. While these effects were not moderated by Type D personality, a decrease in trait anxiety was particularly evident in participants who reported both high levels of social inhibition and low negative affectivity. Linguistic analysis of the writing diaries showed that Type D personality was positively associated with swear word use, but not any other linguistic categories.
Conclusion
These findings support the efficacy of positive emotional writing for alleviating stress and anxiety, but not perceived physical symptoms. Swearing may be a coping strategy employed by high Type D individuals.
Statement of contribution.
What is already known on this subject?
Type D (distressed) personality is characterized by high levels of both negative affectivity and social inhibition, and has been associated with adverse physical and psychological health.
Positive emotional writing is known to reduce subjectively reported physical symptoms and increase positive affect.
What does this study add?
Positive emotional writing was shown to attenuate (1) state anxiety immediately post‐writing, and (2) trait anxiety and perceived stress 4 weeks post‐writing.
The findings demonstrate that positive writing might be a useful intervention for attenuating the adverse psychological effects of Type D personality in the general population.
Type D personality was associated with more frequent use of swear words, which may be a coping mechanism used by high Type D individuals.
Keywords: Type D personality, positive emotional writing, stress, anxiety, physical symptoms
Background
Type D (distressed) personality is characterized by high levels of both negative affectivity (NA) and social inhibition (SI; Denollet, 2005). Type D individuals tend to experience negative emotions, but due to their socially inhibitive nature, may not have the opportunity to express their emotions, and thus may internalize their negative thoughts and feelings (Denollet, 2005). Type D personality has been associated with a disproportionately high prevalence of coronary heart disease and hypertension, and a range of adverse health outcomes in coronary patients (Denollet et al., 1996; Svansdottir et al., 2013). However, the Type D construct has faced criticism, largely because its initial promise as a predictor of cardiac mortality has not been realized following failed replications of this effect (Coyne & de Voogd, 2012; Coyne et al., 2011). Nevertheless, a number of recent studies have begun to investigate the relationship between Type D personality and health outcomes in the general population of ‘otherwise healthy’ individuals. For example, Type D personality is associated with poorer self‐reported health in the general population (Smith et al., 2018; Stevenson & Williams, 2014; Williams, Abbott, & Kerr, 2016). Additionally, within the general population, Type D personality has been associated with increases in self‐reported depression and anxiety (Michal, Wiltink, Grande, Beutel, & Brahler, 2011), dysregulated stress reactivity (Bibbey, Carroll, Ginty, & Phillips, 2015; Howard & Hughes, 2013; Kelly‐Hughes, Wetherell, & Smith, 2014), sleep problems (Conden, Ekselius, & Aslund, 2013), lower subjective quality of life (Stevenson & Williams, 2014), reductions in perceived social support (Williams et al., 2008), maladaptive coping strategies (Booth & Williams, 2015), and adverse health behaviours (Williams et al., 2016).
Despite the associations that have been reported between Type D personality and adverse psychological and physical health outcomes in the general population, attempts to develop suitable interventions to attenuate the adverse health outcomes associated with Type D personality have been limited. One recent study investigated the influence of an 8‐week mindfulness‐based stress reduction intervention on the components of Type D personality (Nyklicek, van Beugen, & Denollet, 2013). While this intervention attenuated NA and SI relative to a waitlist control condition, there was no influence of the intervention on Type D ‘caseness’. The lack of a reduction in Type D caseness is not unsurprising, given that the relative stability of the Type D construct over time has been established (Kupper, Boomsma, de Geus, Denollet, & Willemsen, 2011). However, there exists a lack of research which has investigated suitable approaches to tackling the adverse emotional and health outcomes associated with Type D personality, rather than attempts to modify the trait itself. Further, the intervention administered by Nyklicek et al. (2013) involved attendance at large group sessions, which may not be appealing to high Type D individuals due to their socially inhibitive nature. Thus, there exists a novel opportunity to test the role of Type D personality in relation to the efficacy of an evidence‐based intervention which is reasonably easy to self‐administer at a time and place convenient to the individual, and for which its efficacy with respect to improving psychological and physical well‐being has been supported.
Emotional expressive writing is one such technique, which has been associated with a range of psychological and physical health benefits (Pennebaker, 1997). Perhaps the best known expressive writing paradigm is written emotional disclosure (WED). WED typically involves writing for 20 min per day over 3 days about an important emotional issue which has affected the individual's life and has been associated with a range of outcomes including decreases in self‐reported depression and physical symptoms, work absenteeism, and GP visits (Pennebaker, 1997). Other forms of WED, such as writing about deeply traumatic experiences, have been associated with enhanced immune function (Pennebaker, Kiecolt‐Glaser, & Glaser, 1988), but it is also known that the efficacy of writing about negative emotions is susceptible to individual differences and may be context‐dependent (Pennebaker, 1997).
Positive psychology interventions encourage individuals to consider and evaluate positive aspects of their lives (Sin & Lyubomirsky, 2009). The feasibility and efficacy of these types of interventions have been reliably demonstrated, with extant evidence suggesting that positive psychology interventions can enhance well‐being and attenuate depression symptoms (Bolier et al., 2013; Sin & Lyubomirsky, 2009). Positive emotional writing is one such intervention, which has also been associated with improvements in both psychological and physical health. Similar to WED, this technique typically involves writing for 20 min per day over three consecutive days, but in this case, individuals are instructed to write about intensely positive experiences (Burton & King, 2004). Positive emotional writing has been associated with a reduction in subjectively reported physical symptoms (Burton & King, 2008), increased positive affect and fewer health centre visits over a 3‐month post‐writing follow‐up period in comparison with a control group who wrote about neutral, non‐emotive topics (Burton & King, 2004). Writing about positive experiences has also been shown to enhance emotional intelligence and life satisfaction (Wing, Schutte, & Byrne, 2006), while written benefit finding (writing about the benefits gained from an upsetting experience) is associated with increases in positive affect (Guastella & Dadds, 2006), but findings have been mixed, with another study failing to observe any benefits of positive emotional writing on self‐reported physical symptoms and anxiety, relative to neutral writing, in undergraduate students (Kloss & Lisman, 2002). However, Type D personality is associated with a greater prevalence of self‐reported physical symptoms (Smith et al., 2018; Stevenson & Williams, 2014; Williams et al., 2016) and low mood (Michal et al., 2011), both of which are known to be alleviated by positive emotional writing (Burton & King, 2004, 2008). On this basis, there exists a rationale for testing whether a decrease in self‐reported physical symptoms, stress, and anxiety from positive emotional writing is related to Type D personality.
A further benefit of conducting an emotional writing intervention in conjunction with a measure of Type D personality is the opportunity to interrogate relationships between emotional language use and Type D personality. Previous studies have suggested associations between personality and language use; for example, neuroticism is positively associated with negative emotional word use and negatively associated with positive emotional word use, while extraversion is positively associated with both positive emotional word use and social word use (Pennebaker & King, 1999). Further, frequency of first‐person singular pronoun use (e.g., ‘I’, ‘me’, ‘mine’) has been associated with depression (Pennebaker, Mehl, & Niederhoffer, 2003; Rude, Gortner, & Pennebaker, 2004) and suicidality (Stirman & Pennebaker, 2001). Additionally, word use has been associated with physical health and mortality, with positive emotional word use being associated with increased longevity (Danner, Snowdon, & Friesen, 2001). To the best of our knowledge, no studies to date have evaluated associations between language use and Type D personality, thus we sought here to address this gap in the literature.
The aim of this study was to investigate the influence of Type D personality on changes in (1) state anxiety, (2) trait anxiety, (3) perceived stress, and (4) self‐reported physical symptoms, following a 3‐day positive emotional writing intervention, relative to a neutral writing task. State anxiety was measured immediately before and after each writing session, while trait anxiety, perceived stress, and physical symptoms were measured at baseline and 4 weeks post‐writing. It was hypothesized that positive emotional writing would be associated with reductions in state anxiety, trait anxiety, perceived stress, and physical symptoms relative to writing about neutral topics. It was further hypothesized that there would be an interaction with Type D personality, such that the benefits of positive writing would be greater for high Type D individuals, given that these individuals are likely to experience relatively poorer psychological and physical well‐being, and thus may experience greater benefits from an intervention designed to tackle these issues. A secondary aim was to investigate whether Type D personality was related to language use. It was hypothesized that Type D personality would be associated with greater negative emotion word use and predicated by Pennebaker and colleagues (Pennebaker et al., 2003; Stirman & Pennebaker, 2001), greater use of first‐person singular pronouns.
Method
Participants
A total of 71 participants (19 males, M age = 28.2, SD age = 12.4) took part in this study. Participants were recruited via email and poster advertising. Exclusion criteria were not being fluent in written English and the presence of a diagnosed physical or psychological health condition. Participants received either £10 in cash or course credit (for eligible undergraduate students) upon returning all study materials as compensation for their time.
Materials
DS‐14
The DS‐14 (Denollet, 2005) was employed to measure Type D personality. This 14‐item questionnaire comprises two 7‐item subscales: NA (e.g., ‘I take a gloomy view of things’) and SI (e.g., ‘I often feel inhibited in social interactions’). Two positively worded items on the SI subscale (e.g., ‘I often talk to strangers’) were reverse scored. Responses to each item were made on a five‐point scale ranging between 0 and 4, yielding a total score of between 0 and 28 for each subscale. Both subscales have been found to demonstrate good internal consistency (NA: α = .88, SI: α = .86; Denollet, 2005).
Cohen Hoberman Inventory of Physical Symptoms
The Cohen Hoberman Inventory of Physical Symptoms (CHIPS; Cohen & Hoberman, 1983) was employed as a measure of physical symptoms. Participants indicated how much bother or distress they had experienced, in the past 2 weeks, as a result of each of 33 common physical symptoms, for example, ‘back pain’, ‘headache’, ‘cold or cough’. Participants responded on a five‐point scale ranging from 0 (have not been bothered by the problem) to 4 (problem has been an extreme bother). Responses on each item were summed to provide a total score ranging between 0 and 132. An association between Type D personality and CHIPS scores has been reported previously (Smith et al., 2018; Stevenson & Williams, 2014).
State‐Trait Anxiety Inventory
The State‐Trait Anxiety Inventory (STAI; Spielberger, 1983) incorporates two 20‐item subscales, measuring (1) state anxiety and (2) trait anxiety, with responses measured on a 4‐point Likert scale. The trait anxiety subscale of the STAI required participants to rate how they ‘generally feel’ and the state anxiety subscale asked participants to rate how they feel ‘right now, that is, at this moment’. Positively worded items (e.g., ‘I feel pleasant’) were reverse scored, so that a score of 4 for an individual item represented the highest level of anxiety. A total score for each subscale was calculated by summing together the scores for each of the 20 items on that subscale.
Perceived Stress Scale‐10
The Perceived Stress Scale‐10 (PSS; Cohen, Kamarck, & Mermelstein, 1983) is a 10‐item questionnaire which was used in this study as a measure of perceived background stress. The single‐factor scale asked the participant to report the extent to which they experienced various potentially stressful events in the previous month (e.g., ‘how often have you found that you could not cope with all the things that you had to do?’). Participants responded on a five‐point scale ranging from ‘never’ (0) to ‘very often’ (4). Four positively worded items were reverse scored and the score for each item summed to yield a total score ranging between 0 and 40.
Writing booklets
On each day, participants completed a writing booklet. These comprised the state anxiety subscale of the STAI (see above), followed by a number of lined pages for them to complete the assigned writing task for that day. Following the lined pages, the state anxiety subscale of the STAI was again presented.
Procedure
The study procedure was granted ethical approval by the relevant institutional ethics committee. A single‐blind design was employed. Informed consent was obtained from all individual participants included in the study. Upon providing consent to take part, participants completed the DS14, PSS, STAI trait anxiety subscale, and CHIPS. They were also given an additional copy of each of the PSS, STAI trait anxiety subscale, and CHIPS, and were prompted to complete them exactly 4 weeks after their first writing day. They were then provided with three writing booklets and instructions for the writing task, depending on the writing condition to which they were randomly assigned. All participants were asked to write for three consecutive days within the following week, at a time and place convenient to them. They were asked to avoid the likelihood of disruption where possible, by turning off their phones and choosing a quiet location to write where they were unlikely to be interrupted. On each writing day, participants first completed the state anxiety subscale of the STAI and then were required to write for 20 min about an assigned topic. Participants in the positive writing condition were asked to write about ‘positive experiences’. They were given the following instructions: ‘Think of the most wonderful experience or experiences in your life, happiest moments, ecstatic moments, moments of rapture, perhaps from being in love, or from listening to music, or suddenly ‘being hit’ by a book or painting or from some great creative moment. Choose one such experience or moment. Try to imagine yourself at that moment, including all the feelings and emotions associated with the experience. Now write about the experience in as much detail as possible trying to include the feelings, thoughts, and emotions that were present at the time. Please try your best to re‐experience the emotions involved’. (Burton & King, 2004). Participants were asked to follow these same writing instructions on each of the study days and were told that they could either write about the same experience on each day or write about a new one. Participants in the neutral writing condition were asked to write about ‘aspects of daily life’ and were asked specifically to write about their plans for the rest of the day (Day 1), a detailed description of the shoes they were wearing (Day 2) and a detailed description of their bedroom (Day 3; Burton & King, 2004). After 20 min of writing about their assigned topic, participants completed the state anxiety subscale of the STAI for a second time. Four weeks following consent, participants were reminded by text and/or email to complete the PSS, STAI trait anxiety subscale, and CHIPS 4 weeks after their third writing day. Upon completion of these follow‐up questionnaires, participants returned all study materials to the researcher.
Treatment of data
On each writing day, pre‐writing state anxiety scores were subtracted from post‐writing state anxiety scores to derive a state anxiety change score for each day. These were then averaged to derive a mean state anxiety change score across all of the writing days, for use as the dependent variable in the state anxiety analysis. Similarly, for the trait anxiety, PSS, and CHIPS measures, baseline scores were subtracted from 4‐week follow‐up scores, to derive a change score for each measure. All essays were transcribed and entered into the software program Linguistic Inquiry and Word Count (LIWC; Pennebaker, Booth, Boyd, & Francis, 2015) to enable linguistic analysis. Separate analyses were performed for each linguistic category. For the purpose of a manipulation check, we were interested in the effect of writing condition on affective process word use and ‘time orientation’ word use (i.e., whether word use reflected past, present, or future focus). We were also interested in the association between Type D personality and affective process, social process, and swear word use, as well as use of personal pronouns. For further details of the psychometric properties of LIWC and the number of words per category, see Pennebaker, Boyd, Jordan, and Blackburn (2015).
Predicated by Ferguson et al. (2009), we conceptualized Type D personality as a continuous construct for the purpose of this investigation. Data were analysed using multiple linear regression, following the procedure outlined by West, Aiken, and Krull (1996) for analysing categorical (condition) by continuous (NA and SI) variable interactions. NA and SI were mean centred, and the mean centred variables used in the IVs as well as each of the interaction terms. The following variables were entered as IVs: NA, SI, condition (coded as 0 = neutral writing, 1 = positive writing), NA × SI (Type D personality), NA × condition, SI × condition, NA × SI × condition.
Two participants returned the writing diaries and completed the pre‐ and post‐writing state anxiety measures, but did not complete any of the follow‐up questionnaires. Therefore, the trait anxiety, PSS, and CHIPS analyses are based on the 69 participants for whom these data were available. A further two participants neglected to complete the post‐writing state anxiety scales, and thus, the state anxiety analyses are based on the 69 participants for whom both pre‐ and post‐writing state anxiety data were available. Data were available for all 71 participants to enable LIWC analyses. For the analyses performed, this sample size was sufficient to detect a medium‐to‐large effect (f 2 = 0.23), with 0.8 power, at an alpha level of.05.
Results
There were no significant differences with respect to age (p = .25), Type D score (p = .62) or baseline scores on trait anxiety (p = .57), the PSS (p = .88), and the CHIPS (p = .29), between participants randomized to the positive and neutral writing conditions.
Manipulation check
There was no significant effect of any of the IVs on word count (all p values > .15). There were significant effects of condition, whereby participants assigned to the positive condition used more affect process words (e.g., ‘happy’, ‘cried’), B = 2.766, p < .001; positive emotion words (e.g., ‘love’, ‘nice’, ‘sweet’), B = 2.187, p < .001; negative emotion words (e.g., ‘hurt’, ‘ugly’, ‘nasty’), B = 0.543, p = .002; social process words (e.g., ‘mate’, ‘talk’, ‘they’), B = 2.194, p = .002; and past focus words (e.g., ‘ago’, ‘did’, ‘talked’), B = 4.121, p < .001. Participants assigned to the neutral condition used more present focus words (e.g., ‘today’, ‘is’, ‘now’), B = −4.069, p < .001; and future focus words (e.g., ‘may’, ‘will’, ‘soon’), B = −1.045, p < .001. There were no further significant effects for any of the other affective or social process word categories (see Table 1).
Table 1.
Unstandardized regression coefficients representing the relationships between each of the IVs and selected LIWC variables (word count, personal pronouns, affective processes words, social process words, time orientations, and swear words)
| NA | SI | Condition | NA × SI | NA × Condition | SI × Condition | NA × SI × Condition | |
|---|---|---|---|---|---|---|---|
| Word count | 5.421 | −2.499 | 1.398 | −0.365 | 2.236 | −9.115 | 0.808 |
| First‐person singular pronouns | −0.024 | 0.041 | 1.158 | −0.005 | 0.075 | 0.001 | 0.006 |
| First‐person plural pronouns | 0.002 | 0.002 | 0.531* | −0.007 | 0.096 | −0.034 | 0.001 |
| Second‐person pronouns | 0.005 | 0.009 | 0.148 | 0.003 | −0.020 | 0.002 | −0.006 |
| Third‐person singular pronouns | 0.013 | −0.013 | 0.436 | −0.002 | 0.000 | 0.043 | 0.001 |
| Third‐person plural pronouns | 0.063* | −0.011 | −0.794*** | −0.004 | −0.023 | −0.026 | 0.008 |
| Affective processes | 0.033 | −0.045 | 2.766*** | −0.009 | −0.011 | 0.091 | 0.000 |
| Positive emotion | 0.016 | −0.016 | 2.187*** | −0.008 | 0.013 | 0.010 | 0.001 |
| Negative emotion | 0.015 | −0.023 | 0.543** | 0.000 | −0.020 | 0.073* | −0.002 |
| Anxiety | −0.005 | −0.005 | 0.286** | −0.001 | 0.006 | 0.025 | 0.001 |
| Anger | 0.011* | −0.010* | 0.026 | 0.000 | −0.015 | 0.013 | −0.001 |
| Sad | 0.003 | 0.003 | 0.219*** | 0.000 | −0.011 | 0.016 | −0.002 |
| Social processes | 0.077 | 0.005 | 2.194** | −0.009 | 0.189 | −0.062 | −0.007 |
| Past focus | −0.043 | 0.049 | 4.121*** | −0.017 | 0.166 | 0.039 | 0.022 |
| Present focus | 0.030 | 0.061 | −4.069*** | 0.012 | 0.026 | −0.213 | 0.001 |
| Future focus | 0.011 | 0.006 | −1.045*** | −0.001 | −0.001 | −0.045 | 0.006 |
| Swear words | 0.005 | −0.001 | 0.002 | 0.001** | −0.004 | 0.003 | −0.001 |
LIWC = Linguistic Inquiry and Word Count.
*p < .05; **p < .01; ***p < .001.
Self‐reported mood and physical symptoms
Effects of condition and Type D personality on each of the DVs state anxiety, trait anxiety, PSS, and CHIPS are shown in Table 2.
Table 2.
Effects of condition and Type D personality on each of the DVs state anxiety, trait anxiety, PSS, and CHIPS
| B (SE) | p | |
|---|---|---|
| State anxiety | ||
| NA | −0.057 (0.172) | .74 |
| SI | 0.100 (0.165) | .55 |
| Condition | −5.189 (1.179) | <.001 |
| NA × SI | −0.011 (0.022) | .60 |
| NA × Condition | 0.318 (0.247) | .20 |
| SI × Condition | −0.275 (0.227) | .23 |
| NA × SI × Condition | 0.034 (0.032) | .30 |
| Trait anxiety | ||
| NA | −0.028 (0.257) | .92 |
| SI | −0.420 (0.266) | .12 |
| Condition | −4.280 (1.853) | .02 |
| NA × SI | −0.066 (0.034) | .06 |
| NA × Condition | 0.062 (0.381) | .87 |
| SI × Condition | 0.013 (0.361) | .97 |
| NA × SI × Condition | 0.100 (0.050) | .05 |
| PSS | ||
| NA | 0.143 (0.188) | .45 |
| SI | −0.036 (0.194) | .85 |
| Condition | −3.788 (1.353) | .007 |
| NA × SI | −0.024 (0.25) | .34 |
| NA × Condition | −0.126 (0.278) | .65 |
| SI × Condition | −0.183 (0.264) | .49 |
| NA × SI × Condition | 0.061 (0.037) | .10 |
| CHIPS | ||
| NA | −0.532 (0.369) | .16 |
| SI | −0.602 (0.381) | .12 |
| Condition | −1.913 (2.661) | .48 |
| NA × SI | −0.043 (0.049) | .39 |
| NA × Condition | 0.772 (0.547) | .16 |
| SI × Condition | 0.618 (0.519) | .24 |
| NA × SI × Condition | 0.118 (0.072) | .10 |
CHIPS = Cohen Hoberman Inventory of Physical Symptoms, NA = negative affectivity, PSS = Perceived Stress Scale, SI = social inhibition.
Negative associations indicate a greater reduction in each DV between pre‐ and post‐writing (state anxiety) or between baseline and the 4‐week follow‐up (trait anxiety, PSS, and CHIPS).
State anxiety
There was a significant effect of condition, whereby participants assigned to the positive writing condition reported a greater decrease in state anxiety between pre‐ and post‐writing, averaged across the three writing days compared with those in the control condition, B = −0.011, p < .001. There were no significant effects for any of the other IVs.
Trait anxiety
For trait anxiety, there was a significant effect of condition, whereby participants assigned to the positive writing condition reported a greater decrease in trait anxiety between baseline and the 4‐week follow‐up compared with those in the control condition, B = −4.280, p = .024. Further, the NA × SI × Condition interaction effect approached significance, B = 0.100, p = .050. Inspection of the regression lines generated by the regression equations for this statistical model indicated that the combination of low NA and high SI was associated with the most substantial reduction in trait anxiety following positive writing. The combination of low NA and high SI was also associated with the greatest reduction in trait anxiety for the positive, relative to the neutral writing condition (Figure 1).
Figure 1.
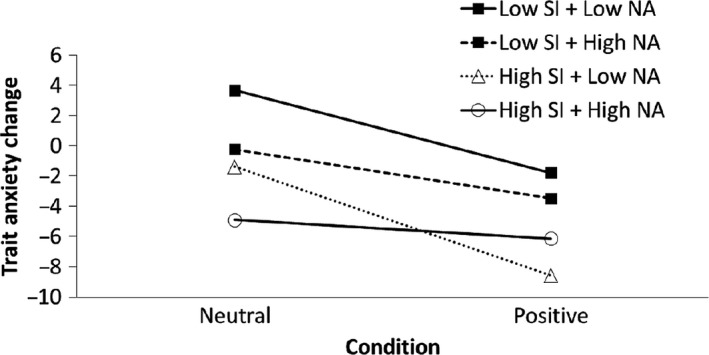
Regression lines showing changes in trait anxiety for each emotional writing condition at specified levels of negative affectivity (NA) and social inhibition (SI) (low = 1 standard deviation below the mean; high = 1 standard deviation above the mean).
Perceived Stress Scale
There was a significant effect of condition, whereby participants assigned to the positive writing condition reported a greater decrease in PSS scores between baseline and the 4‐week follow‐up compared with those in the control condition, B = −3.788, p = .007. There were no significant effects for any of the other IVs.
Cohen Hoberman Inventory of Physical Symptoms
There were no significant effects of NA, SI, condition, or any of the interaction terms on the change in CHIPS scores between baseline and the 4‐week follow‐up.
Association between Type D personality and word use
There was a positive effect of the SI × Condition interaction on negative emotion word use, B = 0.73, p = .031. Additionally, there was a positive effect of NA on anger word use (e.g., ‘hate’, ‘kill’, ‘annoyed’), B = 0.11, p = .029; and a negative effect of SI on anger word use, B = −0.01, p = .049. There was a positive effect of Type D (NA × SI) on swear word use, B = 0.001, p = .004. Finally, there were no significant effects of any of the IVs on personal pronoun use, with the exception of a positive effect of NA on third‐person plural pronoun use (e.g., ‘they’, ‘their’, ‘they'd’), NA: B = 0.063, p = .036 (see Table 1).
Discussion
The aim of the present study was to investigate the association between Type D personality and self‐reported psychological and physical health benefits of positive emotional writing, versus non‐emotive writing. Positive emotional writing reduced state anxiety during the writing sessions, relative to a neutral writing task. Further, a greater reduction in trait anxiety and perceived stress was observed during the 4‐week post‐intervention period for the positive writing condition, compared to the non‐emotive control writing condition, suggesting that the psychological benefits of positive emotional writing persist for at least 4 weeks following engagement with writing. Additionally, for trait anxiety, positive writing was particularly beneficial for individuals who reported high SI, in the context of low NA.
Our findings support previous work which has suggested that positive emotional writing is associated with increases in positive affect over a 3‐month period (Burton & King, 2004). However, unlike previous studies, we found no evidence to support the notion that positive emotional writing can benefit physical health. While we used a self‐report measure of physical symptoms as an indicator of physical health, some previous studies (e.g., Burton & King, 2004) have used different measures of physical health such as retrospectively self‐reported health centre visits. It is possible that self‐report methods for measuring physical symptoms are not sufficiently sensitive to writing interventions or that self‐reported health service utilization represents a subtly different aspect of health. Therefore, future work investigating the effects of positive emotional writing on physical health in Type D individuals should consider alternative measures of physical health, including objectively reported medical visits or biological indices.
It was somewhat surprising that Type D personality was not associated with reductions in physical symptoms, stress, or anxiety. However, participants high on SI, in the context of low NA, experienced a relatively greater decrease in trait anxiety following positive writing. This suggests that individuals who are closed, reserved, and tend to avoid social interaction, and therefore may have limited opportunity to express their emotions, may particularly benefit from positive emotional writing, even if their overall level of NA is not particularly high. While Type D personality was not associated with changes in state anxiety or perceived stress, all study participants reported a decrease in state anxiety and perceived stress. Therefore, positive writing conferred psychological benefits for all participants, and there was no detrimental effect of writing for participants with high Type D personality scores. On this basis, it is suggested that positive emotional writing is a useful intervention for reducing stress and anxiety, and may deliver particular benefits for more socially inhibited individuals (in the context of low NA). This latter finding is particularly noteworthy, given that emotional writing tasks can be completed at a time and place convenient to the individual, which may be particularly convenient for more socially inhibited individuals who may be less inclined to pursue other therapeutic avenues, which may require interaction with a therapist or other clients. However, it is intriguing that the positive writing benefits associated with SI occurred only in the context of low NA. Speculatively, it may be the case that when levels of NA are also high, then any particular benefits of positive writing for high SI individuals may be diminished by the high basal levels of negative emotionality in this group.
A key strength of the present study was the use of LIWC software to enable linguistic analysis of the written essays which participants produced as part of the writing tasks. This enabled participants’ adherence to the writing task instructions to be reliably ascertained. Firstly, it is noteworthy that no IVs were significantly associated with the average word count of the essays across the 3 days of writing. This suggests that despite the relatively mundane topics which participants were required to write about in the neutral condition, task engagement did not differ between writing conditions. Unsurprisingly, there was greater positive emotion word use in the positive writing condition, but unexpectedly, participants in the positive writing condition also used a greater frequency of negative emotion words, relative to the neutral writing condition. This result may be due to (1) low emotive language use more generally in the neutral condition, (2) a tendency of participants in the positive condition to compare overwhelmingly positive experiences to former negative experiences (e.g., ‘My most wonderful moment was when I was in a sad state in the 3rd year of university…’), and (3) use of a negative verb preceded by the word ‘not’ (e.g., ‘we were not disappointed’). Participants in the positive emotional writing condition used a greater frequency of social process words, which was unsurprising given that many positive experiences which participants wrote about in this condition involved social encounters. Finally, participants in the positive emotional writing condition used relatively more past focus words, and relatively fewer present and future focus words. Again, this is unsurprising given that participants in the positive writing condition were asked to reflect on an emotive past experience, whereas the neutral writing tasks required participants to focus more on the present (i.e., description of bedroom and shoes) and future (i.e., description of plans for the rest of the day). Taken together, all of these findings provide confidence that participants adhered to the writing instructions provided to them.
A further advantage of undertaking the linguistic analysis was that it provided insight into the associations between Type D personality and language use. It was anticipated that Type D personality would be associated with emotive language use, but the only such relationships observed were for anger word use, whereby a positive association was observed for NA and a negative association was observed for SI. By contrast, Type D personality was positively associated with swear word use. As an explanation for this finding, it is known that acutely elevated emotional arousal increases swearing fluency (Stephens & Zile, 2017) and enhances coping with physical pain (Stephens, Atkins, & Kingston, 2009). By extension, Type D personality is associated with chronically high emotional arousal and it is feasible that swearing is used as a coping mechanism among high Type D individuals. Additionally, we hypothesized that Type D personality may have been associated with first‐person pronoun use. This is because greater first‐person singular pronoun use is an indicator of self‐focus and has been associated with an array of adverse physical and psychological health outcomes which are also characteristic of Type D personality (Pennebaker et al., 2003; Stirman & Pennebaker, 2001). However, no such relationship emerged here. With respect to the linguistic analysis, a key consideration is that the language use of participants may have been confounded by the specific task instructions and may not be indicative of natural language use. Therefore, an important future direction for this work is to (1) replicate the observations reported here with respect to the anger and swear word use, and (2) investigate the relationship between personal pronoun use and Type D personality using a more natural free writing task, whereby participants can write about a topic of their own choosing.
A further strength of this study was the use of a 4‐week follow‐up period to ascertain the medium‐term effects of positive writing. However, this follow‐up period was notably shorter than some previous investigations of positive emotional writing which have demonstrated the persistence of writing‐induced effects for up to 3 months (Burton & King, 2004). It is not clear whether the benefits of positive writing on stress and anxiety reported here would persist over this timeframe, given that Type D personality is associated with substantial and chronic low mood. Such episodes of low mood may disrupt any beneficial effects of positive writing. Therefore, future investigations of psychological interventions for high Type D individuals should comprise a longer term follow‐up phase to ascertain the duration over which writing effects persist in this group. A further limitation is the sample size of the present study. While the sample size employed was not substantively different from other studies which have investigated the influence of positive emotional writing on similar outcomes (Burton & King, 2004, 2009), the study was adequately powered only to observe significant findings where the effect sizes were medium‐to‐large. Thus, a larger sample size may have been able to detect some more subtle effects. Additionally, demand characteristics may be an important consideration in emotional writing studies. While participants were not made aware prior to taking part in the study that there were two study conditions, which may partially offset this issue, it is feasible that an unconscious bias may have led participants in the positive writing condition to respond more positively to the self‐report measures. The single‐blind approach taken may have exacerbated any demand characteristics, thus future studies in this area should employ a double‐blind procedure to minimize any researcher expectancy effects.
In conclusion, the present study found that positive emotional writing can reduce state anxiety, as well as trait anxiety and perceived stress for 4 weeks post‐writing. Additionally, while Type D personality was not associated with a reduction in stress, anxiety, or physical symptoms as a consequence of emotional writing for trait anxiety, positive writing was particularly beneficial with respect to a decrease in trait anxiety for individuals who reported high SI (in combination with low NA). This is particularly noteworthy given that high SI individuals are less likely to seek therapeutic intervention which requires social interaction; therefore, positive emotional writing, which can be conducted in isolation and at a time and place which is convenient to the individual, may be particularly beneficial for this group. The general decline in stress and anxiety observed across all participants in the sample indicates that positive emotional writing is a beneficial exercise for the general population, with Type D personality not playing a moderating role in its efficacy. In addition, this is the first study to investigate the association between language use and Type D personality. Type D personality was positively associated with swear word use, which may be used as a coping mechanism by high Type D individuals. Further work is needed to ascertain the relationships between Type D personality and natural language use, as well as whether there are associations between the language use of high Type D individuals and both psychological and physical health outcomes.
Conflict of interest
All authors declare no conflict of interest.
References
- Bibbey, A. , Carroll, D. , Ginty, A. T. , & Phillips, A. C. (2015). Cardiovascular and cortisol reactions to acute psychological stress under conditions of high versus low social evaluative threat: Associations with the type D personality construct. Psychosomatic Medicine, 77, 599–608. 10.1097/PSY.0000000000000194 [DOI] [PubMed] [Google Scholar]
- Bolier, L. , Haverman, M. , Westerhof, G. J. , Riper, H. , Smit, F. , & Bohlmeijer, E. (2013). Positive psychology interventions: A meta‐analysis of randomized controlled studies. BMC Public Health, 13(1), 119 10.1186/1471-2458-13-119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Booth, L. , & Williams, L. (2015). Type D personality and dietary intake: The mediating effects of coping style. Journal of Health Psychology, 20, 921–927. 10.1177/1359105315573433 [DOI] [PubMed] [Google Scholar]
- Burton, C. M. , & King, L. A. (2004). The health benefits of writing about intensely positive experiences. Journal of Research in Personality, 38, 150–163. 10.1016/S0092-6566(03)00058-8 [DOI] [Google Scholar]
- Burton, C. M. , & King, L. A. (2008). Effects of (very) brief writing on health: The two‐minute miracle. British Journal of Health Psychology, 13(Pt 1), 9–14. 10.1348/135910707X250910 [DOI] [PubMed] [Google Scholar]
- Burton, C. M. , & King, L. A. (2009). The health benefits of writing about positive experiences: The role of broadened cognition. Psychology & Health, 24, 867–879. 10.1080/08870440801989946 [DOI] [PubMed] [Google Scholar]
- Cohen, S. , & Hoberman, H. M. (1983). Positive events and social supports as buffers of life change stress. Journal of Applied Social Psychology, 13, 99–125. 10.1111/j.1559-1816.1983.tb02325.x [DOI] [Google Scholar]
- Cohen, S. , Kamarck, T. , & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396. 10.2307/2136404 [DOI] [PubMed] [Google Scholar]
- Conden, E. , Ekselius, L. , & Aslund, C. (2013). Type D personality is associated with sleep problems in adolescents. Results from a population‐based cohort study of Swedish adolescents. Journal of Psychosomatic Research, 74, 290–295. 10.1016/j.jpsychores.2012.11.011 [DOI] [PubMed] [Google Scholar]
- Coyne, J. C. , & de Voogd, J. N. (2012). Are we witnessing the decline effect in the Type D personality literature? What can be learned? Journal of Psychosomatic Research, 73, 401–407. 10.1016/j.jpsychores.2012.09.016 [DOI] [PubMed] [Google Scholar]
- Coyne, J. C. , Jaarsma, T. , Luttik, M. L. , van Sonderen, E. , van Veldhuisen, D. J. , & Sanderman, R. (2011). Lack of prognostic value of type D personality for mortality in a large sample of heart failure patients. Psychosomatic Medicine, 73, 557–562. 10.1097/PSY.0b013e318227ac75 [DOI] [PubMed] [Google Scholar]
- Danner, D. D. , Snowdon, D. A. , & Friesen, W. V. (2001). Positive emotions in early life and longevity: Findings from the nun study. Journal of Personality and Social Psychology, 80, 804–813. 10.1037//0022-3514.80.5.804 [DOI] [PubMed] [Google Scholar]
- Denollet, J. (2005). DS14: Standard assessment of negative affectivity, social inhibition, and Type D personality. Psychosomatic Medicine, 67(1), 89–97. 10.1097/01.psy.0000149256.81953.49 [DOI] [PubMed] [Google Scholar]
- Denollet, J. , Sys, S. U. , Stroobant, N. , Rombouts, H. , Gillebert, T. C. , & Brutsaert, D. L. (1996). Personality as independent predictor of long‐term mortality in patients with coronary heart disease. Lancet, 347, 417–421. 10.1016/S0140-6736(96)90007-0 [DOI] [PubMed] [Google Scholar]
- Ferguson, E. , Williams, L. , O'Connor, R. C. , Howard, S. , Hughes, B. M. , Johnston, D. W. , … O'Carroll, R. E. (2009). A taxometric analysis of type‐D personality. Psychosomatic Medicine, 71, 981–986. 10.1097/PSY.0b013e3181bd888b [DOI] [PubMed] [Google Scholar]
- Guastella, A. J. , & Dadds, M. R. (2006). Cognitive‐behavioral models of emotional writing: A validation study. Cognitive Therapy and Research, 30, 397–414. 10.1007/s10608-006-9045-6 [DOI] [Google Scholar]
- Howard, S. , & Hughes, B. M. (2013). Type D personality is associated with a sensitized cardiovascular response to recurrent stress in men. Biological Psychology, 94, 450–455. 10.1016/j.biopsycho.2013.09.001 [DOI] [PubMed] [Google Scholar]
- Kelly‐Hughes, D. H. , Wetherell, M. A. , & Smith, M. A. (2014). Type D personality and cardiovascular reactivity to an ecologically valid multitasking stressor. Psychology and Health, 29, 1156–1175. 10.1080/08870446.2014.915970 [DOI] [PubMed] [Google Scholar]
- Kloss, J. D. , & Lisman, S. A. (2002). An exposure‐based examination of the effects of written emotional disclosure. British Journal of Health Psychology, 7(1), 31–46. 10.1348/135910702169349 [DOI] [PubMed] [Google Scholar]
- Kupper, N. , Boomsma, D. I. , de Geus, E. J. , Denollet, J. , & Willemsen, G. (2011). Nine‐year stability of type D personality: Contributions of genes and environment. Psychosomatic Medicine, 73(1), 75–82. 10.1097/PSY.0b013e3181fdce54 [DOI] [PubMed] [Google Scholar]
- Michal, M. , Wiltink, J. , Grande, G. , Beutel, M. E. , & Brahler, E. (2011). Type D personality is independently associated with major psychosocial stressors and increased health care utilization in the general population. Journal of Affective Disorders, 134(1–3), 396–403. 10.1016/j.jad.2011.05.033 [DOI] [PubMed] [Google Scholar]
- Nyklicek, I. , van Beugen, S. , & Denollet, J. (2013). Effects of mindfulness‐based stress reduction on distressed (type D) personality traits: A randomized controlled trial. Journal of Behavioral Medicine, 36, 361–370. 10.1007/s10865-012-9431-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pennebaker, J. W. (1997). Writing about emotional experiences as a therapeutic process. Psychological Science, 8, 162–166. 10.1111/j.1467-9280.1997.tb00403.x [DOI] [Google Scholar]
- Pennebaker, J. W. , Booth, R. J. , Boyd, R. L. , & Francis, M. E. (2015). Linguistic Inquiry and Word Count: LIWC2015. Austin, TX: Pennebaker Conglomerates. [Google Scholar]
- Pennebaker, J. W. , Boyd, R. L. , Jordan, K. , & Blackburn, K. (2015). The development and psychometric properties of LIWC2015. Austin, TX: University of Texas at Austin; https://doi.org/10.15781/T29G6Z [Google Scholar]
- Pennebaker, J. W. , Kiecolt‐Glaser, J. K. , & Glaser, R. (1988). Disclosure of traumas and immune function: Health implications for psychotherapy. Journal of Consulting and Clinical Psychology, 56, 239–245. 10.1037/0022-006X.56.2.239 [DOI] [PubMed] [Google Scholar]
- Pennebaker, J. W. , & King, L. A. (1999). Linguistic styles: Language use as an individual difference. Journal of Personality and Social Psychology, 77, 1296–1312. 10.1037/0022-3514.77.6.1296 [DOI] [PubMed] [Google Scholar]
- Pennebaker, J. W. , Mehl, M. R. , & Niederhoffer, K. G. (2003). Psychological aspects of natural language use: Our words, our selves. Annual Review of Psychology, 54, 547–577. 10.1146/annurev.psych.54.101601.145041 [DOI] [PubMed] [Google Scholar]
- Rude, S. S. , Gortner, E. M. , & Pennebaker, J. W. (2004). Language use of depressed and depression‐vulnerable college students. Cognition & Emotion, 18, 1121–1133. 10.1080/02699930441000030 [DOI] [Google Scholar]
- Sin, N. L. , & Lyubomirsky, S. (2009). Enhancing well‐being and alleviating depressive symptoms with positive psychology interventions: A practice‐friendly meta‐analysis. Journal of Clinical Psychology, 65, 467–487. 10.1002/jclp.20593 [DOI] [PubMed] [Google Scholar]
- Smith, M. A. , Riccalton, V. , Kelly‐Hughes, D. H. , Craw, O. A. , Allen, S. F. , O'Connor, D. B. , & Wetherell, M. A. (2018). The relationship between Type D personality and physical health complaints is mediated by perceived stress and anxiety but not diurnal cortisol secretion. Stress, 21, 229–236. 10.1080/10253890.2018.1435637 [DOI] [PubMed] [Google Scholar]
- Spielberger, C. D. (1983). Manual for the State‐Trait Anxiety Inventory (STAI). Palo Alto, CA: Consulting Psychologists Press. [Google Scholar]
- Stephens, R. , Atkins, J. , & Kingston, A. (2009). Swearing as a response to pain. NeuroReport, 20, 1056–1060. 10.1097/WNR.0b013e32832e64b1 [DOI] [PubMed] [Google Scholar]
- Stephens, R. , & Zile, A. (2017). Does emotional arousal influence swearing fluency? Journal of Psycholinguistic Research, 46, 983–995. 10.1007/s10936-016-9473-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stevenson, C. , & Williams, L. (2014). Type D personality, quality of life and physical symptoms in the general population: A dimensional analysis. Psychology and Health, 29, 365–373. 10.1080/08870446.2013.856433 [DOI] [PubMed] [Google Scholar]
- Stirman, S. W. , & Pennebaker, J. W. (2001). Word use in the poetry of suicidal and nonsuicidal poets. Psychosomatic Medicine, 63, 517–522. 10.1097/00006842-200107000-00001 [DOI] [PubMed] [Google Scholar]
- Svansdottir, E. , Denollet, J. , Thorsson, B. , Gudnason, T. , Halldorsdottir, S. , Gudnason, V. , … Karlsson, H. D. (2013). Association of Type D personality with unhealthy lifestyle, and estimated risk of coronary events in the general Icelandic population. European Journal of Preventive Cardiology, 20, 322–330. 10.1177/2047487312441723 [DOI] [PubMed] [Google Scholar]
- West, S. G. , Aiken, L. S. , & Krull, J. L. (1996). Experimental personality designs: Analyzing categorical by continuous variable interactions. Journal of Personality, 64(1), 1–48. 10.1111/j.1467-6494.1996.tb00813.x [DOI] [PubMed] [Google Scholar]
- Williams, L. , Abbott, C. , & Kerr, R. (2016). Health behaviour mediates the relationship between Type D personality and subjective health in the general population. Journal of Health Psychology, 21, 2148–2155. 10.1177/1359105315571977 [DOI] [PubMed] [Google Scholar]
- Williams, L. , O'Connor, R. C. , Howard, S. , Hughes, B. M. , Johnston, D. W. , Hay, J. L. , … O'Carroll, R. E. (2008). Type‐D personality mechanisms of effect: The role of health‐related behavior and social support. Journal of Psychosomatic Research, 64(1), 63–69. 10.1016/j.jpsychores.2007.06.008 [DOI] [PubMed] [Google Scholar]
- Wing, J. F. , Schutte, N. S. , & Byrne, B. (2006). The effect of positive writing on emotional intelligence and life satisfaction. Journal of Clinical Psychology, 62, 10.1002/jclp.20292 [DOI] [PubMed] [Google Scholar]