

Abstract
Objectives
Changing public awareness of antimicrobial resistance (AMR) represents a global public health priority. A systematic review of interventions that targeted public AMR awareness and associated behaviour was previously conducted. Here, we focus on identifying the active content of these interventions and explore potential mechanisms of action.
Methods
The project took a novel approach to intervention mapping utilizing the following steps: (1) an exploration of explicit and tacit theory and theoretical constructs within the interventions using the Theoretical Domains Framework (TDFv2), (2) retrospective coding of behaviour change techniques (BCTs) using the BCT Taxonomy v1, and (3) an investigation of coherent links between the TDF domains and BCTs across the interventions.
Results
Of 20 studies included, only four reported an explicit theoretical basis to their intervention. However, TDF analysis revealed that nine of the 14 TDF domains were utilized, most commonly ‘Knowledge’ and ‘Environmental context and resources’. The BCT analysis showed that all interventions contained at least one BCT, and 14 of 93 (15%) BCTs were coded, most commonly ‘Information about health consequences’, ‘Credible source’, and ‘Instruction on how to perform the behaviour’.
Conclusions
We identified nine relevant TDF domains and 14 BCTs used in these interventions. Only 15% of BCTs have been applied in AMR interventions thus providing a clear opportunity for the development of novel interventions in this context. This methodological approach provides a useful way of retrospectively mapping theoretical constructs and BCTs when reviewing studies that provide limited information on theory and intervention content.
Statement of contribution.
What is already known on this subject?
Evidence of the effectiveness of interventions that target the public to engage them with AMR is mixed; the public continue to show poor knowledge and misperceptions of AMR.
Little is known about the common, active ingredients of AMR interventions targeting the public and information on explicit theoretical content is sparse.
Information on the components of AMR public health interventions is urgently needed to enable the design of effective interventions to engage the public with AMR stewardship behaviour.
What does this study add?
The analysis shows very few studies reported any explicit theoretical basis to the interventions they described.
Many interventions share common components, including core mechanisms of action and behaviour change techniques.
The analysis suggests components of future interventions to engage the public with AMR.
Keywords: antimicrobial resistance, Theoretical Domains Framework, behaviour change techniques, components of public health interventions
Background
Antimicrobial resistance (AMR) is, according to the World Health Organisation, becoming a public health concern of paramount importance. AMR refers to the ability of a microorganism to prevent an antimicrobial from working. Such resistance threatens effective prevention and treatment of an ever‐increasing range of infections that are caused by bacteria, parasites, viruses, and fungi. It is suggested, for example, that the continued rise of AMR will lead to 390,000 people dying each year from AMR in Europe and a reduction of 2–2.5% of the Gross Domestic Product by 2050 (The Review on Antimicrobial Resistance, 2014). Thus, AMR is an urgent and escalating public health problem within the United Kingdom, wider Europe and the world (Hopkins, 2016).
Key drivers of AMR include the inappropriate use of antibiotics, the spread of health care‐associated infection between patients from health care to community settings, poor infection prevention and control practices within health care settings, transmission between animals and humans across the food chain and environmental factors such as waste water disposal from domestic, hospital, industrial, or livestock settings (Flowers, 2018; Levy & Marshall, 2004; Michael, Dominey‐Howes, & Labbate, 2014; Weinstein, 2001).
In human health care, the overuse of antibiotics is underpinned by inappropriate prescribing by health care providers (Charani, Castro‐Sanchez, & Holmes, 2014) and incomplete public knowledge and understanding about how and when to take antibiotics effectively (Gualano, Gili, Scaioli, Bert, & Siliquini, 2015; McCullough, Parekh, Rathbone, Del Mar, & Hoffmann, 2016; Pinder, Sallis, Berry, & Chadborn, 2015). There are also low levels of knowledge and understanding about perceived risk of AMR amongst the public (Gualano et al., 2015; Pinder et al., 2015). These factors contribute to the emergence, acceleration, and spread of AMR. Equipping the public with an understanding of AMR and its role within antimicrobial stewardship is therefore a central step towards the culture change that is needed to reduce the drivers of AMR. Engaging the public with AMR will also have synergistic effects on other interventions which directly address prescribers for example (Elouafkaoui et al., 2016; Treweek et al., 2016).
Given the importance of AMR, several governments across the world have their own AMR strategy documents. Within the United Kingdom, the O'Neill (2016) report on AMR demanded the prioritization of global AMR awareness interventions that address the general public at an estimated cost of between $40 and 100 million per year, yet there is no evidence base suggesting how best to engage the public effectively. Review‐level approaches to date have focussed upon effectiveness rather than detailing the key components of AMR interventions (King et al., 2016). Some evidence syntheses indicate these interventions are effective at increasing public knowledge and understanding in relation to AMR (Haynes & McLeod, 2015; Pinder et al., 2015), but, however, other evidence suggests that a range of current interventions are limited in their effectiveness (King et al., 2016). These mixed findings may relate to heterogeneity in study design, context, historical period, outcome measures, and populations (King et al., 2016). Critically, there have been no attempts to date to identify exactly what works, why it works, for whom, when, and in which circumstances. This lack of substantive detail makes it impossible to determine which intervention components are typically used or indeed which are associated with effectiveness.
In relation to why and how such interventions may work, there has been little focus upon the role of behaviour change theory and practice underpinning these interventions to date. The appropriate use of theory within behaviour change interventions is central to the effective design and evaluation of complex interventions (Craig et al., 2008; Glanz & Bishop, 2010; Noar, Benac, & Harris, 2007). The Medical Research Council guidance suggests that a key part of developing an intervention is the theoretical understanding of the likely process through which the intervention will achieve change, so that weak links in the causal chain connecting diverse intervention elements can be identified and strengthened. Theory in this way provides causal explanatory ‘short hand’ for how and why an intervention and its components are working, binding disparate intervention elements in a coherent and efficient way to maximize the use of resources and minimize extraneous intervention components (Davis, Campbell, Hildon, Hobbs, & Michie, 2015). Despite increasing recognition that the design of behaviour change interventions should be based on relevant theories, systematic reviews show that theory is rarely used explicitly within interventions (e.g., Glanz & Bishop, 2010; Michie & Prestwich, 2010). This trend is also evident in AMR interventions. Even when interventions have positive effects, the underlying mechanisms of action/behaviour change processes within interventions are often hidden within a ‘black box’, which does little to inform future interventions (Maindal, Kirkevold, Sandbaek, & Lauritzen, 2010). A lack of systematic process evaluation obscures assessment of intervention mechanisms (Moore et al., 2015).
It is likely that most interventions are designed with an implicit theory in mind; therefore, it may be useful to retrospectively identify which factors are being targeted and the extent to which these map onto pre‐existing theoretical constructs. Such an approach would be inferential, but would help build an evidence base for future intervention design (Little, Presseau, & Eccles, 2015). The Theoretical Domains Framework (TDFv2) represents a useful framework upon which to carry out a retrospective coding of theoretical content. The TDF is useful for this type of approach as it provides a comprehensive summary of the numerous factors which underpin behaviour change (Atkins et al., 2017).
Within the AMR public health interventions literature, there is also a lack of transparency regarding key intervention components (Rawson et al., 2017). These ‘active ingredients’ explain how an intervention exerts its effects (Craig et al., 2008), representing the proposed ‘mechanisms of change’ underpinning interventions. Behaviour change techniques (BCTs) are an effective way of coding the content of interventions, enabling the identification of the active ingredients within interventions. BCTs are described as the smallest component compatible with retaining the postulated active ingredients and can be used alone or in combination with other BCTs (Michie et al., 2013). The focus upon BCTs represents an attempt to develop a common language relating to key aspects of intervention content. Poor reporting of these active ingredients of interventions makes it impossible for others to understand, evaluate, and replicate the active content of behaviour change interventions (Abraham, Johnson, de Bruin, & Luszczynska, 2014; Wood et al., 2016). Taxonomies of BCTs can be used to classify the content of interventions using agreed definitions with precision and specificity (Michie et al., 2013). One widely utilized taxonomy is The Behaviour Change Techniques Taxonomy version 1 (BCTTv1). Previous research has demonstrated that the BCTTv1 can be used to identify the content of existing interventions (Presseau et al., 2015).
As part of a broader investigation using multiple analytic tools to examine the content and delivery of AMR public health interventions identified following a systematic review, the present study describes the examination of the content of published AMR public health interventions in relation to: (1) the behavioural domains being addressed; (2) the role of explicit and implicit theory/mechanisms of action within the interventions; and (3) the number and details of BCTs/mechanisms of change present within these interventions. In a fourth aim, we also explore the coherent links between the TDF domains/mechanisms of action and BCTs/mechanisms of change across the interventions. Given the heterogeneity of interventions and their outcomes, it was not possible to conduct any meta‐analytic approaches. Overall intervention effectiveness is examined elsewhere (Price et al., 2018).
Method
The review
Details of the systematic review undertaken to identify AMR public health interventions are reported in another paper (Price et al., 2018). A summary of the procedure undertaken for the review is provided here to provide a background to the current analysis.
Search strategy
CINAHL, Cochrane Library, EMBASE, MEDLINE, and PsycINFO electronic databases were searched for the articles published between the years 2000 and 2016 using keywords associated with four areas: the population – general public; the intervention – interventions designed to increase antimicrobial awareness and/or to improve antimicrobial stewardship behaviour; the context – AMR or antimicrobial stewardship; the outcomes – all relevant short, medium or long‐term outcomes related to AMR and/or antimicrobial stewardship behaviours (knowledge/awareness, learning, public behavioural, and cognition outcomes).
Study selection
Interventions targeting the general public population and designed to increase public antimicrobial awareness and/or to improve antimicrobial stewardship were deemed eligible to the review. The general public population was conceptualized as any members of the general public within any age group or role, apart from health care workers, patients, and other individuals recruited from health care settings. Furthermore, time bound geographical controls or ‘no exposure’ comparators and all relevant short‐, medium‐, or long‐term outcomes related to AMR and/or antimicrobial stewardship behaviours were included. The procedure for identifying relevant papers is shown in the PRISMA diagram in Figure 1.
Figure 1.
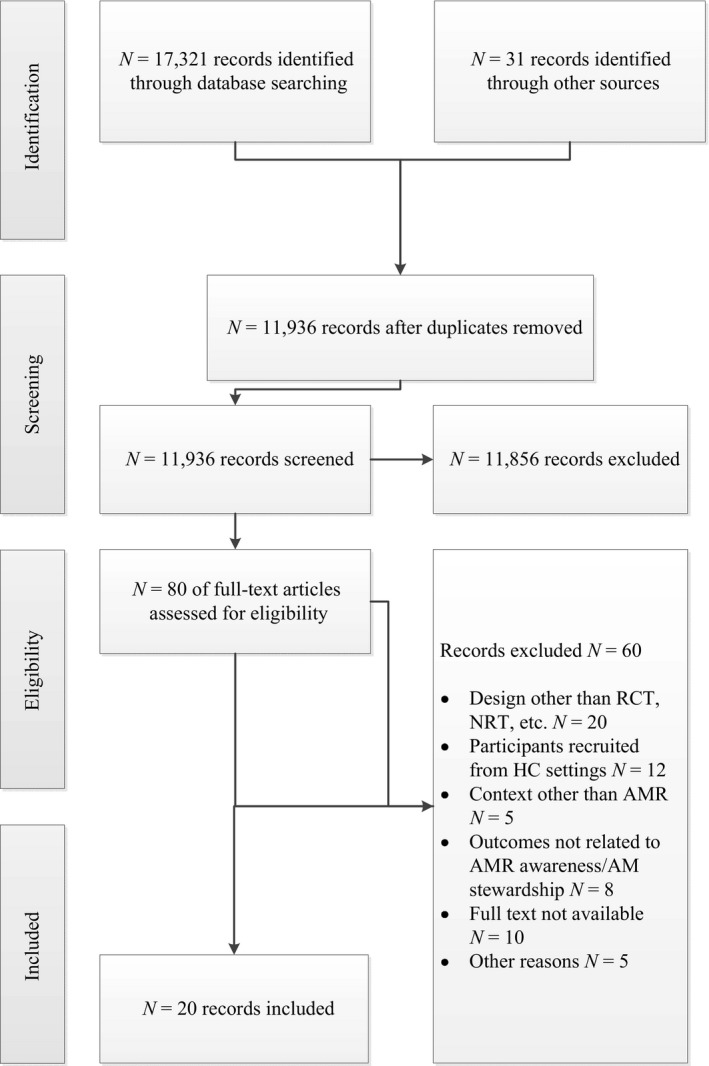
- Note: AM = antimicrobial; AMR = antimicrobial resistance; HC = health care; NRT = Non‐randomized Control Trial; RCT = Randomized Control Trial.
Data extraction – intervention descriptions
Verbatim descriptions of the intervention descriptions were extracted from the identified papers. In addition, up to three requests were made to the study authors of included studies for companion materials (e.g., survey instruments, intervention descriptions, mass media materials).
Coding of theory, TDF domains, and BCTs
The Theory Coding Scheme (Michie & Prestwich, 2010) was used to code explicit, reported theory within the intervention descriptions. In addition, two psychologists (PF and LW) independently coded inferred mechanisms of action within the interventions using the 14 domains of the TDFv2 (Cane, O'Connor, & Michie, 2012; Michie et al., 2005). The coders utilized a data extraction form that was designed for the study, with the coding of each domain that appeared to be targeted by the intervention supported by evidence from the text. Following discussion of the coding with a third party (JMcP), 100% agreement was achieved. Intervention descriptions were also coded for mechanisms of change using the Behaviour Change Technique Taxonomy v1 as proposed by Michie et al. (2013). BCT guidelines directed the coding process (Abraham & Michie, 2008). Each of the 93 BCTs within the BCTTv1 was considered for its presence within each intervention description. Three psychologists (PF, JMcP, LW) independently coded the intervention content of the 20 studies. As with the TDF analysis, the coders utilized a data extraction form that was designed for the study, with the coding of each BCT that appeared to be used by the intervention supported by evidence from the text. Again, following discussion, 100% agreement was achieved. As the purpose of the task was to identify the existence of BCTs within the AMR interventions, it was possible to code the same piece of intervention description using different BCTs. Congruence across TDF/BCT components was assessed by consideration of the logic of data extracted across stages and also using the connections between TDF domains and BCTs as explicated by Michie, Atkins, and West (2014).
Results
Twenty studies were identified from the review. These studies were led by professionals from a range of non‐psychology backgrounds, including medicine, public health, epidemiology, marketing, microbiology, and pharmacology. Table S1 shows the characteristics of the samples targeted by the interventions, the type of design adopted within the intervention studies and provides detail on the nature of the intervention, outcome measures, and significant results (see [Link], [Link]). Targets included the public (n = 7 interventions), children (n = 6 interventions), parents (n = 5 interventions), and university students (n = 1 intervention). All but three interventions demonstrated effectiveness within these samples (Formoso et al., 2013; Mainous, Diaz, & Carnemolla, 2009; McNulty, Nichols, Boyle, Woodhead, & Davey, 2010) (Price et al., 2018). The results relating to the content of interventions described within each study are structured according to four analytic foci (1) the behavioural domains being addressed within AMR public health interventions; (2) the role of theory/mechanisms of action within the interventions; (3) the number and details of BCTs/mechanisms of change present within these interventions; (4) coherent links between the TDF theoretical constructs and BCTs present within the interventions.
The behavioural domains being addressed within AMR public health interventions
Table S2 details the behavioural domains addressed within the interventions, along with the theoretical content within the interventions, presence of BCTs, and level of congruence between TDF domains and BCTs within each intervention (see [Link], [Link]). The behavioural domains were heterogeneous with most interventions targeting multiple behaviours, and/or their antecedents simultaneously. The behavioural domains addressed included the demand for and appropriate use of antibiotics (15 studies); encouraging symptom management and watchful waiting (seven studies); transmission behaviours (behaviours preventing the spread of infection) (six studies); engaging with health professionals to get a prescription or to seek advice (four studies); and making a choice of treatment (one study).
The role of theory/mechanisms of action within the interventions
An analysis of explicit theory within the interventions using the Theory Coding Scheme (Michie & Prestwich, 2010) demonstrated that an explicit theoretical basis was only evident in four of the studies (see Table S2). However, 9/14 (64%) of the TDF domains were coded within the intervention descriptions. Table S2 provides an overview of the TDF domains identified within the intervention descriptions. The number of TDF domains identified from intervention descriptions varied from one to six. On average, three or so identifiable mechanisms of action were identified focussing mainly upon the idea of changing behaviour through increasing knowledge levels, changing the local environment to enable the desired behaviour change, using social and professional role and identity and through using social influence to encourage behaviour change. The most commonly coded domain was ‘Knowledge’ (coded in all 20 descriptions), followed by ‘Environmental context and resources’ (coded in 15 descriptions), ‘Social/professional role and identity’ (coded in 8 descriptions), ‘Social influences’ (coded in 6 descriptions), ‘Skills’ (coded in 3 descriptions), ‘Beliefs about consequences’ (coded in 3 descriptions), ‘Beliefs about capabilities’ (coded in 2 descriptions), ‘Memory, attention and decision processes’ (coded in 2 descriptions), and ‘Reinforcement’ (coded in 2 descriptions). Two TDF domains were unique amongst the most effective interventions: beliefs about capabilities (Stockwell et al., 2010; Wutzke et al., 2007) and reinforcement (Larson, Ferng, McLoughlin, Wang, & Morse, 2009; Wutzke et al., 2007).
The number and details of BCTs/mechanisms of change present within these interventions
BCT coding at group level
Table S2 contains illustrative examples of each of the group and individual BCTs identified within the intervention descriptions. Nine of the possible 16 groupings of BCTs from the BCTTV1 were found within the intervention descriptions. The most frequently used groups of BCTs were ‘Natural consequences’ (n = 16), stressing the psychological consequences of behaviour, and ‘Comparison of outcomes’ (n = 15), which focusses upon weighing up outcomes of behaviour change. ‘Shaping knowledge’ (n = 14) was also a common BCT grouping; as the name suggests these BCTs focus upon ways of enabling learning around AMR and antimicrobial stewardship. Other groupings were less common: ‘Antecedents’ (n = 7), ‘Associations’ (n = 6), ‘Repetition and substitution’ (n = 5), ‘Feedback and monitoring’ (n = 3), ‘Comparison of behaviour’ (n = 3), and ‘Goals and planning’ (n = 2).
BCT coding at individual level
All intervention descriptions contained between one to seven BCTs (Table S2). In total, 14/93 (15%) of the BCTs were coded. The most commonly used BCTs were ‘Information about health consequences’ (16 studies), ‘Credible source’ (15 studies), and ‘Instruction on how to perform a behaviour’ (14 studies). These core BCTs stress the educational emphasis of many of these interventions. Together, they try to educate and persuade through eliciting reflective decisions on the basis of new knowledge from a trusted source that stresses the need for behaviour change. Beyond this backbone of behaviour change content, other BCTs added ‘Prompts and cues’ (n = 6) to trigger behaviour change, ‘Behavioural substitution’ (n = 5) which offers an alternative choice to the behaviour that must be changed, ‘Adding objects to the environment’ (n = 5), and ‘Restructuring the physical environment’ (n = 3) to change the implementation of behaviour. ‘Demonstration of behaviour’ (n = 3) was reported less often again, and other BCTs were reported only once or twice (Table S2). Five of these less frequent BCTs were unique to the most successful interventions: commitment and comparative imagining of future outcomes (Gonzales et al., 2008), monitoring of behaviour without feedback and information on antecedents (Larson et al., 2009) and feedback on behaviour (Larson et al., 2009; Wutzke et al., 2007).
Coherent links between theoretical constructs and BCTs present within the interventions
Drawing upon an iterative conceptual exploration of the plausible, logical connections that could link mechanisms of action within mechanisms of change, the team's previous experience, and ideas from the Behaviour Change Wheel (Michie et al., 2014) we identified evidence of intervention coherence within all of the interventions (Table S2). Perhaps unsurprisingly, most commonly there was coherence between the ‘Knowledge’ TDF domain and the ‘Information about health consequences’ and ‘Instructions on how to perform a behaviour’ BCTs within all 20 studies. The use of a credible, professional source added coherence to most of these interventions. There was also coherence between the ‘Environmental Context and Resources’ TDF domain and the ‘Prompts and cues’, ‘Restructuring the physical environment’, and ‘Adding objects to the environment’ BCTs within 10 studies. Less commonly, there were a few logical links between other mechanisms of action and mechanisms of change. For example, there were logical connections between the ‘Reinforcement’ TDF domain and ‘Feedback on behaviour’ BCT, the ‘Beliefs about consequences’ TDF domain and the ‘Comparative imagining of future outcomes’ BCT and the ‘Skills’ TDF domain was associated with the ‘Demonstration of behaviour’ BCT.
Discussion
The current study analysed the content of 20 studies which aimed to increase public antimicrobial awareness and/or to improve antimicrobial stewardship. We found that only four of these studies reported an explicit theoretical foundation to behaviour change within their intervention. To enhance our understanding of the content and active ingredients of these interventions, we then conducted a theory‐based analysis of the interventions by retrospectively employing the TDF as a coding framework. In addition, we applied the BCT taxonomy to identify the BCTs that were utilized in the studies. Our analysis showed that it is possible to retrospectively analyse the intervention descriptions using this methodology.
While an explicit theoretical framework was only mentioned in few studies, it is apparent from the TDF analysis that the interventions were likely designed with implicit theoretical assumptions in mind, as TDF domains were apparent within all intervention descriptions. In total, nine of the 14 TDF domains were utilized, with preference given for the ‘Knowledge’ and ‘Environmental context and resources’ domains. The information gathered from the tacit theoretical content as assessed by our TDF analysis therefore clearly supplemented the findings of the explicit theory coding provided by the Theory Coding Scheme (Michie & Prestwich, 2010). Previously, Little et al. (2015) have identified the utility of using the TDF for retrospective theory coding when explicit theory is absent. However, this study is the first to apply such an approach within the context of AMR.
The BCT analysis was useful in identifying the ‘active ingredients’ present within the interventions. In total, 14 BCTs (15%) were present across all of the studies, with at least one BCT being utilized within each study. The most common BCTs within the interventions were mainly focussed on educating about the consequences of behaviour and the provision of instructions on performing AMR‐related behaviours using a credible source to implement the messages of the interventions. The fact that a narrow range of BCTs were adopted within these AMR public health interventions provides a clear opportunity for the development of novel interventions in this context in future.
A greater range of TDF domains and BCTs were present within a few of the most successful interventions. These included promoting beliefs about capability and reinforcing behaviour, as well as encouraging a commitment to change behaviour and imagining future outcomes if behaviour is not changed, monitoring behaviour (with and without feedback) and providing information on the antecedents of behaviour. Although uncommon within the AMR interventions, these promising mechanisms may be important in future AMR intervention development.
Given the heterogeneity of the interventions assessed within this analysis, it is hard to make definitive recommendations regarding the value of future intervention content. Our analysis has identified a ‘back bone’ of shared and common intervention ingredients, yet we have also identified the active ingredients unique to effective interventions. We believe that engaging with both these elements represents the best use of the analysis reported here. However, if we want a significant change to the public's engagement with AMR, it could be argued we need a new generation of different interventions.
Using the recommendations within the Behaviour Change Wheel (Michie et al., 2014) and applying logic, we identified evidence of coherence between the TDF mechanisms of action and BCT mechanisms of change within all of the interventions. We identified clear common patterns in what has constituted the ‘active ingredients’ of many previous interventions. These have focussed upon increasing knowledge, changing the local environment, social/professional role and identity and social influence. There were resonances with how these mechanisms of action related to the mechanisms of change associated with natural consequences, comparisons of outcomes, and shaping knowledge. The most common connection was between the BCTs, ‘Information about health consequences’ and ‘Instructions on how to perform a behaviour’ and the TDF domain, ‘Knowledge’. These connections suggest that a key mechanism of action within the AMR public health interventions, to educate through raising public awareness, is operationalized by providing information about the consequences of the appropriate use and misuse of antibiotics while simultaneously providing information about how to take antibiotics appropriately. Within these interventions, there were some indications at times that decisions about AMR stewardship behaviours were underpinned by the ‘Memory, attention and decision‐making processes’ mechanism of action. The use of a credible, professional source to implement the intervention also added coherence within many of these interventions. There were also connections between the ‘Environmental context and resources’ mechanism of action and the ‘Prompts and cues’, ‘Restructuring the physical environment’, and ‘Adding objects to the environment’ mechanisms of change. These BCTs involve altering the physical environment in some way through adding things to the environment to cue a desired behaviour or remove an unwanted behaviour, a key focus of the AMR public health interventions.
Other, less common connections were also established. Most coherently, the ‘Beliefs about consequences’ mechanism of action and the ‘Comparative imagining of future outcomes’ mechanism of change were connected, suggesting a focus on educating about the consequences of behaviour through encouraging the public to reflect on the potential consequences of their own behaviour. There was also a connection between the ‘Skills’ mechanism of action and the ‘Demonstration of behaviour’ mechanism of change. This connection indicates a focus within the interventions on providing information on how to perform appropriate AMR behaviour, through teaching specific skills in the long‐term implementation of the behaviour. Overall, while coherent and making logical sense, at present the interpretation of the links between the TDF mechanisms of action and BCT mechanisms of change are tentative with some arguing that such links should be viewed with caution until a more transparent, systematic method for identifying links is identified (Michie et al., 2016).
The key strength of the current study is that we used an established framework to categorize and describe the theoretical mechanisms of action and mechanisms of change to understand the way in which AMR public health interventions operate. This approach is in line with calls for improved methods for applying theory to intervention design (Michie & Prestwich, 2010), including an increased understanding of how BCTs exert their influence. The findings show that the TDFv2 and BCTTv1 can identify core ingredients of interventions to address AMR knowledge and behaviour. This framework could be applied in future research to the evaluation of other AMR behaviour change interventions, such as those addressing prescribing behaviours. There have, however, been calls for a high level of specificity as behavioural determinants are often specific to particular behaviours, populations, and contexts and so interventions should be individualized, tailored to, and evaluated within specific contexts (Kok et al., 2016). Intervention developers should take this required specificity into account when working with specific populations.
A key limitation of the current analysis is that the ability to code the intervention descriptions was challenging at times due to a lack of detail in the descriptions of the interventions. Thus, it cannot be ruled out that there were omissions in the identification of TDF domains and BCTs due to a lack of detailed intervention reporting. An attempt was made to obtain companion materials to enable a full coding of the interventions; however, there were relatively few responses to our requests despite repeated attempts. The lack of detail in reporting the content of interventions is a widespread problem for the field, leaving readers unable to accurately understand, evaluate, and replicate the intervention reported (Wood et al., 2016). There are guidelines for intervention reporting, for example, TIDieR (Hoffmann et al., 2014) and journal editors should ensure these are followed in an attempt to ensure transferability and replicability of intervention evaluation across populations (Abraham et al., 2014). Another limitation is that most interventions were targeted at directly encouraging the appropriate use of antibiotics within particular target groups, but five studies encouraged the appropriate use of antibiotics in children via interventions directed towards their parents (Cebotarenco & Bush, 2007; Croft et al., 2007; Huang et al., 2007; Stockwell et al., 2010; Trepka, Belongia, Chyou, Davis, & Schwartz, 2001). The types of BCTs coded within these third‐party or ‘relay’ interventions were not dissimilar to those targeted at the individual, but required more careful consideration to consider the behavioural targets of the intervention. Consistent with this, Presseau et al. (2015) argue that future BCT work needs to investigate wider contextual modifiers for a given BCT, such as the extent to which the BCTs address third‐party determinants of behaviour, to help inform the development of future interventions.
Within Figure 2, we present a logic model of how we conceptualize our findings in relation to the context of AMR, the particular problem of the public's engagement with AMR and how both previous and future interventions may engage with AMR. We suggest that to deliver the cultural change required for the public's engagement with AMR, it is imperative to explore the potential effectiveness of new and coherently linked intervention elements. There needs to be a step change in how AMR interventions targeting the public are conceptualized. Addressing BCTs from the goal and planning BCT groupings, for example, or engaging the population in more affective interventions (the TDF domain of Emotions) might be a useful way forward. We believe these present particularly promising directions for future intervention work on the basis of the wider acceptance of goals and planning as important aspects of behaviour change across many domains (National Institute of Clinical Excellence, 2014), and because of our ongoing exploratory research work with the public, which has already identified the importance of the inclusion of emotion focused intervention components within AMR public health interventions elsewhere (Langdridge et al., 2018). Together, these could be a fruitful focus for future intervention work combining the engaging aspects of emotional intervention elements with future planning for what to do when people or their dependents get ill. Therefore, making plans in advance to identify appropriate action in the event of illness may be important in shaping AMR behaviour. In this way, our analysis enables critical reflection on the active content of many previous interventions and draws upon the logic of needing to do things differently if we seek to effect far larger behavioural and cultural change concerning AMR. To provide a different kind of evidence base to structure future interventions to engage the public with AMR and change their AMR‐related behaviour, we believe it is important to systematically investigate the ways in which the public understand, comprehend, and value information concerning AMR and their role in driving the mechanisms of resistance. It is also important to understand how they engage with AMR in the context of other health risks, such as pandemic influenza or sepsis for example.
Figure 2.
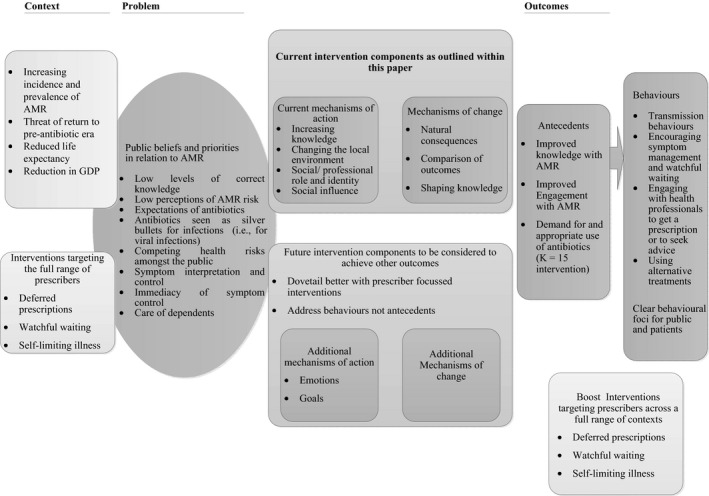
- Note: AMR = antimicrobial resistance; GDP = gross domestic product.
The present study represents the first investigation of its kind to address the active content of AMR public health interventions in relation to behaviour change theory, BCTs, and their connections. We have examined previous reports of interventions and the way that they have harnessed, often tacitly, key intervention components such as mechanisms of action (i.e., theoretical constructs) and mechanism of change (i.e., BCTs). One of the most important steps in fighting AMR is improving the knowledge and understanding of the general public. Although there is some evidence of effectiveness within existing interventions, there is still some way to go to encourage the appropriate use of antibiotics. We would argue there is a growing need for health psychologists to lead in the development, evaluation, and implementation of AMR‐related interventions. The findings of this analysis have provided a framework for future intervention work through making explicit the theory implicit within AMR public health interventions. We have identified a number of theoretical domains and BCTs associated with intervention effectiveness that pave the way for psychological research to improve public health through increasing knowledge, awareness, and engagement with AMR.
Conflict of interest
All authors declare no conflict of interest.
Supporting information
Table S1. Study characteristics.
Table S2. Behavioural domains, Theoretical Domains Framework constructs, behaviour change technique groupings and individual BCTs identified from intervention descriptions.
Acknowledgements
This project was funded by Health Protection Scotland (HPS) (R2456). The opinions expressed in this publication are those of the authors and are not necessarily those of HPS.
References
- Abraham, C. , Johnson, B. T. , de Bruin, M. , & Luszczynska, A. (2014). Enhancing reporting of behavior change intervention evaluations. Journal of Acquired Immune Deficiency Syndromes, 66, S293–S299. 10.1097/qai.0000000000000231 [DOI] [PubMed] [Google Scholar]
- Abraham, C. , & Michie, S. (2008). A taxonomy of behavior change techniques used in interventions. Health Psychology, 27, 379–387. 10.1037/0278-6133.27.3.379 [DOI] [PubMed] [Google Scholar]
- Atkins, L. , Francis, J. , Islam, R. , O'Connor, D. , Patey, A. , Ivers, N. , … Michie, S. (2017). A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implementation Science, 12(1), 77 10.1186/s13012-017-0605-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Azevedo, M. M. , Pinheiro, C. , Yaphe, J. , & Baltazar, F. (2013). Assessing the impact of a school intervention to promote students’ knowledge and practices on correct antibiotic use. International Journal of Environmental Research and Public Health, 10, 2920–2931. 10.3390/ijerph10072920 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cane, J. , O'Connor, D. , & Michie, S. (2012). Validation of the theoretical domains framework for use in behaviour change and implementation research. Implementation Science, 7(1), 37 10.1186/1748-5908-7-37 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cebotarenco, N. , & Bush, P. J. (2008). Reducing antibiotics for colds and flu: A student‐taught program. Health Education Research, 23(1), 146–157. 10.1093/her/cym008 [DOI] [PubMed] [Google Scholar]
- Charani, E. , Castro‐Sanchez, E. , & Holmes, A. (2014). The role of behavior change in antimicrobial stewardship. Infectious Disease Clinics of North America, 28, 169–175. 10.1016/j.idc.2014.01.004 [DOI] [PubMed] [Google Scholar]
- Craig, P. , Dieppe, P. , Macintyre, S. , Michie, S. , Nazareth, I. , Petticrew, M. , & Medical Research Council Guidance . (2008). Developing and evaluating complex interventions: The new Medical Research Council guidance. British Medical Journal, 337, a1655 10.1136/bmj.a1655 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Croft, D. R. , Knobloch, M. J. , Chyou, P. H. , Ellen, D. V. , Janette, C. , Davis, J. P. , … Belongia, E. A. (2007). Impact of a child care educational intervention on parent knowledge about appropriate antibiotic use. Wisconsin Medical Journal, 106, 78–84. [PubMed] [Google Scholar]
- Curry, M. , Sung, L. , Arroll, B. , Goodyear‐Smith, F. , Kerse, N. , & Norris, P. (2006). Public views and use of antibiotics for the common cold before and after an education campaign in New Zealand. New Zealand Medical Journal, 119, U1957. [PubMed] [Google Scholar]
- Davis, R. , Campbell, R. , Hildon, Z. , Hobbs, L. , & Michie, S. (2015). Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychology Review, 9, 323–344. 10.1080/17437199.2014.941722 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elouafkaoui, P. , Young, L. , Newlands, R. , Duncan, E. M. , Elders, A. , & Clarkson, J. E. , … Translation Research in a Dental Setting Research Methodology Group (2016). An audit and feedback intervention for reducing antibiotic prescribing in general dental practice: The RAPiD cluster randomised controlled trial. PLoS Medicine, 13(8), e1002115 10.1371/journal.pmed.1002115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farrell, D. , Kostkova, P. , Weinberg, J. , Lazareck, L. , Weerasinghe, D. , Lecky, D. M. , & McNulty, C. A. (2011). Computer games to teach hygiene: An evaluation of the e‐Bug junior game. Journal of Antimicrobial Chemotherapy, 66(Suppl 5), v39–v44. 10.1093/jac/dkr122 [DOI] [PubMed] [Google Scholar]
- Flowers, P. (2018). Antimicrobial resistance: A biopsychosocial problem requiring innovative interdisciplinary and imaginative interventions. Journal of Infection Prevention. 10.1177/1757177418755308 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Formoso, G. , Paltrinieri, B. , Marata, A. M. , Gagliotti, C. , Pan, A. , Moro, M. L. , … Magrini, N. (2013). Feasibility and effectiveness of a low cost campaign on antibiotic prescribing in Italy: Community level, controlled, non‐randomised trial. British Medical Journal, 347, f5391 10.1136/bmj.f5391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glanz, K. , & Bishop, D. B. (2010). The role of behavioral science theory in development and implementation of public health interventions. Annual Review of Public Health, 31, 399–418. 10.1146/annurev.publhealth.012809.103604 [DOI] [PubMed] [Google Scholar]
- Gonzales, R. , Corbett, K. K. , Wong, S. , Glazner, J. E. , Deas, A. , Leeman‐Castillo, B. , … Kafadar, K. (2008). “Get smart Colorado”: Impact of a mass media campaign to improve community antibiotic use. Medical Care, 46, 597–605. 10.1097/MLR.0b013e3181653d2e [DOI] [PubMed] [Google Scholar]
- Gualano, M. R. , Gili, R. , Scaioli, G. , Bert, F. , & Siliquini, R. (2015). General population's knowledge and attitudes about antibiotics: A systematic review and meta‐analysis. Pharmacoepidemiology and Drug Safety, 24(1), 2–10. 10.1002/pds.3716 [DOI] [PubMed] [Google Scholar]
- Haynes, C. , & McLeod, C. (2015). A review of reviews of educational interventions designed to change the public's knowledge and behaviour in relation to antimicrobial use and antimicrobial resistance that target healthcare professionals and patients. London, UK: Retrieved from https://www.nice.org.uk/guidance/ng63/documents/antimicrobial-resistance-changing-riskrelated-behaviours-in-the-general-population-evidence-review-32 [Google Scholar]
- Hoffmann, T. C. , Glasziou, P. P. , Boutron, I. , Milne, R. , Perera, R. , Moher, D. , … Michie, S. (2014). Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. British Medical Journal, 348, g1687 10.1136/bmj.g1687 [DOI] [PubMed] [Google Scholar]
- Hopkins, S. (2016). UK initiatives to reduce antimicrobial resistant infections, 2013–2018. International Journal of Health Governance, 21(3), 131–138. 10.1108/IJHG-02-2016-0013 [DOI] [Google Scholar]
- Huang, S. S. , Rifas‐Shiman, S. L. , Kleinman, K. , Kotch, J. , Schiff, N. , Stille, C. J. , … Finkelstein, J. A. (2007). Parental knowledge about antibiotic use: Results of a cluster‐randomized, multicommunity intervention. Pediatrics, 119, 698–706. 10.1542/peds.2006-2600 [DOI] [PubMed] [Google Scholar]
- King, S. , Exley, J. , Taylor, J. , Kruithof, K. , Larkin, J. , & Pardal, M. (2016). Antimicrobial stewardship: The effectiveness of educational interventions to change risk‐related behaviours in the general population: A systematic review. Rand Health Quarterly, 5(3), 2. [PMC free article] [PubMed] [Google Scholar]
- Kok, G. , Gottlieb, N. H. , Peters, G.‐J. Y. , Mullen, P. D. , Parcel, G. S. , Ruiter, R. A. C. , … Bartholomew, L. K. (2016). A taxonomy of behaviour change methods: An Intervention Mapping approach. Health Psychology Review, 10, 297–312. 10.1080/17437199.2015.1077155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Langdridge, D. , Davis, M. , Gozdzielewska, L. , McParland, J. , Williams, L. , Young, M. , … Flowers, P . (2018). A visual affective analysis of interventions to increase antimicrobial stewardship amongst the public. Under review. [DOI] [PMC free article] [PubMed]
- Larson, E. L. , Ferng, Y. H. , McLoughlin, J. W. , Wang, S. , & Morse, S. S. (2009). Effect of intensive education on knowledge, attitudes, and practices regarding upper respiratory infections among urban Latinos. Nursing Research, 58, 150–157. 10.1097/NNR.0b013e3181a30951 [DOI] [PubMed] [Google Scholar]
- Lecky, D. M. , McNulty, C. A. , Touboul, P. , Herotova, T. K. , Benes, J. , Dellamonica, P. , … Group, e.‐B. W. (2010). Evaluation of e‐Bug, an educational pack, teaching about prudent antibiotic use and hygiene, in the Czech Republic, France and England. Journal of Antimicrobial Chemotherapy, 65, 2674–2684. 10.1093/jac/dkq356 [DOI] [PubMed] [Google Scholar]
- Levy, S. B. , & Marshall, B. (2004). Antibacterial resistance worldwide: Causes, challenges and responses. Nature Medicine, 10(12 Suppl), S122–S129. 10.1038/nm1145 [DOI] [PubMed] [Google Scholar]
- Little, E. A. , Presseau, J. , & Eccles, M. P. (2015). Understanding effects in reviews of implementation interventions using the Theoretical Domains Framework. Implementation Science, 10, 90 10.1186/s13012-015-0280-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madle, G. , Kostkova, P. , Mani‐Saada, J. , Weinberg, J. , & Williams, P. (2004). Changing public attitudes to antibiotic prescribing: Can the internet help? Informatics in Primary Care, 12(1), 19–26. [DOI] [PubMed] [Google Scholar]
- Maindal, H. T. , Kirkevold, M. , Sandbaek, A. , & Lauritzen, T. (2010). Lifting the lid of the “black intervention box” – The systematic development of an action competence programme for people with screen‐detected dysglycaemia. BMC Health Services Research, 10, 114 10.1186/1472-6963-10-114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mainous, A. G. , Diaz, V. A. , & Carnemolla, M. (2009). A community intervention to decrease antibiotics used for self‐medication among Latino adults. Annals of Family Medicine, 7, 520–526. 10.1370/afm.1061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mazinska, B. , & Hryniewicz, W. (2010). European Antibiotic Awareness Day educational campaign–has it changed public attitudes to antibiotic use in Poland? Pol Merkur Lekarski, 29(173), 296–303. [PubMed] [Google Scholar]
- McCullough, A. R. , Parekh, S. , Rathbone, J. , Del Mar, C. B. , & Hoffmann, T. C. (2016). A systematic review of the public's knowledge and beliefs about antibiotic resistance. Journal of Antimicrobial Chemotherapy, 71(1), 27–33. 10.1093/jac/dkv310 [DOI] [PubMed] [Google Scholar]
- McNulty, C. A. M. , Bowen, J. , Gelb, D. , & Charlett, A. (2007). “The Bug Investigators”: Assessment of a school teaching resource to improve hygiene and prudent use of antibiotics. Health Education, 107(1), 10–26. 10.1108/09654280710716851 [DOI] [Google Scholar]
- McNulty, C. A. M. , Nichols, T. , Boyle, P. J. , Woodhead, M. , & Davey, P. (2010). The English antibiotic awareness campaigns: Did they change the public's knowledge of and attitudes to antibiotic use? Journal of Antimicrobial Chemotherapy, 65, 1526–1533. 10.1093/jac/dkq126 [DOI] [PubMed] [Google Scholar]
- McNulty, C. A. M. , Swan, A. V. , & Boland, D. (2001). Schools’ antimicrobial resistance: National Advice to the Public campaign – A pilot study. Health Education, 101, 235–242. 10.1108/EUM0000000005646 [DOI] [Google Scholar]
- Michael, C. A. , Dominey‐Howes, D. , & Labbate, M. (2014). The antimicrobial resistance crisis: Causes, consequences, and management. Frontiers in Public Health, 2, 145 10.3389/fpubh.2014.00145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michie, S. , Atkins, L. , & West, R. (2014). The behaviour change wheel: A guide to designing interventions (1st ed.). London, UK: Silverback. [Google Scholar]
- Michie, S. , Carey, R. N. , Johnston, M. , Rothman, A. J. , de Bruin, M. , Kelly, M. P. , & Connell, L. E. (2016). From theory‐inspired to theory‐based interventions: A protocol for developing and testing a methodology for linking behaviour change techniques to theoretical mechanisms of action. Annals of Behavioral Medicine. 10.1007/s12160-016-9816-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michie, S. , Johnston, M. , Abraham, C. , Lawton, R. , Parker, D. , & Walker, A. (2005). Making psychological theory useful for implementing evidence based practice: A consensus approach. Quality and Safety in Health Care, 14(1), 26–33. 10.1136/qshc.2004.011155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michie, S. , & Prestwich, A. (2010). Are interventions theory‐based? Development of a theory coding scheme. Health Psychology, 29(1), 1–8. 10.1037/a0016939 [DOI] [PubMed] [Google Scholar]
- Michie, S. , Richardson, M. , Johnston, M. , Abraham, C. , Francis, J. , Hardeman, W. , … Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95. 10.1007/s12160-013-9486-6 [DOI] [PubMed] [Google Scholar]
- Moore, G. F. , Audrey, S. , Barker, M. , Bond, L. , Bonell, C. , Hardeman, W. , … Baird, J. (2015). Process evaluation of complex interventions: Medical Research Council guidance. British Medical Journal, 350, h1258 10.1136/bmj.h1258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute of Clinical Excellence . (2014). Behaviour change: Individual approaches (Public Health Guideline [PH49]). Retrieved from https://www.nice.org.uk/guidance/ph49
- Noar, S. M. , Benac, C. N. , & Harris, M. S. (2007). Does tailoring matter? Meta‐analytic review of tailored print health behavior change interventions. Psychology Bulletin, 133, 673–693. 10.1037/0033-2909.133.4.673 [DOI] [PubMed] [Google Scholar]
- O'Neill, J. (2016). Tackling drug‐resistant infections globally: Final report and recommendations. Retrieved from https://amr-review.org/sites/default/files/160525_Final%20paper_with%20cover.pdf
- Pinder, R. , Sallis, A. , Berry, D. , & Chadborn, T. (2015). Behaviour change and antibiotic prescribing in healthcare settings. Literature review and behavioural analysis. (2014719). London, UK: Public Health England; Retrieved from https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/405031/Behaviour_Change_for_Antibiotic_Prescribing_-_FINAL.pdf [Google Scholar]
- Pontes, M. C. , & Pontes, N. M. (2005). Debiasing effects of education about appropriate antibiotic use on consumers’ preferences for physicians. Health Care Management Review, 30(1), 9–16. 10.1097/00004010-200501000-00003 [DOI] [PubMed] [Google Scholar]
- Presseau, J. , Ivers, N. M. , Newham, J. J. , Knittle, K. , Danko, K. J. , & Grimshaw, J. M. (2015). Using a behaviour change techniques taxonomy to identify active ingredients within trials of implementation interventions for diabetes care. Implementation Science, 10(1), 55 10.1186/s13012-015-0248-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Price, L. , Gozdzielewska, L. , Young, M. , Smith, F. , MacDonald, J. , McParland, J. , … Flowers, P. H. (2018). Effectiveness of interventions to improve the public's antimicrobial resistance awareness and behaviours associated with prudent use of antimicrobials: A systematic review. Journal of Antimicrobial Chemotherapy, 73(6), 1464–1478. 10.1093/jac/dky076 [DOI] [PubMed] [Google Scholar]
- Rawson, T. M. , Moore, L. S. P. , Tivey, A. M. , Tsao, A. , Gilchrist, M. , Charani, E. , & Holmes, A. H. (2017). Behaviour change interventions to influence antimicrobial prescribing: A cross‐sectional analysis of reports from UK state‐of‐the‐art scientific conferences. Antimicrobial Resistance and Infection Control, 6, 11 10.1186/s13756-017-0170-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stockwell, M. S. , Catallozzi, M. , Meyer, D. , Rodriguez, C. , Martinez, E. , & Larson, E. (2010). Improving care of upper respiratory infections among Latino Early Head Start parents. Journal of Immigrant and Minority Health, 12, 925–931. 10.1007/s10903-010-9326-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Review on Antimicrobial Resistance . (2014). Antimicrobial resistance: Tackling a crisis for the health and wealth of nations. London, UK: Retrieved from https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf [Google Scholar]
- Trepka, M. J. , Belongia, E. A. , Chyou, P. , Davis, J. P. , & Schwartz, B. (2001). The effect of a community intervention trial on parental knowledge and awareness of antibiotic resistance and appropriate antibiotic use in children. Pediatrics, 107(1), e6 10.1542/peds.107.1.e6 [DOI] [PubMed] [Google Scholar]
- Treweek, S. , Francis, J. J. , Bonetti, D. , Barnett, K. , Eccles, M. P. , Hudson, J. , … MacLennan, G. (2016). A primary care Web‐based Intervention Modeling Experiment replicated behavior changes seen in earlier paper‐based experiment. Journal of Clinical Epidemiology, 80, 116–122. 10.1016/j.jclinepi.2016.07.008 [DOI] [PubMed] [Google Scholar]
- Weinstein, R. A. (2001). Controlling antimicrobial resistance in hospitals: Infection control and use of antibiotics. Emerging Infectious Diseases, 7, 188–192. 10.3201/eid0702.010206 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wood, C. E. , Hardeman, W. , Johnston, M. , Francis, J. , Abraham, C. , & Michie, S. (2016). Reporting behaviour change interventions: Do the behaviour change technique taxonomy v1, and training in its use, improve the quality of intervention descriptions? Implementation Science, 11(1), 84 10.1186/s13012-016-0448-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wutzke, S. E. , Artist, M. A. , Kehoe, L. A. , Fletcher, M. , Mackson, J. M. , & Weekes, L. M. (2007). Evaluation of a national programme to reduce inappropriate use of antibiotics for upper respiratory tract infections: Effects on consumer awareness, beliefs, attitudes and behaviour in Australia. Health Promotion International, 22(1), 53–64. 10.1093/heapro/dal034 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Study characteristics.
Table S2. Behavioural domains, Theoretical Domains Framework constructs, behaviour change technique groupings and individual BCTs identified from intervention descriptions.