

Abstract
Objective
Untreated compulsive sexual behavior (CSB) poses a risk to efficacious substance use disorder (SUD) treatment. Yet, the ways in which CSB manifests in women with SUDs remains poorly understood. Shame and trauma exposure are well-documented correlates for women’s CSB. Prior theory suggested women with shame and trauma-related symptoms may engage in CSB in an effort to escape aversive internal experiences. Thus, the present study examined experiential avoidance as a mediator of the relationship between defectiveness/shame beliefs, post-traumatic stress disorder (PTSD) symptoms, and CSB in a sample of women with SUDs.
Method
Cross-sectional, self-report data were collected from 446 women (M age = 37.40) in residential treatment for SUDs.
Results
Experiential avoidance partially mediated the relationship between both PTSD symptoms and defectiveness/shame beliefs and CSB.
Conclusions
These results extend theoretical conceptualizations of women’s CSB to a treatment population. CSB intervention efforts may benefit from targeting women’s avoidance of painful experiences.
Keywords: compulsive sexual behavior, substance use, experiential avoidance, sex addiction, shame, PTSD symptoms
Compulsive sexual behavior (CSB) is defined as compulsive, excessive, or otherwise problematic sexual behavior, desire, or drive that results in significant distress or impairment (e.g., excessive masturbation, pornography use, or sexual activity; Kafka, 2010). Such behaviors are over-represented among women with substance use disorders (SUD), with as many as 19.6% endorsing clinical levels of CSB (Deneke, Knepper, Green, & Carnes, 2015). If left untreated, comorbid CSB may increase the risk of relapse following SUD treatment (Schneider & Irons, 2001). Despite this risk, research offered little insight into the risk and protective factors for CSB among women with SUD, thereby hindering treatment efforts (Carnes, 2001; Schnieder & Irons, 2001). Shame and trauma are well-established risk factors for women’s CSB; however, these risk factors, and the mechanisms underlying their association with CSB, remain unexplored among women with SUD (Dhuffar & Griffiths, 2014; McKeague, 2014). In an effort to better understand CSB within this population, the present study examined the relations between defectiveness- and shame-related beliefs (i.e., defectiveness/shame), PTSD symptoms, and CSB among women in residential SUD treatment. We also examined a model in which experiential avoidance mediated the relations between defectiveness/shame, PTSD symptoms, and CSB.
Experiences of Women with CSB
A majority of studies investigating women’s CSB focused on the increased likelihood of CSB among women with trauma histories (e.g., sexual, emotional, and physical abuse, and neglect; Opitz, Tsytsarev, & Froh, 2009; Vaillancourt-Morel et al., 2015). Childhood sexual abuse is the most frequently investigated trauma among women with CSB, with 76.2% of women with CSB endorsing a history of childhood sexual abuse (Schwartz & Southern, 2000). Given the high comorbidity between women’s trauma exposure and CSB, it is not surprising that women who endorse PTSD symptoms are more likely to engage in CSB (Schwartz & Southern, 2000). Researchers speculated that CSB may develop as a maladaptive coping response to aversive internal experiences associated with trauma (e.g., PTSD symptoms; Ferree, 2001). Specifically, Ferree (2001) offers the theoretical explanation that CSB may facilitate a temporary sense of relational control that allows some women to escape the pain and powerlessness experienced as part of trauma and abuse (Ferree, 2001). Thus, it seems plausible that CSB may function among women with PTSD symptoms to alter or alleviate painful cognitive and affective experiences. However, empirical studies have yet to explore this supposition.
In addition to trauma, shame (i.e., a negative self-evaluation in which an individual regards herself as bad and defective; Tagney & Dearing, 2002), is a well-documented correlate of CSB (Dhuffar & Griffiths, 2014; McKeague, 2014). Dhuffar and Griffiths (2014) suggested that shame is a catalyst for CSB, particularly among women. Specifically, researchers theorized that, in response to shame, some women engaged in short-term “feel good” behaviors (e.g., CSB) in order to deflect shame and maintain a homeostatic level of comfort (Derbyshire & Grant, 2015; Gilliland, South, Carpenter, & Hardy, 2011). CSB therefore may be maintained, in part, by both positive reinforcement (i.e., the pleasure associated with sexual activity) and negative reinforcement (i.e., shame-related cognitions diminish, even if only temporarily) following CSB and may impede the use of more adaptive emotion regulation and cognitive strategies (Gilliland et al., 2011). It remains unclear how shame is elicited in such a way that CSB develops. Although it is plausible that shame may occur as a result of trauma (Wilson, Drozdek, and Turkovic, 2006), shame may also increase the risk for CSB among women without trauma histories. Research supported a cyclical relationship between CSB and shame when CSB is used as a long-term avoidance strategy (Reid, Harper, & Anderson, 2009). That is, CSB subsequently exacerbates shame due, in part, to the negative consequences unique to women’s CSB (e.g., sexually transmitted infections, infertility, unwanted pregnancies, legal consequences of prostitution, and social disproval of women’s sexual activity; Dhuffar & Griffiths, 2014). Additional research is needed to determine whether avoidance maintains CSB in the context of shame.
Experiential Avoidance
Experiential avoidance is conceptualized as a propensity to avoid, escape, or change one’s experience of aversive internal events (e.g., thoughts, feelings, memories, and sensations; Hayes, Wilson, Gifford, Follette, & Strosahl, 1996). Experiential avoidance is a primary target of many treatments (e.g., Acceptance and Commitment Therapy and Dialectical Behavioral Therapy) seeking to ameliorate the maladaptive coping strategies elicited by experiential avoidance (e.g., compulsive activity, binge eating, aggression, and substance use; Chapman, 2006). Individuals with high experiential avoidance tend to compulsively engage in problematic behaviors known to induce short-term feelings of comfort (e.g., sexual activity) in an effort to circumvent painful internal experiences (Hayes, Luoma, Bond, Masuda, & Lillis, 2006). Due to the short-term benefit of such maladaptive coping responses, individuals are negatively reinforced to continue engaging in maladaptive behaviors at the expense of processing difficult experiences (Hayes et al., 2006). Numerous studies indicated that individuals with SUD have particularly high levels of experiential avoidance (Chawla & Ostafin, 2007; Stewart, Zvolensky, & Eifert, 2002). For instance, individuals with SUD may experience an urge to use illicit substances, subsequently use illicit substances to escape this aversive state, and experience relief paired with substance-induced pleasure or euphoria. This may explain, in part, why such individuals are more likely to engage in other maladaptive behaviors (e.g., CSB).
Similarly, Carnes (2001) suggested that some individuals are motivated to engage in CSB as a short-term coping strategy in an effort to regulate or avoid negative internal experiences. Although researchers examined the relations between experiential avoidance and CSB among men (Brem, Shorey, Anderson, & Stuart, 2017; Levin, Lillis, & Hayes, 2012; Wetterneck, Burgess, Short, Smith, & Cervantes, 2012), there has yet to be an empirical investigation of the relations between CSB and experiential avoidance among women. Theoretical accounts of the role of experiential avoidance in relation to women’s CSB suggested that CSB may help women distract from, and alleviate, painful cognitive and affective experiences most commonly associated with shame and trauma (Ferree, 2001; Gilliland et al., 2011; McKeague, 2014). Notably, there are a number of treatments that target experiential avoidance (e.g., Mindfulness-Based Cognitive Therapy and Acceptance and Commitment Therapy), which demonstrated efficacy in treating populations with SUDs (Chiesa & Serretti, 2014; Luoma, Kholenberg, Hayes, & Fletcher, 2012; Witkiewitz & Bowen, 2010), suggesting such treatments may be easily applied to populations affected by CSB. Efforts to inform CSB treatment for women with SUD would benefit from an initial empirical investigation of the role of experiential avoidance in CSB.
Summary & Hypotheses
In sum, there is an overrepresentation of defectiveness/shame, CSB, PTSD symptoms, and experiential avoidance among populations afflicted by substance misuse (Chawla & Ostafin, 2007; Dearing, Stuewig, & Tangney, 2005; Deneke et al., 2015; Jacobsen, Southwick, & Costen, 2001). Informed by theories of learning, researchers proposed that women may engage in sexual activity in order to temporarily deflect aversive experiences associated with defectiveness/shame and trauma (Ferree, 2001; Gilliland et al., 2011). For some women, the overreliance on sexual activity as a mechanism of avoidance may facilitate CSB. It follows that defectiveness/shame and trauma symptoms may relate to women’s CSB because some women engage in CSB to avoid negative internal experiences (i.e., experiential avoidance; Dhuffar & Griffiths, 2014; Ferree, 2001; Gilliland et al., 2011; McKeague, 2014). However, this theoretical perspective has yet to be tested empirically. In an effort to inform intervention efforts for this understudied population, the present study investigated experiential avoidance as a mediator of the relations between defectiveness/shame, PTSD symptoms, and CSB among women in residential treatment for SUD. Specifically, we hypothesized that:
Experiential avoidance would mediate the relation between women’s defectiveness/shame and CSB, controlling for the influence of PTSD symptoms, alcohol use and problems, and drug use and problems.
Experiential avoidance would mediate the relation between women’s PTSD symptoms and CSB, controlling for the influence of defectiveness/shame, alcohol use and problems, and drug use and problems.
Method
Participants
Medical records for 446 women in residential treatment for SUDs were included in the present study. The primary diagnoses for this sample, based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM 5; American Psychiatric Association [APA], 2013), were alcohol use disorder (31.25%), opioid use disorder (21.87 %), sedative, hypnotic, or anxiolytic use disorder (19.19%), cocaine use disorder (7.59%), amphetamine-type substance use disorder (5.80%), cannabis use disorder (4.91%), and inhalant use disorder (0.45%). An additional 8.92% of the sample was diagnosed with more than one SUD. The racial/ethnic composition of the sample was as follows: White (96.02%), Black/African American (2.87%), other (0.66%), Hispanic/Latina/o (0.22%), and Native American/American Indian (0.22%). Patients’ mean age was 37.40 (SD = 12.72) years. The majority of the sample reported that they were married (40.61%), followed by never married (35.59%), divorced (14.41%), separated (2.18%), engaged (2.18%), widowed (1.75%), none selected (1.53%), remarried (1.31%), and other (0.44%).
Procedures
We reviewed patients’ medical records from a private, residential substance misuse treatment facility located in the Southeastern United States. Admission dates on records reviewed ranged from September 2013 to September 2016. Admission into the program requires participants to be at least 18 years old and have a primary SUD diagnosis. Patients were referred to the treatment facility through a variety of sources, including employers, courts, physicians, as well as self-referral. Patients completed several self-report measures following admission to the program and after medical detoxification (if necessary). Patients provided consent to have their de-identified medical records used for research purposes. Patient medical records included total scores of each measure only; thus internal consistency estimates could not be calculated. Treatment thereafter typically lasts 28-30 days and is largely based on the 12-step model of recovery. Diagnoses were based on the DSM 5 (APA, 2013) and were determined through consultation of the treatment team, which included a licensed psychologist, psychiatrist, general physician, and substance abuse counselor. All procedures were approved by the Institutional Review Board of the first author.
Measures
Experiential Avoidance
The Acceptance and Action Questionnaire-II (AAQ-II; Bond et al., 2011) is a 10-item self-report measure that assesses experiential avoidance. Responses to items (e.g., “I worry about being unable to control my worries and feelings”) are provided on a scale ranging from 1 (never true) to 7 (always true). The AAQ-II was scored such that higher scores suggest higher experiential avoidance. The AAQ-II demonstrated good psychometric properties across various populations, including treatment-seeking adults (Gratz, Bornovalova, Delany-Brumsey, Nick, & Lejuez, 2007).
Defectiveness/Shame
The Young Schema Questionnaire – Long Form, Third Edition’s (YSQ-L3; Young & Brown, 2003) Defectiveness/Shame subscale assessed self-reported defectiveness/shame beliefs, defined as beliefs that one is inherently flawed, defective, and unlovable. The 15 items (e.g., “If others found out about my basic defects I could not face them”) that comprise the defectiveness/shame subscale are answered on a six-point Likert scale ranging from 1 (completely untrue of me) to 6 (describes me perfectly). Items rated by the individual as a 4, 5, or 6 are considered particularly relevant for that individual and are summed such that higher scores are indicative of more defectiveness/shame beliefs about oneself. Items rated by the individual as a 1, 2, or 3 are recoded into “0.” The YSQ’s defectiveness/shame scale associated with a number of psychiatric symptoms, including depression, anxiety, PTSD, and social phobia (Cockram, Drummond & Lee, 2010; Hawke & Provencher, 2011; Pinto-Gouveia, Castilho, Galhardo & Cunha, 2006; Schmidt, Joiner, Young, & Telch, 1995). The YSQ demonstrated good psychometric properties across various populations (Oei & Baranoff, 2007) and has been used with individuals in residential treatment for SUDs (Shorey, Elmquist, Anderson, & Stuart, 2015).
PTSD Symptoms
The Psychiatric Diagnostic Screening Questionnaire (PDSQ; Zimmerman, 2002; Zimmerman & Mattia, 2001) PTSD subscale was used to assess current PTSD symptoms. The PTSD subscale consists of 15 Yes/No items designed to screen for the presence of criterion A1 (i.e., that the individual experienced or witnessed a traumatic event within their lifetime), criterion B (i.e., the re-experience of trauma through distressing thoughts, dreams, or feelings), and criterion C (i.e., avoidance of stimuli associated with the trauma and numbing of responsiveness) of PTSD from Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition – Text Revision (DSM-IV-TR; American Psychiatric Association [APA], 2000). Scores on the PTSD subscale may range from 0 to 15 with higher scores corresponding to greater PTSD symptoms. The PDSQ demonstrated good psychometric properties within a population of individuals with substance use disorders (Zimmerman, Sheeran, Chelminski, & Young, 2004).
Compulsive Sexual Behavior
The 20-item Sexual Addiction Screening Test-Revised (SAST-R; Carnes, Green, & Carnes, 2010) Core scale assessed core components of CSB experienced in the participant’s lifetime, including preoccupation (i.e., obsessive thinking about sexual behavior, opportunities, and fantasies), loss of control (i.e., inability to stop behavior despite commitments to self and others and despite problems caused by the behavior), affective disturbance (i.e., significant depression, despair, or anxiety over sexual behavior), and relationship disturbance (i.e., sexual behavior has created significant relationship problems). The 20 items of the Core scale (e.g., “Have you made efforts to quit a type of sexual activity and failed?”) are presented in a forced-choice (Yes/No) format with possible scores ranging from 0-20. Higher scores indicate greater risk for CSB. Individuals with Core scale scores greater than or equal to six are considered “at-risk” for clinical levels of CSB (Carnes et al., 2010). The SAST-R demonstrated adequate psychometric properties in clinical and non-clinical samples of women, and across sexual orientations (Carnes et al., 2010).
Alcohol Use and Problems
The Alcohol Use Disorders Identification Test (AUDIT; Saunders, Asaland, Babor, de la Fuente, & Grant, 1993) assessed patient’s self-reported alcohol use and problems in the year prior to treatment admission. Ten items examined the intensity and frequency of alcohol use, symptoms of alcohol tolerance and dependence, and negative consequences of alcohol use. Scores are summed such that higher scores are indicative of greater levels of alcohol use and problems. The AUDIT demonstrated excellent reliability and validity across multiple populations (Babor, Higgins-Biddle, Saunders, & Monteiro, 2001).
Drug Use and Problems
The Drug Use Disorders Identification Test (DUDIT; Stuart, Moore, Ramsey, & Kahler, 2003; Stuart, Moore, Kahler, & Ramsey, 2003) assessed patients’ drug use (i.e., cannabis, cocaine, hallucinogens, stimulants, sedatives/hypnotics/anxiolytics, opiates, and other substances [e.g., inhalants]) and problems in the year prior to treatment admission. Like the AUDIT, the DUDIT’s 14 items examined the intensity and frequency of drug use, symptoms of drug tolerance and dependence, and negative consequences of drug use. The DUDIT evidenced good psychometric properties (Stuart et al., 2003a, 2003b).
Data Analytic Strategy
Descriptive and correlational analyses were conducted using SPSS Version 23.0. Given that our data violated assumptions of normality (i.e., CSB and defectiveness/shame scores evidenced positive skewness), we first conducted a Spearman correlation. Path analysis in Mplus Version 6.12 was conducted to test study hypotheses. Full information maximum likelihood estimation (FIML) was used to handle missing data. FIML was shown to provide more efficient and less biased estimates than alternative strategies such as pairwise or listwise deletion (Enders, 2010; Kline, 2010). Maximum likelihood estimation was also used to account for study variables being non-normally distributed (i.e., CSB and defectiveness/shame scores) as this estimate is robust to issues of non-normality (Kline, 2010). Path analysis allows for simultaneous analysis of a series of structural regression equations. The path model illustrated in Figure 1 was created by regressing CSB on experiential avoidance and both defectiveness/shame and PTSD symptoms simultaneously while controlling for the relationship between defectiveness/shame and PTSD symptoms. Alcohol use and problems, and drug use and problems, were statistically controlled for in all paths by including them as additional predictor variables in the path model. A fully saturated (i.e., zero degrees of freedom) model consisting of 27 parameters was used to test for indirect effects of defectiveness/shame and PTSD symptoms on CSB through experiential avoidance. Model fit indices were neither examined nor reported in the current study because fully saturated models always produce a perfect fit to the data (Kline, 2010).
Figure 1.
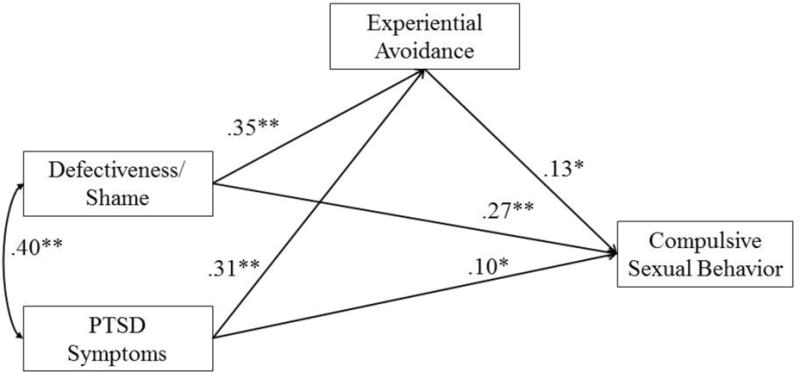
Pathways from women’s defectiveness/shame and PTSD symptoms on compulsive sexual behavior through experiential avoidance. Alcohol use and problems, and drug use and problems, were controlled for in all paths, but were not displayed in the figure due to space constraints. * p <.05, ** p <.001.
The bias-corrected bootstrap method procedure was used to test whether defectiveness/shame and PTSD symptoms were indirectly associated with CSB through experiential avoidance. Bootstrapping resampling allows for a more accurate estimate of indirect effects without relying on the assumption of a normal distribution (Shrout & Bolger, 2002). Bias-corrected confidence intervals provide more accurate weight between Type I and Type II errors and a more precise assessment of indirect effects than traditional tests of mediation (e.g., Sobel test; MacKinnon, Lockwood, & Williams, 2004; Sobel, 1982). Therefore, 5000 bootstrap samples and 95% bias-corrected confidence intervals were used to examine the significance of indirect effects. An indirect effect is statistically significant if the value of zero is not included in the bias-corrected confidence interval. We also calculated the percentage of the total association between each predictor (i.e., PTSD symptoms and defectiveness/shame beliefs) and CSB that was explained by each indirect path by dividing the estimated indirect effect (%IE) for each predictor variable by the total effect for each relationship (i.e., PTSD symptoms and CSB, and defectiveness/shame beliefs and CSB; MacKinnon & Dwyer, 1993).
Results
Descriptive Statistics
Means, standard deviations, and bivariate correlations among variables are shown in Table 1. As expected, experiential avoidance positively related to defectiveness/shame, PTSD symptoms, CSB, and drug use and problems. Both defectiveness/shame and PTSD symptoms positively related to CSB and drug use and problems. Defectiveness/shame and PTSD symptoms were positively related. CSB was positively related to alcohol use and problems, and drug use and problems. Alcohol use and problems was not significantly related to experiential avoidance, defectiveness/shame, or PTSD symptoms.
Table 1.
Means, standard deviations, and Spearman correlations among study variables
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Defectiveness/Shame | – | .43** | .50** | .43** | .04 | .27** |
| 2. PTSD Symptoms | – | .48** | .39** | .08 | .21** | |
| 3. AAQ-II | – | .35** | .01 | .36** | ||
| 4. Compulsive Sexual Behavior | – | .17** | .20** | |||
| 5. Alcohol Use and Problems | – | −.48** | ||||
| 6. Drug Use and Problems | – | |||||
| Mean | 16.72 | 5.64 | 41.42 | 2.10 | 14.78 | 17.18 |
| SD | 23.44 | 5.10 | 12.71 | 3.10 | 12.93 | 15.13 |
Note. PTSD = Posttraumatic stress disorder; AAQ-II = Acceptance and Action Questionnaire-II.
p < .01,
p < .05.
Path Analyses
Results of path analyses are displayed in Figure 1 and Table 2. Results revealed significant paths from both defectiveness/shame and PTSD symptoms to experiential avoidance. The path from experiential avoidance to CSB was also statistically significant. The paths from defectiveness/shame and PTSD symptoms to CSB remained statistically significant in the presence of paths to and from experiential avoidance.
Table 2.
Standardized path coefficients for paths from shame and PTSD symptoms to experiential avoidance and compulsive sexual behavior
| Mediator
|
Outcome
|
|
|---|---|---|
| AAQ-II | Compulsive Sexual Behavior | |
| AAQ-II → | - | .13 (.02)* |
| Defectiveness/Shame → | .35 (.03)** | .27 (.01)** |
| PTSD symptoms → | .31 (.13)** | .10 (.03)* |
| Alcohol use and problems → | .10 (.05) | .18 (.01)** |
| Drug use and problems → | .25 (.04)** | .13 (.01)* |
Note. Standard errors are in parentheses. PTSD = posttraumatic stress disorder; AAQ-II = Acceptance and Action Questionnaire-II.
p <.05,
p <.001
Tests of Mediation
Test for indirect effects using bootstrapping were consistent and revealed significant indirect effects of both defectiveness/shame and PTSD symptoms on CSB through experiential avoidance. Results supported a model by which experiential avoidance partially mediated the relation between CSB and both defectiveness/shame, B = .05, 95% CI [.008, .083], %IE = 12.9, and PTSD symptoms, B = .04, 95% CI [.003, .077], %IE = 11.2.
Discussion
The present study is the first to examine experiential avoidance as a mechanism underlying the relations between defectiveness/shame, PTSD symptoms, and CSB among women in residential treatment for SUD. Results of this investigation provided preliminary support for the hypothesis that women with a SUD engage in CSB due, in part, to an effort to change, escape, or avoid the painful experiences associated with defectiveness/shame and PTSD symptoms.
Findings from the present study extended research previously limited to men (e.g., Wetterneck et al., 2012) to suggest that, for women with SUD, aversive experiences associated with defectiveness/shame and PTSD symptoms are related to CSB, partially through experiential avoidance. These results were consistent with theoretical literature suggesting that CSB is motivated and maintained by efforts to circumvent aversive internal experiences (Carnes, 2001; Dhuffar & Griffiths, 2014; Schwartz & Southern, 2000). For some women, sexual activity may provide a short-term sense of relief from defectiveness/shame and PTSD symptoms; it is plausible that it is through this negative reinforcement cycle that CSB emerges (Reid et al., 2009). Findings were consistent with previous research indicating that individuals with SUD pursue maladaptive emotion regulation strategies that ameliorate painful experiences more readily than do individuals without SUD as a result of having higher levels of avoidance (Chawla & Ostafin, 2007). It follows, then, that women with SUD would be more likely to engage in CSB in an effort to avoid defectiveness/shame and PTSD symptoms.
Our results supported a model by which experiential avoidance only partially mediated the relations between defectiveness/shame, PTSD symptoms, and CSB. Therefore, additional constructs may contribute to the relations among the study variables. Perera, Reece, Monaham, Billingham, and Finn (2009) suggested that low perceived self-worth may explain why women with PTSD symptoms engage in CSB. It is plausible that some traumas (e.g., childhood sexual abuse) facilitate shame-related beliefs (e.g., “I am unlovable,” “others will be unable to meet my needs,” and “I am defective”) which, according to Carnes (2001), encourages such individuals to maintain physical and emotional distance from others, thereby creating a context for some forms of CSB (e.g., excessive masturbation and pornography use). As such, social isolation may be an additional variable which could account for the associations between defectiveness/shame, PTSD symptoms, and CSB. Further research would clarify this supposition.
What remains unclear is why CSB specifically, as opposed to other behaviors (e.g., eating, exercise, self-harm, gambling), might develop alongside trauma and/or defectiveness/shame for a subset of women. Additional research employing qualitative methods may offer some insight into this trajectory. Dhuffar and Griffiths (2014) proposed that factors such as religiosity, culture, relationship difficulties, and age may explain the availability of sexual activity as a viable method of providing temporary relief from painful experiences. For example, there may be generational differences in the consequences associated with women’s sexual activity that contributed to the extent to which women engaged in sexual activity as a means of coping (Dhuffar & Griffiths, 2014). Similarly, technological advances have increased the availability of internet-based sexual opportunities (e.g., sexual chat rooms, pornography, and the use of social media to meet casual sexual partners). These and other variables (e.g., sexual orientation) should be investigated using both longitudinal and qualitative research methods in order to better understand the developmental trajectory of CSB in relation to defectiveness/shame and trauma.
Limitations
A number of limitations should be considered while interpreting the results of the present study. First, our sample was comprised of primarily White women with one or more SUD whose sexual orientation could not be ascertained, which limits the generalizability of our findings. Future studies should aim to replicate and extend these findings using more diverse samples. Second, our data were cross-sectional which precludes efforts to draw conclusions regarding the causality of study variables. We cannot determine whether or not defectiveness/shame, or PTSD symptoms, were present during, prior to, or following CSB. Relatedly, the way in which our chart review was conducted restricted our ability to thoroughly examine the constructs of interest. For instance, we were limited to the measures used by the treatment facility and did not have access to symptom-specific information (e.g., specific PTSD symptom clusters). Choosing our own methods for assessing defectiveness/shame, PTSD symptoms, and CSB may have provided additional information relevant to the research question. Similarly, assessing study variables within a sample with more homogenous trauma experiences (e.g., sexual trauma, military trauma) would elucidate the role of PTSD symptoms in CSB. Additional research employing longitudinal or event-level research (e.g., daily diary data) is needed to further support the directionality of study variables, and the potential influence of defectiveness/shame, PTSD symptoms, and experiential avoidance on women’s CSB. Third, we could not ascertain whether the defectiveness/shame women reported was associated with a history of trauma, their substance use, their sexual activities, or some other event. Similarly, we did not assess the type of trauma to which women were exposed. Research exploring CSB among women would benefit from further clarification of their trauma and shame-related cognitions, including an assessment of both cognitive and affective experiences of defectiveness/shame. Fourth, we did not employ clinical interviews to determine the presence of SUD or PTSD; future research would be improved from the use of structured, clinical interviews to better assess the presence of these and other disorders in relation to CSB. Finally, because only total scores were available for each measure, reliability statistics could not be performed.
Research Implications
In addition to addressing the limitations of the present study, future research should continue to investigate the etiology and unique manifestations of CSB in women, especially those with histories of trauma who endorse shame-related cognitions. It is plausible that exposure to trauma early in life contributes to women’s shame, thereby increasing the likelihood that maladaptive coping responses (e.g., substance use and CSB) may occur. Indeed, Wilson et al. (2006) suggest that shame may be a prolonged consequence of one or more traumatic stressors (i.e., posttraumatic shame) which negatively impacts affect regulation capabilities (e.g., experiential avoidance, cognitive flexibility). These researchers further posited that posttraumatic shame may originate from one’s thoughts about oneself or perceptions of how others perceive him or her, and may yield a variety of affective states (e.g., anger, rage, anxiety, humiliation, and loss) that trigger maladaptive behaviors (e.g., substance use and excessive sexual activity). Future research may benefit from elucidating how shame from various origins (e.g., from self or from others’ evaluations) interacts with various affective states to facilitate CSB among women with a SUD.
Moreover, the present study provided preliminary support for experiential avoidance as an underlying mechanism in the relations between defectiveness/shame, PTSD symptoms, and CSB. However, future research is needed to determine the extent to which other aversive affective states (e.g., depression and anxiety) relate to women’s CSB through experiential avoidance. Indeed, research suggests that men’s CSB may be motivated, in part, by an effort to escape painful affect such as depression and anxiety (Brem et al., 2017; Wetterneck et al., 2012). Furthermore, while experiential avoidance may explain how women’s CSB is maintained, less is known regarding whether, and to what extent, experiential avoidance contributes to the development of women’s CSB. Future research employing qualitative or longitudinal research methods may further clarify the role of experiential avoidance in the development and maintenance of women’s CSB.
Clinical Implications
The results of the present study highlighted the importance of assessing the presence of shame-related cognitions and PTSD among women with SUD who evidence CSB. Clinicians should assess women’s willingness or ability to approach painful experiences, and determine the extent to which CSB is used by women to escape or alter these painful states. Secondly, our findings suggested that it may be beneficial for clinicians to help women become better able to approach and process defectiveness/shame and trauma-relates symptoms, as opposed to avoiding them, in an effort to minimize their use of CSB in response to these experiences. Notably, it remains unknown whether reductions in experiential avoidance will correspond with reductions in CSB among women. Although empirically-informed treatments (e.g., Mindfulness-Based Cognitive Therapy and Acceptance and Commitment Therapy) that target experiential avoidance demonstrated efficacy in reducing substance use and other maladaptive coping behaviors (Chiesa & Serretti, 2014; Luoma, et al., 2012; Witkiewitz & Bowen, 2010), researchers have yet to examine whether these interventions reduce CSB among women with a SUD. Because such interventions are employed in many SUD treatment settings, they may be easily adapted to treat CSB among women with a SUD. Furthermore, given the transdiagnostic nature of Acceptance and Commitment Therapy, this treatment approach may be especially useful for targeting experiential avoidance underlying SUD as well as comorbid conditions (e.g., CSB; Twohig & Crosby, 2010). Researchers should determine whether such interventions that aim to reduce experiential avoidance and substance use will yield reductions in CSB among women with a SUD.
Conclusion
The present study extended previous research by examining relations between defectiveness/shame, PTSD symptoms, experiential avoidance, and CSB among a population of women in residential treatment for substance use. Our preliminary results suggested that targeting experiential avoidance among women with comorbid SUD and CSB may be beneficial. Additional research is needed to better understand contextual antecedents to women’s CSB.
Acknowledgments
This work was supported, in part, by grant K24AA019707 from the National Institute on Alcohol Abuse and Alcoholism (NIAAA) awarded to the last author. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIAAA or the National Institutes of Health.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th. Washington, DC: Author; 2000. text rev. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th. Arlington, VA: American Psychiatric Publishing; 2013. [Google Scholar]
- Babor TF, Higgins-Biddle JC, Saunders JB, Monteiro MG. The Alcohol Use Disorders Identification Test: Guideline for use in primary care. 2nd. Geneva: World Health Organization; 2001. [Google Scholar]
- Bond FW, Hayes SC, Baer RA, Carpenter KM, Guenole N, Orcutt HK, Waltz T, Zettle RD. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: A revised measure of psychological inflexibility and experiential avoidance. Behavior Therapy. 2011;42:676–688. doi: 10.1016/j.beth.2011.03.007. [DOI] [PubMed] [Google Scholar]
- Brem MJ, Shorey RC, Anderson S, Stuart GL. Depression, anxiety, and compulsive sexual behavior among men in residential treatment for substance use disorders: The role of experiential avoidance. Journal of Clinical Psychology and Psychotherapy. 2017;24:1246–1253. doi: 10.1002/cpp.2085. [DOI] [PubMed] [Google Scholar]
- Carnes P. Out of the shadows: Understanding sexual addiction. Center City, MN: Hazelden Publishing; 2001. [Google Scholar]
- Carnes P, Green B, Carnes S. The same yet different: Refocusing the Sexual Addiction Screening Test (SAST) to reflect orientation and gender, sexual addiction and compulsivity. The Journal of Treatment and Prevention. 2010;17(1):7–30. [Google Scholar]
- Chapman AL. Acceptance and mindfulness in behavior therapy: A comparison of dialectical behavior therapy and acceptance and commitment therapy. Internaltional Journal of Behavioral and Consultation Therapy. 2006;2(3):308–313. [Google Scholar]
- Chawla N, Ostafin B. Experiential avoidance as a functional dimensional approach to psychopathology: An empirical review. Journal of Clinical Psychology. 2007;63(9):871–890. doi: 10.1002/jclp.20400. [DOI] [PubMed] [Google Scholar]
- Chiesa A, Serretti A. Are mindfulness-based interventions effective for substance use disorders? A systematic review of the evidence. Substance Use and Misuse. 2014;49(5):492–512. doi: 10.3109/10826084.2013.770027. [DOI] [PubMed] [Google Scholar]
- Cockram DM, Drummond PD, Lee CW. Role and treatment of early maladaptive schemas in Vietnam veterans with PTSD. Clinical Psychology & Psychotherapy. 2010;17(3):165–182. doi: 10.1002/cpp.690. [DOI] [PubMed] [Google Scholar]
- Dearing RL, Stuewig J, Tandney JP. On the importance of distinguishing shame from guilt: Relations to problematic alcohol and drug use. Addictive Behaviors. 2005;30:1392–1404. doi: 10.1016/j.addbeh.2005.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deneke E, Knepper C, Green BA, Carnes PJ. Comparative study of three levels of care in a substance use disorder inpatient facility on risk for sexual addiction. Sexual Addiction and Compulsivity. 2015;22(2):109–125. [Google Scholar]
- Derbyshire KL, Grant JE. Compulsive sexual behavior: A review of the literature. Journal of Behavioral Addictions. 2015;4(2):37–43. doi: 10.1556/2006.4.2015.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dhuffar MK, Griffiths MD. Understanding the role of shame and its consequences in female hypersexual behaviours: A pilot study. Journal of Behavioural Addictions. 2014;3(4):231–237. doi: 10.1556/JBA.3.2014.4.4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders CK. Applied missing data analysis. New York: Guilford Press; 2010. [Google Scholar]
- Ferree MC. Females and sex addiction: Myths and diagnostic implications. Sexual Addiction & Compulsivity. 2001;8:287–300. [Google Scholar]
- Gilliland R, South M, Carpenter BN, Hardy SA. The roles of shame and guilt in hypersexual behavior. Sexual Addiction and Compulsivity: The Journal of Treatment & Prevention. 2011;18(1):12–29. doi: 10.1080/10720162.2011.551182. [DOI] [Google Scholar]
- Gratz KL, Bornovalova MA, Delany-Brumsey A, Nick B, Lejuez CW. A laboratory-based study of the relationship between childhood abuse and experiential avoidance among inner-city substance users: The role of emotional nonacceptance. Behavior Therapy. 2007;38(3):256–268. doi: 10.1016/j.beth.2006.08.006. [DOI] [PubMed] [Google Scholar]
- Hawke LD, Provencher MD. Schema theory and schema therapy in mood and anxiety disorders: A review. Journal of Cognitive Psychotherapy. 2011;25(4):257–276. doi: 10.1891/0889-8391.27.4.359. [DOI] [PubMed] [Google Scholar]
- Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and Commitment Therapy: Model, processes and outcomes. Behavior Research and Therapy. 2006;44:1–25. doi: 10.1016/j.brat.2005.06.006. [DOI] [PubMed] [Google Scholar]
- Hayes SC, Wilson KG, Gifford EV, Follette VM, Strosahl K. Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology. 1996;64:1152–1168. doi: 10.1037//0022-006x.64.6.1152. [DOI] [PubMed] [Google Scholar]
- Jacobsen LK, Southwick SM, Costen TR. Substance use disorders in patients with posttraumatic stress disorder: A review of the literature. The American Journal of Psychiatry. 2001;158(8):1184–1190. doi: 10.1176/appi.ajp.158.8.1184. [DOI] [PubMed] [Google Scholar]
- Kafka MP. Hypersexual disorder: A proposed diagnosis for DSM-V. Archives of Sexual Behavior. 2010;39:377–400. doi: 10.1007/s10508-009-9574-7. [DOI] [PubMed] [Google Scholar]
- Kline RB. Principles and practice of structural equation modeling. 3rd. New York: Guilford Press; 2010. [Google Scholar]
- Levin ME, Lillis J, Hayes SC. When is online pornography viewing problematic among college males? Examining the moderating role of experiential avoidance. Sexual Addiction and Compulsivity. 2012;19:168–180. [Google Scholar]
- Luoma JB, Kholenberg BS, Hayes SC, Fletcher L. Slow and steady wins the race: A randomized clinical trial of Acceptance and Commitment Therapy targeting shame and substance use disorders. Journal of Consulting and Clinical Psychology. 2012;80(1):43–53. doi: 10.1037/a0026070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research. 2004;39:99–128. doi: 10.1207/s15327906mbr3901_4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKeague EL. Differentiating the female sex addict: A literature review focused on themes of gender difference used to inform recommendations for treating women with sex addiction. Sexual Addiction and Compulsivity. 2014;21:203–224. [Google Scholar]
- Oei TPS, Baranoff J. Young schema questionnaire: review of psychometric and measurement issues. Australian Journal of Psychology. 2007;59:78–86. [Google Scholar]
- Opitz DM, Tsytsarev SV, Froh J. Women’s sexual addiction and family dynamics, depression and substance abuse. Sexual Addiction & Compulsivity. 2009;16:324–340. [Google Scholar]
- Perera B, Reece M, Monahan P, Billingham R, Finn P. Childhood characteristics and personal dispositions to sexually compulsive behavior among young adults. Sexual Addiction & Compulsivity. 2009;16:131–145. [Google Scholar]
- Pinto-Gouveia J, Castilho P, Galhardo A, Cunha M. Early maladaptive schemas and social phobia. Cognitive Therapy and Research. 2006;30(5):571–584. [Google Scholar]
- Reid RC, Harper JM, Anderson EH. Coping strategies used by hypersexual patients to defend against the painful effects of shame. Clinical Psychology & Psychotherapy. 2009;16:125–138. doi: 10.1002/cpp.609. [DOI] [PubMed] [Google Scholar]
- Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption–II. Addiction. 1993;88:791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x. [DOI] [PubMed] [Google Scholar]
- Schmidt NB, Joiner TE, Jr, Young JE, Telch MJ. The schema questionnaire: Investigation of psychometric properties and the hierarchical structure of a measure of maladaptive schemas. Cognitive Therapy and Research. 1995;19(3):295–321. [Google Scholar]
- Schneider JP, Irons RR. Assessment and treatment of addictive sexual disorders: Relevance for chemical dependency relapse. Substance Use & Misuse. 2001;36(13):1795–1820. doi: 10.1081/JA-100108428. [DOI] [PubMed] [Google Scholar]
- Schwartz M, Southern S. Compulsive cybersex: The new tea room. Sexual Addiction & Compulsivity. 2000;7:127–144. [Google Scholar]
- Shorey RC, Elmquist J, Anderson S, Stuart GL. The relationship between early maladaptive schemas, depression, and generalized anxiety among adults seeking residential treatment for substance use disorders. Journal of Psychoactive Drugs. 2015;47(3):230–238. doi: 10.1080/02791072.2015.1050133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: New procedures and recommendations. Psychological Methods. 2002;7:422–445. [PubMed] [Google Scholar]
- Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. In: Leinhardt S, editor. Sociological Methodology. Washington, DC: American Sociological Association; 1982. pp. 290–312. [Google Scholar]
- Stewart SH, Zvolensky MJ, Eifert GH. The relations of anxiety sensitivity, experiential avoidance, and alexithymic coping to young adults’ motivations for drinking. Behavior Modification. 2002;26(2):274–296. doi: 10.1177/0145445502026002007. [DOI] [PubMed] [Google Scholar]
- Stuart GL, Moore TM, Kahler CW, Ramsey SE. Substance abuse and relationship violence among men court-referred to batterers’ intervention programs. Substance Abuse. 2003a;24(2):107–122. doi: 10.1080/08897070309511539. [DOI] [PubMed] [Google Scholar]
- Stuart GL, Moore TM, Ramsey SE, Kahler CW. Relationship aggression and substance use among women court-referred to domestic violence intervention programs. Addictive Behaviors. 2003b;28(9):1603–1610. doi: 10.1016/j.addbeh.2003.08.038. [DOI] [PubMed] [Google Scholar]
- Tangney JP, Dearing RL. Shame and guilt. NY: Guilford Press; 2002. [Google Scholar]
- Twohig MP, Crosby JM. Acceptance and commitment therapy as a treatment for problematic internet pornography viewing. Behavior Therapy. 2010;41(3):285–295. doi: 10.1016/j.beth.2009.06.002. [DOI] [PubMed] [Google Scholar]
- Vaillancourt-Morel MP, Godbout N, Labadie C, Runtz M, Lussier Y, Sabourin S. Avoidant and compulsive sexual behaviors in male and female survivors of childhood sexual abuse. Child Abuse and Neglect. 2015;40:48–49. doi: 10.1016/j.chiabu.2014.10.024. [DOI] [PubMed] [Google Scholar]
- Wetterneck CT, Burgess AJ, Short MB, Smith AH, Cervantes ME. The role of sexual compulsivity, impulsivity, and experiential avoidance in internet pornography use. The Psychological Record. 2012;62:3–18. [Google Scholar]
- Wilson JP, Drozdek B, Turkovic S. Posttraumatic shame and guilt. Trauma, Violence, & Abuse. 2006;7(2):122–141. doi: 10.1177/1524838005285914. [DOI] [PubMed] [Google Scholar]
- Witkiewitz K, Bowen S. Depression, craving, and substance use following a randomized trial of mindfulness-based relapse prevention. Journal of Consulting and Clinical Psychology. 2010;78(3):362–374. doi: 10.1037/a0019172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Young JE, Brown G. Young schema questionnaire. NY: Cognitive Therapy Center of New York; 2003. [Google Scholar]
- Zimmerman M. The Psychiatric Diagnostic Screening Questionnaire manual. Los Angeles: Western Psychological Services; 2002. [Google Scholar]
- Zimmerman M, Mattia JI. The Psychiatric Disgnostic Screening Questionnaire: Development, reliability, and validity. Comprehensive Psychiatry. 2001;42:175–189. doi: 10.1053/comp.2001.23126. [DOI] [PubMed] [Google Scholar]
- Zimmerman M, Sheeran T, Chelminski I, Young D. Screening for psychiatric disorders in outpatients with DSM-IV substance use disorders. Journal of Substance Abuse and Treatment. 2004;26:181–188. doi: 10.1016/S0740-5472(03)00207-1. [DOI] [PubMed] [Google Scholar]