

Abstract
This study presents results from a randomized controlled trial of the Protecting Strong African American Families (ProSAAF) program, a family-centered intervention designed to promote strong couple, coparenting, and parent-child relationships in two-parent African American families. A total of 346 African American couples with an early adolescent child participated; all families lived in rural, low-income communities in the southern United States. Intent-to-treat growth curve analyses involving 3 waves and spanning 17 months indicated that ProSAAF participants, compared with control participants, reported greater improvements in relationship communication, confidence, satisfaction, partner support, coparenting, and parenting. More than 80% of the couples attended all six of the in-home, facilitator-led sessions; costs to implement the program averaged $1739 per family. The findings inform the ongoing debate surrounding prevention programs for low-income and ethnic minority couples.
Keywords: African American, costs, growth curve analysis, low-income couples, relationship education, prevention
In this article, we present the conceptual basis and an empirical test of a new family-centered preventive intervention designed for two-parent African American families living in the rural southeastern United States (US). Many of these families are exposed to chronic financial hardship, racial discrimination, and community disadvantage that can undermine couples’ relationship quality (Randall & Bodenmann, 2009). Relationship discord, in turn, can negatively affect multiple dimensions of adults’ lives, including parenting practices, physical and mental health, and work performance (Erel & Burman, 1995; Robles, Slatcher, Trombello, & McGinn, 2014; Whisman & Uebelakcer, 2006). To date, however, few prevention programs have been developed for two-parent African American families. Most programs for this population focus exclusively on the parent-child relationship, parenting practices, and youth development (e.g., Brody et al., 2004) (for exception, see Beach et al., 2014). In addition, recent federally-funded efforts designed to strengthen relationship quality among low-income and ethnic minority couples have been found to be, on average, ineffective in retaining couples and improving relationship quality (see Lavner, Karney, & Bradbury, 2015).
Protecting Strong African American Families (ProSAAF) was developed in response to these multifaceted concerns. The program was designed to meet the needs of two-parent African American families residing in the rural South by providing a preventive intervention that would engage families and promote well-being among couples and families. In this article, we summarize the conceptualization of the program and present results from a randomized controlled trial with rural African American couples. Building on previous studies supporting ProSAAF’s short-term impact (Barton et al., 2017; Beach et al., 2016), the current study uses three waves of data spanning 17 months to investigate the program’s impact on rates of change in couple, coparenting, and parenting interactions, as well as the mechanisms through which these effects occur.
Prevention Programs for Low-Income, Ethnic Minority Couples
Strengthening and stabilizing relationships among low-income and ethnic minority couples is a focal issue to both policymakers and researchers (Cowan & Cowan, 2014). Attention to this topic arises from the divergence in marital entry and stability along racial and socioeconomic lines, and the subsequent effects of this instability on children, families, and the broader society (Amato, 2010, 2012; Lerman, 2013; Trail & Karney, 2012). Various efforts have been undertaken recently to strengthen couple relationships in low-income, ethnic minority families. These efforts have ranged from large-scale randomized controlled trials involving thousands of couples throughout the country (Lundquist et al., 2014; Wood, Moore, Clarkwest, & Killewald, 2014) to small-scale experiments and quasi-experimental projects at single sites (Beach et al., 2014; Owen, Quirk, Bergen, Inch, & France, 2012). The results of these efforts have been mixed. For instance, in evaluations of large-scale federal initiatives, no effects emerged for participants’ outcomes (see Lavner et al., 2015), whereas secondary analyses have uncovered improvements among subsets of participating couples (Amato, 2014; Rhoades, 2015; Williamson, Altman, Hsueh, & Bradbury, 2016). Even supporters of couple-focused prevention programs for low-income populations have noted a lack of convincing evidence to support their widespread implementation (Cowan & Cowan, 2014). These mixed findings have led to criticism of existing preventive interventions for low-income couples, challenging their theoretical foundations, delivery strategies, and continued funding (Johnson, 2012; Johnson & Bradbury, 2015). These diverging results and opinions suggest the need for a new generation of preventive interventions for low-income, ethnically diverse families.
The Protecting Strong African American Families Program
Development of ProSAAF was based on social learning theory and cognitive-behavioral therapy (CBT) approaches to prevention of couple and family problems (e.g., Stanley, Blumberg, & Markman, 1999). As such, program content was designed to provide skills training, behavioral rehearsal and feedback, and reinforcement involving the ways in which couples interact together and think about their relationships. Despite its widespread use, the suitability of CBT-based approaches for promoting healthy couple relationships has been challenged in recent years, particularly for low-income couples (Johnson & Bradbury, 2015; Trail & Karney, 2012). A common theme in this critique is the minimal attention that CBT-based approaches devote to contextual stressors and the potential for environmental factors to shape couples’ relationship functioning. As several empirically-based models of stress and relationship functioning propose (Conger & Elder, 1994; Neff, 2012; Randall & Bodenmann, 2009), stressful environmental circumstances hinder couples’ use of adaptive relationship cognitions and behaviors and foster more negative interpersonal exchanges between partners (e.g., conflict, withdraw) and intrapersonal cognitions about the relationship (e.g., dissatisfaction, maladaptive cognitions). Accordingly, scholars have recommended that preventive interventions for low-income and ethnic minority couples address more explicitly the stressors these couples encounter, either through reducing levels of stress itself or by promoting couples’ resilience (e.g., adaptive coping strategies, managing stress-elicited negative emotions and reactions) when encountering stressors (Beach et al., 2014; Trail & Karney, 2012).
On the basis of this literature, the ProSAAF program was developed for African American couples in the rural South rearing preadolescent and adolescent youths. The six-session program was designed to enhance functioning in multiple family subsystems, with program content devoted to couple functioning, coparenting, youth development, and parent-child relationship quality. The primary unit of focus in the prevention program was the adult romantic-partner dyad, and the intervention itself focused primarily on promoting couple- and adult-level outcomes, including couple relationship functioning, coparenting, and parenting processes. Secondary targets of the program were youth outcomes, which were expected to show effects mediated through the program’s impact on the adult romantic-partner dyads.
ProSAAF content was informed by research on individual and couple processes that have been shown to protect and enhance relationships in African American couples and families (e.g., Cutrona, Russell, Burzette, Wesner, & Bryant, 2011; Marks et al., 2008), the conceptual models of stress and family functioning mentioned previously, and components from previous prevention programs for African American couples and parents (Beach et al., 2014; Brody et al., 2004). We examined these sources to identify malleable, proximal processes in the immediate couple and family context that enhance relationship quality, coparenting, and parenting processes for African American couples living in economically distressed areas. The program was hypothesized to sponsor primarily improvement in couple relationship outcomes in the short- to moderate-term, which in turn, were expected to produce secondary, longer-term benefits for children’s and adult’s psychological and physical well-being. The current study was designed to determine whether ProSAAF was successful in accomplishing its primary aim, improving couples’ relationship quality.
A distinguishing feature of the program is its explicit attention to contextual stressors that rural African American couples experience. Each session focuses on a specific stressor (e.g., work, racism, finances, extended family), and couples are instructed in cognitive and behavioral techniques for handling the stressor together. Thus, program content is not described as focusing on improving couples’ communication per se, but rather on helping couples to deal with the stressors they encounter and to use specific communication strategies to this end. Conversely, the program is also not designed to reduce external sources of stress themselves, but to use tenets from social learning theory to help affected couples respond in mutually supportive and effective ways. ProSAAF is designed to help couples and families to develop a “team” orientation in managing stressors, to increase awareness of the effects of stress, and to attribute certain relationship challenges and negative emotions to external stressors rather than relationship deficits. In this way, the program is designed to prevent declines in relationship quality and mitigate the cognitive and behavioral spillover of stress into the romantic-partner dyad.
Content in each session focused on the enhancement of couple, coparenting, and parenting processes. Specific couple issues included recognizing positive aspects of the partnership, identifying “beneath the surface” issues, strengthening couple identity and unity, and enhancing quality time together. Specific parenting/coparenting issues included parent-child communication, family rules, child misbehavior, and children’s ethnic pride. Consistent with the programs that informed ProSAAF’s development, all program material was evaluated by African American focus groups, and pilot studies were conducted with African Americans prior to the efficacy trial. Feedback from these activities led to curriculum revisions related to timing, instruction clarity, phrasing of discussion questions, and handling of content focused on couple intimacy. Supplemental Table S1 summarizes the components of the ProSAAF program.
Another of ProSAAF’s distinctions is its facilitator-led, in-home delivery approach. Previous studies have shown that African Americans, particularly men, are less likely to attend couple-focused prevention programs than are people of other ethnicities (Hurt et al., 2012; Stanley, Johnson, Amato, & Markman, 2006). Strategies that have been used to promote attendance among minority and low-SES groups are numerous, including cultural adaptation of program content (Kumpfer, Alvarado, Smith, & Bellamy, 2002) and the provision of various incentives to remove barriers to participation (e.g., monetary rewards, free food and childcare, and transportation; see Gross, Julion, & Fogg, 2001). More recently, in-home prevention program for couples have emerged using mainly self-directed approaches, in which participants guide themselves through program content using DVD or Internet-based videos (Bodenmann, Hilpert, Nussbeck, & Bradbury, 2014; Doss et al., 2016). Given these literatures, as well as feedback from focus groups on ways to promote engagement, ProSAAF was designed as a home-based, facilitator-led prevention program.
ProSAAF comprises six weekly sessions, each lasting 2 hours, plus two booster sessions. Sessions were organized around DVD presentations that taught program content and depicted scenarios of program-targeted interactions and behaviors. In each of the sessions, the facilitator guided couples through the video instruction and modeling, structured activities, and discussions of specific topics. The first 60 minutes of each session focused on the couple’s relationship, and the next 30 minutes focused on parenting/coparenting topics. The facilitator then met with the target youth for a 15-minute individual activity dealing with topics such as peer pressure or understanding parents, while the couple took a break in a different room. After the youth activity, the entire family met with the facilitator for a 15-minute joint activity, such as a discussion or a game. This session structure was modeled after the Strengthening Families Program (Kumpfer, Molgaard, & Spoth, 1996).
Previous analyses using data from Wave 1 (W1) and Wave 2 (W2) indicated that, approximately 9 months after baseline, ProSAAF couples’ communication, satisfaction, and confidence were greater than those of couples in the control condition (Barton et al., 2017). In addition, among an initial subset of 139 families (50% intervention), ProSAAF families reported better parenting and youth outcomes than did those in the control condition (Beach et al., 2016). The current study builds on these findings by examining: (a) program effects on rates of change in couple, coparenting, and parenting processes over a 17-month period, and (b) mechanisms of program effects through path models using three waves of data that control for baseline levels. On the basis of prior theory and empirical findings (Barton et al., 2017), couple communication patterns were selected as the mechanism of program effects. Participant attendance and program costs are also summarized briefly, given their relevance to policy and dissemination.
Method
Participants and Procedures
Couples with an African American youth between the ages of 9 and 14 years (age: M = 10.87, SD = .90) took part in the study. All participants lived in small towns and communities in the southern US in which poverty rates are among the highest in the nation and unemployment rates are above the national average (DeNavas-Walt & Proctor, 2014). To be eligible, couples had to be in a relationship for 2 years or more, living together, and coparenting an African American youth in the targeted age range for at least 1 year. Couples had to be willing to spend 6 weeks engaged in a family-centered prevention program and not be planning to move out of the study area during that period. Participant recruitment, randomization, and progress through the study are illustrated in the CONSORT flowchart in Supplemental Figure S1.
Families were recruited by mail and phone via advertisements distributed in their communities as well as through lists that local schools provided. Schools in 16 counties provided information on youths in grades 4 through 6. Only directory information, not student’s educational records, was requested, permitting its release from schools without prior parental notification under the Family Educational Rights and Privacy Act. A total of 1897 families were screened for eligibility. Of these families, 1145 were ineligible because the household was headed by a single parent, the child was not in the targeted age range, the child was not African American, or the family was enrolled in another program. Of the 752 eligible families, 347 did not respond to the solicitation and 59 were unable to schedule an assessment. The remaining 346 families were randomized to the intervention (n = 172) or control (n = 174) condition. Two same-sex couples were excluded from analyses because data analytic techniques required dyads to be distinguishable by sex, and this subsample size precluded group comparisons.
Of the couples in the randomized sample, 63% were married, with a mean length of marriage of 9.8 years (SD = 7.48; range < 1 year to 56 years). Unmarried couples had been living together for an average of 6.7 years (SD = 5.42; range < 1 year to 24 years). Adults’ mean ages were 39.9 years (SD = 9.6; range 21 to 83 years) for men and 36.6 years (SD= 7.45; range 23 to 73 years) for women. The majority of families in the study could be classified as working poor; 51% had incomes below 100% of the federal poverty level and an additional 17% had incomes between 100% and 150% of that level. The majority of both men (74% [65% full-time]) and women (61% [45% full-time]) were employed. Median monthly income was $1,375 (SD = $1,375; range $1 to $7,500) for men and $1,220 (SD = $1440; range $1 to $10,000) for women. Median education levels were high school or GED (ranging from less than grade 9 to a doctorate or professional degree) for men and some college or trade school (ranging from less than grade 9 to a master’s degree) for women. The total number of children residing in the home ranged from 1 to 8, with median of 3 and mode of 2 (M = 2.97; SD = 1.48).
Project staff visited couples’ homes, explained the study in greater detail, and obtained informed consent from adult participants. Each participating family member then completed the W1 assessment using audio computer-assisted self-interview software installed on laptop computers; participants completed surveys on a separate laptops and, if possible, in separate rooms. Participants did not talk to one another or see one another’s responses while completing the survey. Families were visited for W2 and Wave 3 (W3) assessments a mean of 9.4 months and 17.0 months after W1. Each adult was compensated with a $50 check for completing each wave. Randomization took place after couples completed pretest measures. Block randomization by marital status was performed within each county to facilitate group equivalence.
ProSAAF implementation
A trained African American facilitator visited the couple at their home for six consecutive weeks to conduct a 2-hour intervention session. A total of 28 facilitators implemented the program; the total number of families with whom each facilitator worked ranged from 1 to 15. Two booster sessions were scheduled to reinforce material covered during the main intervention. If a couple separated or divorced, an alternative booster session was offered that focused on the coparenting relationship and protecting children from the stress of separation and divorce. The two booster sessions were scheduled approximately 3 and 9 months after program completion (approximately 2 months before W2 and 4 months before W3).
Control group
Couples in the control group were assessed on the same schedule as those in the intervention group, thereby controlling for effects of repeated measurements, maturation, individual differences, and external social changes. After the pretest, couples were mailed the book 12 Hours to a Great Marriage (Markman, Stanley, Blumberg, Jenkins, & Whaley, 2004) and an accompanying workbook that presented reasons for enhancing the couple’s relationship, guidelines, examples of communication and problem-solving strategies, and exercises designed to enrich relationships. Use of the book was not assessed at W2 or W3.
Measures
Effective communication
Participant reports of effective communication were measured using a seven-item version of the Communication Skills Test (Jenkins & Saiz, 1995). The items, rated on a scale ranging from 1 (almost never) to 7 (almost always), were used to assess the frequency of effective communication patterns between partners. Sample items included, “When discussing an issue, my mate and I both take responsibility to keep us on track” and “When [partner name] and I discuss relationship issues, I show that I am listening by repeating what I heard” (men: α ≥ .84; women: α ≥ .86).
Relationship confidence
Participants rated their confidence in the future of their relationships using four items from the Relationship Confidence Scale (Stanley, Hoyer, & Trathen, 1994). Items were rated on a Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Sample items included, “I am very confident when I think of my future with [partner name]” and “I believe [partner name] and I can handle whatever conflicts arise in the future” (men: α ≥ .87; women: α ≥ .91).
Relationship satisfaction
Relationship satisfaction was measured using the Quality of Marriage Index (Norton, 1983). This six-item scale measured global perceptions of relationship satisfaction using a Likert scale ranging from 1 (strongly disagree [questions 1-5] and very unhappy [question 6]) to 5 (strongly agree [questions 1-5] and perfectly happy [question 6]), for example, “[Partner name] and I have a good relationship” (men: α ≥ .92; women: α ≥ .93).
Partner support
Perceived partner support was measured using items from the Spouse Specific Social Support Scale (Culp & Beach, 1998). Five items were used to assess partners’ perceptions of their ability to confide in and receive support from one another; the response set ranged from 1 (almost never) to 5 (almost always). Sample items included, “[Partner’s name] is someone I can confide in,” “I feel I can share my most private worries and fears with [partner’s name],” and “I can tell [partner’s name] about both good things and bad things that happen to me” (men: α ≥ .82; women: α ≥ .87).
Coparenting
Positive coparenting was measured using a 24-item version of the Coparenting Relationship Scale (Feinberg, Brown, & Kan, 2012). This multidimensional self-report measure of coparenting assessed support, closeness, agreement, undermining, and endorsement of the partner’s parenting; the response set ranged from 1 (strongly disagree) to 4 (strongly agree). Sample items included, “We often discuss the best way to meet our child’s needs” and “[Partner’s name] and I have different standards for our child’s behavior” [reverse scored] (men: α ≥ .86; women: α ≥ .90).
Parenting
Parental monitoring and rules enforcement were reported using items from a parenting instrument we have used in previous research with rural African American families. The current scale was composed of seven items rated on a scale ranging from 1 (never) to 5 (all of the time) that assessed the frequency of parental behaviors concerning monitoring (5 items) and household rules (2 items). Sample items included, “When [youth’s name] was going to be with friends outside of school, how often did you find out exactly what s/he would be doing?” and “In the past 30 days, I enforced our house rules” (men: α ≥ .79; women: α ≥ .69).
Program Costs
To estimate provider and family costs, we used a microcosting approach, a method in which all resources used to administer and deliver an intervention are explicitly identified, measured, and valued (National Academies of Sciences Engineering and Medicine, 2016). Additional details of cost categories are described in the Supplemental Material.
Treatment Fidelity
All sessions were audiotaped to allow implementation to be monitored. A sample of sessions (n = 220, corresponding to 25% of all project sessions) was coded using an 87- to 143-point checklist (depending on the session) for adherence to intervention guidelines. All facilitators were assessed at least once. Of the audiotapes reviewed, 10% (n = 22) were coded by more than one rater. The intraclass correlation between raters was .94. Mean fidelity adherence across facilitators was 91% (SD = 9.0%).
Plan of Analysis
We tested intervention effects on rates of change over time using dyadic two-level linear growth curves models (Raudenbush, Brennan, & Barnett, 1995) in Hierarchical Linear Modeling 6.0 software (Raudenbush, Bryk, & Congdon, 2004). Given its capacity to preserve intrapersonal rates of change, growth curve modeling permits more stringent examination of program effects on change over time than do traditional lagged models. For each of the six outcomes, unconditional growth curves first were run to identify measures with significant between-individual variability in rates of change over time. We then added intervention assignment (1 = ProSAAF assignment) as a Level 2 predictor of the slope parameter to determine whether ProSAAF participants changed over time at different rates than did control participants. A different slope among treatment families would indicate not only that differences emerged between treatment and control groups, but also that treatment-specific changes in targeted family constructs continued to diverge between groups over time. To examine mechanisms of program impact, we also conducted mediational analyses to determine whether improved effective communication at W2 would mediate intervention effects on outcomes at W3; these analyses were conducted using path analysis in Mplus 7.4 structural equation modeling software (Muthén & Muthén, 1998–2015). All analyses were conducted according to an intent-to-treat (ITT) approach in which all couples assigned to ProSAAF were compared to all couples assigned to the control group regardless of program attendance. The ITT approach is recommended because it preserves randomization, provides a conservative estimate of program effects, and reflects practical community scenarios of noncompliance (Gupta, 2011).
Results
Treatment and Control Groups’ Equivalence, Descriptive Statistics, and Attrition
We began by conducting equivalence analyses to examine whether experimental groups differed at W1. No differences between conditions at W1 were observed for family characteristics (i.e., marital status, children in the home, income, education, and child age) or study variables (see Supplemental Table S2). Supplemental Table S3 presents the means and standard deviations for study variables. Comparisons by sex on baseline measures indicated that men reported higher initial levels of relationship confidence and satisfaction and less engagement in parenting practices than did women (results available from the first author). Attrition, defined as instances in which no family member participated in the follow-up assessment, was 13.6% at W2 and 12.1% at W3 and did not vary by primary indicators of family processes, sociodemographic variables (i.e., marital status, children in the home, income, education, and child age), or treatment assignment.
Growth Curve Models of Intervention Effects
For analyses of change over time, we first ran unconditional growth curve models to examine the degree of variability in men’s and women’s rates of change over time. Six models were run, one for each of the targeted outcomes (sample equation in Supplemental Material). The results indicated that variance in rate of change was significant for nearly all outcomes; the only exceptions were men’s relationship satisfaction [p = .07], men’s coparenting [p = .06], and women’s parenting [p > .10] (tabulated results available from the first author). Given these results, we proceeded with analyses to determine whether intervention status accounted for variability in rates of change in all outcomes except women’s parenting.
We then added treatment assignment (1 = ProSAAF participant) as a couple-level predictor of men’s and women’s rates of change. This enabled us to test the main effect of the ProSAAF intervention on intra-individual change in targeted outcomes over time. Results, summarized in Table 1 and Figure 1, indicated that ProSAAF participation was associated with significant effects on couple, coparenting, and parenting relationships. Compared with couples in the control condition, ProSAAF families reported improvement over time in effective communication, relationship satisfaction, relationship confidence, partner support, coparenting, and, for men only, intervention-targeting parenting. As shown in Figure 1, ProSAAF couples did not exhibit the general declines in relationship satisfaction, confidence, communication, partner support, coparenting quality, or parenting that characterized couples in the control condition. Thus, consistent with the goals of the program, intervention couples reported better couple and family functioning over time compared with control couples.1
Table 1.
Effect of Intervention on Individuals’ Rates of Change, N = 344 Couples
| Men
|
Women
|
Slope Coefficient Men2
|
Slope Coefficient Women2
|
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | B | SE | p | B | SE | p | ProSAAF | Control | ProSAAF | Control |
|
|
|
|||||||||
| Relationship communication | 0.12** | .04 | .001 | 0.13** | .04 | .001 | .101 | −.097 | .102 | −.119 |
| Relationship confidence | 0.07** | .02 | .001 | 0.05* | .02 | .040 | .016 | −.056 | −.007 | −.054 |
| Relationship satisfaction | 0.09** | .03 | .004 | 0.10** | .03 | .004 | .001 | −.085 | .020 | −.078 |
| Partner support | 0.08** | .03 | .008 | 0.07* | .03 | .018 | −.017 | −.096 | −.038 | −.109 |
| Coparenting | 0.14* | .06 | .033 | 0.19** | .07 | .006 | .001 | −.135 | .026 | −.162 |
| Parenting1 | 0.10** | .03 | .005 | -n/a- | .026 | -.071 | ||||
Between-individual variance in rate of change over time was not significant for women.
All slopes differed significantly between treatment and control groups
p < .05.
p < .01.
Figure 1.
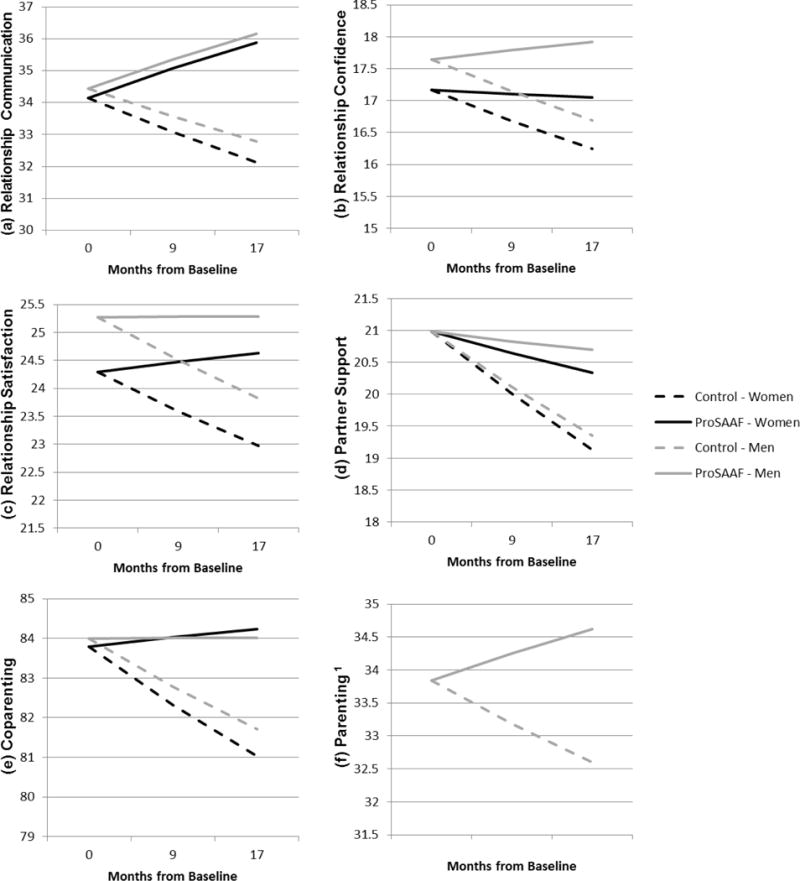
The effect of ProSAAF on rates of change in couple (a-d), coparenting (e) and parenting (f) outcomes.1 Women’s parenting is not shown because the variability between individuals in rate of change over time was not significant.
Mediation Analysis of Intervention Effects
Analyses testing mediation of program effects through effective communication are summarized in Table 2. Results supported the mechanistic role of effective communication for multiple outcomes. First, results from indirect effect (IE) analyses indicated significant IEs through posttest communication for changes in all men’s and women’s outcomes at W3, with the sole exception of women’s parenting. To test full mediation, we also systematically compared a model in which the effect of ProSAAF on men’s or women’s relationship outcomes was constrained to zero to a baseline model in which this effect was freely estimated. Results (also shown in Table 2) indicated no significant decrement in chi-square from the baseline model for men’s and women’s satisfaction and partner support, women’s confidence, and men’s coparenting, thus indicating full mediation of communication on these outcomes (for correlations among 5 outcomes at Wave 5, as well as details on model specification, see Supplemental Table S4 and accompanying text). Thus, mediation analyses confirmed the role of changes in effective communication as mechanism for program effect on other areas.
Table 2.
Summary of ProSAAF Indirect Effects Through Communication (N = 344 dyads)
| Men
|
Women
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Indirect Effect
|
Constrained Model
|
Indirect Effect
|
Constrained Model
|
|||||||
| Outcome | Estimate | 95% CI | χ2 | Δχ2 (1) | p | Estimate | 95% CI | χ2 | Δχ2 (1) | p |
| Satisfaction | .320 | [.030, .716] | 230.182 | 3.103 | .07 | .539 | [.164, 1.03] | 230.028 | 2.949 | .09 |
| Confidence | .184 | [.017, .445] | 233.517 | 6.438 | .01 | .323 | [.087, .611] | 228.053 | 0.974 | .32 |
| Partner support | .304 | [.030, .691] | 230.031 | 2.952 | .09 | .483 | [.152, .930] | 228.689 | 1.610 | .20 |
| Coparenting | .561 | [.065, 1.30] | 228.594 | 1.515 | .22 | .834 | [.260, 1.81] | 230.537 | 4.458 | .04 |
| Parenting | .171 | [.011, .473] | 231.113 | 4.034 | .05 | .046 | [−.031, .231] | — | ||
Note. 95% Confidence Intervals (CI) calculated from 2,000 bootstrapped samples. Baseline Model: χ2 (154) = 227.079. CFI = 0.97. TLI = 0.09. RMSEA = .04, p =.99. Contemporaneous measures between men and women at W1 and W3 were correlated in the model. Constrained model for women’s parenting was not run given lack of significant indirect effect.
p < .05.
p < .01.
Attendance
Of the 172 families assigned to the intervention condition, 81% (n = 139) completed all six sessions. Total sessions attended by remaining families were: 5 sessions, 0.6% (n = 1); 3 sessions, 2.9% (n = 5); 2 sessions, 2.3% (n = 4); 1 session, 4.1% (n = 7); no sessions, 9.3% (n = 16). No differences in high-attending (> 3 sessions) versus low-attending (≤ 3 sessions) couples emerged with respect to marital status, poverty level, or number of children in the home. For booster sessions, 73% (n = 126) of intervention families participated in booster session 1 and 59% (n = 101) participated in booster session 2. All of the families to whom the alternative booster session was offered attended: 4% (n = 7). With the possible exception of the alternative booster, sessions were attended by all family members, including fathers or father figures.
Program Costs
Cost analyses indicated that the mean cost of the program was $1739 per family, with a range of $725 to $3248. This variation arose from differences in number of facilitator visits and travel expenditures per family. Personnel time, travel, and facilitator training combined made up the largest proportion of total program costs (89%). The remaining 11% of the total intervention cost was for a combination of intervention materials, administrative overhead, and prevention supervision. Supplemental Table 4 includes a summary of implementation costs.
Discussion
The ProSAAF program represents one of the first family-centered prevention programs developed to strengthen two-parent African American families with a child in early adolescence, particularly those living in low-resource communities. ProSAAF’s prominent characteristics include its contextualization of CBT-based prevention programming; a focus on multiple family systems, i.e., couple, coparenting, and parenting; and a facilitator-led, in-home delivery model. Results from this study provide important and timely information that supports the efficacy of couple-focused prevention programs to produce change in couple and coparenting dynamics among low-income, ethnic minority populations.
The central aim of the study was to evaluate ProSAAF’s effect on rates of change in couple, coparenting, and parenting trajectories over a 17-month period. Building on the program’s W1 to W2 effects on couple communication, satisfaction, and confidence (Barton et al., 2017) as well as on parenting and child effects in an initial cohort of families (Beach et al., 2016), results from the intent-to-treat growth curve analyses supported the causal effects of ProSAAF participation across all targeted dimensions. Couples in the control group exhibited a general decline in targeted constructs over time, but ProSAAF participants reported largely stable relationship communication, confidence, satisfaction, partner support, coparenting, and parenting from W1 to W3. Furthermore, the linear divergence of the treatment and control groups’ trajectories indicated that treatment effects became more pronounced over time, suggesting that the intervention successfully produced systemic changes in couple relationship dynamics. Thus, the results provide strong evidence for the efficacy of the ProSAAF program and add to other studies showing prevention program effects on African American couple relationship quality and stability (Beach et al., 2014; Stanley et al., 2014). These results also extend research on the impact of programs focused on coparenting, the implementation and impact of which have focused primarily on middle-class, Caucasian parents of newborns and young children (e.g., Feinberg, Jones, Kan, & Goslin, 2010). Hence, current findings demonstrate the 17-month benefits of the program as well as the mechanistic role of effective communication in accounting for its effects.
Mediational analyses supported the hypothesized role of improved effective communication as a mechanism accounting for other program effects. This finding is consistent with previous results that found effective communication to be a plausible mechanism for 9-month program impact on satisfaction and confidence (Barton et al., 2017). Although justifiable reasons exist to examine other intervening variables, this evidence continues to support enhanced effective communication as a plausible point of intervention, particularly when presented as a means to foster couple teamwork and overcome contextual stressors together and not as general “communication skills training.” Collectively, current and previous results from the ProSAAF trial highlight: (a) key processes in the family system (e.g., communication, parental monitoring) that promote change in couple and child outcomes, and (b) the utility of carefully designed and executed cognitive behavioral family interventions for low-income African American families.
In addition to results from analytic models, ProSAAF attendance levels and program costs are important results from the current study. The proportion of couples attending all program sessions, 81%, was higher than rates observed among group-based prevention programs for families (Brown, Feinberg, & Kan, 2012), including those designed for African Americans (Brody, Murry, Chen, Kogan, & Brown, 2006). Attendance rates did not differ with respect to marital status, in contrast to previous studies in which cohabiting couples’ attendance was lower than that of married couples (e.g., Barton et al., 2015). Although attendance levels were generally encouraging, 20% of couples attended three or fewer sessions; this non-attendance emerged despite the no-cost, in-home delivery approach with sessions tailored to couples’ schedule. Program costs, estimated to be slightly more than $1,700 per family, are lower than those of federally-sponsored home visiting programs for new mothers (Zaveri, Burwik, & Maher, 2014), but are higher than the $1200-$1500 per family cost estimated for group-based prevention approaches (Herman et al., 2015; Jones, Feinberg, & Hostetler, 2014). Anecdotally, experiences at our research center have indicated that even less expensive group-based programs are difficult for local community agencies to sustain. Consequently, program costs continue to represent a barrier to widespread implementation, particularly in resource-poor areas of the country. Continued research is needed into innovative delivery approaches that can effectively promote change in family well-being without incurring prohibitive program costs.
Several study limitations should be noted. First, all measures were self-reports. The addition of observational measures of interaction change would strengthen the findings. Second, the control group did not receive the personalized attention that the intervention group received. Simply receiving this attention could have contributed to the changes observed in the ProSAAF participants. Third, the assessment strategy did not investigate the potential moderating effects of contextual stressors or sociodemographic factors. Fourth, long-term impacts on youth development and couple relationship stability remain to be examined. Given potential lagged effects across family subsystems, future research intends to examine program-related changes in couple functioning on subsequent changes in youth outcomes using longer-term follow-up data. These limitations notwithstanding, the results of this prevention trial document the efficacy of the ProSAAF program to promote positive functioning across various relationship dimensions in low-income African Americans families.
Supplementary Material
Acknowledgments
This research was supported by Award Number R01 HD069439 to Steven R. H. Beach from the National Institute of Child Health and Human Development and Award Number P30 DA027827 to Gene H. Brody from the National Institute on Drug Abuse. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Health and Human Development, the National Institute on Drug Abuse, or the National Institutes of Health. The authors thank Eileen Neubaum-Carlan for her editorial assistance in the preparation of this article. We also thank the families for their participation in this research.
Footnotes
Results for females remained unchanged in non-dyadic analyses that included the addition of four female participants from same-sex dyads.
Compliance with Ethical Standards
Disclosure of potential conflicts of interest. The authors report no conflicts of interest.
Research involving human participants. All procedures were approved by the Institutional Review Board of the university at which the research was conducted and complied with the 1964 Helsinki declaration and its later amendments.
Informed consent. Informed consent was obtained from all couples prior to data collection and program participation.
Contributor Information
Allen W. Barton, Center for Family Research, University of Georgia
Steven R. H. Beach, Center for Family Research, University of Georgia
Ashley C. Wells, Center for Family Research, University of Georgia
Justin B. Ingels, Department of Health Policy and Management, University of Georgia
Phaedra S. Corso, Department of Health Policy and Management, University of Georgia
Megan C. Sperr, Center for Family Research, University of Georgia
Tracy N. Anderson, Center for Family Research, University of Georgia
Gene H. Brody, Center for Family Research, University of Georgia
References
- Amato PR. Research on divorce: Continuing trends and new developments. Journal of Marriage and Family. 2010;72(3):650–666. doi: 10.1111/j.1741-3737.2010.00723.x. [DOI] [Google Scholar]
- Amato PR. Marital Quality in African American Marriages. Oklahoma City, OK: National Healthy Marriage Resource Center; 2012. [Google Scholar]
- Amato PR. Does social and economic disadvantage moderate the effects of relationship education on unwed couples? An analysis of data from the 15-Month Building Strong Families evaluation. Family Relations. 2014;63(3):343–355. doi: 10.1111/fare.12069. [DOI] [Google Scholar]
- Barton AW, Beach SR, Hurt TR, Fincham FD, Stanley SM, Kogan SM, Brody GH. Determinants and long‐term effects of attendance levels in a marital enrichment program for African American couples. Journal of Marital and Family Therapy. 2015;42(2):272–287. doi: 10.1111/jmft.12126. [DOI] [PubMed] [Google Scholar]
- Barton AW, Beach SRH, Lavner JA, Bryant CM, Kogan SM, Brody GH. Is communication a mechanism of relationship education effects among rural African Americans? Journal of Marriage and Family. 2017;79:1450–1461. doi: 10.1111/jomf.12416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beach SRH, Barton AW, Lei MK, Brody GH, Kogan SM, Hurt TR, Stanley SM. The effect of communication change on long-term reductions in child exposure to conflict: Impact of the Promoting Strong African American Families (ProSAAF) program. Family Process. 2014;53(4):580–595. doi: 10.1111/famp.12085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beach SRH, Barton AW, Lei MK, Mandara J, Wells AC, Kogan SM, Brody GH. Decreasing substance use risk among African American youth: Parent-based mechanisms of change. Prevention Science. 2016:1–12. doi: 10.1007/s11121-016-0651-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bodenmann G, Hilpert P, Nussbeck FW, Bradbury TN. Enhancement of couples’ communication and dyadic coping by a self-directed approach: A randomized controlled trial. Journal of Consulting and Clinical Psychology. 2014;82(4):580–591. doi: 10.1037/a0036356. [DOI] [PubMed] [Google Scholar]
- Brody GH, Murry VM, Chen Y-F, Kogan SM, Brown AC. Effects of family risk factors on dosage and efficacy of a family-centered preventive intervention for rural African Americans. Prevention Science. 2006;7(3):281–291. doi: 10.1007/s11121-006-0032-7. [DOI] [PubMed] [Google Scholar]
- Brody GH, Murry VM, Gerrard M, Gibbons FX, Molgaard V, McNair L, Neubaum-Carlan E. The Strong African American Families program: Translating research into prevention programming. Child Development. 2004;75(3):900–917. doi: 10.1111/j.1467-8624.2004.00713.x. [DOI] [PubMed] [Google Scholar]
- Brown LD, Feinberg ME, Kan ML. Predicting engagement in a transition to parenthood program for couples. Evaluation and Program Planning. 2012;35(1):1–8. doi: 10.1016/j.evalprogplan.2011.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conger RD, Elder GH., Jr . Families in troubled times. New York: Aldine De Grutyer; 1994. [Google Scholar]
- Cowan PA, Cowan CP. Controversies in couple relationship education (CRE): Overlooked evidence and implications for research and policy. Psychology, Public Policy, and Law. 2014;20(4):361–383. doi: 10.1037/law0000025. [DOI] [Google Scholar]
- Culp LN, Beach SRH. Marriage and depressive symptoms. Psychology of Women Quarterly. 1998;22(4):647–663. doi: 10.1111/j.1471-6402.1998.tb00183.x. [DOI] [Google Scholar]
- Cutrona CE, Russell DW, Burzette RG, Wesner KA, Bryant CM. Predicting relationship stability among midlife African American couples. Journal of Consulting and Clinical Psychology. 2011;79(6):814–825. doi: 10.1037/a0025874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeNavas-Walt C, Proctor BD. Income and poverty in the United States: 2013 (Current Population Reports P60–249) Washington, DC: U.S. Census Bureau; 2014. [Google Scholar]
- Doss BD, Cicila LN, Georgia EJ, Roddy MK, Nowlan KM, Benson LA, Christensen A. A randomized controlled trial of the web-based OurRelationship program: Effects on relationship and individual functioning. Journal of Consulting and Clinical Psychology. 2016;84(4):285–296. doi: 10.1037/ccp0000063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Erel O, Burman B. Interrelatedness of marital relations and parent-child relations: A meta-analytic review. Psychological Bulletin. 1995;118(1):108–132. doi: 10.1037/0033-2909.118.1.108. [DOI] [PubMed] [Google Scholar]
- Feinberg ME, Brown LD, Kan ML. A multi-domain self-report measure of coparenting. Parenting. 2012;12(1):1–21. doi: 10.1080/15295192.2012.638870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feinberg ME, Jones DE, Kan ML, Goslin MC. Effects of family foundations on parents and children: 3.5 years after baseline. Journal of Family Psychology. 2010;24(5):532–542. doi: 10.1037/a0020837. [DOI] [PubMed] [Google Scholar]
- Gross D, Julion W, Fogg L. What motivates participation and dropout among low-income urban families of color in a prevention intervention?*. Family Relations. 2001;50(3):246–254. doi: 10.1111/j.1741-3729.2001.00246.x. [DOI] [Google Scholar]
- Gupta SK. Intention-to-treat concept: A review. Perspectives in Clinical Research. 2011;2(3):109–112. doi: 10.4103/2229-3485.83221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herman PM, Mahrer NE, Wolchik SA, Porter MM, Jones S, Sandler IN. Cost-benefit analysis of a preventive intervention for divorced families: Reduction in mental health and justice system service use costs 15 years later. Prevention Science. 2015;16(4):586–596. doi: 10.1007/s11121-014-0527-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hurt TR, Beach SRH, Stokes LA, Bush PL, Sheats KJ, Robinson SG. Engaging African American men in empirically based marriage enrichment programs: Lessons from two focus groups on the ProSAAM project. Cultural Diversity and Ethnic Minority Psychology. 2012;18(3):312–315. doi: 10.1037/a0028697. [DOI] [PubMed] [Google Scholar]
- Jenkins NH, Saiz CC. Unpublished manuscript. University of Denver; Denver, CO: 1995. The Communication Skills Test. [Google Scholar]
- Johnson MD. Healthy marriage initiatives: On the need for empiricism in policy implementation. American Psychologist. 2012;67(4):296–308. doi: 10.1037/a0027743. [DOI] [PubMed] [Google Scholar]
- Johnson MD, Bradbury TN. Contributions of Social Learning Theory to the promotion of healthy relationships: Asset or liability? Journal of Family Theory & Review. 2015;7(1):13–27. doi: 10.1111/jftr.12057. [DOI] [Google Scholar]
- Jones DE, Feinberg ME, Hostetler ML. Costs to implement an effective transition-to-parenthood program for couples: Analysis of the Family Foundations program. Evaluation and Program Planning. 2014;44:59–67. doi: 10.1016/j.evalprogplan.2014.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kumpfer KL, Alvarado R, Smith P, Bellamy N. Cultural sensitivity and adaptation in family-based prevention interventions. Prevention Science. 2002;3(3):241–246. doi: 10.1023/a:1019902902119. [DOI] [PubMed] [Google Scholar]
- Kumpfer KL, Molgaard V, Spoth R. The Strengthening Families Program for the prevention of delinquency and drug use. In: Peters RD, McMahon RJ, editors. Preventing childhood disorders, substance use, and deliquency. Thousand Oaks, CA: Sage; 1996. [Google Scholar]
- Lavner JA, Karney BR, Bradbury TN. New directions for policies aimed at strengthening low-income couples. Behavioral Science and Policy. 2015;1:13–24. [Google Scholar]
- Lerman R. Economic perspectives on marriage: Causes, consequences, and public policy. In: Cohen L, Wright JD, editors. Research Handbook on the Economics of Family Law. Cheltenham, UK: Edward Elgar Publishing; 2013. [Google Scholar]
- Lundquist E, Hsueh J, Lowenstein AE, Faucetta K, Gubits D, Michalopoulos C, Knox V. A family-strengthening program for low-income families: Final impacts from the supporting healthy marriage evaluation. New York: MDRC; 2014. [Google Scholar]
- Markman HJ, Stanley SM, Blumberg S, Jenkins NH, Whaley C. Twelve Hours to a Great Marriage. San Francisco: Jossey-Bass; 2004. [Google Scholar]
- Marks LD, Hopkins K, Chaney C, Monroe PA, Nesteruk O, Sasser DD. “Together, We Are Strong”: A qualitative study of happy, enduring African American marriages. Family Relations. 2008;57(2):172–185. doi: 10.1111/j.1741-3729.2008.00492.x. [DOI] [Google Scholar]
- Muthén LK, Muthén BO. Mplus User’s Guide. 7th. Los Angeles, CA: Muthén & Muthén; 1998–2015. [Google Scholar]
- National Academies of Sciences Engineering and Medicine. Advancing the power of economic evidence to inform investments in children, youth, and families. Washington, DC: The National Academies Press; 2016. [PubMed] [Google Scholar]
- Neff LA. Putting marriage in its context: The influence of external stress on early marital development. In: Campbell L, Loving TJ, editors. Interdisciplinary research on close relationships: The case for integration. Washington, DC: APA Books; 2012. [Google Scholar]
- Norton R. Measuring marital quality: A critical look at the dependent variable. Journal of Marriage and Family. 1983;45(1):141–151. [Google Scholar]
- Owen J, Quirk K, Bergen C, Inch LJ, France T. The effectiveness of PREP with lower-income racial/ethnic minority couples. Journal of Marital and Family Therapy. 2012;38:296–307. doi: 10.1111/j.1752-0606.2012.00294.x. [DOI] [PubMed] [Google Scholar]
- Randall AK, Bodenmann G. The role of stress on close relationships and marital satisfaction. Clinical Psychology Review. 2009;29(2):105–115. doi: 10.1016/j.cpr.2008.10.004. [DOI] [PubMed] [Google Scholar]
- Raudenbush SW, Brennan RT, Barnett RC. A multivariate hierarchical model for studying psychological change within married couples. Journal of Family Psychology. 1995;9(2):161–174. doi: 10.1037/0893-3200.9.2.161. [DOI] [Google Scholar]
- Raudenbush SW, Bryk AS, Congdon R. HLM 6 for Windows [Computer software] Skokie, IL: Scientific Software International, Inc; 2004. [Google Scholar]
- Rhoades GK. The effectiveness of the Within Our Reach relationship education program for couples: Findings from a federal randomized trial. Family Process. 2015;54(4):672–685. doi: 10.1111/famp.12148. [DOI] [PubMed] [Google Scholar]
- Robles TF, Slatcher RB, Trombello JM, McGinn MM. Marital quality and health: A meta-analytic review. Psychological Bulletin. 2014;140(1):140–187. doi: 10.1037/a0031859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanley SM, Blumberg S, Markman HJ. Helping couples fight for their marriages: The PREP approach. In: Berger R, Hannah M, editors. Handbook of preventive approaches in couple therapy. New York: Brunner/Mazel; 1999. pp. 279–303. [Google Scholar]
- Stanley SM, Hoyer L, Trathen DW. Unpublished manuscript. University of Denver; Denver, CO: 1994. The Confidence Scale. [Google Scholar]
- Stanley SM, Johnson CA, Amato PR, Markman HJ. Premarital education, marital quality, and marital stability: Findings from a large, random household survey. Journal of Family Psychology. 2006;20(1):117–126. doi: 10.1037/0893-3200.20.1.117. [DOI] [PubMed] [Google Scholar]
- Stanley SM, Rhoades GK, Loew BA, Allen ES, Carter S, Osborne LJ, Markman HJ. A randomized controlled trial of relationship education in the U.S. Army: 2‐year outcomes. Family Relations: An Interdisciplinary Journal of Applied Family Studies. 2014;63(4):482–495. doi: 10.1111/fare.12083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trail TE, Karney BR. What’s (not) wrong with low-income marriages. Journal of Marriage and Family. 2012;74(3):413–427. doi: 10.1111/j.1741-3737.2012.00977.x. [DOI] [Google Scholar]
- Whisman MA, Uebelakcer LA. Impairment and distress associated with relationship discord in a national sample of married or cohabiting adults. Journal of Family Psychology. 2006;20:369–377. doi: 10.1037/0893-3200.20.3.369. [DOI] [PubMed] [Google Scholar]
- Williamson HC, Altman N, Hsueh J, Bradbury TN. Effects of relationship education on couple communication and satisfaction: A randomized controlled trial with low-income couples. Journal of Consulting and Clinical Psychology. 2016;84(2):156–166. doi: 10.1037/ccp0000056. [DOI] [PubMed] [Google Scholar]
- Wood RG, Moore Q, Clarkwest A, Killewald A. The long-term effects of Building Strong Families: A program for unmarried parents. Journal of Marriage and Family. 2014;76(2):446–463. doi: 10.1111/jomf.12094. [DOI] [Google Scholar]
- Zaveri H, Burwik A, Maher E. The potential for cost savings from home visiting due to reductions in child maltreatment. Chicago, IL: Chapin Hall; 2014. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.