

Resting tremor is part of the classical parkinsonian triad and classically observed in the upper or lower limbs, legs, mandible, chin, and lips, but tongue tremor is far less often reported, especially as a revealing manifestation of Parkinson's disease (PD).1 Here, we describe a 63‐year‐old patient with a resting tongue tremor as the first symptom of PD.
Observation
A 63‐year‐old patient, without any family medical history, was referred for permanent and disabling abnormal movements of the tongue, which represented his only complaint. This abnormal movement lasted for 1 year and started after a transient ischemic attack characterized by dysarthria and ataxia. Since then, this abnormal movement has persisted, and a mild, intermittent right‐hand tremor accompanied by micrographia then appeared a few months later. The patient was first treated by his general practitioner with gabapentine (800 mg/day) and piribedil (150 mg/day) without any improvement, but with side effects such as nausea and vomiting. The patient was then referred to our neurological department. Neurological examination showed a mild, slow, pill‐rolling resting tremor of the right hand's thumb, an intermittent tremor of the mandible, and a severe rest tremor of the tongue. Tongue tremor disappeared when the tongue was protracted and then reappeared after a few seconds, suggesting a re‐emergence phenomenon (see Video 1). A mild rigidity (1/4 on item 3.3 of the International Parkinson and Movement Disorder Society UPDRS part III score) and bradykinesia of the right arm, as well as a loss of right‐arm swing when walking, were also noted (see Video 1). The rest of the neurological examination was normal.
Brain MRI was normal. Tremor recording was performed, with a SYNERGY‐MEDELEC device. EMG (electromyography) signals were obtained from pairs of silver/silver chloride electrodes placed over the arms’ muscle bellies. As regards the tongue, EMG signal was obtained from adhesive electrodes placed after drying the surface of the tongue. Bandpass was filtered at 20 to 500 Hz. Frequency of tremor and burst duration were measured by manual analysis of EMG. The recording confirmed a 5‐Hz rest tremor of the tongue and right hand (Fig. 1B). 123I‐FP‐CIT single‐photon emission CT (SPECT) demonstrated a marked reduction of tracer uptake in the left striatum (Fig. 1A). Thus, a diagnosis of probable PD, revealed by predominant tongue tremor, was suspected and pramipexole was prescribed at 1.05 mg/day. After 2 months, this treatment led to a clear improvement of body bradykinesia, but not of tongue tremor. Thus, the dose was further increased to 2.1 mg/day.
Figure 1.
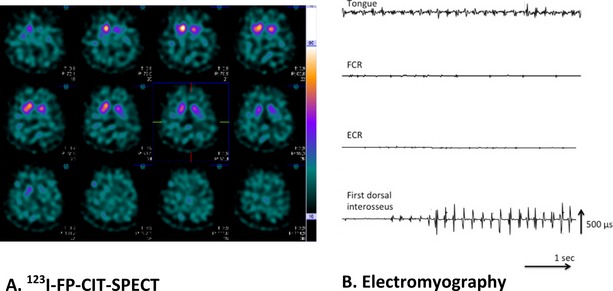
(A) 123I‐FP‐CIT‐SPECT. Asymmetrical reduction of tracer uptake in the left striatum with rostrocaudal gradient. (B) EMG. Polymyographic recording obtained on the right upper limb concern the ECR (extensor carpi radialis), FCR (flexor carpi radialis), and first dorsal interosseous. Polymyographic recording obtained on the tongue shows a regular tremor at 5 Hz, with 90‐ms‐length bursts, intermingled by silent EMG. A regular 5‐Hz oscillation was also recorded on the first dorsal interosseous, composed of 60‐ms‐length bursts, intermingled by silent EMG, and elicited by counting backward. The FCR and ECR are completely inactive.
Discussion
This observation is an uncommon case of de novo PD revealed by a disabling tongue tremor. Tremors of the mandible or chin are relatively frequent in PD, but, more rarely, involve the tongue and usually do not represent a burden for the patient, contrary to what was observed here. The clinical (at rest, re‐emergence phenomenon) aspect of this tongue tremor was suggestive of a parkinsonian tremor. In addition, its electrophysiological (5‐Hz frequency) characteristics were within the range of parkinsonian tremor frequency. This hypothesis was supported by a DATscan showing a dopaminergic denervation in the left striatum.
This observation illustrates that parkinsonian rest tremor can affect various body parts, going from the classical asymmetrical hand or foot tremor to mandible or chin tremor and to much less common presentations such as head tremor.1, 2, 3 Among these unusual initial presentations of PD, tongue tremor has never, to our knowledge, been reported.
Tongue tremor can be also observed in essential tremor. Indeed, Biary and Koller reviewed 20 patients with essential tongue tremor.4 Postural tremor of the upper limbs was present in 16 of 20 patients, and 3 patients had isolated tongue tremor. In these observations, tongue tremor appeared when the tongue was protracted, and it was associated with voice disturbance, which was different from our case. Another differential diagnosis is drug‐induced orolingual tremor. Gabellini et al. reported on 2 cases of tongue tremor after treatment with thioridazine and flunarizine.5 Neuroleptic medication can indeed cause parkinsonism with rest tremor, involving the jaws, but the tongue as well.6 Such etiology was excluded in the present case report. Tongue tremor can also be task specific or associated with oromandibular dystonia (dystonic tremor) or with a dystonia affecting other body parts (tremor associated with dystonia) or can be of indeterminate origin.7
In conclusion, this observation shows that PD can be revealed by a predominant rest tremor of the tongue and that clinicians have to be aware of this rare presentation. Clinical examination may reveal additional features of PD, although not noticed by the patient. A meticulous interrogation is mandatory to exclude neuroleptic intake. DATscan may be useful in uncertain situations. Finally, the disappearance of tongue tremor with levodopa or dopamine agonists will further support the diagnosis of PD.
Author Roles
(1) Research Project: A. Conception, B. Organization, C. Execution; (2) Statistical Analysis: A. Design, B. Execution, C. Review and Critique; (3) Manuscript Preparation: A. Writing of the First Draft, B. Review and Critique.
P.J.: 1A, 1C, 3A, 3B
C.L.: 1C, 3B
H.R.: 1C, 3B
S.T.: 1A, 1C, 3A, 3B
Disclosures
Funding Sources and Conflicts of Interest: The authors report no sources of funding and no conflicts of interest.
Financial Disclosures for previous 12 months: S.T. has received honoraria from TEVA and UCB.
Supporting information
A video accompanying this article is available in the supporting information here.
Video 1. Segment 1: A rest tongue tremor, which disappears after tongue protraction. Then, a re‐emergence of the tremor is observed. A mild hand rest tremor is present. Segment 2: A bradykinesia of the right hand. Segment 3: A reduced right‐arm swing and right‐hand tremor when walking.
Relevant disclosures and conflicts of interest are listed at the end of this article.
References
- 1. Josephs KA, Matsumoto JY, Ahlskog JE. Benign tremulous parkinsonism. Arch Neurol 2006;63:354–357. [DOI] [PubMed] [Google Scholar]
- 2. Roze E, Coêlho‐Braga MC, Gayraud D, et al. Head tremor in Parkinson's disease. Mov Disord 2006;21:1245–1248. [DOI] [PubMed] [Google Scholar]
- 3. Gan J, Xie‐Brustolin J, Gervais‐Bernard H, Vallet AE, Broussolle E, Thobois S. Possible Parkinson's disease revealed by a pure head resting tremor. J Neurol Sci 2009;279:121–123. [DOI] [PubMed] [Google Scholar]
- 4. Biary N, Koller WC. Essential tongue tremor. Mov Disord 1987;2:25–29. [DOI] [PubMed] [Google Scholar]
- 5. Gabellini AS, Martinelli P, Coccagna G. Drug‐induced tremor of the tongue. Ital J Neurol Sci 1989;10:89–91. [DOI] [PubMed] [Google Scholar]
- 6. Hardie RJ, Lees AJ. Neuroleptic‐induced Parkinson's syndrome: clinical features and results of treatment with levodopa. J Neurol Neurosurg Psychiatry 1988;51:850–854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Silverdale M, Schneider S, Bhatia K, Lang AE. The spectrum of orolingual tremor. A proposed classification system. Mov Disord 2008;23:159–167. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
A video accompanying this article is available in the supporting information here.
Video 1. Segment 1: A rest tongue tremor, which disappears after tongue protraction. Then, a re‐emergence of the tremor is observed. A mild hand rest tremor is present. Segment 2: A bradykinesia of the right hand. Segment 3: A reduced right‐arm swing and right‐hand tremor when walking.