

Abstract
Experiencing sexual victimization (SV) prior to becoming homeless is common among homeless youth and is associated with increased HIV risk behavior. This study examined mediating variables that underlie this association, adding to the understanding of gender differences in these paths. Participants were homeless youth in Los Angeles recruited through service access centers who completed a computerized self-administered interview in English or Spanish using an iPad. Findings indicate a high presence of SV across both genders. Female participants experienced PTSD and subsequent engagement with exchange sex, whereas male participants were primarily involved in substance use risk pathways. Results indicate paths in the association between SV and HIV risk behavior differ between male and female homeless youth. Gender-specific, mental-health-informed interventions targeting sexual risk reduction are warranted.
Keywords: Gender issues, Adolescents, Adult survivors, Sexual Abuse, Substance Use, Mental Health
Sexual victimization (SV), including child sexual abuse, sexual assault, and rape, is reported at greater rates among homeless youth compared to their nonhomeless peers (Coates & McKenzie-Mohr, 2010; U.S. Department of Health and Human Services, 2009; Zerger, Strehlow & Gundlapalli & 2008; Tyler, Hoyt, Whitbeck, & Cauce, 2001). SV commonly occurs prior to becoming homeless and is of particular salience because it is often a precipitant of leaving the home (Martijn & Sharpe, 2006). Human immunodeficiency virus (HIV) risk behavior is one of the adverse health outcomes of SV, with high rates of exchange sex, low condom use, more sexual partners, and concurrent sexual partners reported among those with SV histories (Senn, Carey, Vanable, Coury-Doniger, & Urban, 2007). These behaviors increase the likelihood of contracting sexually transmitted infections (STIs) (Giradet et al., 2009; Reynolds, Peipert, & Collins, 2000) and HIV (Wilson, 2010; Wilson & Widom, 2008; Zierler et al., 1991), constituting a growing public health concern among homeless youth.
A model explaining how SV can lead to HIV risk behavior proposes that this relationship is mediated through several causal pathways including drug use, sexual adjustment, psychopathology, and socioenvironmental factors (Miller, 1999). This model was developed based on female samples, but has been supported in research with male samples (Icard et al., 2014; O’Leary, Purcell, Remien & Gomez, 2003; Holmes, Foa & Sammel, 2005; Paul, Catania, Pollack & Stall, 2001). Although mediating variables in this association have been empirically substantiated independently, few studies have analyzed multiple mechanisms together among adolescents or young adults (Littleton, Breitkopf & Berenson, 2007; Northcott, 2010; Melander & Tyler, 2010). Furthermore, in addition to existing gender differences regarding HIV risk behavior (Halcón & Lifson, 2004), research has indicated there may be differences in internalization of SV and coping mechanisms for victimized men and women (Bornovalova, Ouimette, Crawford & Roy, 2009; Senn et al., 2007; Ullman & Vasquez, 2015). Yet, the influence of gender on the relationship between SV and HIV risk behavior remains unclear. Studies of these associations have tended to be limited to one gender or combined both in a single analysis (Senn, Carey, & Vanable, 2008). This may be due to the limited availability of samples that include substantial numbers of both male and female victims (Senn, Carey, & Vanable, 2008). To date, Melander and Tyler (2010) conducted the study best aligned with exploration and analyses of these relationships. This study included additional mediating variables, delineating HIV risk behavior outcomes, and stratifying by gender to understand potential differences in pathways for young men and women. This study found that compared to males, females were more likely to experience partner violence and sexual victimization and females that reported these experiences were more likely to engage in HIV risk behaviors (Melander & Tyler, 2010).
In addition to HIV risk behavior (Senn et al., 2008; Senn et al., 2007), SV is associated with other maladaptive social experiences and emotional outcomes (Barnes, Noll, Putnam & Trickett, 2009; Gwadz, Nish, Leonard, & Strauss, 2007; Kessler et al., 2010; Olshen, McVeigh, Wunsch-Hitzig, & Rickert, 2007; Marshall, DeBeck, Simo, Kerr, & Wood, 2015; Molnar, Shade, Kral, Booth, & Watters, 1998; Noell, Rohde, Seeley, & Ochs, 2001; Simpson & Miller, 2002; Slesnick, Erdem, Collins, Patton, & Buettner, 2010; Tyler et al., 2001; Tyler, 2002; Tyler, Hoyt & Whitbeck, 2000; Wilson, 2010; Wilson & Widom, 2009). These outcomes often serve as mediators in the relationship between SV and HIV risk behavior, exacerbating the likelihood of engaging in sexual risk (Johnson, Rew, & Sternglanz, 2006). Although social and emotional outcomes can be numerous and comorbid, the current study focused on three commonly reported emotional responses to SV that can serve as mediators, namely (a) posttraumatic stress disorder (PTSD), (b) substance use (i.e., illicit drug use, binge drinking), and (c) suicidal ideation, and three negative mediating social experiences, namely (d) gang involvement, (e) intimate partner violence (IPV), and (f) sexual revictimization.
Many negative emotional health conditions have been identified as consequences of SV (Gwadz, Nish, Leonard, & Strauss, 2007; Olshen, McVeigh, Wunsch-Hitzig, & Rickert, 2007; Kessler et al., 2010; Molnar, Shade, Kral, Booth, & Watters, 1998; Simpson & Miller, 2002; Wilson, 2010). Given the traumatizing effects of SV, high rates of PTSD are reported among sexually victimized homeless youth, with some indication of a higher prevalence among women (Gwadz, Nish, Leonard, & Strauss, 2007). Among sexually victimized youth, having PTSD is associated with increased risky sexual behavior (Danielson et al., 2009). Among urban teenagers, a history of SV has also been identified as a correlate of suicidality for both young men and women (Olshen, McVeigh, Wunsch-Hitzig, & Rickert, 2007). Furthermore, youth with suicidal histories report greater sexual risk and STI rates (Huock et al., 2008). SV also increases the likelihood of high-frequency use and misuse of substances (Kessler et al., 2010; Simpson & Miller, 2002; Wilson, 2010), and maladaptive use of substances intensifies sexual risk behaviors (Bailey, Camlin, & Ennett, 1998; Bensley, Van Eenwyk, & Simmons, 2000; Connell, Gilreath, & Hansen, 2009). Specifically, SV has been associated with illicit drug use (Rew, Taylor-Seehafer, & Fitzgerald, 2001), exchange sex (Haley, Roy, Leclerc, Boudreau, & Boivin, 2004), multiple sexual partners, and inconsistent condom use (Solorio et al., 2008) among homeless youth.
In addition to contributing to youth running away from home, SV can result in maladaptive social outcomes (Barnes, Noll, Putnam & Trickett, 2009; Marshall, DeBeck, Simon, Kerr, & Wood, 2015; Noell, Rohde, Seeley, & Ochs, 2001; Slesnick, Erdem, Collins, Patton, & Buettner, 2010; Tyler et al., 2001; Tyler, 2002; Tyler, Hoyt & Whitbeck, 2000). Research has indicated SV contributes to gang involvement (Tyler, 2002), with a recent study of gang-involved youth suggesting that young women were more likely than young men to report a history of SV (Marshall, DeBeck, Simon, Kerr, & Wood, 2015). Adolescents who participate in gangs have significantly increased risk of contracting STIs (Buffardi et al., 2008). Homeless youth who report recent time spent with gang-affiliated peers have also demonstrated increased HIV risk behavior (Rice, Milburn, & Rotheram-Borus, 2007). With regard to revictimization, SV has been identified as predictive risk factor (Barnes, Noll, Putnam & Trickett, 2009) and two studies of adolescent homeless girls indicated that early SV increases the likelihood of being later sexually revictimized (Noell, Rohde, Seeley, & Ochs, 2001; Tyler et al., 2001) and that this experience increases HIV risk behavior and STI reporting (Noell et al., 2001). Homeless youth with SV histories are also more likely to report IPV (Slesnick, Erdem, Collins, Patton, & Buettner, 2010), which is associated with sexual risk taking, inconsistent condom use, unplanned pregnancies, and contracting STIs (Coker, 2007).
The current study presented a rare opportunity to assess multiple mediators in the relationship between SV and HIV risk behaviors, with several indicators of HIV risk, across a sample featuring substantial numbers of both male and female homeless youth, allowing for examination of gender differences. Interventions targeting sexual risk reduction for young men and women may benefit from an understanding of gender-specific pathways from SV to HIV risk behavior. Based on the empirical associations established thus far, we hypothesized that one or more of the six identified potential mediators—suicidal ideation, PTSD, substance use, IPV, revictimization, and gang involvement—would have indirect effects on this pathway among young women. Given a lower prevalence of SV associated with reporting of revictimization, PTSD, and gang involvement among young men, we predicted suicidal ideation, substance use, and IPV would be significant mediators for young men in the sample.
Methods
Participants in this study consisted of homeless youth aged 14 to 24, recruited from one of three drop-in centers between October 2011 and June 2013. The study featured four recruitment waves. Respondents were eligible if they were receiving services from a partnering agency and were recruited by study investigators during operating business hours. A sample of 1,046 youth was recruited from three drop-in centers, located in Santa Monica, Hollywood, and Venice, California.
All youth accessing services in these locations were invited to complete a self-administered self-interview survey; 80.19% agreed to participate. Two staff members monitored the recruitment process to ensure all individuals receiving services during these periods were screened for eligibility and youth did not complete the survey more than once. All participants received a $20 incentive in cash or a gift card. Survey items assessed demographic characteristics (e.g., age, race, gender, sexual orientation), mental health, historical and recent trauma, sex behavior, substance use, and sociocultural factors. All study procedures were approved by the University of Southern California Institutional Review Board.
Measures
Independent and control variables.
Respondents were asked to report their age, gender, race, and sexual orientation. Participants included in the study were recruited because they were seeking and accessing services at one of the partnering access centers. Individuals older than the age of 25 (14 women, 49 men) were excluded from these analyses because they were considered to have aged out of the typical youth range. In addition, individuals identifying as transgender (13 male to female, 4 female to male) were excluded because the subsample size was too small for analyses. The removal of these individuals resulted in an analytic sample of 966 participants (280 women, 686 men). Respondents self-selected the racial category that best described them and self-reported their sexual orientation. See Table 1 for demographic statistics of the sample.
Table 1.
Demographic Characteristics
| Total | Women | Men | |
|---|---|---|---|
| (N = 966) | (n = 280) | (n = 686) | |
| n (%) | n (%) | n (%) | |
| Agea | 21.09 (1.93) | 20.65 (1.92) | 21.25 (1.91) |
| Race | |||
| American Indian or Alaska Native | 26 (2.69) | 6 (2.30) | 20 (2.92) |
| Asian | 6 (0.62) | 3 (1.15) | 20 (2.92) |
| Black or African American | 231 (23.91) | 68 (26.05) | 3 (0.44) |
| Latino or Hispanic | 129 (13.35) | 34 (13.03) | 95 (13.85) |
| Native Hawaiian or Pacific Islander | 6 (0.62) | 2 (0.77) | 4 (0.58) |
| White | 364 (37.68) | 83 (31.80) | 281 (40.96) |
| Mixed | 185 (19.15) | 65 (24.90) | 120 (17.49) |
| Sexual orientation | |||
| Homosexual | 68 (7.04) | 28 (10.85) | 40 (5.95) |
| Queer | 7 (0.72) | 5 (1.94) | 2 (0.30) |
| Bisexual | 131 (13.56) | 81 (31.40) | 50 (7.44) |
| Heterosexual | 700 (72.46) | 134 (51.94) | 566 (84.23) |
| Questioning or unsure | 24 (2.48) | 10 (3.88) | 14 (2.08) |
| Sexual victimizationb | 197 (20.39) | 86 (33.64) | 111 (15.56) |
| Emotional outcomes | |||
| Binge drinkingc | 455 (47.10) | 99 (39.44) | 356 (53.7) |
| Methamphetaminec | 228 (23.60) | 52 (20.47) | 176 (26.51) |
| Cocaine or crackc | 152 (15.73) | 38 (15.08) | 114 (17.17) |
| Heroinc | 98 (10.14) | 18 (7.17) | 80 (12.07) |
| Probable PTSDc | 262 (27.12) | 95 (38.15) | 167 (25.65) |
| Suicidal ideationd | 155 (16.05) | 50 (19.76) | 105 (15.65) |
| Social outcomes | |||
| Intimate partner violenced | 190 (19.67) | 58 (22.83) | 132 (19.73) |
| Revictimizatione | 57 (34.13) | 28 (32.56) | 29 (26.13) |
| Gang involvementf | 86 (8.90) | 19 (12.34) | 67 (16.58) |
| Sexual behaviorg | |||
| Unprotected vaginal sex | 411 (42.55) | 147 (52.50) | 264 (38.48) |
| Unprotected anal sex | 92 (9.52) | 13 (4.64) | 79 (11.52) |
| Multiple partners | 189 (19.57) | 48 (19.05) | 141 (21.04) |
| Concurrent sex | 308 (31.88) | 77 (32.91) | 231 (38.76) |
| Exchange sex | 153 (15.84) | 41 (16.80) | 112 (17.92) |
Figures represent M (SD); range = 14–24
Self-report of sexual victimization prior to homelessness
During previous 30 days
During previous year
Self-reported sexual victimization prior to and after homelessness
During lifetime
During previous 3 months
For this study, SV was defined as “one or more experiences of sexual assault or rape by an adult or older peer prior to homelessness.” This variable was assessed via two survey questions: “Have you ever had an adult or someone much older touch your private sexual body parts when you did not want them to?” and “Have you ever been physically forced to have sex when you did not want to?” These items were adapted from the UCLA PTSD Index for DSM-IV (Pynoos, Rodriguez, Steinberg, Stuber, & Frederick, 1998). Although there were not any indicators for the age at which SV experiences occurred, a follow-up question about event timing assessed whether the trauma occurred prior to or after homelessness, or both. The UCLA PTSD Index has been broadly used in clinical evaluation, trauma research, and post-disaster screening and recovery programs across various settings and cultures in the U.S. and other parts of the world, including with adolescents exposed to community violence and sexual assault (Steinberg, Brymer, Decker, & Pynoos, 2004). The DSM-IV version has good convergent validity with (0.82 in comparison to the Child and Adolescent Version of the Clinician-administered PTSD Scale) and good to excellent test-retest reliability with Cronbach’s alpha in the range of .90 (Steinberg, Brymer, Decker, & Pynoos, 2004).
Mediating variables.
The survey assessed symptoms of PTSD experienced during the previous month using the Primary Care PTSD Screen (Prins et al., 2003). This 4-item measure assesses cognitive intrusion, avoidance, hyper vigilance, and detachment, with a score of 3 or higher indicating probable PTSD (Prins et al., 2003). This measure has good test-re-test reliability (.83), a specificity rate of 0.87, a positive predictive value of 0.65, and a negative predictive value of 0.92 (Prins et al., 2003). Substance use measures were adapted from the Youth Risk Behavior Surveillance (YRBS) study (Eaton et al., 2012). Binge drinking was defined as having five or more drinks within a few hours at least once during the previous 30 days (Eaton et al., 2012). Illicit drug use during the previous 30 days was assessed as any use of cocaine, methamphetamine, or heroin (Eaton et al., 2012). Items related to alcohol and other drug use from the YRBS survey have demonstrated good reliability (Brenner et al., 2002). Suicidal ideation during the previous 12 months was measured by asking participants if they had seriously considered attempting suicide (May & Klonsky, 2011). Convergent and discriminant validity of suicidality items from the YRBS study have been supported in research (May & Klonsky, 2011).
Negative social mediating variables included lifetime gang involvement, past-year physical IPV, and revictimization after being homeless. IPV was defined as being hit, slapped, or physically hurt by a boyfriend or girlfriend during the previous year (Straus, Hamby, Boney-McCoy, & Sugarman, 1996). Revictimization was measured by participants’ self-reported experience of an assault or rape after becoming homeless. Participants were considered revictimized only if they endorsed SV both prior to and after homelessness (Pynoos et al., 1998).
Dependent variables.
All five outcomes of HIV risk behavior, namely having multiple sexual partners, unprotected vaginal sex, unprotected anal sex, concurrent sex, and exchange sex, were assessed relative to the previous 3 months and were original or adapted items from the Youth Risk Behavior Surveillance questionnaire (Eaton et al., 2012). Having multiple partners was defined as two or more sexual partners (Eaton et al., 2012). Unprotected vaginal and anal sex was defined as engaging in these sexual acts without the use of a condom (Eaton et al., 2012). Concurrent sex was defined as vaginal or anal sex with more than one partner at the same time (group sex) or within a 1-week period (Chantala & Tabor, 1999). Exchange sex was indicated if the participant reported exchanging sex for food, money, drugs, a place to stay, or any other commodity (Eaton et al., 2012). Items related to sexual behavior from the YRBS survey have demonstrated good reliability (Brener et al., 2002).
Analysis
Descriptive analyses were conducted to examine youth demographics and characteristics. These descriptive statistics were calculated in conjunction with logistic regression, which was used to determine differences in pathways from SV to HIV risk behavior across genders. The sample was stratified by gender prior to analyses. Analyses were computed using SAS version 9.4 to examine indirect effects involving gang involvement, revictimization, IPV, binge drinking, illicit drug use, PTSD, and suicidal ideation. All outcomes and mediating variables were dichotomous. All identified mediating variables significantly associated with SV at the bivariate level using a one-tailed test (p < .10) were then tested for potential indirect effects. Analyses included direct and indirect effects for SV with all potential mediating variables and HIV risk outcomes. Significance of direct and indirect effects was determined by a two-tailed test (p < .05). The Sobel test was used to determine significant indirect effects.
Results
Sample Characteristics
In this sample of homeless youth (N = 966), ages ranged from 14 to 24 (M = 21.09, SD = 1.93). Participants most frequently self-reported being White (37.68%) or Black (23.91%). Other racial groups included Mixed (19.15%), Latino (13.35%), American Indian (2.69%), Asian (0.62%), and Native Hawaiian (0.62%). Most respondents were men (71.01%) and the majority identified as heterosexual (72.46%). In this sample, there was a relatively high prevalence of SV prior to homelessness (20.39%). Variables measuring HIV risk behavior during the previous 3 months indicated a high prevalence of risky sex behaviors, including unprotected vaginal sex (42.55%), concurrent sex (31.88%), multiple partners (19.57%), exchange sex (15.84%), and unprotected anal sex (9.52%). Table 1 presents all demographic characteristics, SV history, potential mediating variables, and outcomes assessed after stratifying the sample by gender.
Young Men
After controlling for age, race, and sexual orientation, young men who reported being sexually victimized prior to homelessness were 4.32 times (p < .001) more likely to have experienced PTSD during the previous month and 3.57 times (p < .001) more likely to have experienced suicidality during the previous year. With regard to substance use, victimized young men had 1.99 increased odds (p = .009) of using cocaine or crack, 2.38 greater odds (p < .001) of using methamphetamine, and 2.34 greater odds (p = .004) of reporting heroin use. Young men with past SV were also 1.86 times (p = .01) more likely to have engaged in IPV during the previous year. Unstandardized parameter estimates for these associations are represented in the path model in Figure 1.
Figure 1.
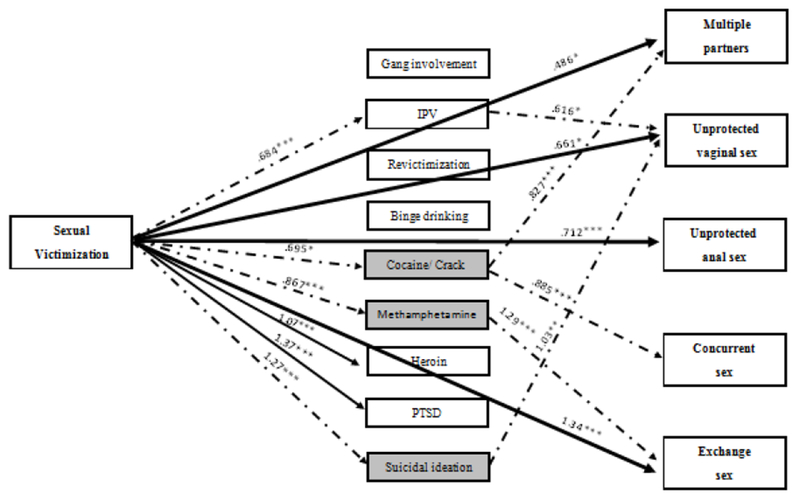
Direct and indirect effects between SV and HIV risk behaviors for male homeless youth.
Unstandardized point estimates (see corresponding odds ratios in the text) of direct associations between sexual victimization and HIV risk outcomes and indirect effects of social and emotional health outcomes among male homeless youth. Solid lines represent direct effects. Dashed lines represent mediating effects. Gray shaded boxes represent significantly mediated paths. See Table 2 for significant results determined by the Sobel test. IPV = intimate partner violence; PTSD = posttraumatic stress disorder. *p < .05; **p < .01; ***p < .001
Tests of mediation in the relationship between SV and HIV risk outcomes resulted in four significant pathways and one nonsignificant pathway (see Table 2 for Sobel test results). Young men who reported using cocaine during the previous 30 days were 1.85 times more likely to have multiple partners (p = .032) and 1.96 times more likely to engage in concurrent sex (p = .025) than non-cocaine-using male participants without past SV. Sexually victimized young men who used methamphetamine were 2.76 times more likely to report exchange sex (p < .001). SV and past-year suicidal ideation significantly increased the likelihood of engaging in unprotected vaginal sex (OR = 1.92, p = .027) among young men.
Table 2.
Sobel Test Results of Mediation Effects
| Test statistic | SE | p | |
|---|---|---|---|
| Men | |||
| Multiple partners | |||
| Cocaine use | 1.854 | 0.399 | .032 |
| Concurrent sex | |||
| Cocaine use | 1.961 | 0.438 | .025 |
| Exchange sex | |||
| Meth use | 2.757 | 0.551 | .003 |
| Unprotected vaginal sex | |||
| Suicidal ideation | 1.925 | 0.703 | .027 |
| Intimate partner violence | 1.680 | 0.250 | .092 |
| Women | |||
| Exchange sex | |||
| Posttraumatic stress disorder | 2.243 | 1.725 | .012 |
Young men who reported SV prior to homelessness were more likely to report multiple partners (OR = 1.63, p = .049), exchange sex (OR = 3.81, p < .001), unprotected vaginal sex (OR = 1.94, p = .031), and unprotected anal sex (OR = 2.37, p = .017). These relationships indicated partial mediation of cocaine or crack use on having multiple partners, methamphetamine use on exchange sex, and suicidal ideation on unprotected vaginal sex. Cocaine or crack use fully mediated the relationship between SV and concurrent sex among young men.
Young Women
Regarding emotional health outcomes, female homeless youth who reported SV were 5.36 times (p < .001) as likely to experience past-month PTSD, 3.02 times (p < .001) as likely to report suicidal ideation, and 1.85 times (p = .046) as likely to use methamphetamine than their nonvictimized female peers. For victimized young women, the odds of reporting IPV were 2.08 times (p < .01) greater compared to their nonvictimized female counterparts. Unstandardized parameter estimates for these relationships are presented in Figure 2. Female youth with past SV and PTSD were 2.24 times (p = .012) as likely to engage in exchange sex. This was the only significant mediating variable found in the model. Significant direct effects included increased odds of engaging in unprotected vaginal sex (OR = 2.32, p < .01) and concurrent sex (OR = 1.78, p = .045). PTSD fully mediated the relationship between SV and exchange sex among young women.
Figure 2.
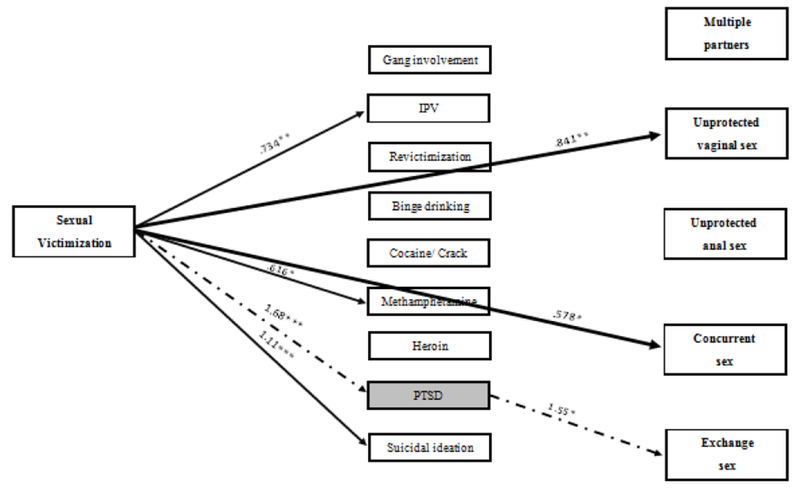
Direct and indirect effects between SV and HIV risk behaviors for female homeless youth.
Unstandardized point estimates (see corresponding odds ratios in the text) of direct associations between sexual victimization and HIV risk outcomes among female homeless youth. Solid lines represent direct effects. Significant indirect effects are indicated by dashed lines. Gray shaded boxes represent significantly mediated paths. IPV = intimate partner violence; PTSD = posttraumatic stress disorder. *p < .05; **p < .01; ***p < .001
Discussion
Homeless youth experience high rates of SV, furthered by maladaptive emotional and social experiences associated with increased risk of contracting HIV (Buffardi et al., 2008; Bailey, Camlin, & Ennett, 1998; Bensley, Van Eenwyk, & Simmons, 2000; Coker, 2007; Connell, Gilreath, & Hansen, 2009; Huock et al., 2008; Noell et al., 2001; Rice, Milburn, & Rotheram-Borus, 2007; Tyler, 2002). This study found several of these mediating variables to be significantly associated with SV among young men, including IPV, cocaine or crack use, methamphetamine use, heroin use, PTSD, and suicidal ideation. Significant pathways included cocaine or crack use to multiple partners and concurrent sex, methamphetamine use to exchange sex, and suicidal ideation to unprotected vaginal sex for young men. For young women, significant associations with SV included IPV, methamphetamine use, PTSD, and suicidal ideation. The sole indirect effect for young women occurred between PTSD and exchange sex.
We hypothesized that substance use, IPV, and suicidal ideation would have indirect effects among young men. These findings were partially supported by the trend in illicit drug use behavior and suicidal ideation as significant mechanisms increasing HIV risk outcomes. Youth with SV histories, including homeless youth, use substances at higher rates (Connell, Gilreath, & Hansen, 2009; Rew et al., 2001). Victimized youth may turn to substances as an avoidance coping mechanism for intrusive thoughts and memories related to their experience (Chawla & Ostafin, 2007; Tyler, Whitbeck, Hoyt, & Yoder, 2000). Drug and alcohol use lowers inhibitions and affects decision-making processes, leading to an increased propensity for HIV risk behavior (Solorio et al., 2008). Research has found substance-using men report increased rates of multiple partners, less frequent condom use, and exchange sex (Solorio et al., 2008). These findings confirm this pathway among male homeless youth with SV histories.
Although homeless women with SV histories tend to use drugs at higher rates than those without, among women in this sample, SV was only associated with increased use of methamphetamine. A study of female homeless adolescents found that some substances, including marijuana and methamphetamine were not significantly greater among those with SV histories compared to those without, however cocaine use was (Chen, Tyler, Whitbeck, & Hoyt, 2004). Research related to gender differences in mechanisms between trauma and substance use has indicated women’s substance use is associated with controlling impulsive behavior (Bornovalova, Ouimette, Crawford & Roy, 2009). The lack of significant associations with other substances may indicate that controlling impulsive behavior is unique to some substance use and not others for females. Other research has indicated that victimized homeless women may use substances to avoid the negative thoughts associated with traumatic thoughts and their subsequent risky sexual practices (Johnson et al., 2006; Tyler, 2002). Given that this was not the case for female homeless youth in this study, this may be explained by other research, which suggests that victimized women’s HIV risk behavior is associated with having sex while under the influence of substances (Mosack et al., 2010). It may be that female youth in this sample were less frequently engaging in risky sexual practices while under the influence, which would account for the absence of significant associations between substances and sexual risk. Further research that aims to identify the processes involved in substance using behaviors, specifically stimulant substances, for sexually victimized women may aide in enlightening these relationships and a potential path for female homeless youth.
Along with suicidal ideation, we hypothesized that PTSD, IPV, revictimization, and gang involvement would have significant indirect effects among young women. Only one of these factors had a significant mediation effect, despite similar trends in HIV risk behavior across both genders. Corresponding with related literature, female homeless youth exhibited high rates of probable PTSD associated with SV (Gwadz et al., 2007; Plotzker et al., 2007). Given it was the sole significant mediator, PTSD may be a particularly salient emotional response warranting clinical attention for female SV victims. This is in line with previous research- Plotzer and colleagues found that PTSD mediated the relationship between sexual victimization and sexual risk in a sample of female injection drug users (Plotzer, Metzger & Holmes, 2007). PTSD is a particularly debilitating clinical condition and can be long lasting (Solorio et al., 2008; Ullman & Vasquez, 2015). This may also be an indication that for these female victims, emotional responses, specifically trauma-related thoughts and behaviors, may be the primary indirect effect facilitating exchange sex.
We also hypothesized that suicidal ideation would mediate the association between SA and HIV risk behavior; however, this was only supported for young men in the sample. Disengaging coping strategies are common when an individual is suicidal, increasing sexual risk behaviors (Huock et al., 2008; Votta & Manion, 2003). Although this phenomenon has been found among both genders, some research has indicated young adult male victims are more likely than young women to experience suicidality (Tewksbury, 2007). In this sample, young men were less likely to endorse suicidality than women. This suggests that although young men may report suicidality less frequently, this symptom is especially prominent for victimized young men and subsequently increases HIV risk behavior.
A surprising aspect of these results, particularly given what previous studies have found, is the lack of statistically significant mediating relationships between social experience variables (i.e., revictimization, IPV, and gang involvement) and HIV risk behavior. For example, although the rates of revictimization were markedly high among both genders in this sample, experiencing SV prior to homelessness was not significantly associated with revictimization for either gender. This is contrary to previous literature, which has reported high rates of revictimization for individuals with early experiences of SV, especially women (Slesnick et al., 2010; Tyler, Hoyt & Whitbeck, 2000). This may indicate that there is a high prevalence of SV after becoming homeless, regardless of prior SV. Additionally, SV histories significantly increased rates of IPV among both genders. However, we identified this as a potential indirect effect only for young men in this analysis, and it was subsequently found to be statistically nonsignificant. Given the high rates of IPV reported by young men in the sample, it is unclear why this was not a significant pathway. Finally, although gang involvement has been linked to a history of SV and HIV risk behavior in previous research (Buffardi et al., 2008; Marshall et al., 2015; Rice et al., 2007), these relationships were not identified in these data. The number of individuals with gang involvement in this sample of homeless youth was rather small, with only 19 young women endorsing participation. A sample with more gang-involved youth may produce different results.
Limitations
It should be noted that there are some limitations to this study. Geographic location is a limitation because this study occurred only in specific regions of Los Angeles. These neighborhoods host and serve large numbers of homeless youth; however, findings may differ among samples elsewhere. The use of self-report measures is a limitation because it increased the likelihood of systematic bias. However, we assumed that these youth are unlikely to over report and more likely to under report given the sensitivity of information. Due to the difficulty of randomly sampling homeless youth, these data are not based on probability sampling. Due to cross-sectional data and time ordering of variables, our ability to infer causality was limited. Last, the measures used in this study generated some limitations. The National Institutes of Health guidelines define binge drinking as four or more drinks for women and five or more drinks for men (NIAAA, 2016). This study inquired about consumption of five or more drinks for both genders in accordance with the Substance Abuse and Mental Health Services Administration (NIAAA, 2016), which may have skewed results with regard to SV and binge drinking among female participants. Additionally, the survey did not include questions related to type, severity, or timing of SV, nor did it assess perpetrator information, limiting the ability to test the influence of these factors on HIV risk behavior.
Conclusion
This study investigated gender differences of mediating pathways in the relationship between SV and HIV risk behavior among homeless youth. Overall, these findings indicate a need for broad prevention efforts that address the high rates of SV and HIV risk behavior for both male and female homeless youth. Furthermore, these results warrant the acknowledgement of gender differences in these relationships in program and treatment planning. An integral component of prevention science is the incorporation of mediators to increase the identification of specific targets for intervention and practice. These findings imply a need for inclusion of maladaptive emotional health responses to SV when targeting HIV risk behavior. Minimizing risky sexual behavior among homeless young men should include efforts to identify and treat illicit drug use and suicidality. Interventions for reducing exchange sex practices among female homeless youth may benefit from including trauma treatment and trauma-informed care. Future studies would benefit from longitudinal data to determine whether these associations are in fact mechanisms that lead to increased HIV risk behavior. Additionally, future research should include more detail about the timing and duration of SV and how participants feel such experiences have affected their lives.
Acknowledgments
(The Youthnet study was supported by the National Institute of Mental Health (R01MH093336). The authors would like to thank the youth who generously shared their experiences as well as the participating organizations and study interviewers who dedicated their time and materials for the purposes of this project.)
These data draw from the Youthnet study, supported by the National Institute of Mental Health (R01MH093336).
Footnotes
Disclosure of Interest (Authors Taylor Harris, Eric Rice, Harmony Rhoades, Hailey Winetrobe, and Suzanne Wenzel declare that they have no conflicts to report.)
Ethical Standards and Informed Consent (All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation [institutional and national] and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all participants for being included in the study.)
References
- Bailey SL, Camlin CS, & Ennett ST (1998). Substance use and risky sexual behavior among homeless and runaway youth. Journal of Adolescent Health, 23, 378–388. doi: 10.1016/S1054-139X(98)00033-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnes JE, Noll JG, Putnam FW, & Trickett PK (2009). Sexual and physical revictimization among victims of severe childhood sexual abuse. Child abuse & neglect, 33(7), 412–420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bensley LS, Van Eenwyk J, & Simmons KW (2000). Self-reported childhood sexual and physical abuse and adult HIV-risk behaviors and heavy drinking. American Journal of Preventive Medicine, 18, 151–158. doi: 10.1016/S0749-3797(99)00084-7 [DOI] [PubMed] [Google Scholar]
- Bornovalova MA, Ouimette P, Crawford AV, & Levy R (2009). Testing gender effects on the mechanisms explaining the association between post-traumatic stress symptoms and substance use frequency. Addictive Behaviors, 34(8), 685–692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brener ND, Kann L, McManus T, Kinchen SA, Sundberg EC, & Ross JG (2002). Reliability of the 1999 youth risk behavior survey questionnaire. Journal of Adolescent Health, 31(4), 336–342. [DOI] [PubMed] [Google Scholar]
- Buffardi AL, Thomas KK, Holmes KK, & Manhart LE (2008). Moving upstream: Ecosocial and psychosocial correlates of sexually transmitted infections among young adults in the United States. American Journal of Public Health, 98, 1128–1136. doi: 10.2105/AJPH.2007.120451 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chantala K, & Tabor J (1999). National Longitudinal Study of Adolescent Health: Strategies to perform a design-based analysis using the Add Health data. Chapel Hill, NC: Carolina Population Center. [Google Scholar]
- Chawla N, & Ostafin B (2007). Experiential avoidance as a functional dimensional approach to psychopathology: An empirical review. Journal of clinical psychology, 63(9), 871–890. [DOI] [PubMed] [Google Scholar]
- Chen X, Tyler KA, Whitbeck LB, & Hoyt DR (2004). Early sexual abuse, street adversity, and drug use among female homeless and runaway adolescents in the Midwest. Journal of Drug Issues, 34, 1–21. doi: 10.1177/002204260403400101 [DOI] [Google Scholar]
- Coates J, & McKenzie-Mohr S (2010). Out of the frying pan, into the fire: Trauma in the lives of homeless youth prior to and during homelessness. J. Soc. & Soc. Welfare, 37, 65. [Google Scholar]
- Coker AL (2007). Does physical intimate partner violence affect sexual health? A systematic review. Trauma, Violence, & Abuse, 8, 149–177. doi: 10.1177/1524838007301162 [DOI] [PubMed] [Google Scholar]
- Connell CM, Gilreath TD, & Hansen NB (2009). A multiprocess latent class analysis of the co-occurrence of substance use and sexual risk behavior among adolescents. Journal of Studies on Alcohol and Drugs, 70(6), 943–951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Danielson CK, Macdonald A, Amstadter AB, Hanson R, de Arellano MA, Saunders BE, & Kilpatrick DG (2009). Risky behaviors and depression in conjunction with—or in the absence of—lifetime history of PTSD among sexually abused adolescents. Child maltreatment. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eaton DK, Kann L, Kinchen S, Shanklin S, Flint KH, Hawkins J, … Wechsler, H. (2012). Youth risk behavior surveillance – United States, 2011. Morbidity and Mortality Weekly Report: Surveillance Summaries, 61, 1–162. [PubMed] [Google Scholar]
- Girardet RG, Lahoti S, Howard LA, Fajman NN, Sawyer MK, Driebe EM, ... & Hammerschlag MR. (2009). Epidemiology of sexually transmitted infections in suspected child victims of sexual assault. Pediatrics, 124(1), 79–86. [DOI] [PubMed] [Google Scholar]
- Gwadz MV, Nish D, Leonard NR, & Strauss SM (2007). Gender differences in traumatic events and rates of post-traumatic stress disorder among homeless youth. Journal of Adolescence, 30, 117–129. doi: 10.1016/j.adolescence.2006.01.004 [DOI] [PubMed] [Google Scholar]
- Halcón LL, & Lifson AR (2004). Prevalence and predictors of sexual risks among homeless youth. Journal of Youth and Adolescence, 33, 71–80. doi: 10.1023/A:1027338514930 [DOI] [Google Scholar]
- Haley N, Roy E, Leclerc P, Boudreau J-F, & Boivin J-F (2004). HIV risk profile of male street youth involved in survival sex. Sexually Transmitted Infections, 80, 526–530. doi: 10.1136/sti.2004.010728 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holmes WC, Foa EB, & Sammel MD (2005). Men’s pathways to risky sexual behavior: Role of co-occurring childhood sexual abuse, posttraumatic stress disorder, and depression histories. Journal of Urban Health, 82(1), i89–i99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Houck CD, Hadley W, Lescano CM, Pugatch D, Brown LK, & Project Shield Study Group. (2008). Suicide attempt and sexual risk behavior: Relationship among adolescents. Archives of Suicide Research, 12, 39–49. doi: 10.1080/13811110701800715 [DOI] [PubMed] [Google Scholar]
- Icard LD, Jemmott JB, Teitelman A, O’Leary A, & Heeren GA (2014). Mediation effects of problem drinking and marijuana use on HIV sexual risk behaviors among childhood sexually abused South African heterosexual men. Child abuse & neglect, 38(2), 234–242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson RJ, Rew L, & Sternglanz RW (2006). The relationship between childhood sexual abuse and sexual health practices of homeless adolescents. Adolescence, 41, 221–234. [PubMed] [Google Scholar]
- Kessler RC, McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM, ... & Benjet C. (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. The British Journal of Psychiatry, 197(5), 378–385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Littleton H, Breitkopf CR, & Berenson A (2007). Sexual and physical abuse history and adult sexual risk behaviors: Relationships among women and potential mediators. Child Abuse & Neglect, 31(7), 757–768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markowitz SM, O’Cleirigh C, Hendriksen ES, Bullis JR, Stein M, & Safren SA (2011). Childhood sexual abuse and health risk behaviors in patients with HIV and a history of injection drug use. AIDS and Behavior, 15(7), 1554–1560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall BDL, DeBeck K, Simo A, Kerr T, & Wood E (2015). Gang involvement among street-involved youth in a Canadian setting: A gender-based analysis. Public Health, 129, 74–77. doi: 10.1016/j.puhe.2014.10.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martijn C, & Sharpe L (2006). Pathways to youth homelessness. Social Science & Medicine, 62, 1–12. doi: 10.1016/j.socscimed.2005.05.007 [DOI] [PubMed] [Google Scholar]
- May A, & Klonsky ED (2011) Validity of suicidality items from the Youth Risk Behavior Survey in a high school sample. Assessment, 18, 379–381. doi: 10.1177/1073191110374285 [DOI] [PubMed] [Google Scholar]
- Melander LA, & Tyler KA (2010). The effect of early maltreatment, victimization, and partner violence on HIV risk behavior among homeless young adults. Journal of Adolescent Health, 47, 575–581. doi: 10.1016/j.jadohealth.2010.04.010 [DOI] [PubMed] [Google Scholar]
- Miller M (1999). A model to explain the relationship between sexual abuse and HIV risk among women. AIDS Care, 11, 3–20. doi: 10.1080/09540129948162 [DOI] [PubMed] [Google Scholar]
- Molnar BE, Shade SB, Kral AH, Booth RE, & Watters JK (1998). Suicidal behavior and sexual/physical abuse among street youth. Child Abuse & Neglect, 22, 213–222. doi: 10.1016/S0145-2134(97)00137-3 [DOI] [PubMed] [Google Scholar]
- Mosack KE, Randolph ME, Dickson-Gomez J, Abbott M, Smith E, & Weeks MR (2010). Sexual risk-taking among high-risk urban women with and without histories of childhood sexual abuse: mediating effects of contextual factors. Journal of child sexual abuse, 19(1), 43–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism (NIAAA) (2016). Drinking levels defined. Retrieved from https://www-niaaa-nih-gov.libproxy2.usc.edu/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking
- Noell J, Rohde P, Seeley J, & Ochs L (2001). Childhood sexual abuse, adolescent sexual coercion and sexually transmitted infection acquisition among homeless female adolescents. Child Abuse & Neglect, 25, 137–148. doi: 10.1016/S0145-2134(00)00223-4 [DOI] [PubMed] [Google Scholar]
- Northcott M (2010). Factors Mediating the Relations between Street Youths’ Experiences of Trauma and their HIV Risk Behaviour (Doctoral dissertation, Carleton University; ). [Google Scholar]
- O’leary A, Purcell D, Remien RH, & Gomez C (2003). Childhood sexual abuse and sexual transmission risk behaviour among HIV-positive men who have sex with men. AIDS care, 15(1), 17–26. [DOI] [PubMed] [Google Scholar]
- Olshen E, McVeigh KH, Wunsch-Hitzig RA, & Rickert VI (2007). Dating violence, sexual assault, and suicide attempts among urban teenagers. Archives of Pediatrics & Adolescent Medicine, 161, 539–545. doi: 10.1001/archpedi.161.6.539 [DOI] [PubMed] [Google Scholar]
- Paul JP, Catania J, Pollack L, & Stall R (2001). Understanding childhood sexual abuse as a predictor of sexual risk-taking among men who have sex with men: The Urban Men’s Health Study☆. Child abuse & neglect, 25(4), 557–584. [DOI] [PubMed] [Google Scholar]
- Plotzker RE, Metzger DS, & Holmes WC (2007). Childhood sexual and physical abuse histories, PTSD, depression, and HIV risk outcomes in women injection drug users: A potential mediating pathway. American Journal on Addictions, 16, 431–438. doi: 10.1080/10550490701643161 [DOI] [PubMed] [Google Scholar]
- Prins A, Ouimette P, Kimerling P, Cameron RP, Hugelshofer RS, Shaw-Hegwer D, … Sheikh J. I (2003). The Primary Care PTSD screen (PC-PTSD): Development and operating characteristics. Primary Care Psychiatry, 9, 9–14. [Google Scholar]
- Pynoos R, Rodriguez N, Steinberg A, Stuber M, & Frederick C (1998). The University of California at Los Angeles Posttraumatic Stress Disorder Reaction Index (UCLA-PTSD RI) for DSM-IV (Revision 1). Los Angeles, CA: UCLA Trauma Psychiatry Program. [Google Scholar]
- Rew L, Taylor-Seehafer M, & Fitzgerald ML (2001). Sexual abuse, alcohol and other drug use, and suicidal behaviors in homeless adolescents. Issues in Comprehensive Pediatric Nursing, 24, 225–240. doi: 10.1080/014608601753260326 [DOI] [PubMed] [Google Scholar]
- Reynolds MW, Peipert JF, & Collins B (2000). Epidemiologic issues of sexually transmitted diseases in sexual assault victims. Obstetrical & Gynecological Survey, 55, 51. doi: 10.1097/00006254-200001000-00023 [DOI] [PubMed] [Google Scholar]
- Rice E, Milburn NG, & Rotheram-Borus MJ (2007). Pro-social and problematic social network influences on HIV/AIDS risk behaviours among newly homeless youth in Los Angeles. AIDS Care, 19, 697–704. doi: 10.1080/09540120601087038 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Senn TE, Carey MP, & Vanable PA (2008). Childhood and adolescent sexual abuse and subsequent sexual risk behavior: Evidence from controlled studies, methodological critique, and suggestions for research. Clinical Psychology Review, 28, 711–735. doi: 10.1016/j.cpr.2007.10.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Senn TE, Carey MP, Vanable PA, Coury-Doniger P, & Urban M (2007). Characteristics of sexual abuse in childhood and adolescence influence sexual risk behavior in adulthood. Archives of Sexual Behavior, 36, 637–645. doi: 10.1007/s10508-006-9109-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simpson TL, & Miller WR (2002). Concomitance between childhood sexual and physical abuse and substance use problems: A review. Clinical Psychology Review, 22, 27–77. doi: 10.1016/S0272-7358(00)00088-X [DOI] [PubMed] [Google Scholar]
- Slesnick N, Erdem G, Collins J, Patton R, & Buettner C (2010). Prevalence of intimate partner violence reported by homeless youth in Columbus, Ohio. Journal of Interpersonal Violence, 25, 1579–1593. doi: 10.1177/0886260509354590 [DOI] [PubMed] [Google Scholar]
- Solorio MR, Rosenthal D, Milburn NG, Weiss RE, Batterham PJ, Gandara M, & Rotheram-Borus MJ (2008). Predictors of sexual risk behaviors among newly homeless youth: A longitudinal study. Journal of Adolescent Health, 42, 401–409. doi: 10.1016/j.jadohealth.2007.09.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg AM, Brymer MJ, Decker KB, & Pynoos RS (2004). The University of California at Los Angeles post-traumatic stress disorder reaction index. Current psychiatry reports, 6(2), 96–100. [DOI] [PubMed] [Google Scholar]
- Straus MA, Hamby SL, Boney-McCoy S, & Sugarman DB (1996). The revised Conflict Tactics Scales (CTS2): Development and preliminary psychometric data. Journal of Family Issues, 17, 283–316. doi: 10.1177/019251396017003001 [DOI] [Google Scholar]
- Sutherland MA (2011). Examining mediators of child sexual abuse and sexually transmitted infections. Nursing research, 60(2), 139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tewksbury R (2007). Effects of sexual assaults on men: Physical, mental and sexual consequences. International Journal of Men’s Health, 6, 22–35. doi: 10.3149/jmh.0601.22 [DOI] [Google Scholar]
- Tyler KA (2002). Social and emotional outcomes of childhood sexual abuse: A review of recent research. Aggression and Violent Behavior, 7, 567–589. doi: 10.1016/S1359-1789(01)00047-7 [DOI] [Google Scholar]
- Tyler KA, Hoyt DR, & Whitbeck LB (2000). The effects of early sexual abuse on later sexual victimization among female homeless and runaway adolescents. Journal of Interpersonal Violence, 15, 235–250. doi: 10.1177/088626000015003001 [DOI] [Google Scholar]
- Tyler KA, Hoyt DR, Whitbeck LB, & Cauce AM (2001). The impact of childhood sexual abuse on later sexual victimization among runaway youth. Journal of Research on Adolescence, 11, 151–176. doi: 10.1111/1532-7795.00008 [DOI] [Google Scholar]
- Tyler KA, Whitbeck LB, Hoyt DR, & Yoder KA (2000). Predictors of self-reported sexually transmitted diseases among homeless and runaway adolescents. Journal of Sex Research, 37, 369–377. doi: 10.1080/00224490009552060 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ullman SE, & Vasquez AL (2015). Mediators of sexual revictimization risk in adult sexual assault victims. Journal of Child Sexual Abuse, 24, 300–314. doi: 10.1080/10538712.2015.1006748 [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services (2009). Report to congress on the runaway and homeless youth programs of the family and youth services bureau for fiscal years 2008 and 2009. Retrieved 22 August 2011, from http://www.acf.hhs.gov/programs/fysb/content/docs/508-fysbcongress-0809.pdf
- Votta E, & Manion IG (2003). Factors in the psychological adjustment of homeless adolescent males: The role of coping style. Journal of the American Academy of Child & Adolescent Psychiatry, 42, 778–785. doi: 10.1097/01.CHI.0000046871.56865.D9 [DOI] [PubMed] [Google Scholar]
- Wilson DR (2010). Health consequences of childhood sexual abuse. Perspectives in psychiatric care, 46(1), 56–64. [DOI] [PubMed] [Google Scholar]
- Wilson HW, & Widom CS (2008). An examination of risky sexual behavior and HIV in victims of child abuse and neglect: a 30-year follow-up. Health Psychology, 27(2), 149. [DOI] [PubMed] [Google Scholar]
- Zerger S, Strehlow AJ, & Gundlapalli AV (2008). Homeless young adults and behavioral health an overview. American behavioral scientist, 51(6), 824–841. [Google Scholar]
- Zierler S, Feingold L, Laufer D, Velentgas P, Kantrowitz-Gordon I, & Mayer K (1991). Adult survivors of childhood sexual abuse and subsequent risk of HIV infection. American Journal of Public Health, 81, 572–575. doi: 10.2105/AJPH.81.5.572 [DOI] [PMC free article] [PubMed] [Google Scholar]