

Abstract
Objective:
Emergency management and operations (EMO) personnel require up-to-date information to make informed decisions during natural and man-made disasters. However, information gaps present challenges for accessing human health risk assessment and risk management strategies for dermal exposure. This article describes the development of a decision support system, the Dermal Exposure Risk Management and Logic (DERMaL) eToolkit.
Design:
The DERMaL eToolkit provides information on key resources used in emergency incidents. Resources were classified according to response phase, resource categories, and information category and evaluated on reliability, accessibility, and preference by subject matter experts in emergency management fields. These rankings were used to generate a value of information score, unique for each resource, which aids in developing reference lists for users during each incident phase.
Results:
This tool will identify and prioritize information resources on dermal risks, and can readily find the most relevant information to suit EMO needs.
Conclusion:
The DERMaL eToolkit can be used as an aid in finding information resources targeted to scenario-driven needs by providing well-vetted and prioritized resources related to dermal hazards, exposure, and risk assessments for EMO.
Keywords: dermal, risk management, emergency management, emergency response, decision support system
INTRODUCTION
Emergency management and operations (EMO) personnel require timely and up-to-date information to make informed decisions during both natural and man-made disasters. Much of the guidance for the EMO community is hazard based. There are dermal risk assessment guidance documents available from the US Environmental Protection Agency (USEPA) and other agencies,1,2 and this guidance may be applied to multiple scenarios and emergency incidents. Figure 1 illustrates the top-down model for guidance for EMO, where the majority of information and guidance identified can be applied to any incident,3,4 followed by information on specific scenarios (man-made or natural disasters),5–9 hazard type,7,11–17 and the domain (environmental, occupational, and community).16,18–21 For example, the Federal Emergency Management Agency (FEMA) created the National Incident Management System and Incident Command System to provide a comprehensive national approach to incident management.3,4 Initiatives managed by the National Library of Medicine (NLM), Centers for Disease Control and Prevention (CDC), and the USEPA are designed to serve as resources applicable to specific scenarios (ie, transportation incidents, industrial accidents, and terrorist attacks) or hazards (ie, chemicals, radiation, and biological agents).5,23–25 Despite availability of such information, detailed resources geared to specific hazards (chemical, biological, radiological, nuclear, environmental, and psychological stressors),16 or routes of exposure1,22,23 continue to be needed.
Figure 1.

Information model on EMO guidance.
The top-down model of guidance for EMO personnel. Much of the information is broad in scope (ie, incident, scenario, and domain) and hazard specific, and narrows down to route of exposure.
There are limited data on the contribution of dermal uptake in risk assessment and risk management strategies. Risk assessment characterizes risk associated with a specific hazard, and risk management focuses on the application of these findings to make decisions to control the risk.26 Information gaps in human health risk assessment and risk management strategies for the dermal route of exposure may result in significant health risks during chemical incidents.27 For example, responders or other EMO personnel may be exposed to chemicals via spills, contact with contaminated materials, or off gassing or vapors absorbed by the skin and may not have the information needed to address such exposures.28–30 The traditional focus in occupational risk assessment on inhalation exposures does not fully address first responders’ needs. This gap could cause responders and the public to be vulnerable to chemical threats that can elicit toxicological responses through skin contact. For example, a common hazard assessment resource, such as the qualitative skin hazard notation, as documented in resources such as skin notation profiles1 is available for only a limited number of chemicals. Dermal contact is often perceived to be a secondary exposure route; however, this route may present significant health risks during a chemical incident.29,31 The potential for dermal exposures during EMO necessitates a systematic approach designed to collect, organize and process relevant data that can be readily applied during chemical emergencies involving dermal exposures.32
The purpose of this article is to describe the development of the Dermal Exposure Risk Management and Logic (DERMaL) eToolkit (https://dermal.nlm.nih.gov/) based on the decision support system (DSS) described in Dotson et al.32 This effort was initiated and led by the National Institute for Occupational Safety and Health (NIOSH), an Institute of the CDC. The DERMaL eToolkit provides information on key resources that can be used in any emergency incident. It addresses the need of EMO personnel for information such as selection of appropriate chemical protective clothing (CPC), decontamination, medical counter treatments, and symptoms diagnosis. The DERMaL eToolkit is currently hosted and supported by the NLM. Other tools that are available for EMO that provide critical decision-making information during mass casualty events include the NLM’s Chemical Hazards Emergency Medical Management (CHEMM) and Wireless Information System for Emergency Responders (WISER),25,33 and the USEPA Computer-Aided Management of Emergency Operations.34 The DERMaL eToolkit supplements such resources by providing dermal-specific information for EMO activities.
METHODS
Conceptual model
Dotson et al.32 outlined a DSS for characterizing dermal exposure during EMO. The outlined DSS facilitates dynamic decision making during the life cycle of an emergency incident (ie, preparedness, response, and recovery) and comprises two modules: (1) resource compilation and (2) prioritization. Figure 2 illustrates the primary components (ie, scenario planning, risk assessment and risk management, and multicriteria decision analysis [MCDA]) of the DSS as applied in EMO. For each component, numerous elements are included to aid users in identifying critical considerations that will affect the overall incident management.
Figure 2.

Primary components of a DSS.
aThe DSS incorporates different components, so that the tool is versatile and can be used in any phase of an incident where there is potential for dermal exposure to chemicals. The DSS assists in characterizing and managing risk during chemical emergencies involving dermal exposures and uses the three principles of (1) scenario planning, (2) MCDA, and (3) risk assessment and management strategies.
bScenario planning is commonly done by using a narrative to depict a possible future. This strategy manages uncertainties in the future, and can be used to evaluate alternative strategies when there are multiple scenarios.
cMCDA is a method applied to understand complicated decisions and assists in choosing among alternatives via systematic analyses of risk levels, uncertainty, and valuation based on multiple criteria.
dRisk assessment characterizes risk associated with a specific hazard, and risk management focuses on the application of these findings to make decisions and policies to control the risk.
The DSS combines scenario planning, MCDA, and risk analysis and provides the architecture for these key elements to be included in the tool so that EMO personnel may utilize the dermal risk resources based on their needs.
Scenario planning has been described as the part of the strategic planning methods that manages uncertainties in the future by using various tools and technologies,35,36 and may also be used to evaluate alternative strategies when there are multiple scenarios.37 Using narratives to depict a plausible future is how scenario planning is most commonly depicted37; however, the DERMaL eToolkit simplifies this process by using three scenario options (eg, preparedness, response, and recovery) that mirror the capabilities in the mission areas in an emergency response identified by the National Preparedness Goal.38 For example, the preparedness scenario addresses needs for the prevention, protection, and mitigation mission areas, the response scenario addresses needs for the response mission area, and the recovery scenario addresses needs for the recovery mission areas. This results in a tool that is versatile and can be used in the five mission areas, as described by FEMA, of an incident where there is potential for dermal exposure to chemicals.
Risk assessment has been effective in evaluating public health and environmental concerns for most public health agencies and organizations.26 In response to decision-making challenges, risk assessment has been paired with MCDA to form a comprehensive framework for environmental management.39 MCDA provides a method to help evaluate alternatives using systematic analysis that integrates risk levels, uncertainty, and valuation,39 and has been successfully used for emerging environmental threats40 and can be used in strategic planning.41·42
Literature review (resource compilation)
To build the comprehensive database for the DERMaL eToolkit, resources were identified, collected, and organized by (1) incident phase, (2) information categories, and (3) resource types. The literature review comprised several database searches, including Doody’s Core Titles, Worldcat, NLM’s LocatorPlus, google scholar, and governmental databases such as the Hazardous Substance Data Bank, NIOSHTIC-2 publications search, and the National Technical Information Service. Peer-reviewed articles from databases such as PubMed were excluded since they were beyond the scope of the eToolkit. Search terms used included:
-
▪
dermal OR skin AND personal protective equipment;
-
▪
dermal OR skin AND emergency responder;
-
▪
dermal OR skin AND hazmat;
-
▪
dermal OR skin AND first responder; and
-
▪
dermal OR skin AND ppe.
The identified resources were compiled in an Microsoft Excel™ spreadsheet for review by three subject matter experts (SMEs), two reviewers were from NIOSH and one reviewer was from the University of Cincinnati. The resources were reviewed for relevancy and content. Resources were removed from the list if there was a newer edition or version of that resource or if the resource was not relevant to dermal exposure. In addition, new resources were added if identified by the literature review team or other SMEs. This effort yielded a final list that comprise 164 resources listed in the Appendix of Dotson et al.32 Each of the resources was “tagged” with information regarding the scenario for which the resource would be of most use (preparedness, response, and recovery), information category (ie, health effects, exposure assessment, exposure control measures, and medical management), and resource type (ie, government document, reference or textbook, on-line resource, and databases).
Value of information scoring (prioritization)
For the DSS, the method to evaluate alternatives is a value of information (VOI) score. Each of the resources in the DERMaL eToolkit was evaluated on reliability, accessibility, and preference, which is a measurement based on personal use. Each of the 164 individual resources in the DERMaL eToolkit was assigned a VOI score, which facilitated prioritization of the resources based on EMO needs.
Additional SMEs with a breadth of expertise in EMO were recruited to rate the resources in the DERMaL eToolkit resource library. Each resource was reviewed and rated by up to 15 SMEs. Professional disciplines for SMEs included certified industrial hygienists, toxicologists, HAZMAT specialists, physicians, fire fighters, national laboratories, and law enforcement officials from local, state organizations, and federal organizations. The SMEs ranked each resource from the literature review with a value from 1 to 5 (with 1 being the lowest and 5 being the highest scores) for three qualities including:
Quality defined as the level of value to the EMO audience;
Accessibility defined as the level of ease to obtain or refer to the resource; and
Preference defined as the level of personal use or something the SME viewed as essential.
These criteria are more fully explained in Dotson et al.32 Application of the VOI scores in the DSS ensures that prioritization of information resources is based on critical needs of EMO personnel.
The crude VOI can be determined by calculating the average of ratings for quality, accessibility, and preference. The overall prioritization process can be further refined to address specific user needs by customizing the weights of the different criteria and factors. To provide a dynamic range in the process, modifying factors were included to further refine resource prioritization. Table 1 depicts how the algorithm would work for a range of resources receiving quality, availability, and preference scores from 1 to 5 for the response and recovery scenarios. The final VOI scores based on SME rankings were determined using the following formula:
where VOI, Value of Information; Q, Quality; A, Accessibility; P, Preference; M, level of detail.
Table 1.
Sample VOI resource scoring used in the DERMaL eToolkit
| Resource | Tester 1 | Tester 2 | Tester 3 | Tester 4 | Level of detail (1-3)* | Mean scores (>1 phase) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q | A | P | Q | A | P | Q | A | P | Q | A | P | Q | A | P | Crude VOI | VOI† | ||
| 1 | 5 | 4 | 5 | 5 | 4 | 5 | 5 | 4 | 5 | 5 | 4 | 5 | 3 | 5.00 | 4.00 | 5.00 | 4.667 | 5.83 |
| 2 | 4 | 5 | 5 | 4 | 5 | 5 | 4 | 5 | 5 | 4 | 5 | 5 | 2 | 4.00 | 5.00 | 5.00 | 4.667 | 4.67 |
| 3 | 4 | 2 | 3 | 4 | 2 | 4 | 5 | 1 | 3 | 5 | 2 | 2 | 3 | 4.50 | 1.75 | 3.00 | 3.083 | 3.85 |
| 4 | 4 | 4 | 2 | 4 | 4 | 4 | 5 | 3 | 4 | 5 | 4 | 3 | 2 | 4.5 | 3.75 | 3.25 | 3.833 | 3.83 |
| 5 | 5 | 2 | 2 | 5 | 2 | 2 | 5 | 2 | 2 | 5 | 2 | 2 | 3 | 5.00 | 2.00 | 2.00 | 3.000 | 3.75 |
| 6 | 5 | 5 | 4 | 5 | 4 | 5 | 4 | 5 | 5 | 5 | 5 | 5 | 1 | 4.75 | 4.75 | 4.75 | 4.75 | 3.56 |
| 7 | 3 | 4 | 3 | 3 | 4 | 3 | 3 | 4 | 3 | 3 | 4 | 3 | 2 | 3.00 | 4.00 | 3.00 | 3.333 | 3.33 |
| 8 | 4 | 4 | 4 | 4 | 3 | 5 | 5 | 4 | 4 | 3 | 2 | 2 | 1 | 4.00 | 3.25 | 3.75 | 3.667 | 2.75 |
| 9 | 3 | 4 | 3 | 4 | 3 | 3 | 2 | 3 | 3 | 3 | 4 | 3 | 1 | 3.00 | 3.50 | 3.00 | 3.167 | 2.38 |
| 10 | 3 | 3 | 2 | 3 | 3 | 3 | 2 | 4 | 2 | 2 | 3 | 2 | 1 | 2.50 | 3.25 | 2.25 | 2.667 | 2.00 |
Abbreviations: Q, Quality; A, Accessibility; P, Preference among SMEs.
The detail (comprehensiveness) of a resource. The value assigned to the scoring is as follows: 1 = −0.25, 2 = 0, and 3 = 0.25.
VOI = (Q + A + P)/3 + [(Q + A + P)/3] × M, where VOI, Value of Information; Q, Quality; A, Accessibility; P Preference; M, level of detail.
The modifying factor (M) in the DERMaL eToolkit is the level of detail in a resource. Each resource was assigned a categorical score of 1-3, where a score of 1 indicated the resource had minimal detail and a score of 3 had detailed information that would be most useful to EMO personnel. The value assigned to the scoring is as follows: a score of 1 was assigned −0.25, a score of 2 was assigned 0, and a score of 3 was assigned +0.25. As such, sources that do not have detailed comprehensive information or which may only contain links to other resources would receive a score of 1 (valued at −0.25) whereas a comprehensive and detailed source would receive a score of 3 (valued at +0.25).
Programming
The DERMaL eToolkit is a Web-based application that communicates with a structured query language database. It was developed using asp.net 4.5, entity framework 6, and model-view-controller architecture. The code for the DERMaL eToolkit was written in C# and uses standard window membership role-based security. The Web site was created using responsive design, so that the eToolkit has easy reading and navigation with minimum resizing, panning, and scrolling across a range of devices including personal computers, tablets, and smart phones.
RESULTS: APPLICATION AND OVERVIEW OF TOOL
The DERMaL eToolkit is organized by (1) scenario, (2) information categories, and (3) resource types. By doing so, EMO personnel can readily find the most relevant information to suit their needs. To demonstrate the use of the DERMaL eToolkit, one of the case studies from Dotson et al.32 is highlighted. In this scenario, an uncontrolled release of benzene (CAS# 71-43-2) from a tanker truck occurs arising from a traffic accident. The responding EMO personnel note that dermal exposure may occur via contact with the spilled benzene liquid and vapor emissions and are concerned about appropriate CPC. Figure 3 displays the homepage of the DERMaL eToolkit. On this page, the responder would select the “hot button” PPE from the response phase, depicted in Figure 3, box A. The buttons for the response phase stand out so that they are easily differentiated from the preparedness and recovery phase buttons for use of the eToolkit under highly stressful conditions. The “hot buttons” were chosen for the response phase because searches related to PPE, DECON, and health information were determined to be the most likely to be used during the response phase. Other tools on the homepage that could be utilized include a dermal checklist for assessing risks during response activities, as shown in Figure 3 box B, adapted from Dotson et al.32 A link to open CHEMM-IST, a decision tool developed by the US Department of Health and Human Services for the rapid identification of possible chemical exposures and syndromes, is also included on the DERMaL homepage, as shown in Figure 3 box C.
Figure 3.

Homepage of the DERMaL eToolkit.
This figure displays the DERMaL eToolkit homepage. Box A displays the “hot buttons” for the response phase, and boxes B (a dermal checklist for assessing risk during response activities) and C (a link to CHEMMIST, a decision tool for the rapid identification of possible chemical exposures and syndromes) highlight different resources that can be used during an emergency response.
Figure 4 displays the search results for the response phase PPE hot button. The search can also be edited on this page by selecting from drop down menus for incident phase, information category, and resource. More than one item can be selected in each search box. Additionally, if there is a specific resource(s) the responder needs, the responder can find the resource(s) by typing a key word or phrase in the Word or Phrase box. For example, the responder may narrow the search by entering “WISER” or “Pocket Guide” in the word or phrase box.
Figure 4.

Search results for PPE in the response phase of the DERMaL eToolkit.
This figure displays the search results for the DERMaL eToolkit response PPE hot button. Different features on the search page includes the ability to customize what information is available (box D), the export function (box E), the resource link (box F), the contextual web search (box H), and the VOI scores, titled Relevance (box I).
The level of information displayed on the search page is customizable. In the default view of the DERMaL eToolkit, the responder will be able to select the link for the resource in a new window or tab and view the title, description, and relevance. In the DERMaL eToolkit, there are several options for customizing visual display of information. By selecting the “Select column” button displayed in Figure 4 box D, the responder will be able to customize the information display. The available selections are shown in Figure 5.
Figure 5.

DERMaL viewer customizability.
This figure depicts the customizability options for the search page display in the DERMaL eToolkit when “Select Columns” is selected.
The DERMaL eToolkit search may be exported into an Excel table by clicking the “Export Table” button in Figure 4 box E, so that the responder may review the resources later if needed. The Excel table includes information such as the Resource ID, Resource, Description, Source, Date, URL, phases, and categories. The exported file is shown in Figure 6.
Figure 6.

DERMaL resource export.
This figure depicts data exported to excel when using the export function of the DERMaL eToolkit. The Excel database contains comprehensive information for each resource, including the VOI scores, phases, and categories.
In this scenario, the search contained resources that the responder would find useful. More specifically, the responder chose the NIOSH Emergency Response Safety and Health (ERSH) database. By clicking the button in Figures 4 and 7, box F, the responder is able to go to the resource page (Figure 7), which contains a variety of information including the description, resource type, source, and the review date. If the responder decides to continue with this resource, selecting box G in Figure 7 will direct the responder to the ERSH home page where information on PPE can be obtained.
Figure 7.

DERMaL resource page.
This image displays the resource page of the DERMaL eToolkit once it has been selected from the search results, and how to navigate to the homepage of the resource. In this example, the resource is the NIOSH ERSH database.
If the information that the responder is not contained within the DERMaL eToolkit, the Google search displayed in Figure 4 box H on the results page of the DERMaL eToolkit provides a contextual Web search that can be used to conduct a predefined Google search such that the most relevant resources will be at the top of the Google search page (Figure 8). In this example, the top items in the predefined search included the “HAZWOPER 40 HR Manual—Environmental Response Training” and the “Personal Protective Equipment Guide for Military Medical Treatment Facility Personnel Handling Casualties from Weapons of Mass Destruction and Terrorism Events.” Additionally, once the contextual Web search has been performed, the responder is able to edit the search field to further explore by including additional terms (ie, chemical name) or removing terms already populating the search box. For example, entering the term “benzene” to the Google search depicted in Figure 8 yielded “OSHA Technical Manual (TM) Section II: Chapter 2 Surface Contaminants, Skin Exposure, Biological Monitoring and Other Analyses” (https://www.osha.gov/dts/osta/otm/otm_ii/otm_ii_2.html) and “Occupational Safety and Health Administration Chemical Sampling Information: Benzene” (https://www.osha.gov/dts/chemicalsampling/data/CH_220100.html). Further modification of the search terms to “benzene skin dermal chemical exposure” yielded “ATSDR- Medical Management Guidelines (MMGs): Benzene” (https://www.atsdr.cdc.gov/mmg/mmg.asp?id=35&tid=14).
Figure 8.
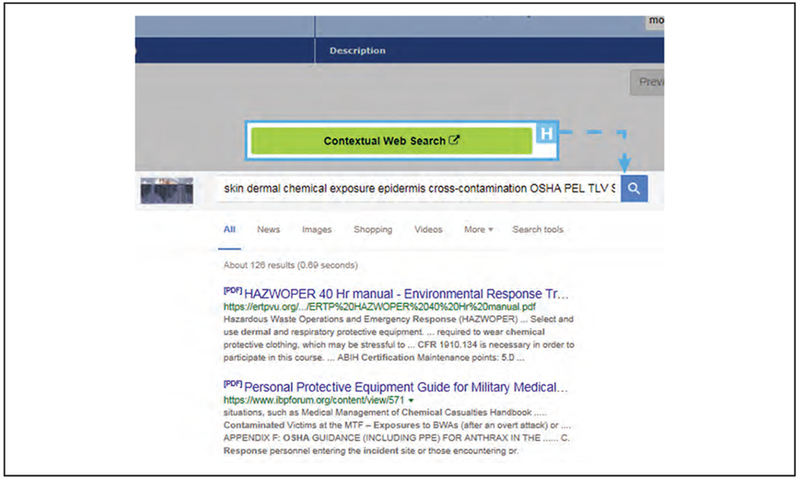
DERMaL predefined contextual Google Web search.
This image displays the contextual Web search option used to conduct a predefined Google search so that the most relevant resources will be at the top of the Google search page. This contextual Web search was created using the DERMaL eToolkit search for PPE in the response phase of an emergency event.
The relevance score, as depicted in Figure 4 (I) on the DERMaL results page, uses the VOI scoring and algorithm described in the methods. The VOI determines the relevance of the resource to the specific search initiated by the responder. The first five resources have the same relevance/shading, and each would be a good resource for the responder to select for information on PPE. These results include the NIOSH Pocket Guide search page, the NIOSH ERSH Database, the Emergency Response Guidebook and mobile app, and OSHA’s occupational chemical database. The brief description included in the default view Figure 4 should assist the responder in determining which resource to utilize.
DISCUSSION
This article describes the design and intended uses of a Web-based tool to support information needs related to making decisions regarding dermal exposure to, and potential health risks associated with, chemical hazards for EMO. The DERMaL eToolkit was developed by NIOSH/CDC and is hosted as an on-line resource by the NLM and is included in the CHEMM Resource page (https://chemm.nlm.nih.gov). The eToolkit is expected to provide immediate utility for identifying and prioritizing information resources on dermal hazards and risks. The use of a systematic and SME-driven process to identify and catalog resources improves the likelihood that EMO decision makers will identify the most useful information. Key features of the eToolkit designed to improve its impact include:
-
▪
provision of well-vetted and prioritized resources related to dermal hazards, exposure, and risk assessments for EMO;
-
▪
addition of a supplemental optimized Google search feature to enhance resources with evergreen on-line content that can add chemical-specific searching ability; and
-
▪
linkage to other user tools for EMO, including the dermal risk assessment checklist tool and the CHEM-IST tools for toxidrome-based chemical identification.
The DERMaL eToolkit in its current form is intended primarily to aid the technical specialist in EMO in finding information resources targeted to scenario-driven needs. One challenge faced in developing the eToolkit was the absence of a ready mechanism to include chemical specificity in the top layer of the output. This limitation is due in part to the fact that many of the most valuable resources are books or databases that have individual chapters or dedicated pages to chemical-specific information that are not individually electronically tagged with a chemical-specific keyword. These resources were included in the eToolkit as the whole resource, and not individual chapter or page content. To offset this limitation, the eToolkit resource output is also supplemented with an optimized Google search that can be modified to include chemical-specific terms. A second limitation of the eToolkit is that it pulls from a dedicated bibliography of vetted resources. While the publication of new dermal hazard and risk-related resources will likely occur at a slow pace, a mechanism to maintain the eToolkit with current content is required.
The DERMaL eToolkit has potential to provide decision support to inform EMO relating to dermal hazards. Figure 9 is modified from Dotson et al.32 and extended to show module 3 of the DERMaL eToolkit. In this figure, module 1 is the resource compilation and module 2 is data integration. The current configuration of the DERMaL eToolkit meets the intent of modules for problem formulation, resource identification, and prioritization. A future design goal is to narrow the output of the DERMaL eToolkit such that it can be used as a decision assist tool. In this case, module 3 would represent a potential decision analysis approach using weight of evidence methods. This module would use both qualitative and quantitative information on dermal risks to support risk management strategies and other EMO needs to answer questions such as: “Which glove material is best for an exposure scenario?” “What medical management is needed?” And “What are the appropriate decontamination procedures?” To be able to arrive at these decisions, the module first must consider the problem formulation (ie, PPE, decontamination, and medical management). Much like the prioritization module, the response phase, resource type, and information category are taken into consideration. However, in module 3, the information is integrated to give an assessment to support the decision based on a set of predetermined SME answers. Developing expert rules to enable module 3 will identify data gaps, such that future studies can focus on filling these knowledge gaps and provide actionable information for the EMO community.
Figure 9.

Future module for the DERMaL eToolkit.
This image illustrates the conceptual framework to expand the DERMaL eToolkit by including a decision module. The decision module integrates information using a weight of evidence approach and gives a qualitative or quantitative assessment to support the decision (ie, what are the appropriate decontamination procedures, what medical management is needed).
ACKNOWLEDGEMENTS
The authors would like to acknowledge the contributions of Dr. Pertti (Bert) Hakkinen, PhD, F-SRA (National Library of Medicine, Office of Clinical Toxicology Specialized Information Services) and Florence Chang (National Library of Medicine, Office of Clinical Toxicology Specialized Information Services) for their critical review of the manuscript and support for the DERMaL eToolkit to be included in the CHEMM Web page (https://chemm.nlm.nih.gov). We would also like to thank Eileen S. Haag, Jud Waters, and Bobby Ortiz at Oak Ridge Associated Universities (ORAU) for the preparation of the DERMaL eToolkit through an interagency agreement between NIOSH/CDC and the US Department of Energy (DOE). Funding: Financial support for this study was provided via an intramural grant from the Centers for Disease Control and Prevention Office of Public Health Preparedness and Response. Disclaimer: The findings and conclusion of this report are those of the authors and do not necessarily represent the views of the National Institute for Occupational Safety and Health.
Contributor Information
Naomi L. Hudson, Education and Information Division (EID), Centers for Disease Control and Prevention (CDC), National Institute for Occupational Safety and Health (NIOSH), Cincinnati, Ohio.
G. Scott Dotson, Education and Information Division (EID), Centers for Disease Control and Prevention (CDC), National Institute for Occupational Safety and Health (NIOSH), Cincinnati, Ohio.
A. Maier, Department of Environmental Health, College of Medicine, University of Cincinnati, Cincinnati, Ohio.
REFERENCES
- 1.NIOSH: Current Intelligence Bulletin 61: A Strategy for Assigning New NIOSH Skin Notations. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, 2009. [Google Scholar]
- 2.USEPA: Dermal expsoure assessment: A summary of EPA approaches. Available at https://ofmpub.epa.gov/eims/eimscomm.getfile?p_download_id=469581 Accessed March 2, 2018.
- 3.FEMA: National Incident Management System. Washington, DC: Department of Homeland Security, Federal Emergency Management Agency; 2018. Available at https://www.fema.gov/national-incident-management-system Accessed March 2, 2018. [Google Scholar]
- 4.FEMA: Incident Command System Resources. Washington, DC: Department of Homeland Security, Federal Emergency Management Agency; 2018. Available at https://www.fema.gov/incident-command-system-resources Accessed March 2, 2018. [Google Scholar]
- 5.NLM: CHEMM: Terrorist Incident. Washington, DC: Department of Homeland Security, Federal Emergency Management Agency; Available at https://chemm.nlm.nih.gov/terrorist.htm 2017. Accessed March 2, 2018. [Google Scholar]
- 6.NIOSH: Emergency Response Resources: Terrorism Response. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, 2016. Available at http://www.cdc.gov/niosh/topics/emres/terrorresp.html Accessed March 2, 2018. [Google Scholar]
- 7.USNRC: About NRC: Emergency Preparedness and Response. Washington, DC: United States Nuclear Regulatory Commission, 2017. Available at http://www.nrc.gov/about-nrc/emerg-preparedness.html Accessed March 2, 2018. [Google Scholar]
- 8.USFA: Fire Department Preparedness and Response to Non-Fire Emergencies. Emmitsburg, MD: U.S. Fire Administration, 2017. Available at https://www.usfa.fema.gov/operations/ops_emergencies.html Accessed March 2, 2018. [Google Scholar]
- 9.NIOSH: Emergency Response Resources: Natural Disaster/Extreme Weather Topics. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, 2015. Available at http://www.cdc.gov/niosh/topics/emres/natural.html Accessed March 2, 2018. [Google Scholar]
- 10.DHS: National strategy for Chemical, Biological, Radiological, Nuclear, and Explosives (CBRNE) standards. 2017. Available at https://www.dhs.gov/national-strategy-chemical-biological-radiological-nuclear-and-explosives-cbrne-standards Accessed March 2, 2018.
- 11.NIOSH: Emergency Response Resources: Chemical Hazards. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, 2016. Available at https://www.cdc.gov/niosh/topics/emres/chemagent.html Accessed March 2, 2018. [Google Scholar]
- 12.CDC: The Public Health Response to Biological and Chemical Terrorism: Interim Planning Guidance for State and Public Health Officials. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Environmental Health, 2001. Available at https://emergency.cdc.gov/Documents/Planning/PlanningGuidance.PDF Accessed March 2, 2018. [Google Scholar]
- 13.CDC: Preparation and Planning for Bioterrorism Emergencies. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Environmental Health, 2017. Available at https://emergency.cdc.gov/bioterrorism/prep.asp Accessed March 2, 2018. [Google Scholar]
- 14.CDC: Emergency Preparedness and Response: Radiation Emergencies. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Environmental Health, 2018. Available at https://emergency.cdc.gov/radiation/ Accessed March 2, 2018. [Google Scholar]
- 15.FEMA: Training—Radiological Emergency Preparedness. Washington, DC: Department of Homeland Security, Federal Emergency Management Agency, 2018. Available at http://www.fema.gov/training-radiological-emergency-preparedness Accessed March 2, 2018. [Google Scholar]
- 16.CDC: Environmental Hazards and Health Effects. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Environmental Health, 2015. Available at https://www.cdc.gov/nceh/ehhe/ Accessed March 2, 2018. [Google Scholar]
- 17.SAMHSA: A Guide to Managing Stress in Crisis Response Professions. Rockville, MD: U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, 2004. Available at https://store.samhsa.gov/shin/content//SMA05-4113/SMA05-4113.pdf Accessed March 2, 2018. [Google Scholar]
- 18.OSHA: Safety and Health Topics: Emergency Preparedness and Response. Washington, DC: U.S. Department of Labor, Occupational Safety and Health Administration; Available at https://www.osha.gov/SLTC/emergencypreparedness/ Accessed March 2, 2018. [Google Scholar]
- 19.OSHA: OSHA Fact Sheet: Planning and Responding to Workplace Emergencies. Washington, DC: U.S. Department of Labor, Occupational Safety and Health Administration, 2004. Available at https://www.osha.gov/OshDoc/data_General_Facts/factsheet-workplaceevergencies.pdf Accessed March 2, 2018. [Google Scholar]
- 20.FEMA: Climate Change. Washington, DC: Department of Homeland Security, Federal Emergency Management Agency, 2018. Available at http://www.fema.gov/climate-change Accessed March 2, 2018. [Google Scholar]
- 21.FEMA: Whole Community. Washington, DC: Department of Homeland Security, Federal Emergency Management Agency, 2018. Available at https://www.fema.gov/whole-community Accessed March 2, 2018. [Google Scholar]
- 22.USEPA: Acute exposure guideline levels for airborne chemicals. 2017. Available at http://www.epa.gov/aegl Accessed March 2, 2018.
- 23.NIOSH: Current Intelligence Bulletin 66: Derivation of Immediately Dangerous to Life and Health Values. Cincinnati, OH: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, 2013. Publication 2014-100. [Google Scholar]
- 24.NIOSH: The Emergency Response Safety and Health Database. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, 2012. Available at http://www.cdc.gov/niosh/ershdb/ Accessed March 2, 2018. [Google Scholar]
- 25.NLM: Wireless Information System for Emergency Responders (WISER). Washington, DC: Department of Homeland Security, Federal Emergency Management Agency; Available at http://wiser.nlm.nih.gov/index.html 2018. Accessed March 2, 2018. [Google Scholar]
- 26.NRC: Science and Decisions: Advancing Risk Assessment. Washington, DC: The National Research Council for the National Academies, The National Academies Press, 2009. [PubMed] [Google Scholar]
- 27.Semple S: Dermal exposure to chemicals in the workplace: Just how important is skin absorption? Occup Environ Med. 2004; 61(4): 376–382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.ATSDR: National Toxic Substance Incidents Program (NTSIP) annual report 2010. 2010. Available at http://www.atsdr.cdc.gov/ntsip/docs/ATSDR_Annual%20Report_031413_FINAL.pdf Accessed March 2, 2018.
- 29.Kales SN, Christiani DC: Acute chemical emergencies. N Engl J Med. 2004; 350(8): 800–808. [DOI] [PubMed] [Google Scholar]
- 30.Centers for Disease Control and Prevention (CDC): Chlorine gas exposure at a metal recycling facility—California, 2010. MMWR Morb Mortal Wkly Rep. 2011; 60(28): 951–954. [PubMed] [Google Scholar]
- 31.Dotson GS, Chen CP, Gadagbui B, et al. : The evolution of skin notations for occupational risk assessment: A new NIOSH strategy. Regul Toxicol Pharmacol. 2011; 61(1): 53–62. [DOI] [PubMed] [Google Scholar]
- 32.Dotson GS, Hudson N, Maier A: A decision support framework for characterizing and managing dermal exposures to chemicals during Emergency Management and Operations. J Emerg Manage. 2015; 13(4): 359–380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.NLM: Chemical Hazards Emergency Medical Management (CHEMM). Washington, DC: Department of Homeland Security, Federal Emergency Management Agency; Available at http://chemm.nlm.nih.gov/ 2017. Accessed March 2, 2018. [Google Scholar]
- 34.USEPA: Computer-Aided Management of Emergency Operations. Washington, DC: U.S. Environmental Protection Agency, 2018. Available at https://www.epa.gov/cameo Accessed March 2018. [Google Scholar]
- 35.Chermack TJ: Improving decision-making with scenario planning. Futures. 2004; 36(3): 295–309. [Google Scholar]
- 36.Moats JB, Chermack TJ, Dooley LM: Using scenarios to develop crisis managers: Applications of scenario planning and scenario-based training. Adv Hum Resour Dev. 2008; 10(3): 397–424. [Google Scholar]
- 37.Goodwin P, Wright G: Enhancing strategy evaluation in scenario planning: A role for decision analysis. J Manage Stud. 2001; 38(1): 1–16. [Google Scholar]
- 38.FEMA: Mission Areas. Washington, DC: Department of Homeland Security, Federal Emergency Management Agency, 2017. Available at https://www.fema.gov/mission-areas Accessed March 2, 2018. [Google Scholar]
- 39.Linkov I, Satterstrom FK, Kiker G, et al. : From comparative risk assessment to multi-criteria decision analysis and adaptive management: Recent developments and applications. Environ Sci Technol. 2006; 32(8): 1072–1093. [DOI] [PubMed] [Google Scholar]
- 40.Huang I, Keisler J, Linkov I: Multi-criteria decision analysis in environmental sciences: Ten years of applications and trends. Sci Total Environ. 2011; 409(19): 3578–3594. [DOI] [PubMed] [Google Scholar]
- 41.Lv Y, Huang GH, Guo L, et al. : A scenario-based modeling approach for emergency evacuation management and risk analysis under multiple uncertainties. J Hazard Mater. 2013; 246–247: 234–244. [DOI] [PubMed] [Google Scholar]
- 42.Stewart TJ, French S, Rios J: Integrating multicriteria decision analysis and scenario planning—Review and extension. Omega. 2013; 41(4): 679–688. [Google Scholar]