

Abstract
Aim:
The aim of this study is to compare wear of the natural teeth against monolithic zirconia and layered zirconia with different surface finishing procedures such as unpolished unglazed, polished unglazed, and polished glazed.
Materials and Methods:
The two-bodied wear test was carried out in a custom-made oral wear simulator with a sample size of 60 zirconia specimen opposing natural teeth. Zirconia specimen was divided into two groups layered and monolithic which further subdivided into unpolished unglazed, polished unglazed, and polished glazed groups (n = 10). The amount of enamel wear occurred for 250,000 cycles when opposed by monolithic and layered zirconia with different surface finishing methods was measured by loss of height of each tooth using three-dimensional scanning and loss of weight using sensitive balance at specified time intervals of 50,000 cycles during masticatory test considering baseline measurement as control. The data were statistically analyzed to compare the enamel wear against layered and monolithic zirconia with different surface finishing protocols by repeated ANOVA test.
Results:
Monolithic polished unglazed zirconia showed least tooth wear followed by monolithic polished glazed zirconia, monolithic unpolished unglazed zirconia, and layered unpolished unglazed zirconia showed highest tooth wear in terms of both height loss and weight loss (P < 0.01).
Conclusion:
Within the limitations of the study, monolithic polished unglazed zirconia is wear-friendly to the opposing natural teeth, and polished surfaces in both the groups showed less tooth wear compared to the glazed surface of zirconia specimen.
Keywords: Monolithic and layered zirconia, polished glazed, polished unglazed, unpolished unglazed zirconia, wear
INTRODUCTION
Wear is “the progressive and destructive loss of a substance or material from the surface of a body brought about by mechanical action.” Dental enamel is highly resistant to wear with an annual wear rate of approximately 30–40 μm. The wear of enamel is mainly resulting from microfracture processes and characterized by delamination and micro-ploughing.[1] The amount of tooth wear caused by the material must be the prime concern while selecting the material for any given clinical restorative treatment. For a restorative material to be ideal, the rate of tooth wear caused by the material should be closely equal to that of natural wear process.[2] Patients concern for esthetic appeal has led to the development of new generation ceramic restorations like zirconia. The clinical success of the zirconia-based restorations has been questioned with the reports of the veneering porcelain chipping. These failures can be attributed mainly in the veneer layer resulting from the mismatch of coefficient of thermal expansion between the zirconia and veneered porcelain and thickness and cooling rates. To reduce these failures, highly sintered monolithic or full anatomic zirconia crowns were developed. This helps in elimination of veneering porcelain layer, improving their clinical success and reliability.[3] Number of authors had studied on factors affecting tooth wear, and they gave a general conclusion that the rate of tooth wear varies depending on the surface finish of ceramic restorations.[4,5] Often chairside adjustments of the occlusal surface of ceramic restoration can alter the glazed surface of the restoration. This study helps us to determine whether the surface of the adjusted ceramic has to be highly polished or reglazed before final cementation and also after cementation as grinding breaks the glaze layer and subjecting the ceramic restoration to reglazing may cause revitrification and is also time-consuming.[6] Some authors recommended that glaze must be avoided because glaze surface is harder than underlying porcelain and is be more abrasive. However, some studies showed inconsistent relationship between hardness and abrasiveness of a restoration.[7] The objective of the study is to quantitatively evaluate the tooth wear caused by monolithic and layered zirconia with different surface finishing methods. The null hypothesis was there would be no difference in the resulting teeth wear when opposed by monolithic and layered zirconia with varied surface treatments.
MATERIALS AND METHODS
Sixty extracted maxillary first premolars were collected, and each tooth was mounted in a polyvinyl chloride tube of height 1 inch and width of 2 cm with the use of self-cure acrylic resin [Figure 1]. Ten teeth specimens mounted in polyvinyl chloride tubes were embedded in the circular aluminum disc of outer diameter 9 cm, inner diameter 5 cm, and height 2 cm.
Figure 1.
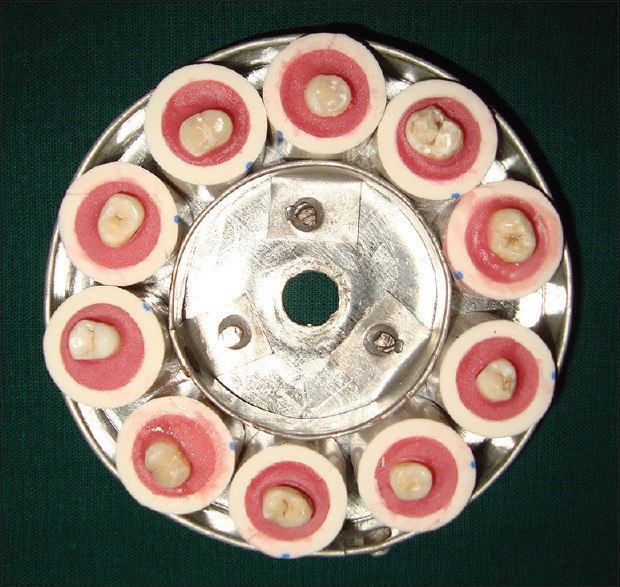
Maxillary premolars mounted in polyvinyl chloride tubes
To standardize the size and shape of the specimen, this study used computer-aided design/computer-aided manufacturing (CAD-CAM) milled zirconia specimen. Zirconia block (DentGallop, USA) was milled into discs of diameter 2 cm and thickness of 2 mm according to the preprogrammed CAD-CAM software. The milled zirconia discs were sintered in sintering oven following the manufacturer's instructions. A total of 60 sintered zirconia discs obtained were sandblasted aluminum oxide particles (250 μ) from a distance of 10 mm for 20 s under 3.5 bar pressure, to increase surface roughness and enhance bonding strength, steam cleaned for 10 min, followed by ultrasonic cleaning, and air-dried. Then, the discs were prepared according to their groups, i.e., unpolished and unglazed (n = 10), polished and unglazed (n = 10), polished and glazed monolithic zirconia (n = 10), unpolished and unglazed (n = 10), polished and unglazed (n = 10), and polished and glazed layered zirconia (n = 10).
Thirty zirconia discs were subjected to layering procedure. Porcelain powder dentin A2 shade was mixed with adequate amount of modeling liquid. Excess water was mopped. Incremental brushing technique was used, by adding an increment of creamy mix of porcelain on the zirconia discs excess anticipating shrinkage to attain a thickness of 1 mm ceramic layer over zirconia disc. Firing was performed in a calibrated porcelain furnace (CY-M1200-1 L, China). Another layer of dentin was applied to compensate for porcelain shrinkage that occurred during the initial firings, and then, enamel A2 shade was applied. Second firing of dentin and enamel was completed following manufacturer specified temperature, pressure, and time. Measurements were made with an Iwanson's guage in the multiple locations on the porcelain disc to ensure the porcelain layer was flat and symmetrical. Specimen to be polished was initially finished with Iris ceramic finishing diamond points followed by Shofu polishing discs (coarse 55 μm, medium 40 μm, fine 24 μm, and superfine 8 μm) in unidirectional manner accordingly to the manufacturer's instructions with zirconia discs mounted on a putty index. The coarse grit disc was used at approximately 10,000 rpm for 5 s. The discs were subsequently polished with medium disc and fine disc without water at approximately 10,000 rpm for 15 s followed by polishing with superfine disc without water at approximately 30,000 rpm for 15 s.
The specimen to be glazed was initially finished with Iris ceramic finishing diamond points followed by Shofu polishing kit in unidirectional manner, and a single coat of glaze was applied and fired in VITA VACUMAT porcelain furnace according to the manufacturer's instructions. Zirconia discs were secured into the aluminum discs [Figure 2] using cold cure acrylic resin in such a way that all discs lie in one plane, and mounted teeth specimens were secured into aluminum discs using putty consistency siloxane impression to facilitate wear scans for every 50,000 cycles.
Figure 2.

Zirconia discs secured in aluminum discs
A custom-made planar oral simulating wear testing machine was constructed [Figure 3]. Apparatus consists of a glass container made of borosil consists of lower fixed aluminum disc and an upper rotating aluminum disc attached to the shaft of motor into which ten ceramic specimens were embedded and the height of the shaft was adjusted such that teeth specimen made a point contact with the opposing ceramic specimen, forming a ball-on-flat contact geometry. This geometric contact is considered to be representative of the masticatory function. The motor along with upper aluminum disc was secured by two iron bars welded at the right angle, and these bars are attached to the base of the apparatus wooden plank. The upper disc was rotated with the help of a 5 kg capacity Johnson's motor operating at a rate of 10 revolutions per minute accompanied with AC Adapter, (100–240V, 1.5A model-BPR 6612). Relicell energy storage battery 12V, 7 AH was attached so that the test can be continued up to 6 h even in the absence of power supply. A load of 5 kg was attached to superior portion of the upper disc to simulate the masticatory load. An aquarium water pump was modified and used so that aluminum discs were continually immersed and washed with artificial saliva which circulates between the reservoir and the container throughout the experiment. The temperature was maintained at 37°C temperature. The test was performed at the frequency of 10 cycles per min and continued for 250,000 cycles in chewing simulator which is comparable to approximately 1-year chewing from a clinical perspective. The amount of enamel wear was measured by weight analysis using sensitive balance with 0.001 g sensitivity and 500 g capacity. Each tooth specimen was weighed before the test, and the respective values were recorded as baseline values of that specimen and after every 50,000 cycles, the procedure was repeated. Three-dimensional (3D) scanning was used to scan each tooth specimen before the test and for every 50,000 cycles of the masticatory test. The procedure was repeated after 1 lakh, 1.5 lakhs, 2 lakhs until 2.5 lakhs cycles and values were recorded. The scans obtained were analyzed for quantitative wear using auto-CAD software for every 50,000 cycles of the masticatory test [Figures 4–6]. The data obtained were statistically analyzed using repeated ANOVA test between and within the groups.
Figure 3.
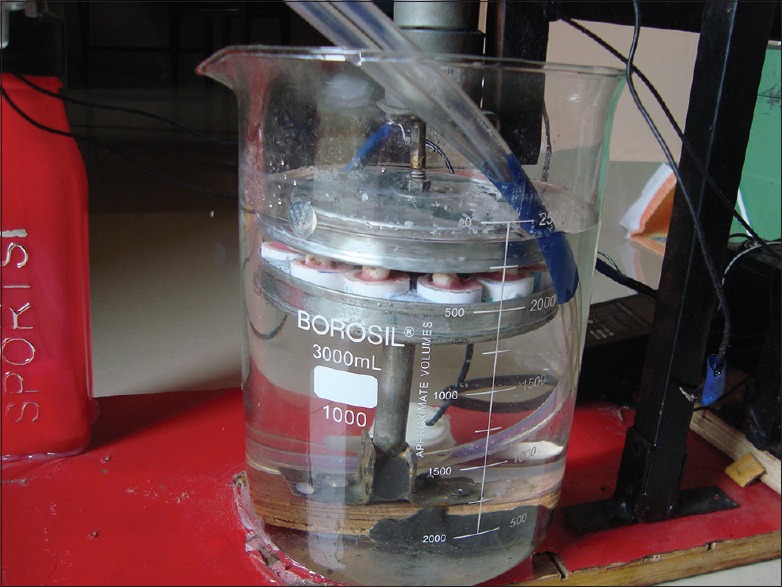
Customized oral wear simulator
Figure 4.
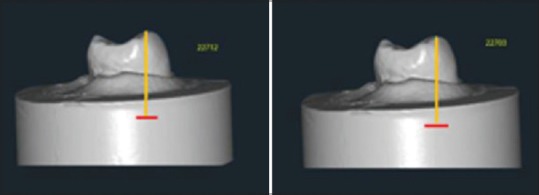
Auto computer-aided design scans showing teeth wear at baseline and after 50,000 cycles
Figure 6.
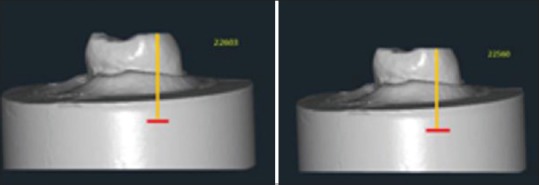
Auto computer-aided design scans showing teeth wear after 2 lakhs and after 2.5 lakhs cycles
Figure 5.
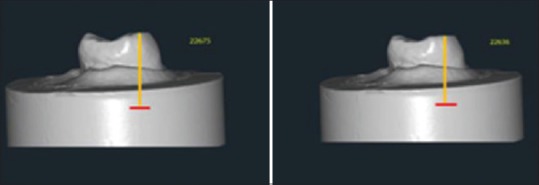
Auto computer-aided design scans showing teeth wear after 1 lakh and after 1.5 lakhs cycles
RESULTS
The mean teeth wear caused by zirconia specimen in terms of height loss and weight loss after 250,000 cycles;
The mean loss of height of tooth samples and its standard deviation for layered unpolished unglazed zirconia, layered polished unglazed zirconia, layered polished glazed zirconia, monolithic unpolished unglazed zirconia, monolithic polished unglazed zirconia, and monolithic polished glazed zirconia was obtained as 207.34 ± 0.92, 117.51 ± 4.66, 155.02 ± 1.62, 68.84 ± 2.71, 33.95 ± 0.96, and 39.67 ± 1.74, respectively. The highest mean loss in height was observed in the layered unpolished unglazed group, and the least was observed in monolithic polished unglazed group.
Table 1 shows the comparison of the mean loss of height in the study groups using repeated ANOVA test. There was statistically significant difference in loss of tooth height among the study groups (P < 0.01).
Table 1.
Height loss of natural teeth opposing monolith and layered zirconia with different surface finishing procedures by using repeated ANOVA test
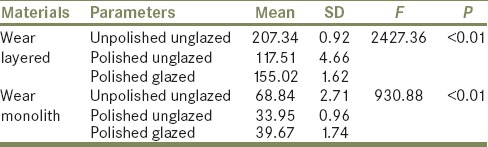
Table 2 shows the comparison of the mean weight in the study groups, which were statistically significant, whereas the mean difference in weight loss between monolithic polished unglazed (1.61 ± 0.45) and monolithic polished glazed (1.68 ± 0.52) groups was − 0.07, with P = 0.2, hence not statistically significant.
Table 2.
showing weight loss of natural teeth opposing monolith and layered zirconia with different surface finishing procedures by using repeated ANOVA test

Graphs 1 and 2 compare the loss of height and weight loss of all six groups. It is observed that monolithic polished unglazed zirconia shows the least amount of wear while layered unpolished unglazed zirconia shows the significantly higher wear of opposing tooth.
Graph 1.
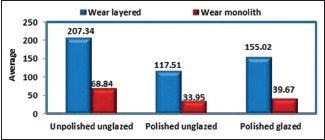
Height loss of natural teeth opposing monolithic and layered zirconia with different surface finishing procedures using repeated ANOVA test
Graph 2.
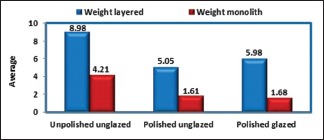
Weight loss of natural teeth opposing monolithic and layered zirconia with different surface finishing procedures using repeated ANOVA test
DISCUSSION
Wear of the teeth is a natural phenomenon and amount of wear that will occur on both the restored surface and opposing enamel is an important consideration as it will affect the vertical dimension of occlusion. Functional finishing of ceramic surfaces during the wear process was documented by Monasky, who reported in his in vitro study that the initially high rate of wear decreased over time, suggesting that the effect of surface roughness on wear may be self-limiting. Jagger and Harrison[8] in his study suggested that the amount of enamel wear caused by glazed and unglazed porcelain is similar. However, factors such as hardness, porosity, resistance to friction, fracture toughness, crystal structure, ceram layering, and nature of the surface finish of ceramics affect the opposing enamel wear.[9,10,11]
The results of this study indicated significant differences in the teeth wear caused by monolithic and layered zirconia with different surface treatments. Therefore, the null hypothesis was rejected. Monolithic polished unglazed zirconia caused the least amount of enamel wear followed by monolithic polished glazed zirconia, and the highest tooth wear was shown by layered unpolished unglazed zirconia. The choice of finishing and polishing technique to achieve the optimum smoothness of glazed porcelain has been the subject of a number of studies. Zalkind et al.[12] found that glazing a porcelain surface which is reduced by an abrasive instrument will not reduce the resulting roughness. They observed that the only way to produce a surface as smooth as it had been before is to polish the abraded surface before refiring to produce a natural glaze.
This study measured two-bodied wear as it was shown that the teeth come in contact more number of times in between meals (394 swallowing cycles) than during eating (146 swallowing cycles) by Flanagan et al.[13] Artificial saliva was used as a medium to simulate oral environment and to flush off the worn particles and to prevent clogging.
As wear simulators try to simulate the mechanisms which occur in the oral cavity during the masticatory process, the wear test setup has to fulfill various prerequisites such as force – the wear testing device simulator should generate clinically relevant forces, which are in the range of 20–120 N; distance – the highest kinematic values of movements were measured to be between 16 and 20 mm; contact time – the contact time between stylus and material should be of a clinically relevant length and should be kept constant during the simulation phase; and clearance – it should be ensured that worn material is cleared from the test surfaces. This can be achieved by a constant exchange of liquid like water or abrasive medium, which fills the test chamber.
Two-thirds of wear can be resulted from contact with opposing teeth which was simulated in this study, and the wear contributing factors are the surface roughness of the specimen; geometry of specimen – increase in the contact area of specimen increases wear; temperature, pH, abrasiveness of the food and flushing action by saliva; and force generated against natural teeth during masticatory and nonmasticatory contacts – higher forces produce higher wear.
Force, time, and duration of the test
The wear increases with increasing number of cycles. Most in vitro wear test methods demonstrate a run-in phase with a steep increase in wear in the initial phase and a flattening of the curve thereafter.[14,15]
The present study used a basic and uncomplicated design that involved the effect of constant sliding load on wear because teeth contact and slide during both centric and eccentric movements and it was thought that basic data were needed before the impact of various variables and loading designs were evaluated and this can be used to predict the clinical conditions. The load chosen in our study was a weight of 5 kg, which is comparable to 49 N of chewing force exerted which vary from individual to individual. It is generally found that males can bite with more force (118–142 lbs) than can females (79–99 lbs.). Length and time of contact were a result of the mechanical design of the wear machine. Theoretically, all teeth specimens were in constant contact with the zirconia specimen, equally distributing the load throughout the simulation phase.
Indirect techniques for the evaluation of tooth wear suggest measuring the loss of tooth surface using cast replicas. For more accurate quantification, image analysis, scanning electron microscopy, computer graphics, 3D scanner, and profilometry were developed. Disadvantages of using cast replicas can be inaccurate replicas and repositioning problems, due to the fact that reproducing of tooth surfaces with impressions before scanning always adds a source of error. Image analysis and 3D scanner techniques are highly accurate, quantitative, applicable to both the clinic and the laboratory, and provides storable 3D databases that enable comparison to other 3D databases. This study used the indirect technique for the evaluation of tooth wear by 3D scan image analysis which is highly accurate, quantitative, and provides storable databases.[16,17,18]
From the results of the study, the average wear caused by monolithic polished unglazed zirconia was least with mean of 33.95, F value (test of equivalence) 930.88, and P < 0.01 [Table 1 and Graph 1]. Similarly, average weight loss caused by monolithic polished unglazed zirconia was least with a mean of 1.61, F value (test of equivalence) 77.74, and P < 0.01 [Table 2 and Graph 2]. This is in accordance with the studies conducted by Wang et al. and Mitov et al.[19,20] who stated that untreated layered zirconia specimen exhibits rough surface which causes more tooth wear might be due to its poor surface properties such as roughness, porosity, and crack propagation which are reduced by surface finishing procedures such as polishing and glazing.
On comparison of wear rates of teeth opposed by monolithic and layered unpolished unglazed groups, it was observed that there was increase in teeth wear from baseline to 1 lakh cycles showing highest teeth wear during 50000–1 lakh cycles and then decreased from 1 lakh to 2.5 lakhs cycles. This is in agreement with previous studies by DeLong et al. and al-Hiyasat et al.[21,22] This might be because of the conical cusp shape, with the reduction in the height of the tooth because of wear, the surface area increase gradually, and the load became distributed over a large area. This can also be due to increase in exposure of underlying wide tooth structure with thick and broadband of resistant enamel remaining around the margins of contact area and increased surface area which decreases further teeth wear by distribution of occlusal loads to wider area.
On comparison of wear rates of teeth opposed by monolithic and layered polished glazed zirconia groups, teeth wear rate was increased from baseline to 2 lakhs cycles showing highest wear during 1.5–2 lakhs cycles and then decreased from 2 lakhs to 2.5 lakhs cycles. The possible reason might be the formation of cracks and their further propagation resulting in the formation of loose particles which will be trapped between the surfaces of teeth and specimen tested, increasing the wear of opposing enamel. This is in accordance with the study conducted by Jung et al. and Janyavula et al.[23,24] who stated that glazed zirconia causes more wear than polished zirconia.
Monolithic polished unglazed zirconia group resulted in the least teeth wear which is attributable to the fact that no porcelain was added in the glazing process.[25,26] The crack-free zirconium surfaces demonstrated no fragment or particle chipping. Therefore, the polished zirconia full-coverage crown without glazing is more effective in reducing antagonistic teeth wear.
In our study, a similar pattern of teeth wear was shown by monolithic polished unglazed and monolithic polished glazed zirconia as well as layered polished unglazed and layered polished glazed zirconia while monolithic and layered polished glazed specimen causing highest teeth wear during after 1 lakh cycles of the study. The possible reason might be that worn out glazed layer exposes underlying well-polished smooth and hard surface which decreases further wear. This is in accordance with study conducted by Stober et al., Rupawala, et al., and Palmer et al.[27,28,29] who emphasized the need for precise polishing of the surface of restoration after occlusal adjustment.
The limitations of the study include limited inclusion of physiologic parameters such as temperature, contact time, variation in forces, and pH cycling. Simple height loss can also be misleading if specimens are not in uniform diameter because as wear progresses, the surface area of the contact increases or decreases. This results in a nonlinear rate of wear and becomes increasingly difficult to compare different samples.
CONCLUSION
Within the limitations of this study, it was concluded that as follows:
Statistically significant wear of enamel was observed opposing monolithic and layered zirconia with different surface finishing's
Monolithic zirconia causes less teeth wear compared to layered zirconia
Polished unglazed monolithic zirconia resulted in less teeth wear compared to unpolished unglazed monolithic zirconia and polished glazed monolithic zirconia
This study represents a 1-year clinical perspective which represents that monolithic polished unglazed zirconia is indicated in full contour restorations, and they should be polished after 6 months of cementation with subsequent follow-up can be more desirable.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Lambrechts P, Braem M, Vuylsteke-Wauters M, Vanherle G. Quantitative in vivo wear of human enamel. J Dent Res. 1989;68:1752–4. doi: 10.1177/00220345890680120601. [DOI] [PubMed] [Google Scholar]
- 2.Ramp MH, Suzuki S, Cox CF, Lacefield WR, Koth DL. Evaluation of wear: Enamel opposing three ceramic materials and a gold alloy. J Prosthet Dent. 1997;77:523–30. doi: 10.1016/s0022-3913(97)70146-x. [DOI] [PubMed] [Google Scholar]
- 3.Ozkurt-Kayahan Z. Monolithic zirconia: A review of literature. Biomed Res. 2016;27:1427–35. [Google Scholar]
- 4.Monasky GE, Taylor DF. Studies on the wear of porcelain, enamel, and gold. J Prosthet Dent. 1971;25:299–306. doi: 10.1016/0022-3913(71)90191-0. [DOI] [PubMed] [Google Scholar]
- 5.Klausner LH, Cartwright CB, Charbeneau GT. Polished versus autoglazed porcelain surfaces. J Prosthet Dent. 1982;47:157–62. doi: 10.1016/0022-3913(82)90180-9. [DOI] [PubMed] [Google Scholar]
- 6.Brewer JD, Garlapo DA, Chipps EA, Tedesco LA. Clinical discrimination between autoglazed and polished porcelain surfaces. J Prosthet Dent. 1990;64:631–4. doi: 10.1016/0022-3913(90)90284-j. [DOI] [PubMed] [Google Scholar]
- 7.Jacobi R, Shillingburg HT, Jr, Duncanson MG., Jr A comparison of the abrasiveness of six ceramic surfaces and gold. J Prosthet Dent. 1991;66:303–9. doi: 10.1016/0022-3913(91)90254-t. [DOI] [PubMed] [Google Scholar]
- 8.Jagger DC, Harrison A. An in vitro investigation into the wear effects of unglazed, glazed, and polished porcelain on human enamel. J Prosthet Dent. 1994;72:320–3. doi: 10.1016/0022-3913(94)90347-6. [DOI] [PubMed] [Google Scholar]
- 9.DeLong R, Douglas WH, Sakaguchi RL, Pintado MR. The wear of dental porcelain in an artificial mouth. Dent Mater. 1986;2:214–9. doi: 10.1016/S0109-5641(86)80016-1. [DOI] [PubMed] [Google Scholar]
- 10.Ekfeldt A, Oilo G. Occlusal contact wear of prosthodontic materials. An in vivo study. Acta Odontol Scand. 1988;46:159–69. doi: 10.3109/00016358809004762. [DOI] [PubMed] [Google Scholar]
- 11.Claus H. The structure and microstructure of dental porcelain in relationship to the firing conditions. Int J Prosthodont. 1989;2:376–84. [PubMed] [Google Scholar]
- 12.Zalkind M, Lauer S, Stern N. Porcelain surface texture after reduction and natural glazing. J Prosthet Dent. 1986;55:30–3. doi: 10.1016/0022-3913(86)90067-3. [DOI] [PubMed] [Google Scholar]
- 13.Flanagan JB. The 24-hour pattern of swallowing in man. J Dent Res. 1963;42:1072. [Google Scholar]
- 14.Heintze SD. How to qualify and validate wear simulation devices and methods. Dent Mater. 2006;22:712–34. doi: 10.1016/j.dental.2006.02.002. [DOI] [PubMed] [Google Scholar]
- 15.Lambrechts P, Debels E, Van Landuyt K, Peumans M, Van Meerbeek B. How to simulate wear? Overview of existing methods. Dent Mater. 2006;22:693–701. doi: 10.1016/j.dental.2006.02.004. [DOI] [PubMed] [Google Scholar]
- 16.DeLong R. Intra-oral restorative materials wear: Rethinking the current approaches: How to measure wear. Dent Mater. 2006;22:702–11. doi: 10.1016/j.dental.2006.02.003. [DOI] [PubMed] [Google Scholar]
- 17.Al-Omiri MK, Harb R, Abu Hammad OA, Lamey PJ, Lynch E, Clifford TJ. Quantification of tooth wear: Conventional vs.new method using toolmakers microscope and a three-dimensional measuring technique. J Dent. 2010;38:560–8. doi: 10.1016/j.jdent.2010.03.016. [DOI] [PubMed] [Google Scholar]
- 18.Hmaidouch R, Weigl P. Tooth wear against ceramic crowns in posterior region: A systematic literature review. Int J Oral Sci. 2013;5:183–90. doi: 10.1038/ijos.2013.73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mitov G, Heintze SD, Walz S, Woll K, Muecklich F, Pospiech P, et al. Wear behavior of dental Y-TZP ceramic against natural enamel after different finishing procedures. Dent Mater. 2012;28:909–18. doi: 10.1016/j.dental.2012.04.010. [DOI] [PubMed] [Google Scholar]
- 20.Wang L, Liu Y, Si W, Feng H, Tao Y, Ma Z. Friction and wear behavior of dental ceramics against natural tooth enamel. J Eur Ceram Soc. 2012;32:2599–606. [Google Scholar]
- 21.Delong R, Pintado MR, Douglas WH. The wear of enamel opposing shaded ceramic restorative materials: An in vitro study. J Prosthet Dent. 1992;68:42–8. doi: 10.1016/0022-3913(92)90282-f. [DOI] [PubMed] [Google Scholar]
- 22.al-Hiyasat AS, Saunders WP, Sharkey SW, Smith GM, Gilmour WH. The abrasive effect of glazed, unglazed, and polished porcelain on the wear of human enamel, and the influence of carbonated soft drinks on the rate of wear. Int J Prosthodont. 1997;10:269–82. [PubMed] [Google Scholar]
- 23.Jung YS, Lee JW, Choi YJ, Ahn JS, Shin SW, Huh JB. A study on the in-vitro wear of the natural tooth structure by opposing zirconia or dental porcelain. J Adv Prosthodont. 2010;2:111–5. doi: 10.4047/jap.2010.2.3.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Janyavula S, Lawson N, Cakir D, Beck P, Ramp LC, Burgess JO. The wear of polished and glazed zirconia against enamel. J Prosthet Dent. 2013;109:22–9. doi: 10.1016/S0022-3913(13)60005-0. [DOI] [PubMed] [Google Scholar]
- 25.Mundhe K, Jain V, Pruthi G, Shah N. Clinical study to evaluate the wear of natural enamel antagonist to zirconia and metal ceramic crowns. J Prosthet Dent. 2015;114:358–63. doi: 10.1016/j.prosdent.2015.03.001. [DOI] [PubMed] [Google Scholar]
- 26.Esquivel-Upshaw JF, Kim MJ, Hsu SM, Abdulhameed N, Jenkins R, Neal D, et al. Randomized clinical study of wear of enamel antagonists against polished monolithic zirconia crowns. J Dent. 2018;68:19–27. doi: 10.1016/j.jdent.2017.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Stober T, Bermejo JL, Rammelsberg P, Schmitter M. Enamel wear caused by monolithic zirconia crowns after 6 months of clinical use. J Oral Rehabil. 2014;41:314–22. doi: 10.1111/joor.12139. [DOI] [PubMed] [Google Scholar]
- 28.Rupawala A, Musani SI, Madanshetty P, Dugal R, Shah UD, Sheth EJ. A study on the wear of enamel caused by monolithic zirconia and the subsequent phase transformation compared to two other ceramic systems. J Indian Prosthodont Soc. 2017;17:8–14. doi: 10.4103/0972-4052.194940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Palmer DS, Barco MT, Pelleu GB, Jr, McKinney JE. Wear of human enamel against a commercial castable ceramic restorative material. J Prosthet Dent. 1991;65:192–5. doi: 10.1016/0022-3913(91)90161-o. [DOI] [PubMed] [Google Scholar]