

Abstract
Increased intake of potassium should be promoted to reduce the risk of cardiovascular disease and stroke and to protect against bone loss, but confidence in recommended intakes depends on the strength of the evidence. All public health recommendations are considerably higher than current average intakes. Evidence on which current potassium intake recommendations for the United States, Europe, and globally have limitations. More recent evidence reviewed by the Agency for Healthcare Research and Quality affirms that more evidence is needed to define specific values for optimal potassium intakes. Potassium requirements undoubtedly vary with a number of factors including energy needs, race, and intake of sodium.
Potassium is an essential nutrient of concern according to recent Dietary Guidelines for Americans Advisory Committees.1–3 Current recommendations for the United States and Canada, established by the Institute of Medicine (IOM), are given as an Adequate Intake (AI) of 4700 mg/d for individuals older than 14 years,4 but the evidence supporting this has been challenged. The average potassium intake of US adults participating in the National Health and Nutrition Examination Survey 2011–2012 was 2795 ± 34 mg/d, with less than 3% of the population meeting the AI.5 This low intake was recently confirmed by 24-hour urinary potassium excretion from National Health and Nutrition Examination Survey 2014; the mean was 2155 mg and was lower in older adults aged 45 to 69 years compared with younger adults aged 20 to 44 years.6 With this large gap between recommended intakes and consumption, it is important to carefully evaluate the strength of the evidence for the current recommendations, especially in the context of the whole diet (eg, energy and other minerals), to determine the priority for manipulating the food supply and altering public health messages.
Evaluating potassium requirements is a timely nutrition topic as the National Academies of Science, Engineering, and Medicine have convened a panel to update the Dietary Reference Intakes (DRIs) for potassium and sodium. To assist them, a systematic review of the relation between potassium and sodium intake and chronic disease was undertaken by the Agency for Healthcare Research and Quality (AHRQ).7 Of great interest is whether the DRI panel will conclude that there is now sufficient evidence to move from an AI to an Estimated Average Requirement (EAR), Reference Dietary Allowance (RDA), and Tolerable Upper Intake Level (UL), for either potassium or sodium. Alternatively, if an AI is retained, will the values change? To set an EAR (the most important reference point), evidence of a dose-response effect on an outcome of interest in a representative population is needed to determine distribution of response.
In this article, we review the basis for the current recommendations for potassium determined by the IOM for the United States and Canada, by the European Food Safety Administration (EFSA) for Europe, and by the World Health Organization (WHO) for global recommendations. We also evaluate the quality of trials that exist to inform the panel charged with setting the DRIs. Lastly, we consider translating the recommendations to current food intake in the context of the whole diet.
DIETARY RECOMMENDATIONS FOR POTASSIUM IN NORTH AMERICA
Establishing the DRI for Potassium
The DRI committee, tasked with establishing the DRIs for potassium in 2005, reviewed the scientific evidence from both epidemiological and intervention studies that assessed the relationship between potassium intake and various health outcomes. When the DRIs were first published, the committee concluded that sufficient evidence existed to establish an AI, but not an EAR (or RDA). Although the AI and RDA for any nutrient are established using different criteria, both the AI and RDA are intended to serve as recommended levels of intake that should reduce the risk of developing a negative health condition in otherwise healthy individuals.4 For potassium, the health conditions considered included potassium balance and hypokalemia, elevated blood pressure, decreased bone mineral density (BMD), and kidney stones. Severe potassium deficiency can cause hypokalemia, but this is rare in relatively healthy individuals.8 In addition, hypokalemia is rarely caused by low potassium intake alone, but usually develops secondary to other conditions such as severe vomiting or diarrhea. Potassium insufficiency, however, can occur even at intakes above those required to prevent hypokalemia. Indeed, the DRI report discusses evidence suggesting that even with a potassium intake minimally sufficient to maintain balance, a chronic intake at this level results in other negative clinical consequences related to chronic disease risk. Therefore, the DRI report focused mainly on these chronic disease outcomes when establishing the AI for potassium. Based on the available data, the committee focused mainly on elevated blood pressure and kidney stones as meaningful pathological end points that may result from insufficient potassium intake, as hypertension is a leading cause of morbidity and mortality worldwide. More than one-third of US adults have hypertension, and it is second only to smoking as a preventable cause of death in the United States.9,10 Thus, a potassium intake sufficient to prevent these conditions, as determined using current evidence, served as the basis for setting the AI.
The AIs established for each age/life stage group as well as the scientific basis for setting each AI are summarized in Table 1. For adults, the AI of 4700 mg/d was set based on the evidence suggesting that potassium intake of this level lowered blood pressure, especially in salt-sensitive individuals, and prevented kidney stones. Although many studies were considered in setting this AI, a study by Morris and colleagues11 is cited throughout the DRI document. The aim of this study was to assess the association between potassium intake and blood pressure and the role of salt sensitivity in healthy, normotensive black and white adult men (n = 38). Moderate salt sensitivity was defined as a salt-induced increase of mean arterial blood pressure of 3 mm Hg or greater, and severe salt sensitivity was defined as an increase of 10 mm Hg or greater. Salt sensitivity occurs more frequently in blacks (as compared with whites), but the researchers in this study hypothesized that this is only true when dietary potassium is low, as blacks also have lower potassium intakes than do whites.5 For the first 2 weeks of the 6-week controlled feeding study, participants consumed a basal diet providing 1200 mg/d of potassium and 350 mg/d of sodium. For the last 4 weeks, sodium was loaded (5700 mg/d), and for the last 3 of those 4 weeks, potassium intake was manipulated with either a placebo or a potassium bicarbonate supplement, making total potassium intake either 1200, 2700, or 4700 mg/d. Salt loading induced a significant increase in blood pressure in blacks only, with salt sensitivity occurring in 79% of blacks as compared with 36% of whites. Five blacks, but no whites, demonstrated severe salt sensitivity, and salt loading induced a significant increase in blood pressure in blacks only. At a moderate potassium intake (2700 mg/d), moderate salt sensitivity was attenuated to the same extent in both blacks and whites, although the frequency was still significantly greater in blacks compared with whites. In addition, blood pressure decreased in blacks, although it remained lower in whites. At a high potassium intake (4700 mg/d), blood pressure decreased further, and the frequency of salt sensitivity in blacks reached the same level as that observed in whites with an intake of 2700 mg/d, with moderate salt sensitivity eliminated. Taken together, these results suggest that a potassium intake of 2700 mg/d was effective for reducing blood pressure and salt sensitivity in whites, but in blacks an intake of 4700 mg/d provided even more heart-health benefits. This would justify setting the AI at 4700 mg/d, but potassium intakes between 2700 and 4700 mg/d were not tested.
TABLE 1.
Summary of the Current US AI and Basis for Establishing Adequate Intake (AI) for Potassium in All Age/Life Stages
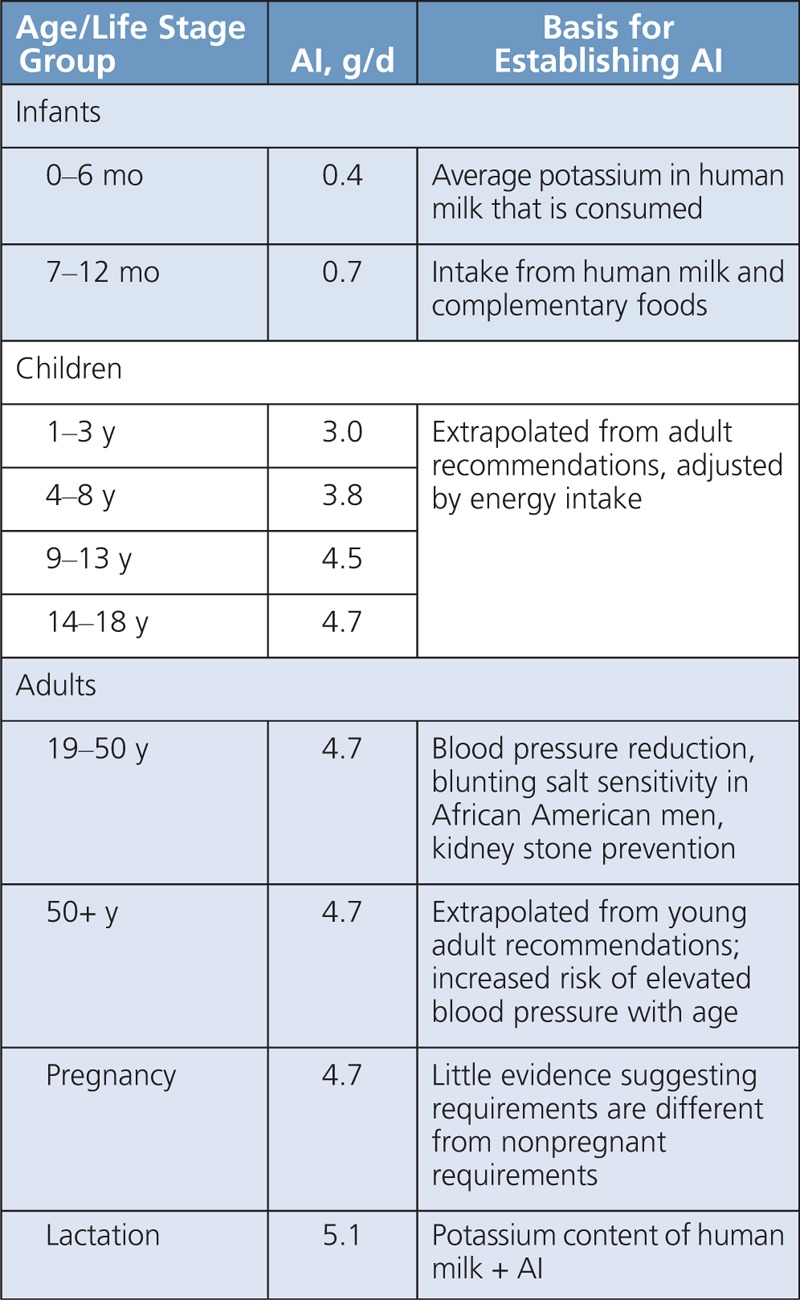
While the study by Morris et al11 supports higher potassium intake, using it as the primary foundation for our current AI is questionable because of several important limitations. First, the sample size was small (n = 38) and relatively homogeneous. The sample included both black and white participants, but only men between the ages of 31 and 65 years, which prevents broader generalizability. Extrapolating the results from such a small and homogeneous sample to other age groups, especially children, is problematic because there is no direct evidence that an intake this high is necessary for everyone. Another limitation is that this was not a crossover study, which precludes any intraindividual comparisons with different levels of potassium intake. This reduces the power to detect differences in blood pressure and salt sensitivity, which otherwise may have been observed at the moderate level of potassium intake (2700 mg/d), especially in blacks. Finally, a large percentage of participants were determined to be salt-sensitive. The introduction of the article by Morris et al11 describes salt sensitivity as a precursor to hypertension, which might suggest that salt sensitivity is a disease state in its own right. This is problematic because, by definition, the AI should meet the needs of an otherwise healthy population. Therefore, this begs the question: Is 4700 mg/d an appropriate AI for everyone, or rather an intake that could be recommended on an individual basis to those who are at increased risk of salt-sensitive hypertension?
POTASSIUM: RECOMMENDATIONS FROM AROUND THE WORLD
Other countries often derive and compare their dietary recommendations to the North American DRIs or to global recommendations developed by the WHO (summarized in Table 2).4,14–17 However, as illustrated in Figure, there are large global variations in potassium consumption, with few countries meeting the WHO recommendation and none meeting the IOM recommendation.14,15,17–23
TABLE 2.
Summary of Global Potassium Recommendations
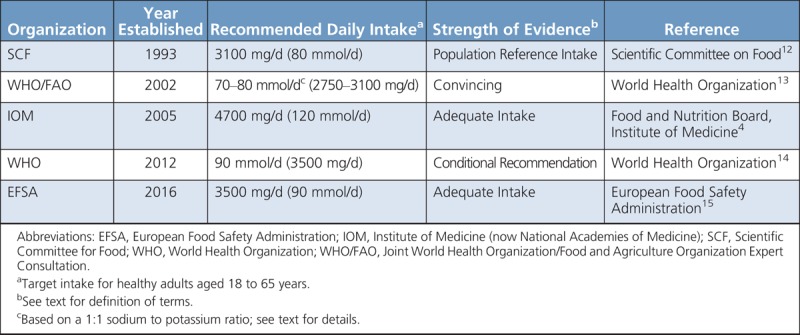
FIGURE.
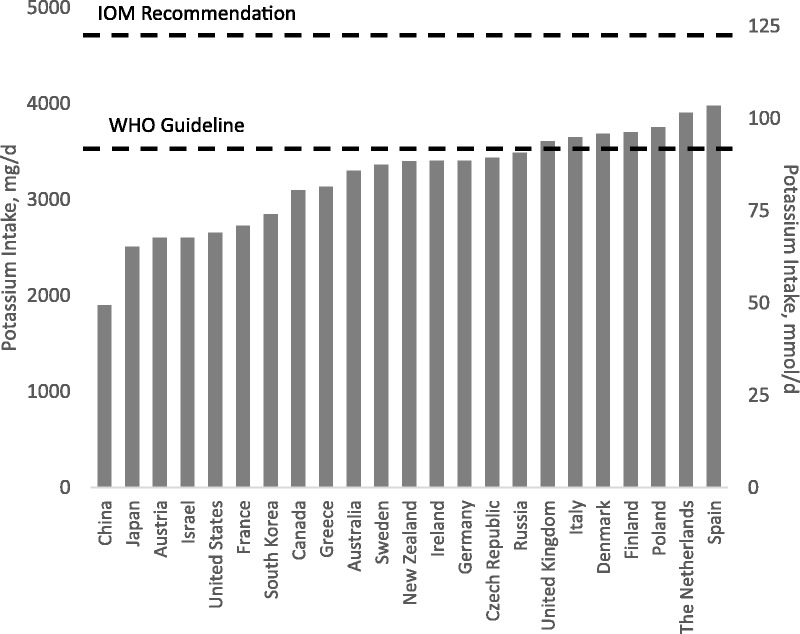
Current potassium intakes in populations around the world. Few countries meet the reference guidelines put forth by World Health Organization and European Food Safety Administration, and none meet the Institute of Medicine recommendation.12,13,15–21
The First Guidelines
The first published reports of potassium guidelines were produced by the Scientific Committee for Food (SCF)12 and a joint committee convened by the WHO and Food and Agriculture Organization.13 These reports were comprehensive in nature, aimed at giving a brief overview of all nutrients and their recommended levels in the context of a healthy diet. The SCF proposed a Population Reference Intake (PRI, equivalent to North American RDA) for potassium of 3500 mg/d (80 mmol/d) to lower blood pressure and assist with sodium excretion.12 Similarly, the WHO/Food and Agriculture Organization Joint Commission recommended potassium intakes of 70 to 80 mmol/d (2750–3100 mg/d) to lower blood pressure and protect against cardiovascular disease (CVD).13 Ironically, this recommendation was designed to keep the Na:K molar intake ratio at approximately 1:1, an idea that is gaining popularity again today. These reports were instrumental in creating a baseline for dietary intakes, allowing later reports to examine the evidence for individual nutrients in greater depth and refine these initial recommendations.
WHO Recommendations
At the request of member states, the WHO convened 3 meetings in 2011 to 2012 to examine evidence for linking potassium intake to noncommunicable diseases. As a result of these meetings, 2 major documents were produced. The first contained the official recommendations of the WHO,14 whereas the second detailed the systematic review and meta-analysis upon which the recommendations were based.24 The key aims were (1) to identify health outcomes correlated with increased levels of potassium intake as compared with lower levels of intake and (2) to compare potassium intakes of less than 90, 90 to 120, 120 to 155, and greater than 155 mmol/d (<3500, 3500–4700, 4700–6000, and >6000 mg/d, respectively) in relation to health outcomes.14 To address these aims, 33 studies in adults and 4 studies in children were included.24 Predictably, the lack of studies in children precluded the establishment of strong recommendations in that population; thus, only results from studies in adults are presented here.
The key end points evaluated were blood pressure, stroke, CVD, coronary heart disease (CHD), blood lipids, and catecholamines. The largest and most consistent effects of increased potassium intake were for blood pressure reduction in hypertensive individuals consuming 90 to 120 mmol (3500–4700 mg) of potassium per day.24 Although this effect was not observed in normotensive individuals, which may be due to the paucity of available studies (3 studies), dietary potassium’s ability to lower blood pressure in hypertensives is important because blood pressure is considered a reliable biomarker for estimating the risk of CVD.14 The relationship between increased potassium intake and reduced incidence of stroke, CVD, and CHD is much weaker.24
Other key observations by the WHO in their evaluation of the evidence included no risk of hyperkalemia (serum potassium concentration >5.5 mmol/L) from potassium-rich foods and no change in blood lipids (total, low-density lipoprotein, and high-density lipoprotein cholesterol) or catecholamines in healthy adults.24 Further, when stratified by sodium intake, the strongest blood pressure–lowering effects were noted in those consuming the highest levels of sodium, suggesting that the effects of sodium and potassium on blood pressure may be inversely linked.24 Although outside the scope of guidelines on potassium, WHO commented that following their guidelines for both sodium and potassium results in a molar intake ratio of approximately 1:1 of Na:K.14
After evaluating the evidence, WHO made a strong recommendation* for increasing potassium intake to reduce blood pressure, CVD, stroke, and CHD.12 In addition, they made a conditional recommendation† to consume at least 90 mmol/d (3500 mg/d) of potassium to achieve these benefits.14 These recommendations point to potassium’s clear and consistent blood pressure–lowering effect, although more studies are necessary to determine the precise level of potassium intake needed to obtain the maximal health benefits.
EFSA Recommendations
At the request of the European Commission, EFSA reviewed and updated the SCF guidance on nutrient intakes in 1993 to provide policy makers with the most up-to-date scientific advice available.12 In the case of potassium, EFSA was charged with examining the PRI set by SCF12 in the context of maintaining optimal health through nutrition.15
In their review, EFSA expanded upon the meta-analysis conducted by the WHO and considered evidence for potassium’s effect on additional health end points, including cardiovascular (stroke, CHD, and CVD) end points, diabetes type 2, bone health, and kidney stones.15 A number of randomized controlled trials (RCTs), observational cohort studies, and meta-analyses were considered.
The strongest evidence was in the reduction of cardiovascular end points, particularly blood pressure and stroke. After reviewing the available evidence, EFSA concluded that there is a strong blood pressure–lowering effect of potassium in hypertensive, but not normotensive, individuals.15 Subgroup analyses revealed that the effect was greater for hypertensive individuals not on any other antihypertensive treatments and that the effect was greatest for those consuming 3500 to 4700 mg/d (90–120 mmol/d) of potassium. Although current data precluded the setting of an Average Requirement (equivalent to the United States and Canadian EAR), they determined that there were sufficient data to set the AI at 3500 mg/d (90 mmol/d). To move from the AI to a PRI, EFSA recommended further research on potassium’s interaction with other nutrients (particularly sodium and chloride) and its impact on cardiovascular end points.15
NEWER EVIDENCE TO INFORM POTASSIUM RECOMMENDATIONS
Conclusions From the AHRQ Report
A systematic review of the evidence for potassium and sodium intakes and chronic disease risk reduction was undertaken by the AHRQ7 in preparation for the DRI update panel for these nutrients. The review evaluated the evidence from potassium intervention studies on the association between potassium intake with intermediate outcomes, that is, blood pressure and kidney stone formation, or final outcomes, that is, CVD, CHD, stroke, kidney disease, and mortality.
The AHRQ report concluded there was moderate strength evidence supporting the benefit of increased potassium intake from supplements on both systolic blood pressure (SBP) and diastolic blood pressure (DBP) in adults, based on 10 parallel RCTs and 8 crossover RCTs. The report also concluded that a moderate strength of evidence exists to support the effect of increased potassium from either supplements or foods on blood pressure (both SBP and DBP) in individuals with prehypertension or hypertension based on 18 RCTs (11 parallel, 7 crossover). In contrast, a low strength of evidence, based on only 3 RCTs (2 parallel, 1 crossover), suggests that increased potassium does not affect blood pressure in normotensive individuals. The report cited insufficient evidence for the moderating effects of age, sex, race/ethnicity, comorbidities (diabetes, kidney disease, obesity), intake of other minerals (calcium, magnesium, sodium), and potassium form (potassium chloride vs others) in relation to potassium and BP. There is also insufficient evidence to suggest an effect of increased potassium intake on blood pressure in children and adolescents, nor is there sufficient evidence to suggest a reduction in the formation of kidney stones with increased potassium intake. Perhaps of most interest to the field of nutrition science, the AHRQ report found insufficient evidence on the effect of increasing potassium via dietary changes alone on blood pressure in adults. Only 3 of the 26 trials reviewed for this topic consisted of any type of dietary potassium manipulation, highlighting the need for more dietary interventions to properly answer this important question.
Dietary Potassium Intervention Trials
Numerous meta-analyses conducted over the past 30 years support the findings of the AHRQ, generally concluding that there is a positive relationship between increased potassium supplementation and a reduction in blood pressure in adults.24–28 In contrast, overall findings on the effect of increased dietary potassium intake and blood pressure have been conflicting. The majority of these systematic reviews and meta-analyses included dietary interventions and supplement trials, despite the fact that only a few dietary trials exist. Because RCTs related to dietary intake will have the greatest weight for the DRI panel recommendations, it is important to evaluate these trials separately for their scientific quality and effect size.
The 2018 AHRQ report examined the effects of potassium from both food and supplement sources.
An early dietary intervention trial29 assessed the effects of both an increase in dietary potassium and a reduction in dietary sodium on blood pressure in hypertensive individuals (DBP between 90 and 100 mm Hg) from an Australian population.29 Two hundred twelve subjects (aged 52.3 ± 0.8 years; 181 males and 31 females) were placed in 1 of the following 4 diet groups: normal diet (control), high-potassium diet (>100 mmol/3900 mg K/d), reduced-sodium diet (50–75 mmol/1150–1725 mg Na/d), or high-potassium/low-sodium diet. During the 12-week intervention, subjects were regularly counseled on how to adequately modify their food choices based on their group (eg, avoiding salt/high sodium foods or increasing fruit and vegetable intake). Both SBP and DBP were significantly reduced in each dietary intervention group compared with control subjects, but no significant differences were observed between groups. Reductions in the high-potassium group were 7.7 ± 1.1 and 4.7 ± 0.7 mm Hg for SBP and DBP, respectively. This study showed no additive effect of increased potassium and sodium reduction.
A more recent study based in the United Kingdom assessed the effects of increased potassium intake from both dietary sources and supplements on blood pressure in untreated prehypertensive individuals (DBP 80–100 mm Hg).30 In a crossover design, subjects (n = 48, 22–65 years old) completed four 6-week dietary interventions including a control diet, an additional 20 or 40 mmol K/d (780 or 1560 mg/d) from fruit and vegetables, and 40 mmol potassium citrate per day in capsule form. Similar to Chalmers and colleagues’29 study, nutrition coaching was used to regulate participant food choice during each dietary intervention with a focus on increasing fruit and vegetable intake. However, this study found no significant changes in blood pressure (ambulatory and supine blood pressure) between the control group and any of the dietary or supplement interventions. A smaller increase in dietary potassium (increase of 780–1560 mg/d compared with 3900 mg/d) as well as lower baseline blood pressure (SBP 137.7 vs >150 mm Hg, DBP 88.6 vs >95 mm Hg) may explain some of the contrasting findings between these 2 trials. The focus on only increasing dietary potassium from fruit and vegetable sources in the study of Berry et al30 compared with controlling both potassium and sodium intake in Chalmers and colleagues’29 study could also be the reason for the disparity in their findings.
However, similar to the study of Berry et al,30 Miller and colleagues31 found null results from an RCT designed to assess the effect of a potassium-focused Dietary Approaches to Stop Hypertension (DASH) diet on blood pressure in an urban African American population. Subjects (N = 123) were primarily female (71%) with controlled hypertension (SBP 120–140mmhg, DBP 80–90 mm Hg) on stable doses of antihypertensive medication. In a parallel design, the intervention group (DASH-plus) received extensive nutrition coaching geared toward increasing the purchase and consumption of high-potassium foods (eg, fruits, vegetables, beans, nuts), whereas the control group received initial instruction on how to adopt the DASH diet to improve health, but minimal dietary advice thereafter. Despite an estimated intake of 3700 mg/d of potassium (2300 mg/d over baseline), there was no significant difference in SBP (1.5 mm Hg [95% confidence interval, −2.6 to 5.6 mm Hg]; P = .48) or DBP (1.3 mm Hg [95% confidence interval, −1.3 to 3.9 mm Hg]; P = .33) in the DASH-plus intervention group compared with the control group. The authors pointed out that the lack of observed effect may have been due to medication changes, which occurred in a large percentage of participants despite a design aimed for a population on stable doses. The primary concern with studies designed around nutrition coaching is the ability of the participants to follow the diet correctly and report their dietary choices accurately. While adherence can be measured with modest accuracy in these trials (via spot urine collections in the study of Miller et al31 and 24-hour urine collection in the 2 previously mentioned studies), one of the primary limiting factors in these dietary nutrition counseling interventions is the lack of a controlled diet.
Controlled feeding interventions are almost nonexistent except for the high-quality DASH studies.32–34 The DASH intervention revealed that a dietary pattern rich in fruit and vegetables, fiber, and low-fat dairy products, with reductions in saturated and total fat and sodium, could significantly reduce blood pressure in nonmedicated hypertensive individuals compared with the average American diet.32 Although the initial DASH trial diet led to a dramatic increase in potassium consumption (DASH diet = 4101md/d, DASH combination diet [DASH diet + low-fat dairy, low saturated and total fat] = 4415 mg/d, control diet = 1752 mg/d) and reduction in blood pressure, because of other dietary modifications these beneficial effects cannot be attributed to potassium alone. In a subsequent study, the DASH collaborative research group assessed the effects of the DASH diet plus reduced dietary sodium on blood pressure. Investigators randomly assigned participants (SBP/DBP >120/80 mm Hg, not taking antihypertensive drugs) to a control diet (n = 204; aged 49 ± 10 years), similar to typical intake in the United States, or the DASH diet (n = 208; aged 47 ± 10 years), which as in the previous study aimed for a high potassium intake level (≈4700 mg/d).33 Within each diet, participants consumed foods at levels of high (150 mmol/d, 3450 mg/d), intermediate (100 mmol/d, 2300 mg/d), and low (50 mmol/d, 1150 mg/d) sodium for 30 consecutive days each, in a random-order crossover design. Researchers found that the DASH diet resulted in a significantly lower SBP at every sodium level and a significantly lower DBP at the high and intermediate sodium levels. Further, the combination of the DASH diet and low sodium lowered SBP by 11.5 and 7.1 mm Hg in participants with and without hypertension, respectively. Findings were similar in an Australian study utilizing dietary advice and sodium supplements in a crossover design to assess the effects of high versus low sodium on blood pressure in the context of a high potassium diet (≈3400 mg/d).35 Despite sodium supplementation up to 120 mmol/d (2760 mg/d), 24-hour ambulatory blood pressure and resting auscultatory SBP were reduced by 2.9 mm Hg, 1.4 mm Hg, and 5.5 mm Hg compared with baseline measurements, respectively. Low sodium reduced blood pressure more than did high-sodium diets, similar to the DASH study. The study also lacked a low potassium control arm, making it difficult to conclude if the effects were related to potassium intake.
Potassium and Bone
The AHRQ7 did not review evidence for potassium interventions or intakes and bone health outcomes. More than 200 million people worldwide suffer from osteoporosis, including 30% of postmenopausal women in both the United States and Europe.36
Cross-sectional observational studies show a consistent bone benefit with increased fruit and vegetable intakes in adolescent boys and girls,37–40 premenopausal and postmenopausal women,39,41 and elderly men and women.37,42 Higher potassium intakes have also been associated with reduced urinary calcium excretion and improvement in overall calcium balance.43 Current and past diet history was investigated in the Aberdeen Prospective Osteoporosis Screening study, looking at specific associations between mineral intake and bone outcomes in premenopausal women (aged 45–49 years, n = 994). Women who reported lower intake of fruit and vegetables during early adulthood, compared with those who reported medium or high intake, had significantly lower BMD at the lumbar spine and femoral trochanter (P < .01), although significant differences in lumbar spine, femoral neck, and femoral trochanter BMD between the lowest and highest quartiles of potassium intake were lost after adjustment for cofounding variables (age, weight, height, physical activity level, smoking, socioeconomic status; P < .06).41 However, in a second study by the same group in a similar population, women (aged 45–55 years) with lower intakes of fruits and vegetables had lower forearm BMD and higher bone resorption, with potassium intake accounting for 7.4% of the variation in forearm BMD.44
Clinical dietary intervention trials assessing the impact of potassium on bone are lacking. In an ancillary study to the main DASH trial, Lin and colleagues45 examined the effects of 2 dietary patterns (DASH vs control) and 3 sodium levels (1150, 2300, 3450 mg/d) on bone metabolism in a subset of 186 individuals (23–76 years). The DASH diet significantly reduced bone turnover from baseline (osteocalcin by 8%–11% and C-telopeptide by 16%–18%) compared with the control group, whereas a reduction in sodium intake decreased calcium excretion for both diet groups.45 Findings from potassium supplementation trials typically show persistent hypocalciuria with treatment in both men and women.43,46 In a randomized double-blind placebo-controlled study, men and women (n = 52) randomly assigned to 6 months of 60 or 90 mmol/d (2340 or 3510 mg/d) of potassium citrate supplementation had decreases in urinary calcium and net acid excretion, resulting in positive calcium balance in the group on the highest dose (90 mmol/d) compared with control (0 mmol/d).47 Serum C-telopeptide, a marker of bone turnover, also decreased significantly in both potassium groups. Similar studies have also found decreases in both net acid and calcium excretion, as well as a positive influence on bone biomarkers with increases in potassium supplementation.48,49
There have been few studies examining the relationship between potassium supplementation and BMD and/or bone microarchitecture. In a randomized, prospective controlled trial, Jehle et al50 investigated the effect of 30 mmol/d of potassium chloride versus potassium citrate on spine (L2–L4) and hip BMD in postmenopausal women (N = 161, 58.6 ± 4.8 years) for 12 months. Women taking potassium citrate showed significant increases in spine BMD from baseline at 3, 9, and 12 months, reaching an increase of 0.89% (P < .05) at month 12, whereas women in the potassium chloride group showed a decreased spine BMD of −0.98% (P < .05). In a second study, the same group examined the effect of 60 mEq‡ potassium citrate/d for 24 months on bone outcomes in 201 elderly (>65 years old) men and women. A significant 1.6% difference in spine BMD and significant improvements in trabecular thickness, trabecular number, and FRAX index score in the potassium citrate supplementation group compared with the control group showed the potential for potassium to improve bone health in the elderly.51
CONSIDERATIONS FOR REVISED RECOMMENDATIONS
Diet, Supplements, or Fortification?
Increasing potassium intake can occur through dietary choices that include potassium-rich foods or through potassium salts provided as supplements, fortifiers, or salt replacers. Which is most effective and which is most easily achieved? The AHRQ report concluded that more dietary interventions looking specifically at the effects of increasing potassium from food sources are needed to understand the effect of dietary potassium on blood pressure and other CVD outcomes. Studies need to be conducted in different subgroups to determine differential effects by sex, age, race, and those with vulnerable conditions. Design considerations influencing study quality include control and duration of the intervention and best assessment measures of exposure and outcomes. When these factors vary greatly from one study to the next, it is difficult to pool the data for meaningful interpretation. For example, the range in duration of potassium supplementation trials reviewed by the AHRQ was from 4 weeks to 36 months, compared with dietary interventions of 4 to 12 weeks. A recent analysis of the time course of diet-induced changes in blood pressure showed effects were achieved by 1 week.52 Trials with bone outcomes require long interventions (years) to see structural changes.
Giving recommendations for potassium (and sodium) on the basis of energy intake would make translation of the recommendation intakes more practical.
Recommendations in the Context of Energy
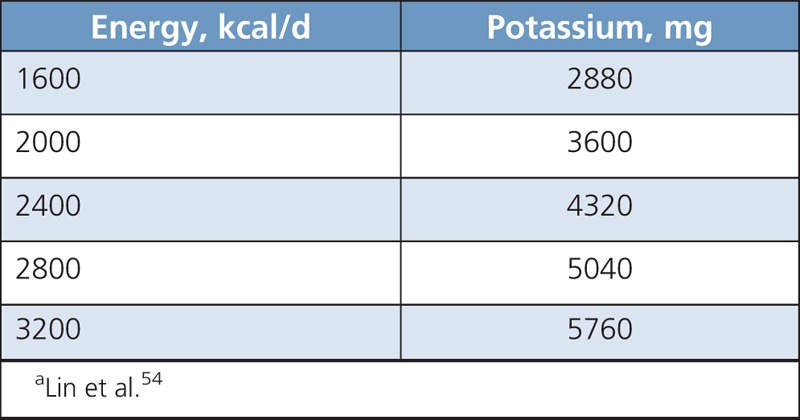
Giving recommendations for potassium (and sodium) on the basis of energy intake would make translation of the recommendation intakes more practical. Both potassium and sodium concentrations in foods are highly correlated with the energy concentration (r = 0.72 for potassium and r = 0.81 for sodium).53 Recommending a single absolute value for potassium (or sodium) intake makes meal planning difficult for families or groups in which there is a broad range of energy requirements. It may be time to consider a linear model (such as 1.8 mg/kcal for potassium) for these nutrients (Table 3).54 The DRI panel should minimally adjust recommendations for broadly different subgroups with different energy requirements, such as men versus women, adults versus children, and increased energy needs in pregnancy and lactation. This has been the approach for B vitamins, the need for which varies in proportion to energy metabolism.
TABLE 3.
Potassium Recommendations Adjusted for Energy for a Target of 1.8 mg/kcala
There is no currently accepted recommendation for Na:K intake ratio.
Potassium Versus Na:K Ratio
The 2005 DRI panel recognized that both potassium and sodium effects depend on the intake of the other electrolytes. This is logical given their interdependency and the need to keep their concentrations within narrow limits to achieve fluid balance. Dietary potassium can blunt the effect of sodium on blood pressure, but high levels of salt can blunt the hypocalciuric effect of potassium. However, the evidence for adjusting recommendations for sodium intake based on the intake of potassium and other ions or recommending a particular Na:K ratio was considered too weak. The recent AHRQ review7 concluded that there is still insufficient evidence to recommend a specific Na:K ratio.
There is no currently accepted recommendation for Na:K intake ratio. Some comparisons and suggestions are presented in Table 4.55,56 The molar ratio of the sodium UL (100 mmol) divided by the potassium AI (120 mmol) is much lower than the current average molar ratio intakes of 2.18 in US adults.5 The UL for sodium was used rather than the AI because it is the current target given the AI is not practically achievable with our food supply.57 Processed foods have added sodium as a preservative and have greatly increased the Na:K intake ratio from preagriculture revolution times.58 The range in Na:K intake is wide as discovered in the INTERSALT assessment of 32 countries. Various groups have recommended an intermediate target intake ratio between 1 and 2.
TABLE 4.
What Is the Ideal Na:K Ratio (There Is No Currently Accepted Ratio)?
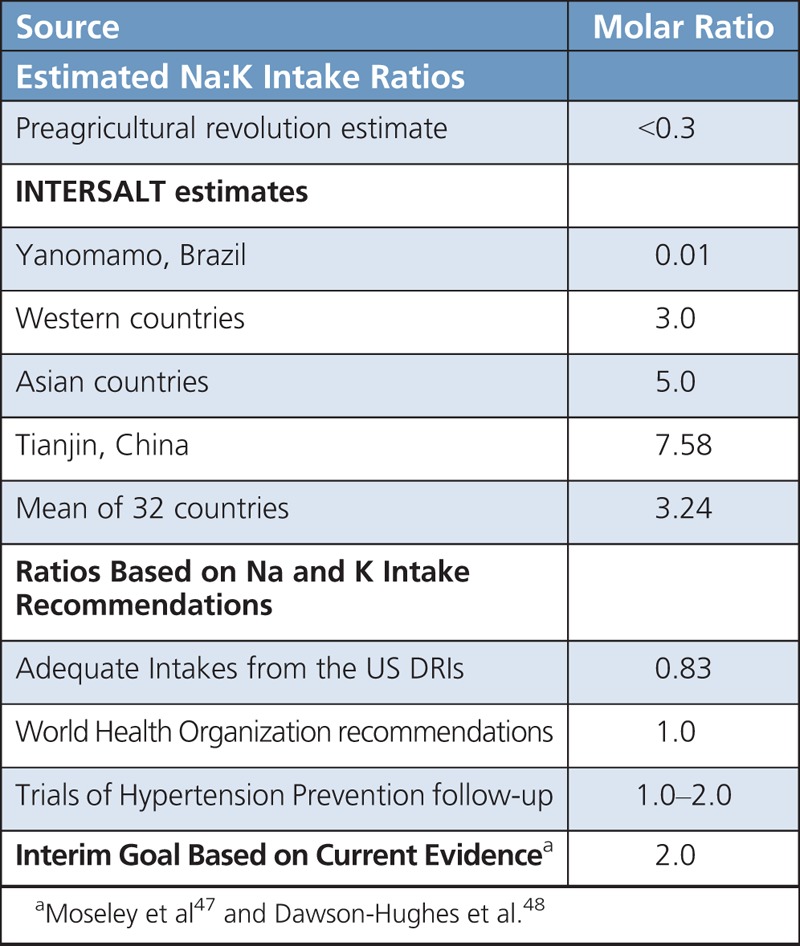
Additional reports have found positive associations between the Na:K intake ratio and blood pressure.59,60 Thus, the evidence continues to accumulate. Achieving both increased potassium and reduced sodium intakes, relative to current intakes, has significant challenges.61 It may be more practical to achieve a more moderate increase in potassium and more moderate reduction in sodium than to focus on either in isolation. This calls for research on safety and efficacy of a range in Na:K ratios.
Safety
The safety concerns with consuming potassium for the general public are few due to the kidney being able to rapidly increase its rate of excretion in response to potassium loading. The maximum excretion rate in healthy adults after adaptation to high intake was estimated to be 31.3 g (800 mmol/d),62 which is approximately 10-fold higher than the average American intake from food. The 2005 DRI committee concluded that there is no evidence that a high level of potassium from foods has adverse effects in healthy individuals and did not set a UL for potassium.4 However, the committee noted 2 areas of caution. First, potassium in supplement form can lead to acute toxicity, even in generally healthy adults. The committee based this conclusion on 4 trials conducted between 1980 and 1990, which reported gastrointestinal discomfort in healthy individuals and patients receiving 0.8 to 2.3 g (20–60 mmol/d) of supplemental potassium chloride.4
More recently, the AHRQ panel noted that, of 26 RCTs assessing the effects of potassium supplementation on blood pressure, 6 reported a greater risk of minor gastrointestinal distress.7 The administered potassium was in the form of potassium chloride in all but 1 study, which examined potassium citrate,63 and the intake level ranged from 511 to 3067 mg (20–150 mmol/d). Two of the 6 trials were conducted in healthy individuals,64,65 and one of these trials found no difference in gastrointestinal distress between the intervention and the control groups.7 The remaining 4 trials included either only adults with hypertension66–68 or only patients with abnormal renal calcium metabolism,63 in whom gastrointestinal discomfort may have been exacerbated. The AHRQ panel rated the strength of evidence for potassium-related adverse outcomes as low.
A separate meta-analysis of 22 RCTs in individuals with normal kidney function that specifically searched for and recorded all available data on potential adverse effects concluded that there were no increased adverse effects, minor complaints, or major adverse events in the increased-potassium groups compared with the control groups in both adults and children.24 The intake of potassium in these trials ranged from less than 3500 to greater than 6000 mg (<90 to >155 mmol/d) and was from both diet and supplements.
The second area of caution noted by the 2005 DRI committee was in individuals with renal impairment (patients with diabetes type 1, chronic renal insufficiency, end-stage renal disease, severe heart failure, and adrenal insufficiency), as consumption of high levels of potassium may lead to hyperkalemia (serum potassium concentration >5.5 mmol/L) and, subsequently, an increased risk of potentially lethal cardiac arrhythmias.4 This statement was based on 3 cases of hyperkalemia and 1 case of cardiac arrhythmia reported in patients taking potassium-containing salt substitutes or potassium supplements to replace potassium losses induced by spironolactone or angiotensin-converting enzyme inhibitors.4,24 In these patients, safety concerns associated with potassium supplementation require medical supervision. Otherwise, in healthy adults who are the target of any UL value, there have been no reports of hyperkalemia.4 Clinical trials including potassium supplementation as high as 15 600 mg (400 mmol/d) for several weeks and 4500 mg (115 mmol/d) for up to a year reported increased plasma concentrations but not beyond the reference range (3.5–5 mmol/L).69,70 Similar results were observed in a recent RCT comparing the bioavailability of potassium from potatoes and potassium supplement in healthy men and women. Supplementation with 2300 mg (60 mmol) of potassium gluconate added to a controlled diet containing 2300 mg (60 mmol/d) of potassium increased the plasma concentration from 3.6 to 4.1 mmol/L, but the increase was transient, lasting for approximately 4 hours, and followed immediately by increased renal potassium excretion.71 These findings suggest that the body is able to efficiently adapt to high potassium intake and that potassium supplementation may be a potential strategy to mitigate the deleterious effects of high sodium intake in Americans. Nevertheless, the adverse effects of potassium loading have not been previously evaluated in the context of diets low in sodium. Most RCTs administering potassium supplements used them in the setting of high sodium intake.4 Additional evidence is needed to determine if potassium supplements are equally safe when consumed as part of diets with low sodium-to-potassium ratio.
Additional evidence is needed to determine if potassium supplements are equally safe when consumed as part of diets with low sodium-to-potassium ratio.
MEETING THE POTASSIUM REQUIREMENT
A diet abundant in fruits and vegetables has been regarded for many years as optimal for maintaining overall health. Fruits and vegetables are rich in the minerals (ie, potassium, calcium, magnesium, etc) required for normal cardiovascular health and the development and maintenance of healthy bone and may also provide various bioactive constituents (eg, phytochemicals, including polyphenols and carotenoids) that help to further regulate favorable heart and bone health outcomes.58,72
The inadequate intake of potassium in the United States has not gone unnoticed by our federal agencies. The 2015–2020 Dietary Guidelines for Americans, which are published by the US Department of Agriculture and the Department of Health and Human Services, include a section on underconsumed nutrients and nutrients of public health concern, and one of the nutrients discussed is potassium.3 The Dietary Guidelines cite low intakes of vegetables, fruits, and dairy foods as the causative factor for low potassium intake. They recommend choosing specific fruits, vegetables, and dairy products that are high in potassium to improve intake and provide a list of such foods. The public health concern of deficient potassium intake has also been recognized by the Food and Drug Administration, which is the governing body that regulates food labeling. In 2016, they passed new regulations for the nutrition facts label on food products, which will now require that the potassium content of foods be displayed on the label.73 They cite the known link between potassium intake and blood pressure as well as the inadequate population intake of potassium as the rationale for implementing this change. The combined efforts of the US Department of Agriculture/Department of Health and Human Services and the Food and Drug Administration in promoting awareness of potassium intake for the public are important steps in increasing intake to align with the AI.
CONCLUSIONS
There is still much to learn about the effect of dietary potassium, both alone and in the context of the whole diet, on overall health. Improving the evidence for efficacy and safety for all population groups is needed to refine intake recommendations and public health messages, as well as to strategize how to best achieve increased levels in our diet.
Evidence is substantial for a benefit of potassium between 3500 and 4700 mg/d for lowering blood pressure. However, further discrimination within this range (or even lower) to recommend intakes greater than 3500 mg/d is not possible with existing data. Recommendations that consider differences in intake due to energy needs, racial differences in metabolism, and intake of other minerals, especially sodium, would be more practically translatable and should be a continuous emphasis of further research.

No caption available
No caption available
*A strong recommendation indicates the “development group is confident that the desirable effects of adherence outweigh the undesirable effects.” In addition, a strong recommendation means that most patients would benefit from following this guidance, clinicians should give this advice to their patients, and policy makers can adopt these guidelines in most situations.
†A conditional recommendation indicates the “development group is not confident about the trade-off.” Conditional recommendations imply that many patients would benefit from following this advice, although many will not, and policy makers must involve stakeholders before adopting the recommendation as policy.
‡mEq = mmol for potassium.
Funding Source: PHS U01HL117835.
C.M.W. is on the advisory boards of the International Life Sciences Institute and YINI and has research grants from the Alliance for Potato Research and Education, Dairy Management Incorporated, and National Institutes of Health.
REFERENCES
- 1.Dietary Guidelines Advisory Committee. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2005. Washington, DC: US Department of Agriculture, Agricultural Research Service; 2004. [Google Scholar]
- 2.Dietary Guidelines Advisory Committee. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2010. Washington, DC: US Department of Agriculture, Agricultural Research Service; 2011. [Google Scholar]
- 3.US Department of Health and Human Services and US Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. 8th ed. December 2015. http://health.gov/dietaryguidelines/2015/guidelines/. Accessed June 7, 2018.
- 4.Food and Nutrition Board, Institute of Medicine. Sodium and chloride. In: Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate. Washington, DC: National Academies Press; 2005:269–423. [Google Scholar]
- 5.Bailey RL, Parker EA, Rhodes DG, et al. Estimating sodium and potassium intakes and their ratio in the American diet: data from the 2011–2012 NHANES. J Nutr. 146:745–750. 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cogswell ME, Loria CM, Terry AL, et al. Estimated 24-hour urinary sodium and potassium excretion in us adults. JAMA 2018; 319(12):1209–1220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Newberry SJ, Chung M, Anderson CAM, et al. Sodium and Potassium Intake: Effects on Chronic Disease Outcomes and Risks. Comparative Effectiveness Review No. 206. (Prepared by the RAND Southern California Evidence-based Practice Center under Contract No. 290-2015-00010-I.) AHRQ Publication No. 18-EHC009-EF. Rockville, MD: Agency for Healthcare Research and Quality; 2018. https://doi.org/10.23970/AHRQEPCCER206. Accessed July 22, 2018. [PubMed] [Google Scholar]
- 8.National Institutes of Health, Office of Dietary Supplements. Potassium: Fact Sheet for Health Professionals. Current version March 21, 2018. https://ods.od.nih.gov/factsheets/Potassium-HealthProfessional/. Accessed July 19, 2018.
- 9.Lopes AD, Mathers CD. Measuring the global burden of disease and epidemiological transitions: 2002–2030. Ann Trop Med Parasitol. 2006;100(5–6):481–499. [DOI] [PubMed] [Google Scholar]
- 10.Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke status—2017 update: a report from the American Heart Association. Circulation 2017; 135:e146–e603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Morris RC, Jr, Sebastian A, Forman A, Tanaka M, Schmidlin O. Normotensive salt sensitivity: effects of race and dietary potassium. Hypertension. 1999;33:18–23. [DOI] [PubMed] [Google Scholar]
- 12.SCF, Nutrient and energy intakes for the European Community. In: Food—Science and Technique. Luxembourg: European Commission; 1993:248. [Google Scholar]
- 13.WHO, Diet, Nutrition and the Prevention of Chronic Disease: Report of a Joint WHO/FAO Expert Consultation. WHO Technical Report Series 916. Geneva, Switzerland: World Health Organization; 2003. [PubMed] [Google Scholar]
- 14.World Health Organization. Guideline: Potassium Intake for Adults and Children. Geneva, Switzerland: World Health Organization; 2012. [PubMed] [Google Scholar]
- 15.EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Turck D, Bresson J-L, Burlingame B, et al. Dietary reference values for potassium. EFSA J. 2016; 14:4592. [Google Scholar]
- 16.Strohm D, Ellinger S, Leschik-Bonnet E, Maretzke F, Heseker H. German Nutr Soc (DGE). Revised reference values for potassium intake. Annals Nutr Metab. 2017;71:118–124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Asakura K, Uechi K, Sasaki Y, Masayasu S, Sasaki S. Estimation of sodium and potassium intakes assessed by two 24 h urine collections in healthy Japanese adults: a nationwide study. Br J Nutr. 2014;112(7):1195–1205. [DOI] [PubMed] [Google Scholar]
- 18.Du SF, Wang H, Batis C, Zhang B, Zhang J, Popkin BM. Understanding the patterns and trends of sodium intake, potassium intake, and sodium to potassium ratio and their effect on hypertension in China. Am J Clin Nutr. 2014;99(2):334–343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.van Mierlo LA, Greyling A, Zock PL, et al. Suboptimal potassium intake and potential impact on population blood pressure. Arch Intern Med 2010, 170(16):1501–1502. [DOI] [PubMed] [Google Scholar]
- 20.Cogswell ME, Zhang ZF, Carriquiry AL, et al. Sodium and potassium intakes among US adults: NHANES 2003–2008. Am J Clin Nutr 2012; 96(3):647–657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lee HS, Duffey KJ, Popkin BM. Sodium and potassium intake patterns and trends in South Korea. J Hum Hypertens. 2013;27(5):298–303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Boylan S, Welch A, Pikhart H, et al. Dietary habits in three Central and Eastern European countries: the HAPIEE study. BMC Public Health 2009; 9:439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Welch AA, Fransen H, Jenab M, et al. Variation in intakes of calcium, phosphorus, magnesium, iron and potassium in 10 countries in the European Prospective Investigation into Cancer and Nutrition study. Eur J Clin Nutr 2009; 63:S101–S121. [DOI] [PubMed] [Google Scholar]
- 24.Aburto NJ, Hanson S, Gutierrez H, Hooper L, Elliott P, Cappuccio FP. Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses. Br Med J. 2013;346:f1378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Whelton PK, He J, Cutler JA, et al. Effects of oral potassium on blood pressure. Meta-analysis of randomized controlled clinical trials. JAMA 1997, 277(20):1624–1632. [DOI] [PubMed] [Google Scholar]
- 26.Cappuccio FP, MacGregor GA. Does potassium supplementation lower blood pressure? A meta-analysis of published trials. J Hypertens. 1991;9(5):465–473. [DOI] [PubMed] [Google Scholar]
- 27.Geleijnse JM, Kok FJ, Grobbee DE. Blood pressure response to changes in sodium and potassium intake: a metaregression analysis of randomised trials. J Hum Hypertens. 2003;17(7):471–480. [DOI] [PubMed] [Google Scholar]
- 28.Binia A, Jaeger J, Hu Y, Singh A, Zimmermann D. Daily potassium intake and sodium-to-potassium ratio in the reduction of blood pressure: a meta-analysis of randomized controlled trials. J Hypertens. 2015;33(8):1509–1520. [DOI] [PubMed] [Google Scholar]
- 29.Chalmers J, Morgan T, Doyle A, et al. Australian National Health and Medical Research Council dietary salt study in mild hypertension. J Hyperten. 1986;4(6):S629–S637. [PubMed] [Google Scholar]
- 30.Berry SE, Mulla UZ, Chowienczyk PJ, Sanders TA. Increased potassium intake from fruit and vegetables or supplements does not lower blood pressure or improve vascular function in UK men and women with early hypertension: a randomised controlled trial. Br J Nutr. 2010;104(12):1839–1847. [DOI] [PubMed] [Google Scholar]
- 31.Miller ER, 3rd, Cooper LA, Carson KA, et al. A dietary intervention in urban African Americans: results of the “Five Plus Nuts and Beans” randomized trial. Am J Prev Med. Jan 2016;50(1):87–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Appel LJ, Moore TJ, Obarzanek E, et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med. 1997;336(16):1117–1124. [DOI] [PubMed] [Google Scholar]
- 33.Sacks FM, Svetkey LP, Vollmer WM, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet DASH-Sodium Collaborative Research Group. N Engl J Med. 2001;344(1):3–10. [DOI] [PubMed] [Google Scholar]
- 34.Svetkey LP, Simons-Morton DG, Proschan MA, et al. Effect of the dietary approaches to stop hypertension diet and reduced sodium intake on blood pressure control. J Clin Hypertens (Greenwich). 2004;6(7):373–381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Nowson CA, Morgan TO, Gibbons C. Decreasing dietary sodium while following a self-selected potassium-rich diet reduces blood pressure. J Nutr. 2003;133(12):4118–4123. [DOI] [PubMed] [Google Scholar]
- 36.Sözen T, Özişik L, Başaran NÇ. An overview and management of osteoporosis. Eur J Rheumatol. 2017;4(1):46–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Prynne CJ, Mishra GD, O’Connell MA, et al. Fruit and vegetable intakes and bone mineral status: a cross sectional study in 5 age and sex cohorts. Am J Clin Nutr. 2006; 83(6):1420–1428. [DOI] [PubMed] [Google Scholar]
- 38.Tylavsky FA, Holliday K, Danish R, Womack C, Norwood J, Carbone L. Fruit and vegetable intakes are an independent predictor of bone size in early pubertal children. Am J Clin Nutr. 2004;79(2):311–317. [DOI] [PubMed] [Google Scholar]
- 39.Li JJ, Huang ZW, Wang RQ, et al. Fruit and vegetable intake and bone mass in Chinese adolescents, young and postmenopausal women. Public Health Nutr. 2013; 16(1):78–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Vatanparast H, Baxter-Jones A, Faulkner RA, Bailey DA, Whiting SJ. Positive effects of vegetable and fruit consumption and calcium intake on bone mineral accrual in boys during growth from childhood to adolescence: the University of Saskatchewan Pediatric Bone Mineral Accrual Study. Am J Clin Nutr. 2005;82(3):700–706. [DOI] [PubMed] [Google Scholar]
- 41.New SA, Bolton-Smith C, Grubb DA, Reid DM. Nutritional influences on bone mineral density: a cross-sectional study in premenopausal women. Am J Clin Nutr. 1997;65(6):1831–1839. [DOI] [PubMed] [Google Scholar]
- 42.Tucker KL, Hannan MT, Chen H, Cupples LA, Wilson PW, Kiel DP. Potassium, magnesium, and fruit and vegetable intakes are associated with greater bone mineral density in elderly men and women. Am J Clin Nutr. 1999;69(4):727–736. [DOI] [PubMed] [Google Scholar]
- 43.Frassetto L, Morris RC, Jr, Sebastian A. Long-term persistence of the urine calcium-lowering effect of potassium bicarbonate in postmenopausal women. J Clin Endocrin Metab. 2005;90(2):831–834. [DOI] [PubMed] [Google Scholar]
- 44.New SA, Robins SP, Campbell MK, et al. Dietary influences on bone mass and bone metabolism: further evidence of a positive link between fruit and vegetable consumption and bone health? Am J Clin Nutr 2000, 71(1):142–151. [DOI] [PubMed] [Google Scholar]
- 45.Lin PH, Ginty F, Appel LJ, et al. The DASH diet and sodium reduction improve markers of bone turnover and calcium metabolism in adults. J Clin Nutr 2003; 133(10):3130–3136. [DOI] [PubMed] [Google Scholar]
- 46.Lemann J, Jr, Gray RW, Pleuss JA. Potassium bicarbonate, but not sodium bicarbonate, reduces urinary calcium excretion and improves calcium balance in healthy men. Kidney Intl. 1989;35(2):688–695. [DOI] [PubMed] [Google Scholar]
- 47.Moseley KF, Weaver CM, Appel L, Sebastian A, Sellmeyer DE. Potassium citrate supplementation results in sustained improvement in calcium balance in older men and women. J Bone Miner Res. 2013;28(3):497–504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dawson-Hughes B, Harris SS, Palermo NJ, Castaneda-Sceppa C, Rasmussen HM, Dallal GE. Treatment with potassium bicarbonate lowers calcium excretion and bone resorption in older men and women. J Clin Endocrinol Metab. 2009;94(1):96–102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Marangella M, Di Stefano M, Casalis S, Berutti S, D’Amelio P, Isaia GC. Effects of potassium citrate supplementation on bone metabolism. Calcif Tissue Int. 2004;74(4):330–335. [DOI] [PubMed] [Google Scholar]
- 50.Jehle S, Zanetti A, Muser J, Hulter HN, Krapf R. Partial neutralization of the acidogenic Western diet with potassium citrate increases bone mass in postmenopausal women with osteopenia. J Am Soc Nephrol. 2006;17(11):3213–3222. [DOI] [PubMed] [Google Scholar]
- 51.Jehle S, Hulter HN, Krapf R. Effect of potassium citrate on bone density, microarchitecture, and fracture risk in healthy older adults without osteoporosis: a randomized controlled trial. J Clin Endocrinol Metab. 2013;98(1):207–217. [DOI] [PubMed] [Google Scholar]
- 52.Juraschek SP, Woodward M, Sacks FM, Carey VJ, Miller ER, (III), Appel LJ. Time course of change in blood pressure from sodium reduction and the DASH diet. Clin Trial Reg 2017, 70:923–929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Drewnowski A, Maillot M, Rehm C. Reducing the sodium-potassium ratio in the US diet: a challenge for public health. Am J Clin Nutr. 2012;96:439–444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Lin PH, Windhauser MM, Plaisted CS, Hoben KP, McCullough ML, Obarzanek E. for the DASH Collaborative Research Group. The linear index model for establishing nutrient goals for the Dietary Approaches to Stop Hypertension trial. J Am Diet Assoc. 1999;99(suppl):S40–S44. [DOI] [PubMed] [Google Scholar]
- 55.Iwahori T, Miura K, Ueshima H. Time to consider use of the sodium-to-potassium ratio for practical sodium reduction and potassium increase. Nutrients. 2017;9:700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Burmier M. Should we eat more potassium to better control blood pressure in hypertension? [published online ahead of print January 2, 2018]. Nephrol Dial Transplant. 2018. [DOI] [PubMed] [Google Scholar]
- 57.Institute of Medicine. Sodium Intake and Populations: Assessment of Evidence. Washington DC: The National Academies Press; 2013. [Google Scholar]
- 58.Weaver CM. Potassium and health. Adv Nutr. 2013;4(3):368S–377S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Stamler J, Chan Q, Daviglus ML, et al. Relation of dietary sodium (salt) to blood pressure and its possible modulation by other dietary factors: the INTERMAP study. Hypertension 2018, 71:631–637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Weaver CM, Bailey FL, McCabe LD, et al. Mineral intake ratios are significant, but weak predictors of blood pressure in US adults. J Nutr. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Drewnowski A, Maillot M, Rehm C. Reducing the sodium-potassium ratio in the US diet: a challenge for public health. Am J Clin Nutr. 2012;96:43–444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Berliner RW, Kennedy TJ, Jr, Hilton JG. Renal mechanisms for excretion of potassium. Am J Physiol. 1950;162(2):348–367. [DOI] [PubMed] [Google Scholar]
- 63.Barcelo P, Wuhl O, Servitge E, Rousaud A, Pak CY. Randomized double-blind study of potassium citrate in idiopathic hypocitraturic calcium nephrolithiasis. J Urol. 1993;150(6):1761–1764. [DOI] [PubMed] [Google Scholar]
- 64.Naismith DJ, Braschi A. The effect of low-dose potassium supplementation on blood pressure in apparently healthy volunteers. Br J Nutr. 2003;90(1):53–60. [DOI] [PubMed] [Google Scholar]
- 65.Graham UM, McCance DR, Young IS, Mullan KR. A randomised controlled trial evaluating the effect of potassium supplementation on vascular function and the renin-angiotensin-aldosterone system. J Hum Hypertens. 2014;28(5):333–339. [DOI] [PubMed] [Google Scholar]
- 66.Bulpitt CJ, Ferrier G, Lewis PJ, Daymond M, Bulpitt PF, Dollery CT. Potassium supplementation fails to lower blood pressure in hypertensive patients receiving a potassium losing diuretic. Ann Clin Res. 1985;17(4):126–130. [PubMed] [Google Scholar]
- 67.Patki PS, Singh J, Gokhale SV, Bulakh PM, Shrotri DS, Patwardhan B. Efficacy of potassium and magnesium in essential hypertension: a double-blind, placebo controlled, crossover study. Br Med J. 1990;301(6751):521–523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Svetkey LP, Yarger WE, Feussner JR, DeLong E, Klotman PE. Double-blind, placebo-controlled trial of potassium chloride in the treatment of mild hypertension. Hypertension. 1987;9(5):444–450. [DOI] [PubMed] [Google Scholar]
- 69.Siani A, Strazzullo P, Giacco A, Pacioni D, Celentano E, Mancini M. Increasing the dietary potassium intake reduces the need for antihypertensive medication. Ann Intern Med. 1991;115(10):753–759. [DOI] [PubMed] [Google Scholar]
- 70.Rabelink TJ, Koomans HA, Hene RJ, Dorhout Mees EJ. Early and late adjustment to potassium loading in humans. Kidney Int. 1990;38(5):942–947. [DOI] [PubMed] [Google Scholar]
- 71.Macdonald-Clarke CJ, Martin BR, McCabe LD, et al. Bioavailability of potassium from potatoes and potassium gluconate: a randomized dose response trial. Am J Clin Nutr. 2016, 104(2):346–353. [DOI] [PubMed] [Google Scholar]
- 72.Mühlbauer RC, Lozano A, Reinli A. Onion and a mixture of vegetables, salads, and herbs affect bone resorption in the rat by a mechanism independent of their base excess. J Bone Min Res. 2002;17(7):1230–1236. [DOI] [PubMed] [Google Scholar]
- 73.Department of Health and Human Services, Food and Drug Administration. Food labeling: revision of the nutrition and supplement facts labels; serving sizes of foods that can reasonably be consumed at one eating occasion; dual-column labeling; updating, modifying, and establishing certain reference amounts customarily consumed; serving size for breath mints; and technical amendments; final rules. Fed Regist. 2016;81(103):33742–33999. [PubMed] [Google Scholar]