

Abstract
Introduction
Surgical treatment of condylar neck fractures requires an extraoral approach when, due to the degree of difficulty of the fracture, an intraoral approach or an endoscopically supported treatment is not possible. In contrast to the cosmetically more favorable oral approach, extraoral approaches offer a better overview of the operating field and thus an easier fracture repositioning and osteosynthetic treatment. In 2007, Marti et al. described a minimal pre- and retroauricular incision with no extension to the hair-bearing skin and which aimed to improve the parotidectomy approach.
Materials and Methods
We present two cases in which minimal incision was used as a surgical approach for treatment of the condylar neck.
Discussion
Using the minimal incision, we were able to access the condylar neck. This type of approach as well as having the advantages of an open approach makes it possible to conceal the scar in the periauricular region and reduce the likelihood of salivary fistula.
Keywords: Mandibular condyle, Mandibular fracture, Surgical treatment, Surgical approach
Surgical treatment of condylar neck fractures requires an extraoral approach when, due to the degree of difficulty of the fracture, an intraoral approach or an endoscopically supported treatment is not possible. In contrast with the cosmetically more favorable oral approach, extraoral approaches offer a better overview of the operating field and thus an easier fracture repositioning and osteosynthetic treatment [1].
In 2007, Marti et al. described a minimal pre- and retroauricular incision with no extension to the hair-bearing skin and which aimed to improve the parotidectomy approach. The aim of this approach is to reduce dissection of areas outside the surgical field, shorten time of surgery, and reduce postoperative complications [2]. This method also has superior aesthetic outcomes compared to classic facelift approaches for parotidectomy [2].
We present two cases in which minimal incision was used as a surgical technique for treatment of the condylar neck. The first was a case of bilateral condylar fracture, for which we used the classic transparotid approach on one side (case 1), while the minimal incision technique was applied on the contralateral side. In the second case, we used the approach to remove a plate that had been placed on the condylar neck.
Surgical Technique
Surgery is performed under general anesthesia. Incision starts along the internal face of the tragus. It continues inferiorly anterior to the ear and is curved, separated by 1 mm from the lobule. The incision rises 2 mm away from the crease behind the conchal cartilage and ends at the level of the middle of the ear (Fig. 1). Dissection of the parotid skin flap in the subcutaneous plane is then performed. The posterior branch of the greater auricular nerve is identified and preserved. Afterward, an SMAS flap is elevated inferiorly to reach the condyle.
Fig. 1.
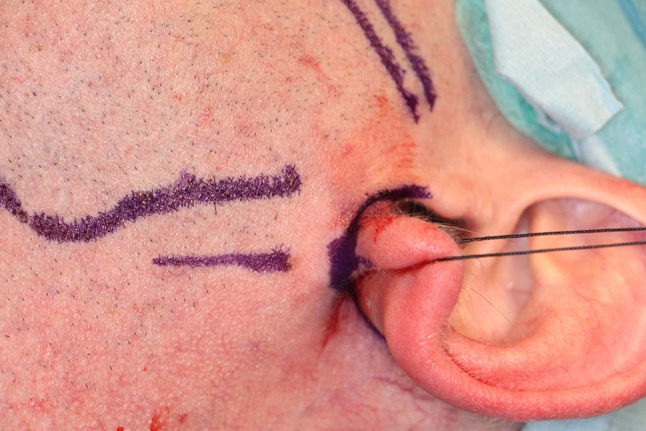
Case 1: the operative path of the minimal incision is marked around the earlobe. The lower horizontal line marks the incision used for the classic transparotid approach, while the upper line traces the posterior border of the mandibular ramus
The capsule of the parotid gland is incised. To protect the branches of the facial nerve, the parotid capsule is cut parallel to it. Further preparation via the parotid gland up to the muscle masseter is executed bluntly and also parallel to the path of the branch of the facial nerve. After incision and displacement of the m. masseter, the periosteum is exposed. This is cut at the trailing edge of the R. mandibulae and the ascending mandibular branch and the condylar neck region are exposed. After an anatomically correct repositioning of the fracture, osteosynthesis is fixed (Fig. 2). The wound is subsequently closed layer by layer including isolating suture of the parotid capsule (Fig. 3a–c)
Fig. 2.

Case 1: surgical field obtained using the minimal incision approach. Osteosynthesis of the condylar fracture using 2 2.0-mm titanium plates. The caudal part of the approach reveals a preserved greater auricular nerve
Fig. 3.
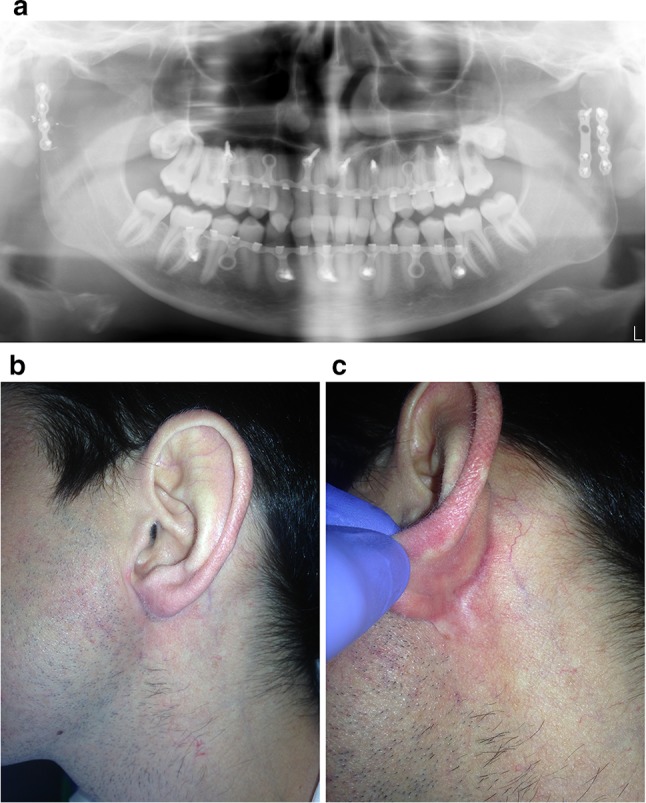
Case 1: a panoramic radiograph of the postoperative phase: the image shows the hybrid system used for intermaxillary fixation and to guide postoperative occlusion. Two 2.0-mm plates used for osteosynthesis in the left condyle and a 2.0-mm plate for osteosynthesis in the right condyle; b, c appearance of the scars 1 year postoperatively
Using the minimal incision, we were able to access the condylar neck, eliminating the need for a retromandibular incision and posterior loading included in the facelift approach. This type of incision makes it possible to conceal the scar in the periauricular region and reduce the likelihood of salivary fistula, as in addition to suturing the parotid gland capsule, a flap is raised from the SMAS, which is later repositioned to form a barrier.
This approach may be an attractive alternative to the approaches for condyle fractures.
Acknowledgements
The author thanks Oliver Shaw (IIS-FJD) for editing the report for aspects related to the English language.
References
- 1.Weingart D. The transparotideal approach. In: Kleinheinz J, Meyer C, editors. Fractures of the mandibular condyle. Basic considerations and treatment. New Malden: Quintessence Publishing Co Ltd; 2009. p. 135. [Google Scholar]
- 2.Martí-Pagès C, García-Díez E, García-Arana L, Mair D, Biosca MJ, Gimeno-Medina X, Hernández-Alfaro F. Minimal incision in parotidectomy. Int J Oral Maxillofac Surg. 2007;36:72. doi: 10.1016/j.ijom.2006.09.008. [DOI] [PubMed] [Google Scholar]