

Abstract
Introduction
Various methods are deployed by an oral and maxillofacial surgeon to control the osteotomised/ fractured bony segments intraoperatively till the time a stable fixation in the desired position is achieved. Few of these include the use of bone holding crocodile forceps, towel clips, reduction forceps, wires, digital control (Thota and Mitchell in Br J Orthod 26(4):325, 1999). In our technique, we present the use of an IMF screw to manipulate bony segments intraoperatively.
Materials and Methods
We used this novel technique in a series of 12 patients. An IMF screw was fixed in the greatest bulk of the bony fragment so as to control it and hold it in the desired position in various surgical procedures.
Conclusion
This technique was found to be minimally invasive and easy to perform to achieve a good hold and control of the bony segments.
Keywords: IMF, Screws, Bony segments
In a series of 12 patients, this novel technique was utilized for various purposes. An IMF screw was fixed in the greatest bulk of the bony fragment (osteotomized bony segment, segment of comminuted fractures, traction of fragments, etc.) so as to control it and hold it in the desired position. This technique was found to be minimally invasive and easy to perform to achieve a good hold and control of the bony segment/segments. When compared with other methods to achieve the same purpose such as the use of reduction forceps or towel clips where a two-point control is required or by use of a crocodile forceps wherein a large surface area is covered or manual control, it is noted that these methods are very subjective and a usual fatigue of the operator/assistant’s hand can lead to a complete loss of the desired goal. Whereas the use of IMF screws in different types of cases such as:
Retrieval, control and manipulation of the proximal fragment in condylar fractures (3 cases)—to hold the fragments in anatomically reduced position until final fixation is done (Fig. 1).
Malunited collapsed mandibular fractures of symphysis/parasymphysis (4 cases)—1 IML screw on either side in the body region between the tooth roots above the nerve through which a wire is passed is used to manually distract the fragments and hold them in functional occlusion until IML is done.
Genioplasty (3 cases)—to manipulate, position and hold the advancement segment until final plate fixation is done (Fig. 2).
Le Fort I Osteotomy (2 cases)—1 screw below ANS with a wire passed through it as well as one wire each is passed through the orthodontic molar brackets on either side. These 3 wires help in manual manipulation of the segment for advancement and controlling the Yaw.
Fig. 1.
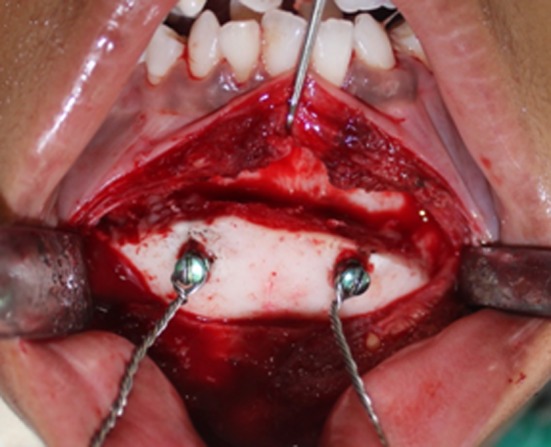
Two IML screws in the chin for the purpose of controlled advancement during genioplasty
Fig. 2.

One IML screw in the fractured condyle fragment for proper reduction
These above uses of IML screws were found to be very reliable, minimally invasive and highly effective. Besides, the IMF screw is readily available and cost-effective easy and simple to apply and an effective technique [2]. The screw is removed once the bony fragments are fixed, and it leaves only a residual single monocortical hole of 2 mm which heals uneventfully eventually. Another variation is the use of a self tapping variant of IMF screw that allows it to be directly threaded to control the bony segment.
We recommend the use of this effective technique whenever such situations are encountered by surgeons.
Compliance with Ethical Standards
Conflict of interest
None.
Contributor Information
Neelam N. Andrade, Email: drnnandrade@gmail.co, Email: drnnadrade@yahoo.co.in
Smriti S. Choradia, Email: smritibora@gmail.com
Neha Aggarwal, Email: agg_neha1989@yahoo.co.in.
Paul C. Mathai, Email: paulmathai89@gmail.com
References
- 1.Thota LG, Mitchell DA. Cortical bone screws for maxillomandibular fixation in orthognathic surgery. Br J Orthod. 1999;26(4):325. doi: 10.1093/ortho/26.4.325. [DOI] [PubMed] [Google Scholar]
- 2.Roccia F, Tavolaccini A, Dell’Acqua A, Fasolis M. An audit of mandibular fractures treated by intermaxillary fixation using intraoral cortical bone screws. J Craniomaxillofac Surg. 2005;33(4):251–254. doi: 10.1016/j.jcms.2005.02.005. [DOI] [PubMed] [Google Scholar]