

Abstract
BACKGROUND:
Multinodular and Vacuolating Neuronal Tumor (MVNT) of the cerebrum is a benign lesion described recently in the WHO CNS tumours in 2016. Although this tumour is uncommon, clinicians should be acquainted with the possible presentation and imaging findings.
CASE REPORT:
We present a case of a young gentleman whose only symptom was absence seizures. Brain imaging showed lesions, compatible with this rare diagnosis.
CONCLUSION:
Our description of imaging findings on MRI highlights the characteristic cystic appearances of note in the right occipital lobe, in contrast to the temporal lobe as the predominant location found in previous cases.
Keywords: MVNT, DWI, FLAIR, MRI, CNS tumours
Introduction
Multinodular and Vacuolating Neuronal Tumor (MVNT) of the cerebrum is a rare benign distinct entity included in the WHO 2016 Central Nervous System (CNS) tumours [1].
Case report
A 33-year-old Caucasian gentleman presented with absence seizures. No other relevant symptoms, signs, medical, surgical nor drug history of note.
Brain MRI revealed multiple small cystic lesions, involving the cortex and subcortical white matter (Figures 1 and 2) of the right occipital lobe. The gadolinium-enhanced examination was performed which showed no pathological enhancement. A repeat MRI eight months later demonstrated no significant changes verifying stability with time. The radiological findings were compatible with multinodular and vacuolating neuronal tumour (MVNT) of the cerebrum [2].
Figure 1.
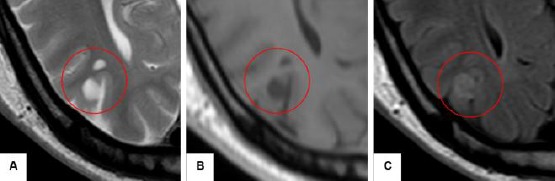
(A) T2-weighted (B) T1-weighted and (C) Fluid-attenuated inversion recovery (FLAIR) MRI. There are multiple well-defined cortical-based lesions. These appear hyperintense on T2-weighted and FLAIR imaging and are hypointense on T1-weighted sequences. No associated vasogenic oedema or mass effect is seen
Figure 2.
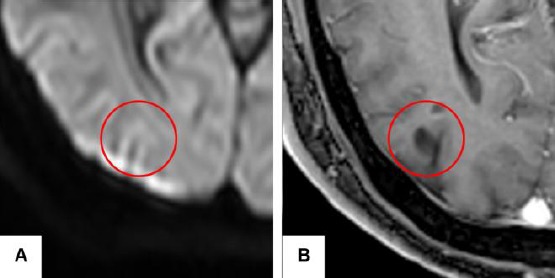
(A) Diffusion-weighted Imaging and (B) contrast enhanced T1 weighted sequences. The lesion does not restrict diffusion, and there is no pathological contrast uptake
This case was discussed at the neurology multidisciplinary team meeting. Only surveillance imaging was needed given its benign nature and stability over time.
Discussion
MVNT, recently included in the WHO 2016 classification of CNS tumours [1], is a rare benign, multinodular, non-neurocyte, glial/neuronal lesion with a unique membrane-bound appearance of the neuronal cytoplasm. Lesions have a round to elliptic shape, are between 1 mm to 5 mm in size and can be found as separate entities or in clusters. Due to its indeterminate pathological nature, characterisation is debatable as the entity shares features of a developmental abnormality and neoplasm, but behaves more like the former [2]. First described by Huse et al., these tumours do not show gender predisposition, may be associated with seizure activity of adult onset or unpredictable neurological deficiency and predominantly occur in the temporal lobe [3].
MRI is the gold-standard diagnostic test as no abnormalities are usually seen on CT scans unless the lesion is large. On MRI, the tumour appears as a non-contrast enhancing, T2/FLAIR hyperintense with the absence of restricted diffusion, no mass effect or encompassing oedema nor observable calcification. On T1 weighted imaging, lesions range from isointense to hypointense.
Only a few cases of this uncommon tumour have been published so far, all presenting with similar clinical presentation and type of localisation. This uncommon tumour of heterogeneous lineage may be confounded with other more frequent lesions including DNET and gliomas; however the former involves more cortical thickening while the latter show more cortical diffusion [2] [3].
In conclusion: (i) multinodular and vacuolating neuronal tumour (MVNT) of the cerebrum, is a new neuronal cytoplasmic pattern described in the WHO of CNS tumors 2016; (ii) lesions are benign, multinodular, well circumscribed, non-contrast enhancing, T2/FLAIR hyperintense, involving the cortex and superficial white matter, with absence of restricted diffusion and mass effect; and (iii) MVNT may or may not be symptomatic and may be found incidentally. DNET is the most common differential diagnosis.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System:a summary. Acta Neuropathol. 2016;131:803–820. doi: 10.1007/s00401-016-1545-1. https://doi.org/10.1007/s00401-016-1545-1 PMid:27157931. [DOI] [PubMed] [Google Scholar]
- 2.Nunes RH, Hsu CC2, da Rocha AJ, et al. Multinodular and Vacuolating Neuronal Tumor of the Cerebrum:A New “Leave Me Alone” Lesion with a Characteristic Imaging Pattern. AJNR Am J Neuroradiol. 2017 doi: 10.3174/ajnr.A5281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Huse JT, Edgar M, Halliday J, Mikolaenko I, Lavi E, Rosenblum MK. Multinodular and vacuolating neuronal tumours of the cerebrum:10 cases of a distinctive seizure-associated lesion. Brain Pathol. 2013;23:515–24. doi: 10.1111/bpa.12035. https://doi.org/10.1111/bpa.12035 PMid:23324039. [DOI] [PMC free article] [PubMed] [Google Scholar]