

Abstract
BACKGROUND:
Gunshot wounds and blast injuries to the upper limbs produce complex wounds requiring management by multiple surgical specialities.
AIM:
We sought to determine the pattern of peripheral nerve injuries among Iraqi soldiers in the war.
METHODS:
We performed a 3 year retrospective cohort analysis based on medical records of patients with sustaining gunshot wounds and blast injuries to the upper limbs. Ethical approval was obtained from the institutional review board. The patients included were male, serving military personnel of all age groups and ranks presenting with weakness or sensory loss of radial nerve. Three hundred eighteen patients aged 24 years or older with a high-energy, diaphyseal fracture of the humerus and complete motor and sensory radial nerve palsy were reviewed retrospectively. In these patients, the physical examination and electrodiagnostic study were carried out by experienced neurologists. Seddon’s classification system was used to assess the severity of the injury. The data related to the types of fracture, the type of damage, the factors causing damage and the failure of treatment were entered into the IBM SPSS 23 software after extraction of files. Based on mid-range indicators and data distribution, traumatic injuries among Iraqi soldiers in the war against ISIL were then investigated.
RESULTS:
A group of 318 patients with mean age of 25.41 ± 6 years were enrolled in the study, of which 127 patients were included with an open fracture and 191 patients with closed lesions. All 127 patients with a transected radial nerve had an open humerus fracture and were part of a complex upper-extremity injury. 113 of 127 subjects had primary repair of the radial nerve and recovered well. 14 of 127 subjects were not recovered. 3 of them had iatrogenic radial nerve injury due to the internal fixation device. Furthermore, all 191 patients with closed injuries recovered well. The average time to initial signs of recovery was 8 weeks (range, 1–27 weeks). Axonotmesis and Neurotmesis were found in 283 (89%) subjects. The average time to full recovery was determined to be 6 months (range, 1–22 months). The blast was found to be the main cause of nerve injury in 236 (74.2%) cases, followed by gunshot damage (21.4%, 68 subjects), falling from height and motor vehicle accidents (4.4%, 14 subjects) and multiple injuries (17%, 54 cases).
CONCLUSIONS:
Trauma caused by factors such as explosions and gunshot worsens the condition of the injuries and presents the treatment conditions with many challenges. However, the success rate in post-surgical recovery of humerus fracture and injured radial nerve can be remarkably higher in young people as compared to other age groups.
Keywords: Gunshot wounds, Radial nerve, Humerus fracture, Upper limbs, Seddon’s classification
Introduction
The radial nerve is the largest neural network and major peripheral nerve of the upper limb. The nerve arises in the brachial plexus and receives from the lower parts of the cervical segment of the spinal cord and upper parts of the thoracic segments. This nerve affected some forearm muscles in the lower parts of the elbow and involved in providing cutaneous sensory innervation for a large part of the back of the hand. The control of the forearm extensor muscles, wrist and fingers are also provided by this nerve [1] [2]. Therefore, if the radial nerve is damaged in the arm, elbow, or upper part of the forearm, the person will not be able to raise the wrists and fingers from the back to the forehead due to paralysis of the forearm’s extensor muscles, where cannot extend at the metacarpophalangeal joints, leading to the wrist drop as the most common symptom of radial nerve damage [3].
Studies have shown that men are more likely to be injured in the upper extremity, especially the radial nerves due to some issues such as occupation, driving accidents, insignificant safety issues more than women [4]. Among the most important signs of radial neuropathy, pain, paralysis, loss of ability, numbness, bending of the wrists, stretching, lack of coordination, tingling and atrophy can be pointed out [5] [6].
The most common mechanisms of damage to the radial nerve are in the head of the humerus and the dorsolateral humerus [7]. Radial nerve damage commonly occurs at the spiral groove of the humerus which can be linked to compression, and also another reason may be involved in the occurrence of radial nerve damage such as fractures of the humerus or external pressure [8]. Radial nerve damage is one of the most common damages to the peripheral nervous system associated with humerus bone fracture [8]. The bone fracture of the humerus accounts for about 3 to 5% of all fractures, and radial nerve paralysis (RNP) occurs in 2 to 17% of the humerus bone fractures.
RNP can be partial or complete, and humerus fractures account for about 3 to 5% of all fractures, [9] [10] [11]. Radial nerve damage due to trauma can be commonly found in situations such as battle scenes where people are exposed to direct gunshot and explosions. Most types of sensory and motor injuries result from trauma for the patient and cause many problems in the daily activities of individuals [12].
The type and location of traumatic nerve injury are very important regarding the area of the nerve involved and how to prognosis [13]. In general, penetrating wounds, which occurred during the war, are often the result of projectiles to the combatant’s body. These injuries can be caused by direct bullet collisions or from fragmentation munitions or fragmentation munitions caused by explosive ordnance such as mines, grenades, mortars and bombs [14]. Such war injuries have a high potential for nerve damage, especially in motor organs. The explosions or gunshot have caused extensive destruction and damage to the tissues due to the high speed and direct transfer of energy to the organs and tissues, as well as their high temperatures. These injuries not only leave a different tissue traumatic pattern but also severely complicate the treatment process [15]. Radial nerve damage treatment is very important due to the extremely complex anatomy of the nerve area [16]. Based on the time of injury, radial nerve damage is divided into two primary and secondary groups. Loss of function occurs at the time of injury, in the primary form, and mainly due to closed fractures. However, in the secondary type, loss of function occurs due to conservative treatment or trapping the nerve in the fracture holes or broken parts of the bone, as well as following surgery [11] [16] [17]. According to published data, secondary damage to the radial nerve occurs in 4% to 32% of patients undergoing surgery for stabilising the fracture [18]. Therefore, the adoption of a therapeutic approach is very important. Treatment for radial nerve injuries caused by penetrating ulcers is a surgical repair of the nerve.
Some researchers in this field believe that when radial nerve injury is caused by pressure or stretching, a preservative and protective treatment can be used for a limited period [19]. Other therapies for the treatment of radial nerve damage can be referred to the transfer of the tendon; this treatment is used when there is no indication of nerve repair due to the atrophy of extensor muscles and replacement of the fibrous tissue [20]. Each of the therapies used to treat radial nerve injuries depends on a variety of factors, such as the type of injury, the site of injury, and the degree of nerve damage.
Regarding the pivotal role of this issue and problems above, the present study was aimed to investigate the types of radial nerve injury caused by the bullet and explosive injuries among Iraqi soldiers in the war against ISIS fighters.
Material and Methods
We performed a 3-year retrospective cohort analysis based on medical records of patients with sustaining gunshot wounds and blast injuries to the upper limbs, which conducted from June 2015 to April 2018 in collaboration with Islamic Azad University and Bouali Hospital. During this period, patients were enrolled by inclusion and exclusion criteria. The sampling process was to initially cover all Iraqi soldiers and military personnel available in all age groups exposed to bullet wounds and explosive injuries and other traumatic injuries in fighting ISIS fighters, including operations military, vehicle accidents, clashes, etc. Among these patients, patients with weak or radial sensory loss in their medical records were selected after being referred to the military emergency hospital. Demographic data, trauma history, trauma characteristics, the severity of the injury, electrophysiological study and physical examination were extracted. Seddon classification system was used to assess the severity of injury in these patients.
Finally, medical records of 318 patients who suffered from humeral fractures and complete radial nerve palsy were investigated. Data were analysed by SPSS 23IBM software, which presented by descriptive statistics (frequency, percentage, mean ± standard deviation, etc.).
Results
This retrospective study was performed on 318 patients with a minimum age of 24 years who were injured by gunshot or blast injury with humerus fractures and complete paralysis of the radial nerve at Tehran’s Bouali Hospital between 2015 and 2018. The mean age of these patients was determined to be 25.41 ± 6 years. 127 patients with open fracture and complicated injuries in upper limbs and 191 patients with closed injuries and radial nerve palsy were included (Figure 1).
Figure 1.
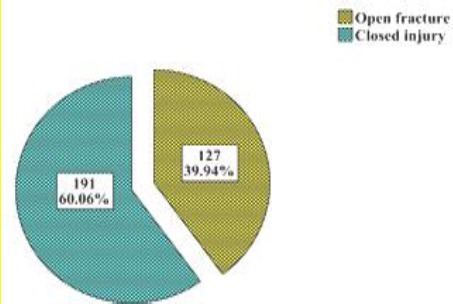
Frequency of open fracture and closed injuries in patients
Out of 127 patients, 113 patients with an open fracture (Figure 3) improved by primary repair of the radial nerve, but 14 patients (11%) did not recover at all. 3 of them with absolutely no improvement had iatrogenic radial nerve injury due to the internal fixation device. Our findings indicated that all 191 patients with intact explored nerves were improved. The average recovery time was determined as 8 weeks (the range was between 1 and 27 weeks), and the total average recovery period was calculated as 6 months (range 1-22 months). In the current study, Axonotmesis and Neurotmesis have seen in 283 (89%) subjects. According to the data, the explosion was found to be the main cause of radial nerve injury in 236 individuals (74.2%), followed by gunshot damage (21.4%, 68 subjects), falling from height and accidents caused by motor vehicles (4.4%, 14 subjects) and multiple injuries (17%, 54 case), (Figure 2).
Figure 3.
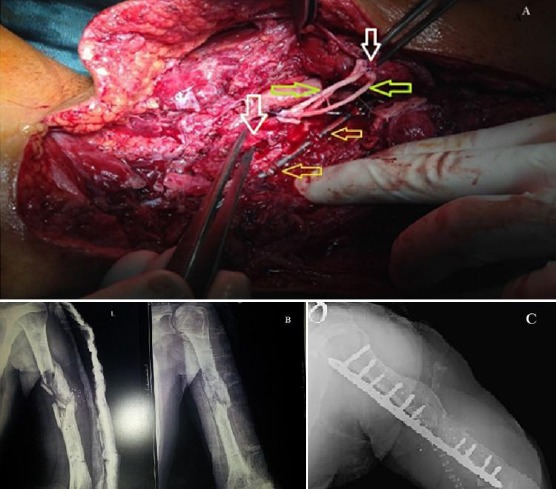
A) Severely injured left upper extremity gunshot wound with segmental radial nerve defect (white arrow). After débridement, segmental radial nerve defect reconstruction with interposition of sural nerve allograft of 6 cm (green arrow) and nerve coaptation wraps in place was performed. The superior and inferior halves of the proximal and distal radial nerve trunk were anastomosed with three segments of the sural nerve stumps. Each nerve ending was anastomosed using a perineural technique under microscopic magnification. Internal fixation of midshaft humerus fracture (orange arrow); B) Preoperative X-Ray of midshaft humerus fracture caused by gunshot; C) Open reduction and internal fixation with shortening of the humerus and iliac crest bone graft resulted in a union.
Figure 2.
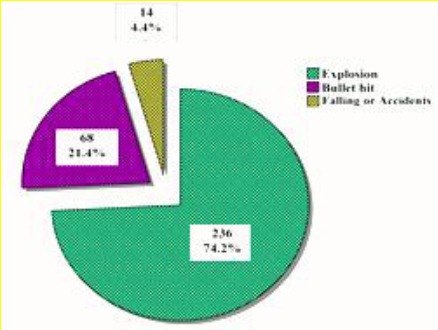
Frequency of major causes of nerve injury
A large number of the lesions were ≤ S2 and M2 levels before the operation. The results were classified into three groups. Good outcome was defined as ≥ M4 and ≥ S4, the fair outcome was represented by M2-M3 / S2-S3, and poor outcome was ≤ M1 and ≤ S1 (Table 1 and 2).
Table 1.
Modified British Medical Research Council (BMRC) grading of sensorimotor recovery, and motor recovery on the quality of outcome after radial nerve repair [27]
| Motor recovery |
|---|
| Poor |
| M0 No contraction |
| M1 Return of perceptible contraction in the proximal muscles |
| Fair |
| M2 Return of perceptible contraction in both proximal and distal muscles |
| M3 Return of perceptible contraction in both proximal and distal muscles of such of degree that all-important muscles are sufficiently powerful to act against resistance |
| Good |
| M4 Return of function as in stage 3 with the addition that all synergic and independent movements are possible |
| M5 Complete recovery |
| Sensory recovery |
| Poor |
| S0 No sensation |
| S1 Deep pain re-established |
| Fair |
| S2 Some response to touch and pin, with over-response |
| S3 Good response to touch and pin, without over-response |
| Good |
| S4 Location and some tactile discrimination |
| S5 Complete recovery |
Table 2.
Summary of patients data and grading of recovery
| Total number of patients n=318 | |||
|---|---|---|---|
| Closed fracture 191 (60%) | Open fracture 127 (40%) | ||
| Improved: 191 | Improved: 113 | Not recovered: 14 | |
| M2/S3 | 7 (3,6%) | 51 (45,1%) | |
| M3/S3 | 49 (25,6%) | 15 (13,2%) | |
| M3/S4 | 19 (9,9%) | 32 (28,3%) | |
| M4/S3 | 22 (11,5%) | 12 (10,6%) | |
| M5/S4 | 56 (29,3%) | 3 (2,6%) | |
| M5/S5 | 38 (19,8%) | ||
| M0/S0 | 6 | ||
| M0/S1 | 5 | ||
| M0/S2 | 3 | ||
Discussion
In addition to incidents and everyday events, battle scenes are high-risk situations that can expose the person to the most severe traumatic injuries. War trauma can be either penetrating or non-penetrating. Penetrating injuries are caused by gunshot, knives and other sharp objects clipart, and non-penetrating injuries are due to accident, falling, explosion wave, etc. [21]. According to the investigations carried out in this area, penetrating injuries as a result of war projectiles are one of the most common causes of injury in the battlefields [22]. Motor organs and long bones are important parts of the body that suffer from trauma, tissue damage and fracture. The humerus is a large bone in the arm or forelimb that may be fractured in its various parts, such as head and neck, trunk, and areas near the elbow joint as a result of accidents, and falling. Each of these fractures has its characteristics and has different treatment regimens. On the battlefield, in addition to closed damage to the humerus and the bone, Penetrating injuries also occur in the area due to projectiles.
These injuries are often caused by direct bullet encounters or by the explosives collapse such as mines, grenades, mortar bomb and bombs [14]. Projectile-induced injuries due to high speed, direct energy transfer and extreme heat cause massive damage to the tissue and make the traumatic pattern and treatment process more complex [15].
The most important complication of humerus trauma and humerus fracture in this area is radial nerve neuropathy. Based on available data, up to 5% of the total fractures are related to the humerus fracture, which is associated with a radial nerve palsy [9][11][23], and often this neuronal injury occurs between two-thirds of the upper and one-third of the lower humerus. Understanding damage patterns, especially in military, and familiarity with the complexities of these types of injuries can play a decisive role in the quality of the treatment process and improve the success rate of patient recovery significantly.
Therefore, research projects focusing on the subjects in the present study are necessary and inevitable. Non-surgical treatment, especially in the case of the elongation and mild rupture, and surgical intervention (early exploration or late exploration) are performed by a specialist diagnosis. The surgical process has complications such as infection, iatrogenic damage to the nerve and the lack of improvements in fracture due to disruption of the blood supply to the tissue. According to the data reported by the American Orthopedic Surgery Board, intramedullary nailing (IMN) and Open Reduction and Internal Fixation (ORIF) have been accounted for 1.5% and 3% of infected d cases. The iatrogenic paralysis rate in IM and ORIF methods has been estimated to be 3.1% and 7.8%, respectively. Furthermore; nonunion of bone fractures has been reported in 3.1% and 1.6% of subjects for IMN and ORIF methods [24]. Compared with the statistics above, which is a result of reports published between 2004 and 2013, we conclude that only 1% of subjects showed absolutely no improvement in radial nerve, which is considerably more favourable than global published data.
Moreover, no infections or nonunion was found in our study. The most important factor which may have affected our results in recovery of the radial nerve e is probably the young age of our patients. Although this issue has become a challenge for researchers and clinicians; however, the high rate of treatment success in our study demonstrated that rapid recovery depends mainly on the age of patients. Due to the young age of patients in our study (mean age of patients 25.41 ± 6), the improvement rate was high, and the treatment complications were surprisingly low. Nouraei et al., (2014) also reported that young patients have fewer complications such as nonunion, infection, neurovascular problems and osteonecrosis [25]. Although healing in healthy older adults (≥ 65 years of age) is not impaired per se, age-related changes are obvious in all phases of wound repair [26].
In conclusion, the diagnosis of radial nerve injury after humeral fractures is easy. However, the verify of the damage degree of the radial nerve is very difficult. It is the degree for damage of radial nerve playing a decisive role in the judgment of whether exploration is necessary or not. Complex peripheral nerve injuries of the upper extremity are challenging to manage. They require an understanding of not only the mechanism and type of nerve injury but also the timing of repair. One has to be careful not to downgrade function by intervening too early in a closed injury. Care should be taken not to intervene too late, precluding motor recovery, in an open nerve injury. Closed injuries benefit from serial examinations to determine the extent of injury and recovery, whereas open or sharp injuries benefit from expeditious operative exploration and repair. These characteristics guide surgical decision making. Options for repair are numerous and include primary repair, grafting, nerve and tendon transfer, and free functional muscle transfer. A careful history and physical examination, along with the judicious use of electrodiagnostic and radiologic studies are just the beginning of the complex management algorithms of peripheral nerve injuries and are tempered with an experienced approach to repair. All the tools in one’s armamentarium should be considered, while individualised care in response to the unique attributes of these complex cases is applied.
We recommend early radial nerve exploration (within the first 2 weeks) in patients with open fractures or high-energy closed fractures of humerus with radial nerve injury. To draw a more convincing conclusion on the optimal management strategy, more methodologically improved trials with standardised outcome measures are recommended in future work.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Drake R, Vogl AW, Mitchell AW. Gray's Anatomy for Students E-Book:Elsevier Health Sciences. 2009 [Google Scholar]
- 2.Botte MJ. Surgical anatomy of the hand and upper extremity: Lippincott Williams & Wilkins. 2003 [Google Scholar]
- 3.Patel S, Zhang D, Earp BE. Acute Combined Median and Radial Nerve Palsies after Distal Humeral Shaft Fracture. Archives of Bone and Joint Surgery. 2018;6(2):150–4. PMid:29600269 PMCid:PMC5867360. [PMC free article] [PubMed] [Google Scholar]
- 4.Ring D, Chin K, Jupiter JB. Radial nerve palsy associated with high-energy humeral shaft fractures 1. Journal of Hand Surgery. 2004;29(1):144–7. doi: 10.1016/j.jhsa.2003.09.013. https://doi.org/10.1016/j.jhsa.2003.09.013 PMid:14751118. [DOI] [PubMed] [Google Scholar]
- 5.Baron R, Maier C, Attal N, Binder A, Bouhassira D, Cruccu G, et al. Peripheral neuropathic pain. Pain. 2017 https://doi.org/10.1097/j.pain.0000000000000753. [Google Scholar]
- 6.Thomsen NO, Dahlin LB. Injury to the radial nerve caused by fracture of the humeral shaft:timing and neurobiological aspects related to treatment and diagnosis. Scandinavian journal of plastic and reconstructive surgery and hand surgery. 2007;41(4):153–7. doi: 10.1080/02844310701445586. https://doi.org/10.1080/02844310701445586 PMid:17701727. [DOI] [PubMed] [Google Scholar]
- 7.Kato N, Birch R. Peripheral nerve palsies associated with closed fractures and dislocations. Injury. 2006;37(6):507–12. doi: 10.1016/j.injury.2006.02.044. https://doi.org/10.1016/j.injury.2006.02.044 PMid:16643920. [DOI] [PubMed] [Google Scholar]
- 8.Li Y, Ning G, Wu Q, Feng S. Review of literature of radial nerve injuries associated with humeral fractures-an integrated management strategy. PLoS One. 2013;8(11):e78576. doi: 10.1371/journal.pone.0078576. https://doi.org/10.1371/journal.pone.0078576 PMid:24250799 PMCid:PMC3826746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.DeFranco MJ, Lawton JN. Radial nerve injuries associated with humeral fractures. J Hand Surg Am. 2006;31(4):655–63. doi: 10.1016/j.jhsa.2006.02.013. https://doi.org/10.1016/j.jhsa.2006.02.013 PMid:16632062. [DOI] [PubMed] [Google Scholar]
- 10.Shah A, Jebson PJ. Current treatment of radial nerve palsy following fracture of the humeral shaft. J Hand Surg Am. 2008;33(8):1433–4. doi: 10.1016/j.jhsa.2008.05.029. https://doi.org/10.1016/j.jhsa.2008.05.029 PMid:18929216. [DOI] [PubMed] [Google Scholar]
- 11.Shao YC, Harwood P, Grotz MR, Limb D, Giannoudis PV. Radial nerve palsy associated with fractures of the shaft of the humerus:a systematic review. J Bone Joint Surg Br. 2005;87(12):1647–52. doi: 10.1302/0301-620X.87B12.16132. https://doi.org/10.1302/0301-620X.87B12.16132 PMid:16326879. [DOI] [PubMed] [Google Scholar]
- 12.Tuncel U, Turan A, Kostakoglu N. Acute closed radial nerve injury. Asian journal of neurosurgery. 2011;6(2):106. doi: 10.4103/1793-5482.92175. https://doi.org/10.4103/1793-5482.92175 PMid:22347334 PMCid:PMC3277063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sabri BM, Yılmaz G, Adem E, Davut K, Özlem B. Difficulty in clinical evaluation of radial nerve injury due to multiple trauma to the humerus, wrist, and hand. J Clin Imaging Sci. 2014;4:16. doi: 10.4103/2156-7514.129263. https://doi.org/10.4103/2156-7514.129263 PMid:24744973 PMCid:PMC3988597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wright J. A History of War Surgery: Amberley Publishing. 2011 [Google Scholar]
- 15.Bartlett C, Helfet DL, Hausman MR, Strauss E. Ballistics and gunshot wounds:effects on musculoskeletal tissues. J Am Acad Orthop Surg. 2000;8(1):21–36. doi: 10.5435/00124635-200001000-00003. https://doi.org/10.5435/00124635-200001000-00003 PMid:10666650. [DOI] [PubMed] [Google Scholar]
- 16.Reichert P, Wnukiewicz W, Witkowski J, Bocheńska A, Mizia S, Gosk J, et al. Causes of Secondary Radial Nerve Palsy and Results of Treatment. Medical Science Monitor :International Medical Journal of Experimental and Clinical Research. 2016;22:554–62. doi: 10.12659/MSM.897170. https://doi.org/10.12659/MSM.897170 PMid:26895570 PMCid:PMC4762296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Larsen LB, Barfred T. Radial nerve palsy after simple fracture of the humerus. Scand J Plast Reconstr Surg Hand Surg. 2000;34(4):363–6. doi: 10.1080/028443100750059156. https://doi.org/10.1080/028443100750059156. [DOI] [PubMed] [Google Scholar]
- 18.Bumbasirevic M, Lesic A, Bumbasirevic V, Cobeljic G, Milosevic I, Atkinson HD. The management of humeral shaft fractures with associated radial nerve palsy:a review of 117 cases. Arch Orthop Trauma Surg. 2010;130(4):519–22. doi: 10.1007/s00402-009-0951-4. https://doi.org/10.1007/s00402-009-0951-4 PMid:19669771. [DOI] [PubMed] [Google Scholar]
- 19.Tubiana R. Problems and solutions in palliative tendon transfer surgery for radial nerve palsy. Techniques in hand & upper extremity surgery. 2002;6(3):104–13. doi: 10.1097/00130911-200209000-00002. https://doi.org/10.1097/00130911-200209000-00002. [DOI] [PubMed] [Google Scholar]
- 20.Kato H, Minami A, Suenaga N, Iwasaki N, Kimura T. Long-term results after primary repairs of zone 2 flexor tendon lacerations in children younger than age 6 years. Journal of Pediatric Orthopaedics. 2002;22(6):732–5. https://doi.org/10.1097/01241398-200211000-00007 PMid:12409897. [PubMed] [Google Scholar]
- 21.Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States:data from the American Migraine Study II. Headache. 2001;41(7):646–57. doi: 10.1046/j.1526-4610.2001.041007646.x. https://doi.org/10.1046/j.1526-4610.2001.041007646.x PMid:11554952. [DOI] [PubMed] [Google Scholar]
- 22.Beekley AC, Watts DM. Combat trauma experience with the United States Army 102nd forward surgical team in Afghanistan. The American journal of surgery. 2004;187(5):652–4. doi: 10.1016/j.amjsurg.2004.02.001. https://doi.org/10.1016/j.amjsurg.2004.02.001 PMid:15135685. [DOI] [PubMed] [Google Scholar]
- 23.Lowe JB, 3rd, Sen SK, Mackinnon SE. Current approach to radial nerve paralysis. Plast Reconstr Surg. 2002;110(4):1099–113. doi: 10.1097/01.PRS.0000020996.11823.3F. PMid:12198425. [DOI] [PubMed] [Google Scholar]
- 24.Gottschalk MB, Carpenter W, Hiza E, Reisman W, Roberson J. Humeral Shaft Fracture Fixation:Incidence Rates and Complications as Reported by American Board of Orthopaedic Surgery Part II Candidates. J Bone Joint Surg Am. 2016;98(17):01049. doi: 10.2106/JBJS.15.01049. https://doi.org/10.2106/JBJS.15.01049 PMid:27605696. [DOI] [PubMed] [Google Scholar]
- 25.Nouraei MH, Majd DA, Zamani F. Comparing the treatment results of proximal humerus fracture based on surgical or nonsurgical methods. Advanced Biomedical Research. 2014;3:253. doi: 10.4103/2277-9175.146385. https://doi.org/10.4103/2277-9175.146385 PMid:25590031 PMCid:PMC4283251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Pahlavan S, Baldwin KD, Pandya NK, Namdari S, Hosalkar H. Proximal humerus fractures in the pediatric population:a systematic review. J Child Orthop. 2011;5(3):187–94. doi: 10.1007/s11832-011-0328-4. https://doi.org/10.1007/s11832-011-0328-4 PMid:21779308 PMCid:PMC3100455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Brooks DM. Peripheral nerve injuries. Medical Research Council Special Report Series, HMSO. 1954:418–429. PMid:13223114. [Google Scholar]