

Abstract
The earliest account of orthostatic tremor (OT) dates back to 1970, when Pazzaglia and colleagues reported on three patients with a peculiar disorder only occurring on standing. Although Pazzaglia et al. did not use the term OT, they first provided both the clinical and neurophysiological features of such a condition.
Keywords: orthostatic tremor, tremor, standing
“The farther backward you can look, the farther forward you are likely to see.” Winston Churchill
Although the term “orthostatic tremor” (OT) first entered the medical literature in 1984, when Heilman described 3 patients with a movement disorder characterized by tremor of the legs upon standing,1 the earliest account of OT dates back to 1970.2 Pazzaglia et al. reported on, in the Italian journal Rivista Sperimentale di Freniatria (Fig. 1), 3 patients affected with an “unusual disorder of erect standing position” featuring tremor of the legs, which started with a short latency when they stood.2
Figure 1.
Cover of the issue containing the paper by Pazzaglia et al.
When Pazzaglia et al. saw the first of these 3 patients, in January 1968, they were left perplexed (translated from Italian):
This observation left us deeply puzzled, since we were unable to find any pathophysiological explanations for such a peculiar disorder of erect standing position; so puzzled to doubt about its true organic nature.
This patient had no other neurological disturbances apart from an extreme difficulty to stand:
There were fast and regular oscillations of the antigravitary muscles, exclusevely present on standing. The subject put effort into avoiding falls by widening of his feet, bending over the trunk, or by putting weight onto one leg. […] After a few seconds, he had to lean onto something or to walk: In this way, everything stopped immediately, with his obvious relief. This was the only symptom.
They also provided the electrophysiological features of OT, although the first description in this regard has been generally attributed to Thompson, who, in 1986, described 1 OT patient noting a 16‐Hz tremor of the legs when standing.3 Pazzaglia et al. found a 14‐to 16‐Hz tremor of the legs on standing, which was abolished when the subject leaned onto something (Fig. 2).2 Notably, they also picked up a postural tremor of the arms at a lower frequency (Fig. 2),2 which has been subsequently recognized as part of the condition in the majority of OT patients.4
Figure 2.
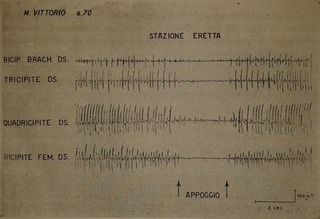
Original picture of the article by Pazzaglia et al. (with permission). Up to down, surface electromyography recording of the right biceps, triceps, rectus femoris, and biceps femoris muscles. In the leg, a 14‐ to 16‐Hz tremor can be seen, which stops when the patient leans onto something (arrows). In the arm, a tremor at a lower frequency is seen.
The other 2 patients in their series had similar symptoms in the context of another neurological disorder: tabes dorsalis (syphilitic myelopathy) and flaccid paralysis likely resulting from a spinal stroke, respectively. On electrophsyiology, the 2 patients had less regular contractions of the leg muscles at a lower frequency of approximately 10 to 12 Hz.2 Currently, we would diagnose these 2 patients with pseudo‐OT.4
Very interestingly, Pazzaglia et al. wondered whether such a peculiar condition was associated with inappropriate postural responses:
With the aim to establish whether such hyperkinesias were triggered by postural responses on standing or were simply related to the vertical position of the body, the first patient underwent tilt table testing. We hence observed that the vertical position of the body in the absence of postural loading did not elicit any symptoms.
They therefore speculated that the disorder was a result of the dysfunction of the regulating system of the postural tonus, involving, at the same time, the spinal and supraspinal level.2 Thirty‐six years later, Spiegel provided similar evidence using a slightly more sophisticated technology,5 but such a hypothesis has not yet been entirely settled.
Author Roles
(1) Conception; (2) Manuscript: A. Writing of the First Draft; B. Review and Critique.
R.E.: 1, 2A
E.A.: 2B
K.P.B.: 2B
Disclosures
Funding Sources and Conflicts of Interest: The authors report no sources of funding and no conflicts of interest.
Financial Disclosures for previous 12 months: R.E. received funding for travel from Ipsen. K.P.B. receives royalties from Oxford University Press and received funding for travel from GlaxoSmithKline, Orion Corporation, Ipsen, and Merz Pharmaceuticals.
Acknowledgments
The authors are grateful to Luigi Tagliabue, editor of Rivista Sperimentale di Freniatria, who kindly allowed the publication of the original picture of the article published in 1970 by Pazzaglia et al.
Relevant disclosures and conflicts of interest are listed at the end of this article.
References
- 1. Heilman KM. Orthostatic tremor. Arch Neurol 1984;41:880–881. [DOI] [PubMed] [Google Scholar]
- 2. Pazzaglia P, Sabattini L, Lugaresi E. Su di un singolare disturbo della stazione eretta (osservazione di tre casi) [On an unusual disorder of erect standing position (observation of three cases)]. Riv Freniatr 1970;96:450–457. [PubMed] [Google Scholar]
- 3. Thompson PD, Rothwell JC, Day BL, Berardelli A, Dick JP, Kachi T, Marsden CD. The physiology of orthostatic tremor. Arch Neurol 1986;43:584–587. [DOI] [PubMed] [Google Scholar]
- 4. Erro R, Bhatia KP, Cordivari C. Shaking on standing: a critical review. Mov Disord Clin Pract 2014;1:173–179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Spiegel J, Krick C, Fuss G, Sood D, Becker G, Dillmann U. Orthostatic tremor during modification of standing. Mov Disord 2006;21:173–178. [DOI] [PubMed] [Google Scholar]