

Abstract
Background
Chronic obstructive pulmonary disease (COPD) manifests itself in complex ways, with local and systemic effects; because of this, a multifactorial approach is needed for disease evaluation, in order to understand its severity and impact on each individual. Thus, our objective was to study the correlation between easily accessible variables, usually available in clinical practice, and maximum aerobic capacity, and to determine models for peak oxygen uptake (VO2peak) estimation in COPD patients.
Subjects and methods
Individuals with COPD were selected for the study. At the first visit, clinical evaluation was performed. During the second visit, the volunteers were subjected to the cardiopulmonary exercise test. To determine the correlation coefficient of VO2peak with forced expiratory volume in 1 second (FEV1) (% pred.) and the COPD Assessment Test score (CATs), Pearson or Spearman tests were performed. VO2 at the peak of the exercise was estimated from the clinical variables by simple and multiple linear regression analyses.
Results
A total of 249 subjects were selected, 27 of whom were included after screening (gender: 21M/5F; age: 65.0±7.3 years; body mass index: 26.6±5.0 kg/m2; FEV1 (% pred.): 56.4±15.7, CAT: 12.4±7.4). Mean VO2 peak was 12.8±3.0 mL⋅kg−1⋅min−1 and VO2peak (% pred.) was 62.1%±14.9%. VO2peak presented a strong positive correlation with FEV1 (% pred.), r: 0.70, and a moderate negative correlation with the CATs, r: -0.54. In the VO2peak estimation model based on the CAT (estimated VO2peak =15.148− [0.185× CATs]), the index explained 20% of the variance, with estimated error of 2.826 mL⋅kg−1⋅min−1. In the VO2peak estimation model based on FEV1 (estimated VO2peak =6.490+ [0.113× FEV1]), the variable explained 50% of the variance, with an estimated error of 2.231 mL⋅kg−1⋅min−1. In the VO2peak estimation model based on CATs and FEV1 (estimated VO2peak =8.441− [0.0999× CAT] + [0.1000× FEV1]), the variables explained 55% of the variance, with an estimated error of 2.156 mL⋅kg−1⋅min−1.
Conclusion
COPD patients’ maximum aerobic capacity has a significant correlation with easily accessible and widely used clinical variables, such as the CATs and FEV1, which can be used to estimate peak VO2.
Keywords: chronic obstructive pulmonary disease, exercise, oxygen uptake, symptoms
Introduction
Chronic obstructive pulmonary disease (COPD) is a highly prevalent disease in clinical practice, currently affecting around 3 million subjects worldwide.1 Research indicates that it will become the third leading cause of death in 2030, with an evident impact on health care public expenditure.1,2
The costs for treatment and care of individuals with COPD increase substantially with the progression in severity of the disease, which leads to a circle of increased symptoms perception, reduced daily living activities, worsened quality of life perception, and increased exercise intolerance.3,4
The complexity of COPD manifestation makes it difficult to choose a treatment protocol that encompasses each patient’s needs and to understand the disease impact on the individual’s life. Moreover, designing a severity staging system easily applicable in clinical practice is extremely difficult.5
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) was established with the purpose to define COPD diagnosis, treatment, and prevention guidelines.7 According to these guidelines, COPD staging was exclusively based on pulmonary function, and by means of forced expiratory volume in the first second (FEV1) each patient was classified into 1 of 4 stages (mild, moderate, severe, and very severe).6
Therefore, pulmonary function evaluation, and especially FEV1, stood out in the care of individuals with COPD; besides, studies have shown FEV1 value to determine prognosis and mortality risk in this population.7 However, because COPD is a complex and heterogeneous disease with wide variation of symptoms and exacerbation frequency, updates of disease classification were proposed. The new 2017 GOLD classification has come to consider pulmonary function, symptoms perception, and exacerbation frequency as fundamental parameters for the disease staging.8
In addition, evidence showed that COPD severity strongly correlates with exercise intolerance, which can be assessed by cardiopulmonary exercise test (CPET), which is the gold standard to assess the maximum aerobic capacity.9,10 Despite the importance of CPET for COPD management, the high cost involved in its performance makes its application unfeasible in clinical practice.
For successful management of COPD, it is fundamental to apply evaluation methods which, apart from pulmonary function, take into consideration the individual’s perception of their own disease, symptoms and impact on their general health, functional capacity, and quality of life. The COPD Assessment Test (CAT) consists of a unidirectional questionnaire that considers the individual’s perception of the disease and reflects their functional status.11 However, whether the CAT score (CATs) could estimate peak oxygen uptake (VO2) in this population has never been investigated.
Thus, the objective of the present study was to assess the correlation between easily accessible variables, usually available in clinical practice, such as the CATs and pulmonary function parameters, and maximum aerobic capacity, and to determine models for peak VO2 estimation in COPD patients.
Methods
Subjects
We recruited for the present study individuals with a diagnosis of COPD (stages I–IV), according to the criteria established by the GOLD,12 who participated in previous studies and were undergoing COPD treatment at Sao Carlos Medical Specialties Center (CEME), Brazil. The collection of data happened between August 2015 and September 2017.
The exclusion criteria were as follows: no telephone contact; no confirmation of COPD diagnosis according to the GOLD criteria;12 conditions compatible with COPD exacerbation according to the GOLD criteria12 over the 3 months preceding the evaluations; use of home oxygen therapy; previous or current treatment with antiarrhythmic drugs; cardiac pacemaker; body mass index below 18.5 kg/m2 or above 35 kg/m2; musculoskeletal diseases or deficits (cognitive, visual, auditory) that would compromise the performance of physical exercise on a cycle ergometer; previous or current history of alcoholism; any evaluation nonattendance.
Ethics aspects
The study was approved by the Committee of Ethics in Research with Human Beings (protocol no 1.484.831). The volunteers received elucidation and guidance regarding all the experimental procedures to which they would be submitted and their noninvasive nature. After agreeing to participate in the study, all the volunteers signed a formal consent form, in compliance with the National Health Council Resolution no 466/2012.
Outcome measurements
The primary outcome of the present study was the relationship between VO2peak, FEV1 (% pred.) and the CATs in COPD patients. Subsequently, FEV1 (% pred.) and the CATs were used independently to determine VO2peak estimation equations for this population.
Protocol
The experimental procedures were performed over 2 visits at the laboratory. During the first visit, the volunteers underwent a clinical evaluation, which consisted of personal and anthropometric data collection, history of current and previous disease and comorbidities investigation, and pulmonary function evaluation. During the second visit, the volunteers performed the CPET.
Inquiry
An inquiry was applied in an interview format; the volunteers answered questions related to personal data (name, age, address, telephone contact, and profession); history of current and previous disease (diagnosis, treatment, exacerbations, and/or hospitalizations); and symptomatology (evaluated through the CAT, which will be described in the following).
CATs
In order to investigate the patients’ symptomatology, the CAT questionnaire (in its version validated for the Portuguese language) was applied through an interview.13 The questionnaire includes questions about 8 items: cough, catarrh, chest tightness, dyspnea, limitations in home-based activities, confidence in leaving home, sleep, and energy. For each item, the volunteer chooses only 1 option, whose score ranges from 0 to 5, where 0 corresponds to the absence of symptoms and 5 to maximum symptom perception. The final score is given by the sum of all items, thus varying from 0 to 40, with higher values reflecting greater COPD symptoms perception.14
Lung function test
To confirm their COPD diagnosis and staging, the volunteers underwent spirometry (CPFS/S, Med. Graphs and 1085 ELITE DTM, Medical Graphics Corporation, St Paul, MN, USA). The volunteers performed 3 acceptable and reproducible forced expiratory maneuvers according to the criteria established by the American Thoracic Society/European Respiratory Society.15 Predicted values were obtained considering reference values for the Brazilian population.16 All lung function variables were analyzed postbronchodilator.
CPET
All volunteers performed a CPET on a cycle ergometer (Corival Recumbent, Medical Graphics Corporation). An Oxycon Mobile® system (Mijnhardt/Jäger, CareFusion Corporation, Würzburg, Germany) was used to analyze exhaled gases.
The protocol included a 5-minute rest until gas exchange measurements were stable. Afterwards, the volunteers performed a warm-up; they were instructed to start the exercise and maintain a cadence of 60 rpm for 1 minute, with 0 workload. Then, the exercise phase was started; a ramp protocol was applied, with load increases from 5 to 10 W/min, until tolerance limit. The load increase was individualized according to each patient’s exercise tolerance; patients were encouraged to perform the test until exhaustion. Thus, an exercise period of between 8 and 12 minutes was guaranteed.
In order to guarantee the volunteers’ safety, the CPET was performed by a physician and 2 physiotherapists, who monitored a 12 leads electrocardiogram (WinCardio Systems, Micromed, Brasília, Brazil) and minute-to-minute blood pressure.
Statistical analysis
The results are presented as mean and SD or median and interquartile range, according to data distribution. Data normality was analyzed by the Shapiro–Wilk test. Pearson or Spearman test was used to measure the correlation coefficient of VO2peak with BMI, FEV1 (% pred.), and CATs. Correlation magnitude was determined considering the following classification scheme for r values: 0.26–0.49, low or weak; 0.50–0.69, moderate; 0.70–0.89, strong or high; and 0.90–1.0, very high. Simple and multiple linear regressions were applied to determine VO2peak estimation models based on the CATs and FEV1 (% pred.). The level of significance was set at 5% (P≤0.05).17,18
Statistical analysis was performed using SigmaPlot for Windows, version 11.0 (SyStat Software, Inc., San Jose, CA, USA) and SPSS, version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Subjects’ characteristics
A total of 249 individuals were selected to participate in the present study based on the preestablished inclusion criteria. Ninety-two of them were not reachable by telephone. Thus, 157 individuals were contacted, 44 of whom refused to participate in the study, 29 of whom presented exclusion criteria, 15 of whom reported not having a COPD diagnosis and not making use of medications, and 6 of whom were deceased. After this selection, 63 individuals attended the first visit at the laboratory, 12 of whom did not have a COPD diagnosis confirmed by the GOLD criteria, 14 of whom presented exclusion criteria, 2 of whom died during the study period, and 8 of whom did not complete all the evaluations or discontinued participation. Thus, 27 volunteers completed the study protocol, as shown in the flow diagram presented in Figure 1.
Figure 1.
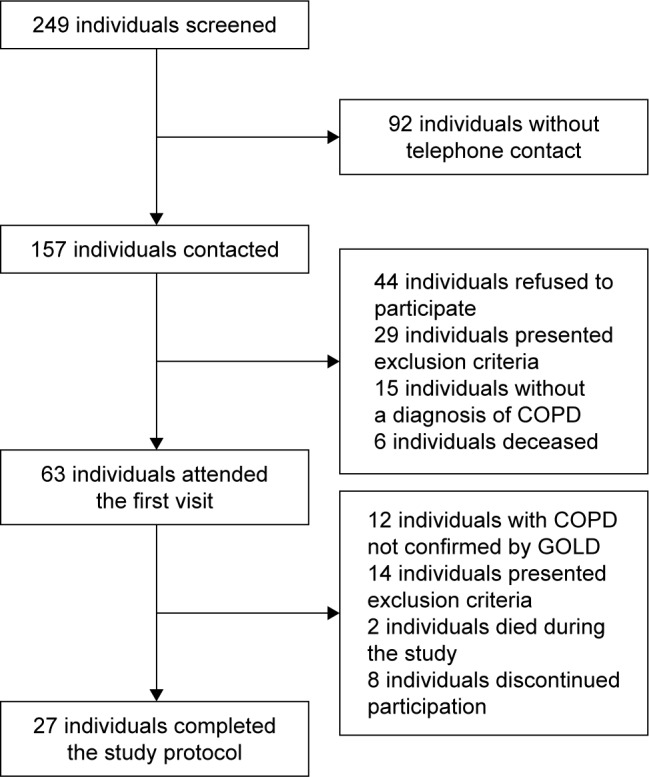
Study flowchart.
Abbreviations: COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
The subjects’ anthropometric and clinical characteristics are shown in Table 1.
Table 1.
COPD patients’ anthropometric and clinical characteristics
| Characteristics | COPD (n=27) |
|---|---|
| Age, years | 65.0±7.3 |
| Gender, male/female | 21/5 |
| BMI, kg/m2 | 26.6±5.0 |
| CATs | 12.4±7.4 |
| Lung function | |
| FEV1/FVC | 49.1±15.7 |
| FEV1, % predicted | 56.4±19.4 |
| GOLD stage, n (% of patients) | |
| 1. Mild | 3 (11.1) |
| 2. Moderate | 13 (48.1) |
| 3. Severe | 7 (25.9) |
| 4. Very severe | 4 (14.9) |
| GOLD risk class, n (% of patients) | |
| A | 7 (25.9) |
| B | 10 (37.1) |
| C | 2 (7.4) |
| D | 8 (29.6) |
Note: Data are presented as mean ± SD or number (%).
Abbreviations: BMI, body mass index; CATs, COPD assessment test score; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
Maximum aerobic capacity
The volunteers presented a mean VO2peak of 12.8±3.0 mL⋅min−1⋅kg−1, which represents 62.1%±14.9% of the predicted value. The variables obtained in the CPET are presented in Table 2.
Table 2.
Variables obtained in the CPET in COPD patients
| CPET variables | COPD (n=27) |
|---|---|
| Rest | |
| HR peak, bpm | 77.1±9.8 |
| SBP, mmHg | 137.0±14.0 |
| DBP, mmHg | 82.4±8.9 |
| SpO2, % | 94.0±2.4 |
| BORG dyspnea score | 0.2±0.8 |
| BORG lower limbs fatigue score | 0.1±0.6 |
| Incremental exercise | |
| VO2peak, mL⋅min−1 | 972.6±298.9 |
| VO2peak, mL⋅min−1⋅kg−1 | 12.8±3.0 |
| VO2peak, % predicted | 62.1±14.9 |
| VCO2peak, mL⋅min−1 | 1,080±389.5 |
| RER | 1.1±0.1 |
| VE, L⋅min−1 | 43.4±17.0 |
| VE/MVV | 73.9±22.8 |
| HR peak, bpm | 124.7±15.9 |
| SBP peak, mmHg | 204.4±24.5 |
| DBP peak, mmHg | 106.6±10.3 |
| SpO2 peak, % | 86.8±8.9 |
| Power, W | 72.8±39.2 |
| Exercise time, seconds | 568.4±142.0 |
| BORG dyspnea score peak | 6.1±2.3 |
| BORG lower limbs fatigue score peak | 4.3±3.6 |
Note: Values are presented as mean ± SD.
Abbreviations: CPET, cardiopulmonary exercise test; DBP, diastolic blood pressure; HR, heart rate; MVV, maximal voluntary ventilation; RER, respiratory exchange ratio; SBP, systolic blood pressure; SpO2, oxygen saturation; VCO2, carbon dioxide output; VE, minute ventilation; VO2, pulmonary oxygen uptake.
VO2peak presented a strong positive correlation with FEV1 (r: 0.70, P≤0.05) and a moderate negative correlation with CATs (r: −0.54, P≤0.05). VO2peak did not present a significant correlation with BMI. Significant correlations are presented in Figure 2.
Figure 2.

Significant correlations between (A) CATs and VO2peak and (B) FEV1 (% pred.) and VO2peak in COPD patients.
Abbreviations: CATs, COPD Assessment Test score; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; % pred., percentage of predicted value; VO2, pulmonary oxygen uptake.
VO2peak estimation models
Considering the significant correlations found between VO2peak and CATs and FEV1 (% pred.), a simple linear regression analysis was performed. In the VO2peak estimation model based on the CATs, this variable explained 20% of VO2peak variance, and the following predictive equation was obtained: Estimated VO2 peak (mL⋅kg−1⋅min−1) =15.148−(0.185× CATs), with an estimated standard error of 2.826 mL⋅kg−1⋅min−1. The model is described in Table 3.
Table 3.
VO2peak estimation model based on CATs in COPD patients
| Variable | Coefficient | Standard error | P-value |
|---|---|---|---|
| R2=0.200 | |||
| Constant | 15.148 | 1.072 | <0.001 |
| CATs | −0.185 | 0.0742 | 0.019 |
Abbreviations: CATs, COPD assessment test score; COPD, chronic obstructive pulmonary disease; VO2, pulmonary oxygen uptake.
In the model based on FEV1 (% pred.), this variable explained 50% of VO2peak variance, and the following equation was obtained: estimated VO2 peak (mL⋅kg−1⋅min−1) = 6.490+ (0.113× FEV1), with an estimated error of 2.231 mL⋅kg−1⋅min−1. The model is described in Table 4.
Table 4.
VO2peak estimation model based on FEV1 (% pred.) in COPD patients
| Variable | Coefficient | Standard error | P-value |
|---|---|---|---|
| R2=0.501 | |||
| Constant | 6.490 | 1.338 | <0.001 |
| FEV1 (% pred.) | 0.113 | 0.0224 | <0.001 |
Abbreviations: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; % pred., percentage of predicted value; VO2, pulmonary oxygen uptake.
Multiple linear regression analysis was also performed considering CAT and FEV1 (% pred.), which explained 55% of VO2peak variance, and the following equation was obtained: estimated VO2 peak (mL⋅kg−1⋅min−1) =8.441−(0.0999× CATs) + (0.1000× FEV1), with an estimated standard error of 2.156 mL⋅kg−1⋅min−1. The model is described in Table 5.
Table 5.
VO2peak estimation model based on CATs and FEV1 (% pred.) in COPD patients
| Variable | Coefficient | Standard error | P-value |
|---|---|---|---|
| R2=0.553 | |||
| Constant | 8.441 | 1.774 | <0.001 |
| CAT | −0.0999 | 0.0599 | 0.109 |
| FEV1 (% pred.) | 0.1000 | 0.0230 | <0.001 |
Abbreviations: CATs, COPD assessment test score; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; % pred., percentage of predicted value; VO2, pulmonary oxygen uptake.
Discussion
The COPD patients who participated in the present study presented a mean VO2peak of 12.8±3.0 mL⋅kg−1⋅min−1, which represented 62.1%±14.9% of the predicted value. For this population, VO2peak presented a strong positive correlation with FEV1 and a moderate negative correlation with CATs. In the VO2peak estimation model based on CAT (estimated VO2 peak [mL⋅kg−1⋅min−1] =15.148− [0.185× CATs]), this variable explained 20% of the variance, with an estimated error of 2.826 mL⋅kg−1⋅min−1. In the VO2peak estimation model based on FEV1 (% pred.) (estimated VO2 peak [mL⋅kg−1⋅min−1] =6.490+ [0.113× FEV1]), this variable explained 50% of the variance, with an estimated error of 2.231 mL⋅kg−1⋅min−1. The CATs and FEV1 (% pred.) in the VO2peak estimation model based on CAT and FEV1 (% pred.) (estimated VO2peak [mL·kg–1·min–1] =8.441−[0.0999× CATs] + [0.1000× FEV1]) were able to explain 55% of the variance, with an estimated error of 2.156 mL⋅kg−1⋅min−1.
Due to COPD pathophysiology, it was expected that the volunteers would present deficits in their maximum aerobic capacity, measured by VO2peak, which is the most widely used variable obtained from the CPET. The values of VO2peak and percentage of the predicted value found in the present study are consistent with reported data, such as those presented in the study by Barron et al,19 in which COPD patients underwent CPET on a cycle ergometer and presented a mean VO2peak of 16.7 mL⋅kg−1⋅min−1, representing 69.9% of the predicted value.
In the study by Robles et al,20 COPD patients performed a CPET and presented VO2peak values similar to those found in our study (mean value of 14.2 mL⋅kg−1⋅min−1). The study by Skjørten et al21 also showed similar CPET parameters for COPD patients without pulmonary hypertension for: reached workload, pulmonary ventilation, and heart rate at the peak of the exercise. However, their results showed a VO2peak value higher than the one observed in our study (mean of 17.6 mL⋅kg−1⋅min−1). However, since the authors did not present predicted percentage values for the analyzed specific population, we believe that this result might have been observed due to differences in the ethnic characteristics of the population.
The parameters obtained in the CPET have great relevance for individuals with COPD, as shown in the study by Hiraga et al,22 where the authors stated that exercise capacity parameters measured during the CPET may be used to determine a prognosis for COPD individuals.
Understanding COPD severity and determining a prognosis is a major challenge in clinical practice due to the complexity of pulmonary and extrapulmonary manifestations, and it is now accepted that airflow limitation alone, marked by FEV1, is an insufficient marker of the disease severity.23–25
Because of this, the GOLD initiative proposes that the disease approach should be multidimensional and recommends that the symptoms and risk of exacerbation be considered to establish the severity of the disease and the risk groups.1 This new approach frames a significant portion of patients into a different risk category, thus allowing the identification and consequent closer monitoring of more severe patients.26
According to Hernández et al26 this new approach criteria classifies higher proportions of patients in the lighter and more severe groups, which also occurred in our study, considering that approximately 11% of the volunteers were framed as mild (GOLD 1) and 15% as very serious (GOLD 4), according to GOLD 2007,1 while approximately 26% were classified as risk A and 30% as risk D by GOLD 2015. These data highlight the importance of assessing the perception of symptoms of COPD patients and reiterate the need to consider this variable concomitantly to the limitation of airflow in clinical practice.
In addition to the importance of assessing airflow limitation and perception of symptoms in COPD to understand the disease severity, it is interesting to note that these variables correlate with the exercise capacity in this population. In our study, we found a moderate correlation between the perception of symptoms and VO2peak and a strong correlation between FEV1 and VO2peak.
The moderate correlation between CATs and VO2peak found in COPD patients in our study is in agreement with the findings by Chuang et al,27 which showed a significant moderate negative correlation between the 2 variables (r=−0.53, P<0.0001).20
The strong correlation between FEV1 and VO2peak that we found in our study was an expected result, on the basis of results presented in previous studies, such as that by Frisk et al,28 that showed a significant reduction of VO2peak over the course of 4.5 years in COPD subjects and that this decrease was related to an FEV1 reduction.
Interestingly, the correlation between FEV1 and VO2peak is not a unique characteristic of COPD; the study by Hassel et al29 showed that a predictive model of VO2peak in an elderly population without chronic diseases can be significantly improved by the inclusion of the FEV1 and that, especially in elderly men, this parameter is an important predictor of cardiovascular fitness.
The strength of this study is the determination of a VO2peak estimation model for individuals with COPD based on CATs and FEV1, which are easy to obtain in clinical practice. To date, no other studies are available that have proposed VO2peak estimation models for COPD patients using simple variables which are easily obtainable in clinical practice. This result is relevant in clinical practice because, despite the importance of VO2peak to understand the impact of the disease on the patient’s health condition and to establish a prognosis, high costs of CPET, due to the need of a specific equipment and of specialized personnel, make it difficult to be used on a large scale in the daily clinical care of COPD patients.
Thus, indirect methods for VO2peak estimation are needed. In the present study, we proposed an estimation model based on the CATs, which has been gaining prominence in clinical practice and has become part of the new approach for COPD patients’ risk classification.8 Given this parameter’s importance for the health condition understanding of COPD patients, we expected that a model based on the CATs would be able to reliably estimate VO2peak. This hypothesis was confirmed by our results that showed that the CATs was able to explain 20% of the dependent variable. The proposed prediction equation presented an estimated error of 2.8 mL⋅kg−1⋅min−1, corresponding to <1 SD (3.0 mL⋅kg−1⋅min−1) of directly measured VO2peak values.
We also expected FEV1 to be an important parameter in VO2peak estimation in COPD patients, because of its importance in the classification of COPD risk and severity, its well-known correlation with maximal aerobic capacity, and its capacity to improve VO2peak estimative models in an elderly population without chronic disease. This hypothesis was confirmed by our findings, which showed that FEV1 was able to explain 50% of the dependent variable, with an estimated error of 2.2 mL⋅kg−1⋅min−1.
Using the 2 variables (CATs and FEV1) concomitantly for VO2peak estimation in COPD patients, we obtained an even more robust model, where the independent variables were able to explain 55% of the dependent variable, with an estimated error of 2.1 mL⋅kg−1⋅min−1.
The use of CATs and FEV1 for VO2peak estimation, both isolated and concomitantly, generated models with estimated errors corresponding to <1 SD. It is worth noting that the VO2peak estimation model used in clinical practice presents an error around 20%–30%.30 Thus, the models we proposed can be used in clinical practice, also due to the practicality and low cost needed to obtain the independent variables.
The present study has limitations that must be considered. Since a BMI below 18.5 kg/m2 or above 35 kg/m2 was defined as an exclusion criterion, the VO2peak estimation equations we presented should not be used for COPD patients presenting these specific characteristics. In addition, due to the sample characteristics, it was not possible to analyze the gender impact on maximal aerobic capacity, which may be a limitation to estimateVO2peak. However, we emphasize that the findings of the present study are clinically relevant and may greatly contribute to COPD patients’ pulmonary rehabilitation, also considering the low cost, simplicity, and practicality to estimate aerobic capacity in these patients. We also emphasize that new studies are fundamental to help understand the influence of clinical variables, such as symptoms and pulmonary function, on maximal aerobic capacity in COPD patients. It is worth mentioning that the monitoring over time of these variables in this specific population may provide data of great interest for COPD patients’ rehabilitation.
Conclusion
We conclude that clinical variables that are easy to assess and widely used in clinical practice present a significant correlation with maximum aerobic capacity in COPD patients and that VO2peak estimation models based on the CATs and FEV1 can be used in this specific population.
Acknowledgments
The authors would like to thank all the volunteers who participated in this study and all researchers of the Cardiopulmonary Physiotherapy Laboratory of Federal University of Sao Carlos (LACAP – UFSCar) for their support. This study was funded by CNPq (protocol no 163789/2015–0) and FAPESP (protocol no 2015/26501–1).
Footnotes
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. doi: 10.1164/rccm.200703-456SO. [DOI] [PubMed] [Google Scholar]
- 2.Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):2011–2030. doi: 10.1371/journal.pmed.0030442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hu J, Meek P. Health-related quality of life in individuals with chronic obstructive pulmonary disease. Heart Lung. 2005;34(6):415–422. doi: 10.1016/j.hrtlng.2005.03.008. [DOI] [PubMed] [Google Scholar]
- 4.Polkey MI, Moxham J. Attacking the disease spiral in chronic obstructive pulmonary disease: an update. Clin Med. 2011;11:461–464. doi: 10.7861/clinmedicine.11-5-461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Coton S, Vollmer WM, Bateman E, et al. Severity of airflow obstruction in chronic obstructive pulmonary disease (COPD): proposal for a new classification. COPD. 2017;14(5):469–475. doi: 10.1080/15412555.2017.1339681. [DOI] [PubMed] [Google Scholar]
- 6.Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS, GOLD Scientific Committee Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163(5):1256–1276. doi: 10.1164/ajrccm.163.5.2101039. [DOI] [PubMed] [Google Scholar]
- 7.Gedebjerg A, Szépligeti SK, Wackerhausen LH, et al. Prediction of mortality in patients with chronic obstructive pulmonary disease with the new Global Initiative for Chronic Obstructive Lung Disease 2017 classification: a cohort study. Lancet Respir Med. 2018;6(3):204–212. doi: 10.1016/S2213-2600(18)30002-X. [DOI] [PubMed] [Google Scholar]
- 8.Global Initiative for Chronic Obstructive Lung Disease . Global Strategy for Diagnosis, Management, and Prevention of COPD. GOLD; 2017. [Accessed April 11, 2018]. Available from: https://goldcopd.org/gold-2017-global-strategy-diagnosis-management-prevention-copd/ [Google Scholar]
- 9.Waschki B, Kirsten AM, Holz O, et al. Disease progression and changes in physical activity in patients with COPD. Am J Respir Crit Care Med. 2015;192(3):295–306. doi: 10.1164/rccm.201501-0081OC. [DOI] [PubMed] [Google Scholar]
- 10.Guenette JA, Chin RC, Cheng S, et al. Mechanisms of exercise intolerance in global initiative for chronic obstructive lung disease grade 1 COPD. Eur Respir J. 2014;44(5):1177–1187. doi: 10.1183/09031936.00034714. [DOI] [PubMed] [Google Scholar]
- 11.Gulart AA, Munari AB, Queiroz AP, Cani KC, Matte DL, Mayer AF. Does the COPD assessment test reflect functional status in patients with COPD? Chron Respir Dis. 2017;14(1):37–44. doi: 10.1177/1479972316661924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Global Initiative for Chronic Obstructive Lung Disease . Global Strategy for Diagnosis, Management, and Prevention of COPD. GOLD; 2018. [Accessed June 13, 2018]. Available from: https://goldcopd.org/wp-content/uploads/2017/11/GOLD-2018-v6.0-FINAL-revised-20-Nov_WMS.pdf. [Google Scholar]
- 13.da Silva GPF, Morano MTAP, Viana CMS, de Araujo Magalhães CB, Pereira EDB. Validação do Teste de Avaliação da DPOC em português para uso no Brasil [Portuguese-language version of the COPD Assessment Test: validation for use in Brazil] J Bras Pneumol. 2013;39(4):402–408. doi: 10.1590/S1806-37132013000400002. Portuguese. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi: 10.1183/09031936.00102509. [DOI] [PubMed] [Google Scholar]
- 15.Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirom-etry. Eur Respir J. 2005;26(2):319–338. doi: 10.1183/09031936.05.00034805. [DOI] [PubMed] [Google Scholar]
- 16.Alberto de Castro Pereira C, Sato T, Carla Rodrigues S. Novos valores de referência para espirometria forçada em brasileiros adultos de raça branca [New reference values for forced spirometry in white adults in Brazil] J Bras Pneumol. 2007;33(4):397–406. doi: 10.1590/s1806-37132007000400008. Portuguese. [DOI] [PubMed] [Google Scholar]
- 17.Dancey CP, Reidy J. Estatística Sem Matemática Para Psicologia: Usando SPSS Para Windows [Statistics without maths for psychology: using SPSS for Windows] Porto Alegre: Artes Médicas; 2006. [Google Scholar]
- 18.Dourado VZ, Vidotto MC, Guerra RL. Reference equations for the performance of healthy adults on field walking tests. J Bras Pneumol. 2011;37(5):607–614. doi: 10.1590/s1806-37132011000500007. [DOI] [PubMed] [Google Scholar]
- 19.Barron A, Francis DP, Mayet J, et al. Oxygen uptake efficiency slope and breathing reserve, not anaerobic threshold, discriminate between patients with cardiovascular disease over chronic obstructive pulmonary disease. JACC Heart Fail. 2016;4(4):252–261. doi: 10.1016/j.jchf.2015.11.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Robles P, Araujo T, Brooks D, et al. Cardiorespiratory responses to short bouts of resistance training exercises in individuals with chronic obstructive pulmonary disease. J Cardiopulm Rehabil Prev. 2017;37(5):356–362. doi: 10.1097/HCR.0000000000000282. [DOI] [PubMed] [Google Scholar]
- 21.Skjørten I, Hilde JM, Melsom MN, et al. Cardiopulmonary exercise test and PaO2 in evaluation of pulmonary hypertension in COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:91–100. doi: 10.2147/COPD.S150034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hiraga T, Maekura R, Okuda Y, et al. Prognostic predictors for survival in patients with COPD using cardiopulmonary exercise testing. Clin Physiol Funct Imaging. 2003;23(6):324–331. doi: 10.1046/j.1475-0961.2003.00514.x. [DOI] [PubMed] [Google Scholar]
- 23.Jones P, Miravitlles M, van der Molen T, Kulich K. Beyond FEV1 in COPD: a review of patient-reported outcomes and their measurement. Int J Chron Obstruct Pulmon Dis. 2012;7:697–709. doi: 10.2147/COPD.S32675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Westwood M, Bourbeau J, Jones PW, Cerulli A, Capkun-Niggli G, Worthy G. Relationship between FEV1 change and patient-reported outcomes in randomised trials of inhaled bronchodilators for stable COPD: a systematic review. Respir Res. 2011;12(1):40. doi: 10.1186/1465-9921-12-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Tsiligianni I, Kocks J, Tzanakis N, Siafakas N, van der Molen T. Factors that influence disease-specific quality of life or health status in patients with COPD: a review and meta-analysis of Pearson correlations. Prim Care Respir J. 2011;20(3):257–268. doi: 10.4104/pcrj.2011.00029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hernández M, García G, Falco J, et al. Impact of using the new GOLD classification on the distribution of COPD severity in clinical practice. Int J Chron Obstruct Pulmon Dis. 2018;13:351–356. doi: 10.2147/COPD.S112551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Chuang ML, Lin IF, Lee CY. Clinical assessment tests in evaluating patients with chronic obstructive pulmonary disease: a cross-sectional study. Medicine. 2016;95(47):e5471. doi: 10.1097/MD.0000000000005471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Frisk B, Hardie JA, Espehaug B, et al. Peak oxygen uptake and breathing pattern in COPD patients – a 4-year longitudinal study. BMC Pulm Med. 2015;15(1):93. doi: 10.1186/s12890-015-0095-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hassel E, Stensvold D, Halvorsen T, Wisløff U, Langhammer A, Steinshamn S. Lung function parameters improve prediction of VO2peak in an elderly population: the Generation 100 study. PLoS One. 2017;12(3):e0174058. doi: 10.1371/journal.pone.0174058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Meneghelo RS, Araújo CGS, Stein R, et al. III Diretrizes da Sociedade Brasileira de Cardiologia Sobre Teste Ergométrico [Guidelines for exercise testing of the Brazilian Cardiology Society] Rev Bras Fisioter. 2011;95(5):1–26. [Google Scholar]