

Abstract
Patient’s desires for an un-operated look and shorter recovery times have lead to a blending of surgical and non-surgical techniques to effect facial rejuvenation. Anatomical changes within the skeleton and soft tissue compartments are discussed. A brief review of adjunctive techniques to replace volume lost in aging is presented. These techniques (autologous fat grafting and injectable fillers) are contrasted with more involved surgical procedures (rhytidectomy and sub-periosteal mid-face lifting). In patients with mild jowling, the “liquid facelift” can approach the results seen in surgical face-lifting. In patients with significant jowling, the addition of volume replacement at the time of rhytidectomy enhances the rejuvenation. The addition of volume replacement at the time of rhytidectomy has the potential to allow less aggressive surgical dissections to accomplish a harmonious result.
Introduction
The eye sees what the mind knows. Patients desiring rejuvenation will often pull their cheeks upward with a finger placed over the malar mound and request this to be their desired post-operative look. Many aesthetic surgeons will then manipulate the face to show an up and back lift which more closely simulates the classic surgical facelift look.
The aging process within the face has been advanced by better understanding of the structures of the face. Ligamentous attach points around the orbit, along the anterior masseteric border, mental check ligaments and mastoid fusions contribute much to facial stability. When tissue ptosis inevitably occurs, jowls form in the part of the face without ligamentous support. With knowledge of these ligaments, surgeons can correct laxity between the masseteric and mental ligaments which results in smoothing of the jowls, without the need for heroic skin traction. This produces a much more natural facial appearance than the extended subcutaneous dissection and strong skin traction, characteristic of the 1970s. Surgical techniques also may employ undermining of the investing fascia of the face, the superficial musculo-aponeurotic system (SMAS) and elevation of the submalar fat and longitudinal tightening of the platysma in the Deep Plane Rhytidectomy. Subperiosteal mid-face lifting has gained popularity as well as suture suspension techniques such as the MACS lift1 as a way to accomplish a more vertical vector facelift.
Facial fat has been determined to follow a consistent pattern of compartmentalization.2, 3 The borders of these compartments compose many of the ligaments which support the face. Clever study of photos over time, in faces with obvious markers such as moles, has determined that the face, in many places, doesn’t descend as much as it deflates.4 The orbit of youth is a transverse oval. The lower eyelid looses its vertical shortness and becomes more elongated contributing to the circular appearance of the aged orbit. Loss of volume within the sub-orbicularis occuli fat pad (SOOF) of Ramirez5 as well as outward rotation of the bony orbit unmasks the edematous malar mound and pseudo-herniation of the orbital fat pads.
Attempts to rejuvenate the mid-face have included surgery in many different tissue planes. Sub-periosteal mid-face lifts have enjoyed popularity as a method to upwardly lift the soft tissues of the face. Several more involved rhytidectomy dissection techniques incorporate Ristow’s space3 or reposition the submalar fat over the zygomatic muscles. The deep plane and composite rhytidectomies were popularized by Hamra.6
Early attempts to graft fat were highly variable, with some fat surviving and in other instances volume achieved was the result of oil cysts. Autologous fat grafting has been advanced by the work of Coleman7 and others to a predictable volumizing procedure. The volume of the grafted fat fluctuates with body weight, a possible disadvantage over shorter term injectable fillers. Off-the-shelf fillers utilizing hyaluronic acid, calcium hydroxyapetite and poly-l-lactic acid are convenient for shorter term restoration and offer little or no down time for the patient and volume stability regardless of body fat composition.
The most common request for correction of lines associated with aging involves the nasolabial fold. The nasolabial fold, though it can be prominent in youth, is a significant concern for the patient seeking restoration of the aging face. The nasolabial fold deepens as a result of underlying bony resorption in the pyriform aperture as well as deflation of the fat within the deep medial cheek compartment. With age, the pyriform aperture as well as the alar base retrude from a position anterior to the lacrimal crest in youth to a position posterior to that in aging. Bony retrusion in the maxilla and the glabella associated with aging has been documented by CT scan performed over time (See Figures 1 and 2).
Figure 1.

Sample computed tomographic scans of )left) a female subject in the young age group and (right) a female subject in the old age group, with mean angular measurements applied. Reprinted with permission.8
Figure 2.

Sample computed tomographic scans of )left) a male subject in the young age group and (right) a male subject in the old age group, with mean pyriform aperture area applied. Reprinted with permission.8
Facial Aesthetics
Facial shape and proportion has been analyzed since the advent of perspective art. The mathematical relationship of ϕ, employing the ratios of 0.61:1:1.61 and the Fibrinachi sequence repeat in the many triangles that determine the ideal face. Marquart has made an overlay mask which can be applied to an AP photograph to help determine the appropriate location for prominences and proportion balance9 (See Figure 3).
Figure 3.
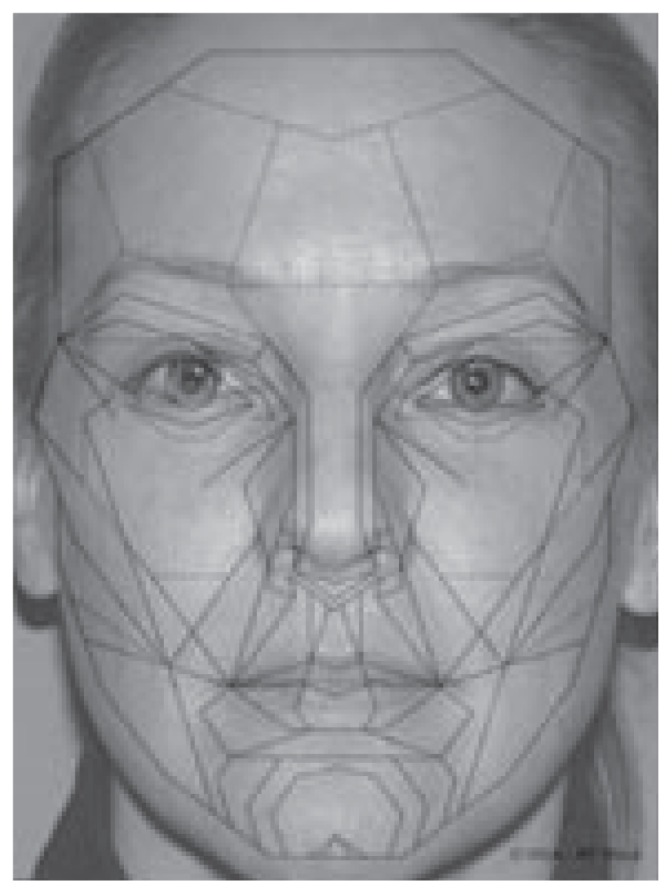
Marquardt mask overlay of patient in Case 2.
Archetypal Facial Mask copyright by Dr. Stephen R. Marquardt and courtesy of Dr. Marquardt and www.beautyanalysis.com
Volumizing Modalities
Volume can be replaced or shifted depending on pre-treatment assessment and desired outcome. Patient’s willingness to undergo a procedure often relates to the anticipated down time, risk and cost. Though bruising may restrict social activities, injectable fillers placed with either topical anesthesia or trigeminal nerve blocks offers the patient the most immediate results with little risk and less immediate cost than surgery. Duration of action varies between six months to over two years and is location specific. FDA approved temporary fillers are depicted in Table 1.
Table 1.
FDA Approved absorbable soft tissue fillers

|

|
|||
|---|---|---|---|---|
|
|
||||

|

|
|

|

|
|
|
||||
|
Radiesse# (Bioform Medical) | Sculptra* (Sanofi Aventis Pharmaceutical) | Restylane, Perlane (Medicis Aesthetics Holdings) | Zyderm, Zyplast (Allergan) |
|
|
||||
| Hylaform, Hyalform Plus (Genzyme Biosurgery) | Cosmoderm, Cosmoplast (Allergan) | |||
|
|
||||
| Juvederm 30, Juvederm 30 HV, Juvederm 24HV (Allergan) | Evolence (Colbar Lifesciences) | |||
|
|
||||
| Elevess (Anika Therapeutics) | ||||
Indicted for use for both correction of moderate to severe facial folds and wrinkles and for correction of the signs of lipoatrophy in people with HIV.
Indicted for use for both correction of moderate to severe facial folds and wrinkles and for correction of the signs of lipoatrophy in people with HIV.

Case 1- Left: Preoperative/Right: Postoperative
This patient is 58-year old with osteoporosis, who has undergone four injection sessions over a 13-month period for soft tissue and bony augmentation. Results following placement of five vials of Sculptra in the deep subcutaneous layer of malar/submalar/perioral/brow regions and and 1.4 cc of Radiesse placed over the infraorbital rim periosteum.
Utilizing the lifting effects of the deep medial cheek compartment and by augmenting the pyriform aperture with fillers such as poly-l-lactic acid (Sculptra®) or calcium hydroxyapetite (Radiesse®) the eyelid can be restored to a more youthful transverse oval shape, the nasolabial fold can be effaced and the jowl muted. See Cases 1 and 2.
Micro fat grafting placed in the deep medial cheek compartment may require more than one fat grafting session. Each session requires a fat harvesting session. Many patients prefer these procedures with either conscious sedation or general anesthesia, although many can be performed under local anesthesia. Often fat grafting is combined with other facial aesthetic surgical procedures such as rhytidectomy (facelift). There have been many anecdotal reports of a stem-cell rejuvenating effect on the skin following fat grafting. Typical augmented areas include the malar/submalar regions, the chin, the mandibular angle and border, the eyebrow and temple. Care should be exercised in the individual with weight instability, as these individuals may look markedly different at a higher weight. See Case 3.

Case 2 - Left: Preoperative/Right: Postoperative
This patient is a 41-year old who desires more youthful appearance. Results following injection of 3 vials of Sculptra in two injection sessions, injecting the malar/ submalar/mandibular angle and brow.

Case 3 - Left: Preoperative/Right: Postoperative
This patient is 51-year old who is four months followup from a short scar SMAS imbrication facelift with upper and lower blepharoplasty who underwent autologous fat grafting at the time of her facelift with 5.5 cc of fat placed per side in the deep medial cheek compartment for augmentation of her malar region, as well as augmentation of the peri-oral region.

Case 4-Left: Preoperative/Right: Postoperative
This patient is 69-year old who had had a facelift and blepharoplasty 20 yrs ago, who was concerned about her recurrent facial laxity. A sub-periosteal mid-face cheek lift/endoscopic brow lift and SMAS imbrication mini-rhytidectomy was performed to restore volume in the upper cheeks.
Midface subperiosteal cheek lifting is often performed with a concomitant brow or temple lift to avoid bunching of soft tissues around the infra-lateral orbit. Mid-face lifting may be performed at the time of a conventional rhytidectomy; however, edema can be prolonged due to additional lymphatic disruption. Various methods of fixation are employed, each with subtle aesthetic differences in results. Individuals with pronounced malar mounds or a chubby face are challenging patients as these features may be accentuated depending on the technique selected. See Case 4.
Potential Complications
The potential for complications associated with all injectable fillers have points of commonality as well as some unique potential problems. Injectables as well as surgical procedures carry a risk of temporary bruising. Vascular embolization can occur with all the injectable fillers. In close proximity to the angular artery and periorbital vessels, due to communication with the retinal artery, techniques should be employed to flash the needle prior to injection if performing a bolus injection. Fanning injections pose less theoretical risk than a bolus, as the statistical likelihood of delivering an embolizing particle is reduced based upon the reduced potential time that the moving needle would be intraluminal. Hyaluronic acid injections can be dissolved with available preparations of hyaluronidase (Vitrase®). Granulomatous formations can occur with both poly-l-lactic acid and hydroxyapetite. Hygroscopic swelling of hyaluronic acid based fillers can place pressure on vessels as well as sensory nerves.
Microfat grafting poses some embolization potential, but due to the larger cannula or needle size, the risk is reduced except in areas of the larger vessels which are generally palpable (angular, facial) or have a constant location (supra trochlear and supraorbital aa.; 1.6 cm and 2.6 cm from the midline). A technique called Fat Autografting Muscle Injections (FAMI) is gaining in popularity10. In this technique, the fat is grafted within the belly of the levator anguli oris. The blood supply of the deep medial cheek compartment relies solely on the infra-orbital artery. The levator anguli oris directly overlies the infraorbital foramen. Injections of fat as well as other fillers have the potential to devascularize the deep medial cheek compartment’s blood supply as well as result in dysesthesias of the infra-orbital nerve. Theoretically this will have less potential when fat is grafted with a cannula rather than a beveled needle. Asymmetric graft take and the need to re-graft are commonplace.
Complications of mid-face lifting include facial nerve branch palsy, synkinesis, failure of fixation, ectropion, chemosis, scleral show and exaggeration of the malar mound of Furnas. Failure to control the dissection space may result in accumulation of blood, serum, or infection in the sub-periosteal space.
Conclusion
Though the face looks fallen, and the conventional approach has been the facelift procedure, the aesthetic results of rejuvenation employing volume repositioning or replacement results in a more harmonious correction of the features of facial aging than that achieved by the facelift operation alone. Volume restoration done by injectable fillers only, commonly called the liquid facelift, is an effective method of correcting many features of aging, and can approach the results of surgical procedures in selected patients. Injectable fillers have a temporary effect; however, some of these modalities effectively compete with surgery, when one considers dollars spent divided by longevity of result for both the surgical procedure and the “liquid facelift”. With properly injected fillers combined with botulinum A toxin intermittently, and aggressive skin care, many patients can forgo or forestall an aggressive surgical procedure.
Biography
Jerome Lamb, MD, MSMA member since 1989, is a board certified plastic surgeon in private practice in Independence, Missouri since 1988.
Contact: docflyboy@yahoo.com

Footnotes
Disclosure
Dr. Lamb conducts training sessions and speaking on volume restoration from Sanofi-Aventis.
References
- 1.Tonnard PL, Verpaele AM. Short-Scar Face Lift. Quality Medical Publishing; 2007. [Google Scholar]
- 2.Rohrich RJ, Pessa JE. The Fat Compartments of the Face: Anatomy and Clinical Implications for Cosmetic Surgery. PRS. 2007;119:2219. doi: 10.1097/01.prs.0000265403.66886.54. [DOI] [PubMed] [Google Scholar]
- 3.Rohrich RJ, Pessa JE, Ristow B. The Youthful Cheek and the Deep Medial Fat Compartment. PRS. 2008;121:2107. doi: 10.1097/PRS.0b013e31817123c6. [DOI] [PubMed] [Google Scholar]
- 4.Lambros V. Observations on Periorbital and Midface Aging. PRS. 120(5):1367–76. doi: 10.1097/01.prs.0000279348.09156.c3. discussion 1377. [DOI] [PubMed] [Google Scholar]
- 5.Ramirez O. The Beautiful Eye. Facial Plast Surg Clin North Am. 2005 Nov;13(4):493–504. doi: 10.1016/j.fsc.2005.06.001. [DOI] [PubMed] [Google Scholar]
- 6.Hamra Sam T. Composite Rhytidectomy. Quality Medical Publishing; 1993. [Google Scholar]
- 7.Coleman SR. Facial Augmentation with Structural Fat Grafting. Clinics in Plastic Surgery. 2006 Oct; doi: 10.1016/j.cps.2006.09.002. [DOI] [PubMed] [Google Scholar]
- 8.Shaw RB, Kahn DM. Aging of the Midface Bony Elements: A three-Dimensional Computed Tomographic Study. PRS. 2007;119:675. doi: 10.1097/01.prs.0000246596.79795.a8. Figures 1 & 3. [DOI] [PubMed] [Google Scholar]
- 9.Marquardt SR. http://www.beautyanalysis.com/index2_mba.htm.
- 10.Amar R. Fat Autografting Muscle Injections. Presentation at the annual meeting of the American Society for Aesthetic Plastic Surgery. 2005 May 4; [Google Scholar]