

Abstract
Background
With the increasing need for high-quality exercise interventions in China, relatively little is known about issues and challenges related to recruitment of older Chinese adults into exercise-based disease prevention interventions. This study aims to describe the recruitment process and outcomes of 2 exercise interventions conducted in Shanghai, China.
Methods
Recruitment information was ascertained from 2 community-based randomized controlled trials for 2 exercise interventions, the first designed to improve health outcomes for older women with knee osteoarthritis and the second to study changes in cognitive function in adults with mild cognitive impairment. Results were summarized in terms of recruitment sources, number screened, screening-to-enrollment ratios, and costs.
Results
Recruitment was primarily achieved through working with local residential divisions (i.e., neighborhood associations and residential committees). Both studies achieved their planned target number of older adults (45 and 46, respectively) within a 1-year time frame, with a screening-to-randomized ratio of 5:1 and demonstrated excellent retention rates (range 87%–93%) at 6 months. The recruitment cost for the 2 studies averaged RMB 189 (about USD 30) per initial recruit and RMB 738 (about USD 119) per participant randomized. Some major issues encountered during the recruitment process included (1) the use of community neighborhoods to support the conduct of the projects, (2) access to participants, and (3) feasibility.
Conclusion
Analysis of the 2 randomized controlled trials has provided valuable insights into the recruitment process and identified resources that can help better planning and recruitment for future interventions. Recommendations aimed at increasing the success of future recruitment efforts are provided.
Keywords: Community stakeholders, Exercise intervention, Older adults, Participant access, Randomized controlled trial, Recruitment
1. Introduction
With an increase in the aging population and the prevalence of noncommunicable chronic diseases in China,1, 2, 3, 4 there is an urgent public health need to develop and evaluate interventions that can help prevent the onset and progression of chronic disease in older Chinese adults at risk for health problems. Mounting evidence indicates that exercise can bring about significant health benefits for older adults.5, 6, 7 In China, researchers in the field of health promotion and disease prevention have recently increased their efforts to conduct randomized controlled trials (RCTs) of exercise interventions. These RCTs help determine the efficacy and effectiveness of interventions aimed at improving or preventing chronic diseases among older Chinese adults.1, 8, 9, 10
Despite the growing number of RCTs targeting older Chinese adults, there has been little attention paid to understanding the process by which participants are recruited into these trials. Because the success of most RCTs involving exercise interventions depends primarily on the recruitment and retention of study participants, the extent to which target recruitment and retention goals are met can have a major impact on study costs, outcomes, and subsequent outreach of the intervention to the intended populations.11, 12, 13 Although the disease prevention literature readily acknowledges the difficulties and challenges inherent in recruiting study participants, especially older adults,12, 14 knowledge regarding best practices for 2 reaching populations in China for RCTs involving exercise interventions remains limited. With the pressing need for preventive interventions that might ward off chronic disease and improve the quality of life among older Chinese populations, it is critical that we increase our understanding of how to develop effective recruitment strategies, maximize intervention participation, and ensure the success of interventions.
This article attempts to fill this knowledge gap by describing and analyzing the recruitment process and outcomes of 2 community-based RCTs of exercise interventions involving older Chinese adults in Shanghai, China. In doing so, we summarize many of the recruitment issues encountered and offer recommendations for future studies.
2. Methods
This paper covers 2 previously published RCTs that evaluated 2 distinct exercise interventions conducted in Shanghai between 2012 and 2014. Details of the design, methodologies, and outcomes of each intervention are fully described elsewhere.15, 16 The protocol for each study was approved by the Shanghai University of Sport Ethics Committee. An informed written consent was obtained from each participant.
2.1. Community neighborhoods and target populations
The study area covered 2 administrative divisions (Wujiaochang Town and Yinhang Neighborhood Association) in the Yangpu district, Shanghai. The 2 divisions comprised 89 residential committees (subdivisions under the jurisdiction of towns or neighborhoods), 10 of which were targeted for participant recruitment by researchers conducting the 2 studies. The selection of these residential committees was based on (1) availability of classroom space for the interventions and (2) participant access to the research facility sponsoring the studies. In both interventions, the town office and neighborhood association were the initial contact points where recruitment approval was sought.
Both trials targeted community-dwelling older adults living in the study area defined. Specifically, the Tai Ji Quan for Osteoarthritis project targeted older women with knee osteoarthritis,15 whereas the Dumbbell for Healthy Brain project targeted individuals with mild cognitive impairment.16
2.2. General recruitment strategies
Although most RCTs use either community-wide promotions17 or referrals for recruiting participants,18, 19 the 2 studies described here used a top-down approach. That is, local community administrative authorities (i.e., local town offices or neighborhood associations) were first asked for permission to recruit community-dwelling older adult residents living in these neighborhoods.
Once permission was granted from a town office or neighborhood association, recruitment efforts started at the level of local residential committees, which helped coordinate and assist in initial recruitment efforts. Methods of recruitment included phone calls, promotional meetings, in-person contacts, and word of mouth. These efforts resulted in a list of potential volunteers who expressed an interest in participating. The list was then provided to the researchers, who arranged for screening, recruitment, group assignment, and baseline assessment, all of which took place at a designated research facility. The following provides a detailed description of the recruitment process for each of the 2 RCTs.
2.3. Tai Ji Quan for Osteoarthritis
The local town office was first approached by research staff members, who inquired about the possibility and feasibility of conducting an exercise project in the study area. At the same time, a list of the potential residential committees was compiled in consultation with an administrator, along with information on the number of older adults living in the neighborhoods and the availability of exercise facilities.
After this initial step, research staff contacted representatives at 4 local residential committees to explain the research activities in more detail and to seek permission to conduct the study. After permission was granted, the residential committees, using the recruitment methods described earlier, took the lead in mobilizing the residents at each residential complex by encouraging them to sign up for the research project.
After the sign-up list was generated, research staff used it to conduct a formal prescreening per the study's inclusion and exclusion eligibility criteria. At that time, a medical doctor performed a second screening (including radiography at a local hospital) to verify osteoarthritis. Those who qualified per study criteria were then scheduled to visit a laboratory where the study assessment and intervention activities were further detailed and explained.
On agreeing to participate, each participant signed an informed consent form. Participants were then assigned to either the Tai Ji Quan group or the control group, and a baseline assessment was conducted. A total of 46 participants were needed to achieve an adequate power analysis.15 To meet this target enrollment number, recruitment was conducted in waves between 2012 and 2013.
Recruitment costs were documented, including project staff time specifically devoted to participant recruitment, diagnosis of knee condition conducted by medical experts as part of recruitment eligibility screening, and remuneration made to neighborhoods and individuals during the recruitment process.
2.4. Dumbbell for Healthy Brain
A recruitment strategy similar to the one used for the osteoarthritis study was used in this study. Specifically, research staff made initial contact with a leader of a local neighborhood association where the study was to be conducted. The leader then contacted 6 local residential committees within the study area and requested that they assist in recruitment for the project. After agreeing to do so, the residential committees took the lead using the recruitment methods described earlier to encourage residents at each residential complex to sign up for the research project.
After a list of potential participants was generated, it was given to research staff members, who made initial contact with each individual via phone call. During the call, potential participants were prescreened to ensure that they met study eligibility criteria and understood the general procedures involved in the study. Those who qualified were scheduled for a laboratory visit, where the study assessment and intervention activities were further detailed and explained. Upon agreeing to participate, an informed consent form was obtained from each participant. Individuals were then assigned to either the dumbbell group or the control group, and baseline assessments were conducted. Forty-five participants were needed per the study's power analysis.16 Recruitment took place in waves between 2013 and 2014.
Cost information for this project was also documented, including remunerations made to neighborhood and residential committees and participants, research staff expenses, cost of maintaining research records, and cost of transportation services for participants traveling to and from the research laboratory.
2.5. Data analysis
For data analysis, the following information was recorded: number of neighborhood and residential committees invited to participate, number of committees that agreed to participate in the recruitment effort, number of recruitment days required, number of potential participants recruited, and recruitment costs. All numbers were tabulated and summarized in Excel spreadsheets (Office 2016; Microsoft, Redmond, WA, USA).
3. Results
3.1. Tai Ji Quan for Osteoarthritis
A chart that describes the recruitment process and group allocation is shown in Fig. 1. Of the 4 residential committees approached, 3 agreed to offer recruitment assistance, and 1 was excluded owing to the unusually low number of older adult residents in that neighborhood. A total of 238 individuals from the 3 participating residential committees signed up for the research project. Initial prescreening identified 103 individuals who did not meet the basic study criteria and thus were subsequently excluded. The remaining 135 individuals underwent further screening for eligibility, and 89 of those were found to be ineligible primarily (i.e., not having a diagnosis of knee osteoarthritis, too physically activity, unavailable/time conflict, and unwilling to accept protocol). A total of 46 individuals qualified for the study. After signing a consent form, the participants were randomized into 2 intervention conditions, 23 in the Tai Ji Quan group and 23 in the control group.
Fig. 1.
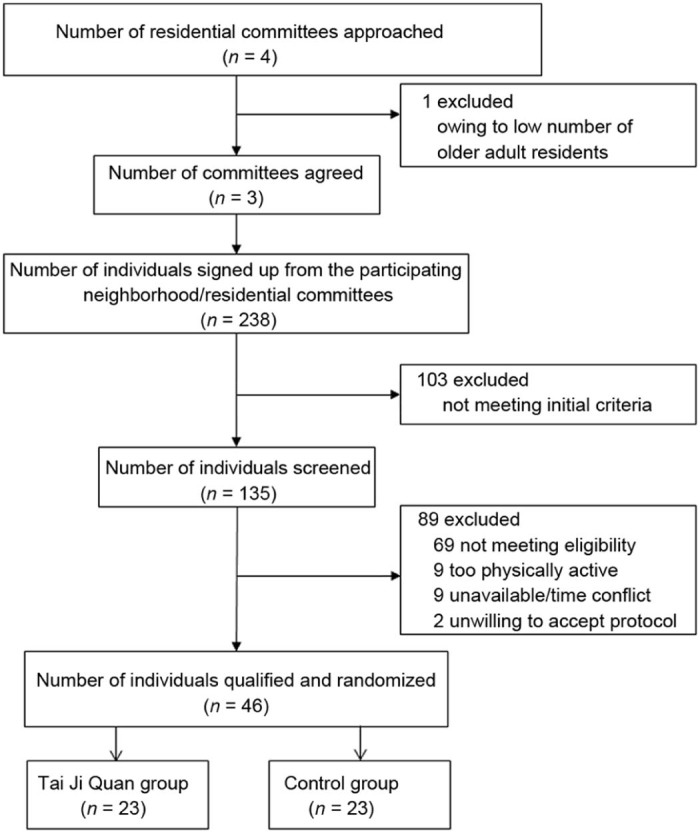
Recruitment flow chart for the Tai Ji Quan for Osteoarthritis study.
The overall recruitment took about 12 months, with 3 staggered waves of recruitment activities. The top portion of Table 1 summarizes the recruitment activities for each wave of this project. Overall, the recruitment became more efficient in terms of the number of days taken to recruit potential participants as the recruitment effort progressed. The number of days taken to recruit an initial pool of subjects was reduced from 112 days in Wave 1 to 56 days in Wave 3. Recruitment became more effective and efficient in the last wave, with the smallest screening-to-enrollment ratio being observed in Wave 3 (3:1 in Wave 1, 3:1 in Wave 2, and 2:1 in Wave 3).
Table 1.
Recruitment information for each study.
| Recruitment | Wave of recruitment | |||
|---|---|---|---|---|
| Wave 1 | Wave 2 | Wave 3 | Wave 4 | |
| Tai Ji Quan for Osteoarthrosis | ||||
| Days taken to recruit potential participants | 112 | 85 | 56 | NA |
| Number of participants recruited | 42 | 58 | 35 | NA |
| Number of participants enrolled in the study | 13 | 18 | 15 | NA |
| Dumbbell for Healthy Brain | ||||
| Days taken to recruit potential participants | 61 | 156 | 39 | 21 |
| Number of participants recruited | 30 | 99 | 60 | 31 |
| Number of participants enrolled in the study | 0 | 6 | 24 | 15 |
Abbreviation: NA = not applicable.
With respect to intervention retention, by the end of the 6-month intervention, a total of 6 participants had dropped out, 2 in the intervention group (8.70%) and 4 in the control group (17.39%), owing either to time conflicts or to health-related issues. The study had an overall retention rate of 87.0%.
Recruitment costs for the project are summarized in Table 2. In total, the study cost about RMB 48,767 (about USD 7866), including costs of magnetic resonance imaging (MRI) testing; remuneration paid to participating communities (i.e., neighborhood or residential committees), medical personnel participants, and research staff; and expenses related to research records and transportation services for participants. Remunerations accounted for RMB 31,000 (about USD 5000, 63.57%) of the total expenses, and MRI testing amounted to RMB 16,360 (about USD 2639, 33.55%). For this project, the cost per initial recruit was RMB 361 (RMB 48,767/135 individuals, about USD 58) and RMB 1060 (RMB 48,767/46 individuals, about USD 171) per randomized participant.
Table 2.
Recruitment cost information for each study (RMB).
| Wave of recruitment | Tai Ji Quan for Osteoarthritis | Dumbbell for Healthy Brain | |||||
|---|---|---|---|---|---|---|---|
| Wave 1 | Wave 2 | Wave 3 | Wave 1 | Wave 2 | Wave 3 | Wave 4 | |
| MRI testing | 3960 | 8700 | 3700 | NA | NA | NA | NA |
| Remuneration | |||||||
| Neighborhood associations/residential committees | 600 | 800 | 600 | 400 | 800 | 400 | 200 |
| Medical personnel | 2600 | 2800 | 2600 | NA | NA | NA | NA |
| Research staff | 8000 | 5000 | 3000 | 860 | 3100 | 4200 | 1950 |
| Participants | 1540 | 2120 | 1340 | 532 | 1852 | 1320 | 660 |
| Research records | 378 | 464 | 285 | 240 | 900 | 450 | 225 |
| Transportation | 280 | NA | NA | 56 | 112 | 90 | 84 |
| Total | 48,767 | 18,431 | |||||
Abbreviations: MRI = magnetic resonance imaging; NA = not applicable.
3.2. Dumbbell for Healthy Brain
Fig. 2 shows the recruitment process and group allocation for the Dumbbell for Healthy Brain project. Of the 6 residential committees initially approached, 4 decided to participate and offered recruitment assistance. The other 2 were excluded—one was unwilling to participate, and the other was considered unsuitable owing to lack of space.
Fig. 2.
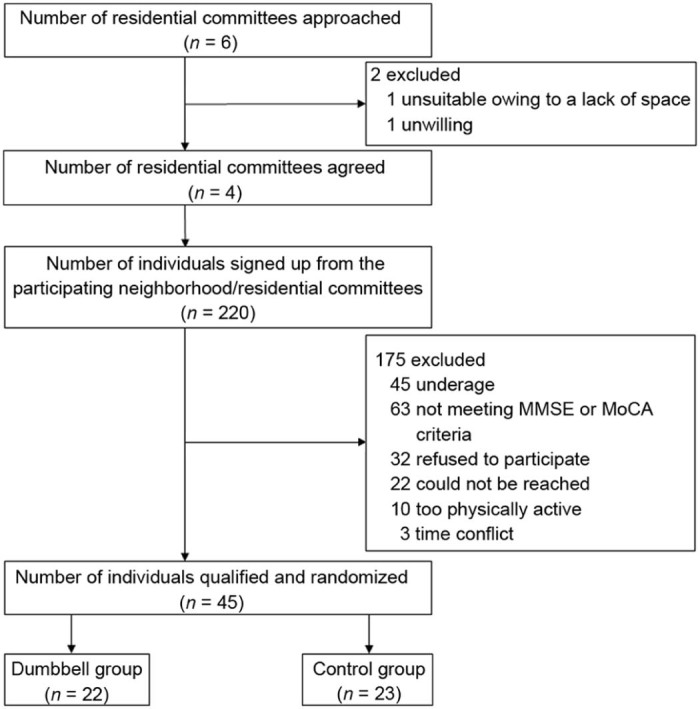
Recruitment flow chart for the Dumbbell for Healthy Brain study. MMSE = Mini-Mental State Examination; MoCA = Montreal Cognitive Assessment.
From the 4 residential committees assisting in recruitment, a total of 220 residents signed up for the project. After initial screening, 175 individuals were excluded for reasons of not meeting the study criteria. A total of 45 individuals qualified for the study, with 22 assigned to the dumbbell intervention group and 23 assigned to the control group.
It took a total of 4 waves of recruitment to enroll the target number of study participants (Table 1). Although there was some overall variation across the 4 waves, the recruitment became more efficient over time in terms of number of days taken, number of individuals recruited, and number of participants enrolled. It is worth noting that in Wave 1, a 2-month recruitment effort resulted in no qualified participants being enrolled in the project. Subsequent recruitment waves yielded much better results: Wave 2 took 156 days to enroll 6 participants, Wave 3 took 39 days to enroll 24 participants, and Wave 4 took 21 days to enroll 15 participants. Improvements in screening-to-enrollment ratios in the last 3 waves also occurred: 16.5:1 in Wave 2, 2.5:1 in Wave 3, and 2.1:1 in Wave 4.
After the 3-month intervention, 3 participants were lost to follow-up: 1 in the intervention group (4.5%) and 2 in the control group (8.7%). The study had an overall retention rate of 93%.
Recruitment costs for this project are summarized in Table 2. The study had a total direct cost of RMB 18,431 (about USD 2973), with most expenses related to participant remuneration during the recruitment process and to instructors' training (RMB 16,274, 88.30%). The project cost RMB 83 (about USD 13, RMB 18,431/220 individuals) for each initial recruit and RMB 409 (about USD 66, RMB 18,431/45 individuals) per randomized participant.
4. Discussion
In this article, we report on the recruitment process, outcomes, and strategies used in 2 RCTs involving exercise interventions conducted in Shanghai, China. The top-down recruitment strategy was shown to be effective in both studies in that they successfully achieved their planned target number of older adult participants and demonstrated an excellent retention rate. The recruitment became more effective and efficient as each project progressed, with notable improvement made in the screening-to-enrollment ratios.
Because both studies were designed to be scientifically controlled trials, stringent inclusion and exclusion criteria for each intervention were applied in recruiting study participants, which resulted in a large proportion of individuals being excluded using the community-based recruitment strategy (81% for Tai Ji Quan for Osteoarthritis and 80% for Dumbbell for Healthy Brain) during the initial screening process. Each study had about a 5:1 screening-to-enrollment ratio (5.2:1 for Tai Ji Quan for Osteoarthritis and 4.9:1 for Dumbbell for Healthy Brain). This information could serve as useful preliminary data for planning future studies.
Costs related to recruitment from both projects were analyzed, with a higher cost documented for the Tai Ji Quan for Osteoarthritis study,15 presumably owing to medical-related expenses such as functional MRIs and services rendered by medical doctors in performing the medical procedures related to screening. In addition to expenses paid to research staff for efforts related to recruiting and screening, remuneration paid to communities during the initial phase and to participants during the recruitment process was another major cost item. Across both studies, the costs were generally higher per participant randomized (range RMB 409–1060) than per initial recruit (range RMB 83–361). The total combined costs for the 2 studies for the community-based recruitment strategy were about RMB 189 per initial recruit and RMB 738 per participant randomized. In the absence of any comparison data from other studies in China, the cost information from these 2 studies may serve as a baseline for planning future recruitment efforts.
In both studies, there were some notable issues and challenges encountered during the recruitment process. First, among residential committees and older adult dwellers, there was a general lack of awareness about the importance of participating in research studies. For example, when they were initially approached, a few neighborhood associations and residential committees expressed little interest in participating or showed a lack of knowledge about the importance of participating in exercise-based interventions. However, as a result of persistent efforts by research staff, some eventually agreed to participate. This issue seems to have become less problematic as the recruitment effort progressed and as the research staff became better at explaining the nature and benefit of the study to the community.
Second, because of randomization at the individual level, it was sometimes difficult to control for “contamination” among participants living in the same residential area. For example, because of the close proximity of their residences, participants in the intervention group sometimes interacted with participants in the control group, thereby possibly influencing or changing the behaviors of control participants. Such incidents may happen on a regular basis and are difficult to avoid because residential committees often organize structured activities and meetings, thus allowing for active social interactions among residents of the same neighborhood or residential complex.
Third, a lack of understanding of research protocols appears to be common among some older adult participants. For example, a fair number of older adults refused to participate or to be randomized, asking “why is it necessary?” or questioning the need for randomization. Compared with Western countries, RCTs remain relatively uncommon among older adults living in Chinese communities. Therefore, there is a need for better education in such communities and among older residents regarding the value and benefits derived from conducting scientifically based exercise studies and the importance of establishing evidence-based prevention interventions as part of community preventative services for older Chinese adults.
4.1. Strengths and limitations of the studies
The use of residential neighborhoods as a primary resource for recruitment is unique and represents a strength. Similarly, the successful recruitment and retention in both studies may enhance dissemination and translational goals of these interventions. One notable limitation is that the studies used only 1 recruitment method. Even though both studies achieved their target enrollment numbers, it is unclear whether a single recruitment approach would work equally well in other cities or regions of China or among harder-to-reach populations (e.g., people with significant mobility issues). A second limitation is that the recruitment strategies were not tested in advance, nor were they guided by manuals of operation that clearly specified contact and screening methods prior to the start of the trial. Thus, there was a trial-and-error element that may have lengthened the learning curve regarding recruitment in each study, as is shown by the improved efficiency in the recruitment process as later recruitment waves took place (Table 1).
4.2. Lessons learned
The various lessons learned from analyzing the recruitment process for the 2 community-based exercise interventions are summarized here.
-
•
For both studies, it was important to engage core community stakeholders (e.g., neighborhood associations and residential committees) months prior to the start of the project to explain the goals and assess the needs and preferences of potential participants.
-
•
Not having a detailed manual of operations prior to the start of recruitment increased the time, effort, and cost of recruitment. Although adjustments were made along the way that improved the efficiency of recruiting, planning ahead and having a detailed strategic plan for engaging community leaders at various levels in community neighborhoods would have been extremely helpful.
-
•
Pilot testing the interventions in advance with a small number of eligible participants was particularly helpful in determining various aspects of recruitment and implementation feasibility. Such an effort made the recruitment more effective (i.e., in achieving the recruitment goals) and more efficient (i.e., in reducing costs and time) because the researchers were more familiar with the environment and more skillful in their recruitment operations.
-
•
Regular monitoring for possible contamination across the intervention conditions was important to gauge intervention fidelity.
-
•
Frequent contacts and interactions with core community stakeholders were important in building a trusting andcollaborative relationship with community leaders. This helped to maximize access to the potential target populations.
-
•
Research staff members were trained in using effective communication skills with community leaders and older adults, which helped facilitate the recruitment process and improve outcomes.
-
•
Careful attention was paid to providing potential participants with details regarding the protocols for the studies, including need for randomization, specifics of interventions, and time commitment. This enhanced participation because it clarified the need for the study and the degree of involvement and commitment that participating in the study required.
-
•
Remunerations to community stakeholders and gatekeepers were important in facilitating the recruitment process. Remunerations enabled these individuals to offer their time and commitment in coordinating recruitment efforts in their local communities. Likewise, incentives to participants that covered their costs for transportation and time spent in completing laboratory assessments greatly enhanced their willingness to participate in the study.
4.3. Recommendations
Based on our analysis of the recruitment process in the 2 intervention studies, the following recommendations are made for planning future RCTs involving community-dwelling older Chinese adults.
4.3.1. Engage with community stakeholders
Establish relationships with community stakeholders (gatekeepers) from town offices, neighborhood associations, residential committees, and group committees where the study is planned. We should build administrative support early in the study's planning stages. Once the collaborative working relationship is established, regular contact and interactions with these gatekeepers are encouraged to foster long-term trust and credibility, which may lead to increased access to potential participants. Researchers should also consider sharing the study results in formats most useful to the community stakeholders and older adults.
4.3.2. Conduct feasibility studies
During the planning stages, it is important to conduct feasibility studies that assess access to study communities, participants, and facilities (e.g., exercise rooms). Such an effort should include initial contacts with local neighborhood and residential entities and focus-group activities involving the intended study populations. A neighborhood-specific plan may be needed to accommodate various organizational needs and availability of resources. A strong feasibility study will ensure pragmatic expectations about the conduct of a trial in a specific community and help accomplish the recruitment goal within timelines.
4.3.3. Set realistic recruitment expectations
Setting a clear recruitment expectation is an important part of the recruitment plan, and the plan should be pilot tested before recruitment begins. For example, researchers should have a clear expectation of the number of targeted older adults who might be recruited from a defined study area; the number of individuals who might not meet the prescreening study criteria (e.g., required age range or frail medical status); the number of individuals who might decline to participate; the number of individuals who might fail to meet the study eligibility criteria, including those who may refuse to be randomized; and the number of anticipated dropouts for preventable or unpreventable reasons.
4.3.4. Avoid intervention contamination
When an intervention takes place within a single social or residential unit (e.g., neighborhood or residential area), caution needs to be taken to avoid contamination between study conditions. One solution to the problem is the use of cluster RCTs in which residential committees are used as the unit of randomization to allocate clusters of residents to the intervention arms of the trial.20
4.3.5. Clarify the informed consent process
Most trials involve a significant time commitment to complete study intake assessments and participate in the interventions. It is therefore important that informed consent be fully explained to potential participants. This includes reviewing the study procedures and answering any questions regarding study eligibility, randomization, assessment, and exercise activities. Consent should be verified by asking individuals to explain in their own words what the study is about and what the procedures entail. This will ensure that individuals understand the research process before they sign the consent form. Such an effort will likely reduce the study's attrition rate.
4.3.6. Offer remunerations
Careful consideration of appropriate remunerations to community stakeholders and participants (in the form of cash, gift cards, or vouchers) as a token of appreciation for their time may greatly facilitate recruitment efforts. Such expenses must be part of the approved research project budget and should not influence or enhance intervention compliance or act as coercion for compliance.
5. Conclusion
In describing and analyzing the recruitment process and outcomes of 2 completed community-based exercise intervention RCTs, this article highlights various factors that may be considered in the design and development of RCTs involving exercise interventions for older adults in Chinese communities. With the increasing public health need for the development and evaluation of exercise-based disease prevention interventions to reduce the incidence of noncommunicable diseases among older Chinese adults, it is important that we understand the barriers and challenges to recruitment when designing and conducting future studies. It is essential that we apply the lessons learned from past research to current and future studies to maximize effectiveness and efficiency in the recruiting process.
Authors' contributions
LH participated in data acquisition, analysis, and interpretation in the study of Tai Ji Quan for Osteoarthritis. JL contributed to data acquisition, analysis, and interpretation in the study of Dumbbell for Healthy Brain. NC performed the medical screening to verify osteoarthritis. YL conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Competing interests
None of the authors declare competing finanical interest.
Acknowledgment
This study was supported by the Shanghai City Committee of Science and Technology Key Project (No. 12490503200) and the National Natural Science Foundation of China (No. 81572213, No. 11372194). The authors express sincere gratitude to Dr. Fuzhong Li for his detailed comments and assistance during the various stages of writing this manuscript.
Footnotes
Peer review under responsibility of Shanghai University of Sport.
References
- 1.Li F. Physical activity and health in the presence of China's economic growth: meeting the public health challenges of the aging population. J Sport Health Sci. 2016;5:258–269. doi: 10.1016/j.jshs.2016.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Min Y., Jiang L.X., Yan L.J.L., Wang L.H., Basu S., Wu Y.F. Tackling China's noncommunicable diseases: shared origins, costly consequences and the need for action. Chin Med J. 2015;128:839–843. doi: 10.4103/0366-6999.152690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tang S., Ehiri J., Long Q. China's biggest, most neglected health challenge: non-communicable diseases. Infect Dis Poverty. 2013;2:7. doi: 10.1186/2049-9957-2-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.The World Bank . World Bank; Washington DC: 2011. Toward a healthy and harmonious life in China: stemming the rising tide of non-communicable diseases.http://www.worldbank.org/content/dam/Worldbank/document/NCD_report_en.pdf; Available at. accessed 19.05.2016. [Google Scholar]
- 5.Bauman A., Merom D., Bull F.C., Buchner D.M., Fiatarone Singh M.A. Updating the evidence for physical activity: summative reviews of the epidemiological evidence, prevalence, and interventions to promote “active aging”. Gerontologist. 2016;56:268–280. doi: 10.1093/geront/gnw031. [DOI] [PubMed] [Google Scholar]
- 6.Garber C.E., Blissmer B., Deschenes M.R., Franklin B.A., Lamonte M.J., Lee I.M. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43:1334–1359. doi: 10.1249/MSS.0b013e318213fefb. [DOI] [PubMed] [Google Scholar]
- 7.World Health Organization Physical activity and older adults. http://www.who.int/dietphysicalactivity/factsheet_olderadults/en/ Available at. accessed 19.05.2016.
- 8.Guo Y., Shi H., Yu D., Qiu P. Health benefits of traditional Chinese sports and physical activity for older adults: a systematic review of evidence. J Sport Health Sci. 2016;5:270–280. doi: 10.1016/j.jshs.2016.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lü J., Fu W., Liu Y. Physical activity and cognitive function among older adults in China: a systematic review. J Sport Health Sci. 2016;5:287–296. doi: 10.1016/j.jshs.2016.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wang X.Q., Pi Y.L., Chen P.J., Liu Y., Wang R., Li X. Traditional Chinese exercise for cardiovascular disease: systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc. 2016;4:e002562. doi: 10.1161/JAHA.115.002562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Probstfield J.L., Frye R.L. Strategies for recruitment and retention of participants in clinical trials. JAMA. 2011;306:1798–1799. doi: 10.1001/jama.2011.1544. [DOI] [PubMed] [Google Scholar]
- 12.Provencher V., Ben Mortenson W.B., Tanguay-Garneau L., Bélanger K., Dagenais M. Challenges and strategies pertaining to recruitment and retention of frail elderly in research studies: a systematic review. Arch Gerontol Geriatr. 2014;59:18–24. doi: 10.1016/j.archger.2014.03.006. [DOI] [PubMed] [Google Scholar]
- 13.McHenry J.C., Insel K.C., Einstein G.O., Vidrine A.N., Koerner K.M., Morrow D.G. Recruitment of older adults: success may be in the details. Gerontologist. 2015;55:845–853. doi: 10.1093/geront/gns079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bower P., Brueton V., Gamble C., Treweek S., Smith C.T., Young B. Interventions to improve recruitment and retention in clinical trials: a survey and workshop to assess current practice and future priorities. Trials. 2014;15:399. doi: 10.1186/1745-6215-15-399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhu Q., Huang L., Wu X., Wang L., Zhang Y., Fang M. Effects of Tai Ji Quan training on gait kinematics in older Chinese women with knee osteoarthritis: a randomized controlled trial. J Sport Health Sci. 2016;5:297–303. doi: 10.1016/j.jshs.2016.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lü J., Sun M., Liang L., Feng Y., Pan X., Liu Y. Effects of momentum-based dumbbell training on cognitive function in older adults with mild cognitive impairment: a pilot randomized controlled trial. Clin Interv Aging. 2015;11:9–16. doi: 10.2147/CIA.S96042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ory M.G., Lipman P.D., Karlen P.L., Gerety M.B., Stevens V.J., Singh M.A. Recruitment of older participants in frailty/injury prevention studies. Prev Sci. 2002;3:1–22. doi: 10.1023/a:1014610325059. [DOI] [PubMed] [Google Scholar]
- 18.Warren-Findlow J., Prohaska T.R., Freedman D. Challenges and opportunities in recruiting and retaining underrepresented populations into health promotion research. Gerontologist. 2003;43:37–46. doi: 10.1093/geront/43.suppl_1.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Brach M., Moschny A., Bücker B., Klaaβen-Mielke R., Trampisch M., Wilm S. Recruiting hard-to-reach subjects for exercise interventions: a multi-centre and multi-stage approach targeting general practitioners and their community-dwelling and mobility-limited patients. Int J Environ Res Public Health. 2013;10:6611–6629. doi: 10.3390/ijerph10126611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.DiGuiseppi C., Coupland C. The design and use of cluster randomised controlled trials in evaluating injury prevention interventions: part 1. Rationale, design and informed consent. Inj Prev. 2010;16:61–67. doi: 10.1136/ip.2009.023119. [DOI] [PubMed] [Google Scholar]