

Abstract
Background:
In Oman, a higher proportion of patients presented with breast cancer are relatively young age and with an advanced stage. This could be due to lack of awareness and knowledge about breast cancer among young women.
Aim:
To assess the breast cancer knowledge, awareness and factors associated with the practice of breast self-examination (BSE) among females in Buraimi, Oman.
Methods:
A cross-sectional survey was conducted among females attending the two days health exhibition event at a polyclinc, in Al-Buraimi, governorate. A pretested questionnaire to assess their knowledge, awareness and practices concerned to breast cancer was used. The collected data was categorized, analyzed using descriptive statistics and logistic regression model. All the statistical analysis was performed using SPSS 21.0 version.
Results:
Out of the total of one hundred and eighty nine (189) participants, 80% had information of breast cancer. Participants had better knowledge of symptoms but less knowledge about risk factors. When probed about BSE, only 43% performed it and only 21% of them do it monthly on regular basis. The main reasons for regular monthly BSE is mainly because of fear of breast cancer (9%), doctor's advice (6%) and awareness through media (5%).
Conclusion:
Our study participants showed insufficient knowledge in some areas related to sign and symptoms and risk factors of breast cancer and identified a negative influence of low knowledge on the practice of BSE. Thus, educational interventions need to be emphasized to provide comprehensive information of breast cancer.
Keywords: Awareness, breast cancer, breast self-examination, community-based, knowledge, Middle East, Oman, screening, young females
Introduction
Breast cancer is by far the most frequent cancer of women (23% of all cancers), ranking second overall when both sexes are considered together. It is the leading cause of cancer mortality in women and constitutes 14% of female cancer deaths.[1] The pattern of breast cancer in Arab countries is very disturbing.[2,3] In Oman, breast cancer is the most frequent malignant tumor diagnosed in females, parallel to established global data, and on an average, 100–150 new cases are reported annually.[4] The primary factors that increase the risk of breast cancer in women include certain inherited genetic mutations, a personal or family history of breast cancer, and biopsy-confirmed hyperplasia.[5] Since breast cancer is a progressive disease, small tumors are more likely to be at an early stage, and their early detection is more likely to have more successful treatment and a better prognosis.[6] The three screening tests usually considered for early detection are clinical breast examination (CBE), X-ray mammography, and breast self-examination (BSE).[7,8] In industrial countries, breast cancer mortality is declining where screening mammography is the standard for care.[9] BSE is appealing as a patient-centered, noninvasive screening procedure that allows women to become comfortable with their own bodies.[10] Regular performance of BSE does not mean that the breast cancer is necessarily self-detected. BSE increases body awareness so that there is heightened awareness of changes that may be detected during BSE or at some other time. The aim of this study was to evaluate the knowledge, attitude, and practice of breast cancer screening behaviors among females in Buraimi, Oman.
Materials and Methods
Study design and setting
This is a cross-sectional study conducted on female participants who have consented to participate in this research irrespective of their age, marital status, and education was included in the study. All the female participants who attended the health exhibition at Buraimi polyclinic were approached by the trained female interviewers from College of Health Sciences, Buraimi, Oman. All the female visitors, university students, and health workers attending this event were invited to participate in the survey. We included a total of 189 female participants who shared their responses during the study period were considered as our sample.
Study questionnaire
A predesigned self-administered questionnaire was used to collect the information from the teachers. The questionnaire was derived from other published studies dealing with the same topic as well as from our own experience. It included questions related to personal data and history of related health events. It also investigated the knowledge and awareness of teachers regarding breast cancer and their practice of screening procedures. The data collection process was made by the investigators themselves. The structured English form was first translated into Arabic by an author. This version was revised and translated back to English by another author and compared with the original form to ascertain the precision of translation. Knowledge about the risk of breast cancer was assessed by questionnaire items. These items included having had breast cancer once before, late age at first pregnancy, early onset of menstruation, having had a breast biopsy, having a family history of breast cancer, advanced age, and late-onset of menopause in addition to five items recently identified, namely breastfeeding, exposure to radiation, hormonal treatment, and high-fat diet and obesity.
The knowledge of women about the common screening methods (mammography, CBE, and BSE) was assessed by asking three questions. The source of knowledge was detected by asking the participant to define a source of her knowledge about breast cancer; it was permissible to give more than one source.
A pilot study was carried out on 30 female students (not included in the final study). This study was formulated with the following objectives: test the clarity of the questions, test the validity and applicability of the study tools, accommodate the aim of the work to actual feasibility, identify the difficulties that may be faced during the application, as well as study all the procedures and activities of the administrative aspects.
Ethical considerations
Ethical approval was taken from the Institutional Ethical Board of College of Health Sciences, University of Buraimi. A written format explaining the purpose of the research was explained by the interviewer to the participant, and oral consent was taken before enrolling in the study. To maintain confidentiality, questionnaires were made anonymous.
Statistical analysis
The statistical package for the social sciences (SPSS Statistics for Windows, Version 19.0. Armonk, IBM Corp., NY) was used for data processing. Simple descriptive statistics were used (mean ± standard deviation for quantitative variables, and frequency with percentage distribution for categorized variables). To find the most important factors considered as predictors of having satisfactory knowledge, a logistic regression analysis was used. A model was developed using all factors suspected to be associated with satisfactory knowledge level.
Results
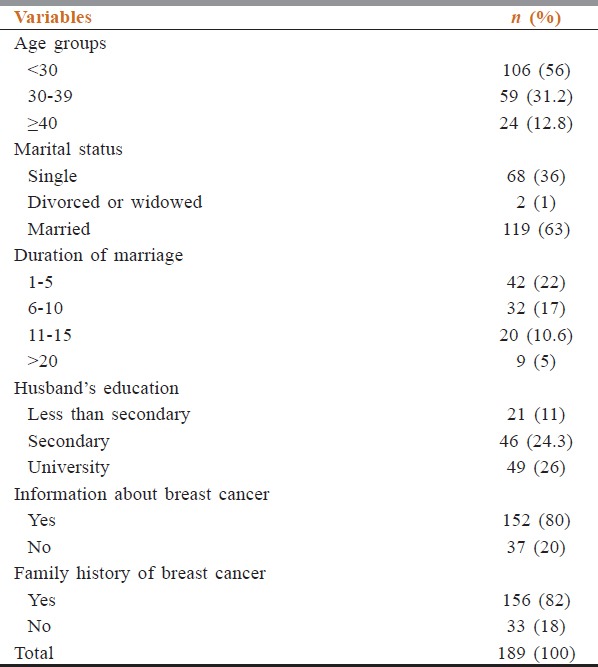
A total of 189 (n = 189) participants agreed to participate in the study and shared their responses to the questions in the questionnaires. Table 1 shows general characteristics of the study population. A majority of the participants in this study were married (n = 119, 63%) and the remaining were single (n = 68, 36%) and two were widowed/divorced. Their age ranged between 21 and 58 years. Most participants (87%) were aged <40 years and were ever married (64%). Of the total 121 who were ever married, around two-thirds of the participants (79/121) were married for more than 5 years. Most of husbands had secondary or university education (82%). About two-thirds (67.5%) of the participants had information about breast cancer.
Table 1.
Demographic characteristics of the study participants (n=189)
Participants’ knowledge regarding the symptoms and signs of breast cancer is shown in Table 2. A higher proportion of participants responded correctly the presence of breast mass (84%), breast pain (77%), and abnormal enlargement of breast (73.5%). Further, participants correctly identified smoking (74%), consumption of fatty foods (72.5%), family history of cancer (72%), personal hygiene (70%), and menopause age above 50 years (67.7%) are some of the important risk factors.
Table 2.
Participants knowledge about breast cancer (n=189)
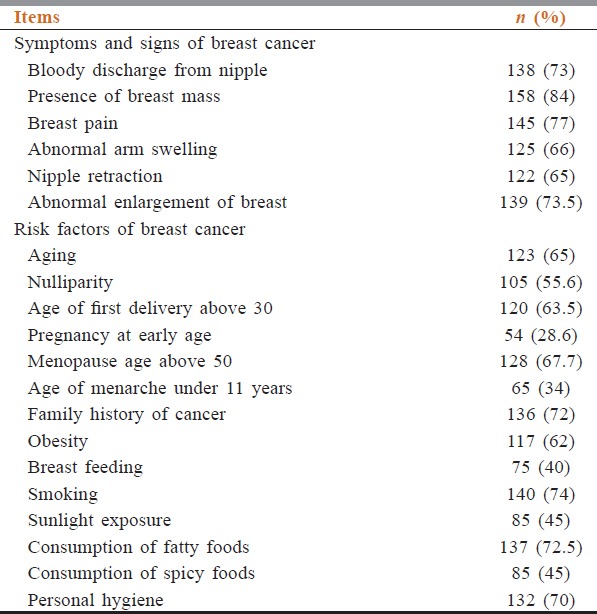
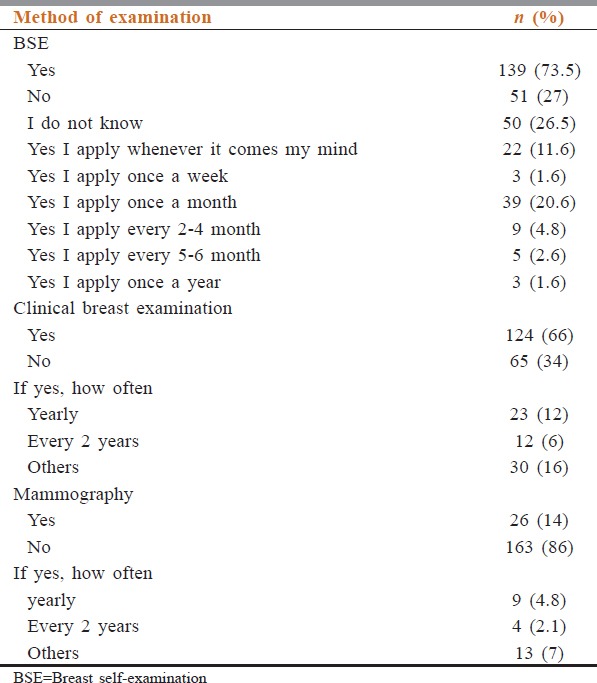
Table 3 illustrates participants’ knowledge and the frequency of application of breast examination. About three-fourth (73.5%) declared that they do know how to practice BSE, 20.6% expressed that they do self-examination of breast every month. In addition, 66% of the participants also underwent CBE, and only 14% reported that they underwent breast examination through mammography.
Table 3.
Knowledge and awareness about breast examination
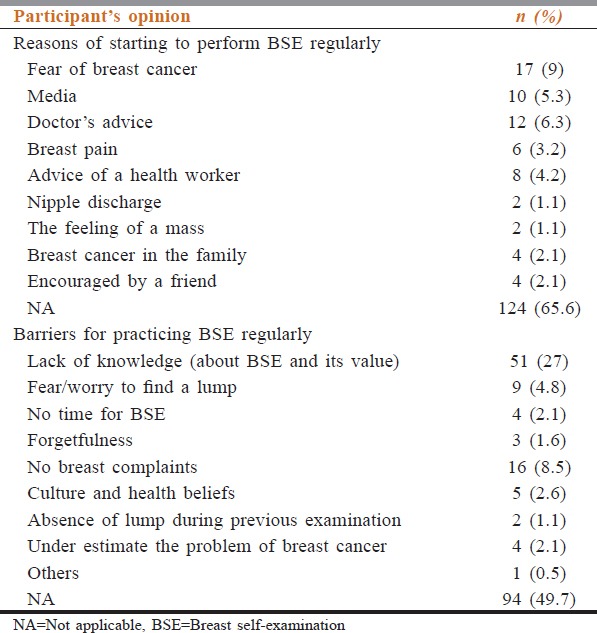
When requested the participants opinion about reasons of starting to perform BSE regularly, about 65.6% does not stated any reason, however, some participants stated its because of fear (9%), doctors advise (6.3%), and media broadcasting (5.3%) [Table 4]. Further, when asked about reasons for nonpracticing BSE regularly, participants’ answers included lack of knowledge about BSE and its value (27%), no breast complaints (8.5%), fear of finding a lump (4.8%), and no time for BSE (2.1%) are some of the barriers reported by the them.
Table 4.
Participants’ opinions about reasons of starting and barriers for practicing breast self-examination regularly
Discussion
This study demonstrated the knowledge and awareness of breast cancer among female participants ranged from little to adequate knowledge. The knowledge about the risk factors such as early age pregnancy, age of menarche under 11 years, nonbreastfeeding, and high sunlight exposure was not well recognized by the study participants. This might reflects the religious culture that encourages misconceptions concerning women opinions about the reasons of poor practicing of BSE. One of the major factors why most of the patients experience late presentation of breast cancer because most of the women do not carry BSE and not aware of undergoing screening for BSE. In this study, 27% of the respondents have never heard about BSE, while 66% of the respondents underwent CBE and only 14% were aware of mammography. This may be due to poor health education about the breast cancer in the society. Therefore, providing BSE education to all the females is warranted. Further, our respondents also have poor knowledge of the use of mammography as a screening tool for early detection of breast cancer. Health education about the benefits of mammography screening should be encouraged.
This study participants reported some of the barriers for participating BSE includes lack of knowledge and understanding of its value, thinking no breast complaints, and fear to find a lump. Our survey findings indicate that the women failed to obtain a mammography was the poor belief that examination is not important because of lack of educational programs to enhance women's perceived self-efficacy to have a mammography test.
Conclusion
The study points to the insufficient knowledge of the participants in some areas of knowledge related to sign and symptoms and barriers of breast cancer and identified the negative influence of low knowledge on the practice of BSE. Accordingly, relevant educational programs with the aim of improving the knowledge level of women regarding the breast cancer are needed considering the high prevalence of breast cancer among Omani females. At the same time, there is an urgent need for regular update courses for health staff, especially nurses about breast cancer education and various screening methods.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank Dr. J.F Thomas, the Dean of College of Health Sciences and the University administration for their support and encouragement. The authors also thank all the female students of University of Buraimi and the women who made this study successful through their active participation and contribution
References
- 1.Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. doi: 10.3322/canjclin.55.2.74. [DOI] [PubMed] [Google Scholar]
- 2.Amr SS, Sa’di AR, Ilahi F, Sheikh SS. The spectrum of breast diseases in Saudi Arab females: A 26 year pathological survey at Dhahran health center. Ann Saudi Med. 1995;15:125–32. doi: 10.5144/0256-4947.1995.125. [DOI] [PubMed] [Google Scholar]
- 3.Mansoor I. Profile of female breast lesions in Saudi Arabia. J Pak Med Assoc. 2001;51:243–7. [PubMed] [Google Scholar]
- 4.Chiedozi LC, El-Hag IA, Kollur SM. Breast diseases in the Northern region of Saudi Arabia. Saudi Med J. 2003;24:623–7. [PubMed] [Google Scholar]
- 5.Mehdi I, Monem EA, Al Bahrani BJ, Al Kharusi S, Nada AM, Al Lawati J, et al. Age at diagnosis of female breast cancer in Oman: Issues and implications. South Asian J Cancer. 2014;3:101–6. doi: 10.4103/2278-330X.130442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tabár L, Duffy SW, Vitak B, Chen HH, Prevost TC. The natural history of breast carcinoma: What have we learned from screening? Cancer. 1999;86:449–62. [PubMed] [Google Scholar]
- 7.Sherma CD, Hossfeld DK. Breast cancer in manual of oncology. In: Bosch FX, editor. International Union Against Cancer: Middle East. 5th ed. Berlin, Heidelberg, USA: Springer Verlag; 1990. pp. 257–76. [Google Scholar]
- 8.Siahpush M, Singh GK. Sociodemographic predictors of pap test receipt, currency and knowledge among Australian women. Prev Med. 2002;35:362–8. doi: 10.1006/pmed.2002.1086. [DOI] [PubMed] [Google Scholar]
- 9.Reynolds T. Declining breast cancer mortality: What's behind it? J Natl Cancer Inst. 1999;91:750–3. doi: 10.1093/jnci/91.9.750. [DOI] [PubMed] [Google Scholar]
- 10.Vainio H, Bianchini F. Vol. 7. Lyon (France): IARC Press; 2002. Breast Cancer Screening: International Agency for Research on Cancer (IARC) Handbooks of Cancer Prevention. [Google Scholar]