

Abstract
Malignant peritoneal mesothelioma (MPM) is a rare disease with a wide clinical spectrum. It arises from the peritoneal lining and commonly presents with diffuse, extensive spread throughout the abdomen and, more rarely, metastatic spread beyond the abdominal cavity. Computed tomography, magnetic resonance imaging and positron-emission tomography are important diagnostic tools used for the preoperative staging of MPM. The definitive diagnosis is based on histopathological analysis, mainly via immunohistochemistry. In this regard, paired-box gene 8 negativity represents a useful diagnostic biomarker for differentiating MPM from ovarian carcinoma. In addition, BRCA1-associated protein-1 (BAP1) loss is specific to MPM and allows it to be distinguished from both benign mesothelial lesions and ovarian serous tumors. Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) has become an increasingly important therapeutic approach, while systemic therapies are still being developed. Histology, Ki-67, completeness of cytoreduction, age, sex, and baseline thrombocytosis are commonly used to optimize patient selection for CRS with HIPEC. Additionally, it is well recognized that, compared to other subtypes, an epithelial morphology is associated with a favorable prognosis, whereas baseline thrombocytosis predicts an aggressive biologicalbehavior. Platelets and other immunologic cytokines have been evaluated as potential novel therapeutic targets. Epigenetic modifiers, including BAP1, SETD2 and DDX3X, are crucial in mesothelial tumorigenesis and provide opportunities for targeted treatment. Overexpression of the closely interacting phosphoinositide 3-kinase (PI3K) and the mammalian target of rapamycin (mTOR) pathways appears crucial in regulation of the malignant phenotype. The use of targeted therapies with PI3K-mTOR-based inhibitors requires further clinical assessment as a novel approach.
Keywords: Peritoneal, mesothelioma, cytoreductive surgery, heated intraperitoneal chemotherapy, genomic profiling
Introduction
Mesothelioma arises primarily from the mesothelial cells of the serosal membrane lining the pleural, peritoneal and pericardial cavities, and the tunica vaginalis. Among the various types of mesothelioma, diffuse malignant peritoneal mesothelioma (MPM) accounts for nearly one-fourth of cases, with an estimated annual incidence of 2500 cases worldwide [1]. MPM is a heterogeneous, aggressive tumor mainly caused by exposure to asbestos or other carcinogens such as talcum; 33% of diagnosed patients have a history of asbestos exposure, a clearly lower rate than that in patients with malignant pleural mesothelioma [2]. Chronic peritonitis is a less clear risk factor [3]. Patients with MPM are more commonly female, of younger age, and have a better prognosis than those with pleural mesothelioma [4]. The disease typically presents with non-specific features, including abdominal pain, palpable pelvic masses, altered bowel habit, tumor nodules of variable size located diffusely throughout the peritoneal cavity, and massive malignant ascites [5]. The morphologic appearance ranges from epithelioid to sarcomatoid and biphasic subtypes. Among these, epithelioid tumors have a better prognosis [6].
Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) is a treatment option for patients with good performance status and potentially resectable disease [7,8]. Despite improved outcomes and the comparatively long-term survival, the combined therapy is associated with significant perioperative morbidity in more than half of patients [9]. Treatment for inoperable MPM consists of palliative chemotherapy with pemetrexed, cisplatin and gemcitabine, either alone or in combination, whereas second-line therapy is currently not defined [10].
Given the limited therapeutic options in the advanced setting, the prognosis remains dismal, with median survival reported to be one year in a historical series [11] and 13 months in a multicenter registry study [12]. This article provides an overview of our current knowledge concerning the epidemiology, clinical presentation, diagnosis, pathology, genetics, therapeutic interventions and prognostic factors of MPM.
Materials and methods
The PubMed database was searched using the terms “peritoneal, mesothelioma”, “pleural, mesothelioma”, “immunohistochemistry, mesothelioma”, “genomic profiling, mesothelioma”, “treatment, mesothelioma”, and “prognosis, mesothelioma”. Publications between September 1999 and February 2018 were eligible for inclusion. Case series of patients with MPM describing diagnostic and therapeutic considerations along with targeted approaches were also included in this study.
Epidemiology
The incidence of MPM has been increasing since the 1970s and its mortality increased by 2.78% each year from 1994-2008 [3,13]. It currently represents the second most common site of malignant mesothelioma, accounting for 20% of reported cases [14]. Slight differences in incidence rates among western countries have been described, ranging from 0.5-3 cases per million [15]. The UK reports the highest incidence, estimated at 3.6 and 0.7 cases per 100,000 people for men and women, respectively [16].
The reported female-to-male ratio for MPM is 0.70 [17]. Interestingly, female patients live significantly longer than male patients, which suggests that sex has substantial prognostic relevance [18,19]. Patients with MPM are significantly younger, and have a shorter median overall survival (OS) than those with the pleural variant (mean age, 63.3 versus 70.8 years, respectively). In addition, females diagnosed with MPM live significantly longer than male patients; no racial predilection has been described [18].
Etiology
The main carcinogen leading to the development of MPM is asbestos; nevertheless, only 33-50% of patients diagnosed with MPM report prior exposure to asbestos [15]. The long latency between asbestos contact and the onset of mesothelioma implies that the incidence of this disease will continue to increase in the future [20]. Several additional environmental factors have been implicated, including talc, mica, erionite (volcanic ash), and thorotrast. In addition, Hodgkin's disease, chronic peritonitis and exposure to therapeutic radiation have been correlated with MPM [15].
Clinical presentation
MPM is usually diagnosed at an advanced stage, probably because disease manifestations are non-specific in the early stage. Clinical presentation is quite variable, depending on the extent of tumor spread within the abdominal cavity. Accumulation of ascites and growth of tumor masses result in abdominal distension in 30-80% of patients. Abdominal pain is the second most common presenting symptom in approximately 27-58% of cases [16]. The typical growth pattern of MPM is diffuse, rather than infiltrative [21]. Swelling of lymph nodes due to local involvement may lead to the obstruction of the superior vena cava, while an acute abdomen can be caused by malignant bowel obstruction or perforation[22]. Patients may also suffer from unspecific symptoms, such as early satiety, anorexia, weight loss, vomiting, constipation, and/or diarrhea. Less common complaints include new-onset hernia, fever of unknown origin and night sweats [23]. Nevertheless, approximately 8% of patients are diagnosed incidentally [24].
Diagnostic considerations
The precise diagnosis of MPM is based on a detailed medical history, followed by radiological, laboratory, and pathological examinations. Computed tomography (CT), magnetic resonance imaging (MRI), and positron-emission tomography (PET) are the main imaging modalities used; nevertheless, there is no pathognomonic imaging finding for MPM. CT scan may reveal a solid, heterogeneous, soft-tissue mass with irregular margins and demonstrate high contrast between the enhanced tumor and the non-enhanced ascites [25]. Peritoneal and mesenterial thickening are also frequent findings [12]. Since extra-abdominal spread is uncommon, further imaging is rarely indicated. Diffusion-weighted and dynamic gadolinium-enhanced MRI may demonstrate more accurately the extent of the disease, but these modalities are not implemented routinely [26]. PET scanning provides information about the stage of MPM for preoperative patients and allows the detection of lymph node involvement, which may be undetectable on CT scan [3]. PET can also detect potential recurrent disease with more sensitivity [27]. Based on cross-sectional imaging, the differential diagnosis for MPM may include peritoneal carcinomatosis, serous peritoneal, and ovarian carcinoma, as well as lymphomatosis and tuberculous peritonitis.
Biopsy is essential for establishing diagnosis and can be performed either radiographically or surgically. Laparoscopy represents a preferable diagnostic approach, considering its lower invasiveness and clear intraoperative assessment [12,28]. Whereas the wall of the mobile small bowel is typically not involved in peritoneal carcinomatosis, during either laparoscopy or laparotomy in patients with no medical history of abdominal operations, the serosal layer of the small bowel wall, consisting of mesothelial cells, is commonly diffusely involved. The mesentery is involved in both cases.
CA-125 and CA 15-3 baseline levels are elevated in 53.3% and 48.5% of patients, respectively [29]. Serum mesothelin-related protein has a higher sensitivity of 60% [30], whereas serum high-mobility group box 1 (HMGB1), hyaluronic acid, and osteopontin could be useful markers for monitoring disease recurrence [29].
Histology and immunohistochemistry
Histologically, MPM is divided into epithelioid, sarcomatoid, and biphasic subtypes. Among these, epithelioid is the most common, representing 75-90% of reported cases, and is associated with the best prognosis, as mentioned above [6]. Approximately 25% of MPMs are biphasic, while the sarcomatoid subtype is extremely rare. The epithelioid subtype is composed of cells that resemble normal mesothelial cells in a predominantly tubulopapillary or trabecular pattern with uncommon mitotic figures. The biphasic subtype consists of both epithelioid and sarcomatoid elements, with each component contributing at least 10% of the overall histology [31]. The sarcomatoid subtype is composed of tightly arranged spindle cells with sporadic malignant osteoid, chondroid or muscular features. The prognosis of biphasic and sarcomatoid subtypes is significantly worse, similar to that of the corresponding pleural mesothelioma variants [3,32].
The diagnosis of MPM based entirely on histologic patterns may be challenging; thus, immunohistochemical panels are usually used and can provide the more sensitive and specific information needed for an accurate diagnosis (Fig. 1). In addition, there is increasing interest in using markers relatively tissue-specific transcription factors. Furthermore, the optimal immunohistochemical panel for distinguishing MPM from ovarian serous tumors remains to be clearly defined. There is a general consensus that EMA, calretinin, CK5/6, Wilms tumor 1 (WT-1), HBME-1, thrombomodulin, podoplanin, mesothelin, and D2-40 are immunoreactive in MPM. However, WT1 [33,34], D2-40 [35], calretinin [32], and cytokeratin 5/6 [36] can also be positive in the majority of serous carcinomas. On the other hand, TTF1, CEA, Ber-Ep4, LeuM1, B72.3, MOC31 and cluster of differentiation (CD) 15 are commonly expressed in adenocarcinoma rather than mesothelioma [37]. Overall, it is recommended to use at least two mesothelioma markers and two carcinoma markers [3,38].
Figure 1.
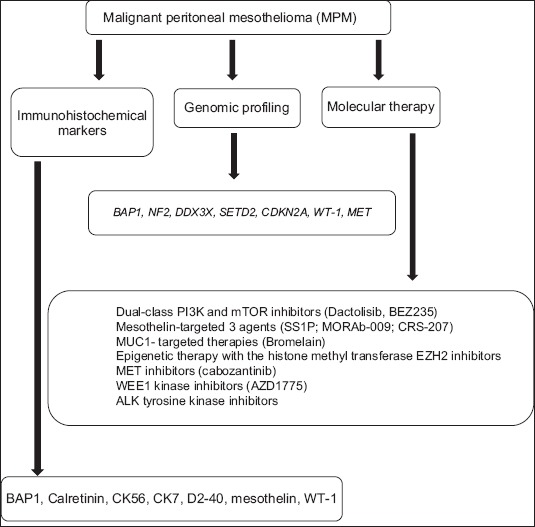
Immunohistochemical and molecular profiling and molecular therapies of malignant peritoneal mesothelioma (MPM)
Genomic profiling of MPM
The genetic alterations that drive mesotheliomas occur at distinct frequencies depending on the anatomic origin of the tumor. One study revealed chromosome 9p21 deletion more frequently in pleural than in peritoneal tumors (85% vs. 36%), whereas 5p15 and 7p12 gains were more common in peritoneal than in pleural tumors [39].
BAP1 is a tumor-suppressor gene that enhances BRCA1-mediated cell growth suppression, which plays a significant role in the organogenesis of the Müllerian system [40]. It is expressed in a variety of ovarian tumors, particularly serous carcinoma, and has been established as a sensitive and specific marker for ovarian serous carcinomas, as well as an important parameter in the differential diagnosis with MPM. Its sensitivity ranges between 90% and 100% [41]. The expression of PAX8 in the Müllerian lesions is generally strong and diffuse. However, PAX8 is expressed in only a small minority of MPMs, according to the limited relevant literature available [41].
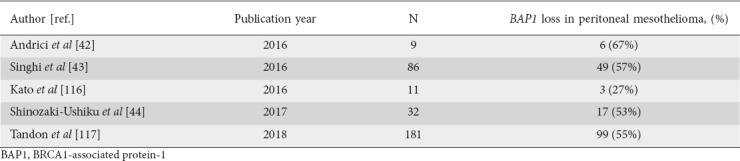
BAP1 is lost in almost 50% of pleural mesotheliomas and two thirds of MPMs, but in less than 1% of high-grade serous carcinomas [42]. Table 1 depicts the available studies that reported a loss of BAP1 in MPM. One study identified that frequent loss of BAP1 immunostaining in MPM did not affect significantly the outcome [43]. Therefore, loss of nuclear BAP1 confirm the diagnosis of MPM but does not offer prognostic information. On the other hand, preservation of BAP1 cannot distinguish MPM from other Müllerian lesions, because of its suboptimal sensitivity [42,44]. Cytogenetically, 40-70% of both pleural and peritoneal mesotheliomas harbor a loss of 9p including cyclin-dependent kinase activator inhibitor 2A (CDKN2A), or 22q including NF2 [43]. The combination of homozygous CDKN2A deletion and hemizygous NF2 loss in MPM is an independent prognostic factor, associated with shorter progression-free survival (PFS) and OS. In addition, tumor suppressor gene BAP1 mutation can predispose to MPM. An array comparative genomic hybridization study involving 33 MPM patients revealed focal deletions affecting BAP1 and CDKN2A in 61% and 33% of cases, respectively, suggesting that similar genetic alterations drive MPM and pleural mesothelioma but at different frequencies [45]. The genomic profiling of patients with MPM is summarized in Fig. 1.
Table 1.
BAP1 loss in peritoneal mesothelioma
Limited evidence is currently available for the functional role of specific microRNAs (miRNAs) in MPM [46]. It has been suggested that miR-380-5p—a miRNA normally negligibly expressed in telomerase-positive MPM tissues—may interfere with telomerase activity and promotes cell growth impairment and induction of apoptosis in relevant models of MPM [47].
Treatment options
Surgical therapy
Given the rarity of MPM, data on the best treatment strategies have been based mostly on single institutional retrospective reports [15]. In the absence of coexisting medical conditions that would increase surgical risk, CRS is a reasonable approach. Surgery must be performed by an experienced surgical team; peritonectomy could be either limited to peritoneal surfaces visibly infiltrated by the disease or extended in the case of total parietal peritonectomy [48]. There is some controversy about the implementation of these two strategies. In a controlled study, the reported 5-year survival rates of selective versus parietal peritonectomy were 40% and 63.9%, respectively (P=0.0269) [49]. The complete parietal peritonectomy was performed without increasing post-surgical morbidity or mortality.
MPM has a specific pattern of intraperitoneal dissemination. Parietal peritoneal surfaces are typically diffusely involved, which may necessitate extensive peritonectomy. The perihepatic regions may pose a substantial challenge, specifically the posterior aspect of the hepatoduodenal ligament. The extensive involvement of small- and large-bowel mesenteries is generally not amenable to cytoreduction.
The presence of lymph node metastases has been demonstrated to be a negative prognostic factor for survival [50]. All enlarged lymph nodes should be removed and assessed histologically. Lymph node groups that have been recommended for histopathologic evaluation include the deep epigastric lymph nodes, external, internal and common iliac lymph nodes, as well as lymph nodes at the origin of the gastroepiploic vessels [50,51].
CRS and HIPEC
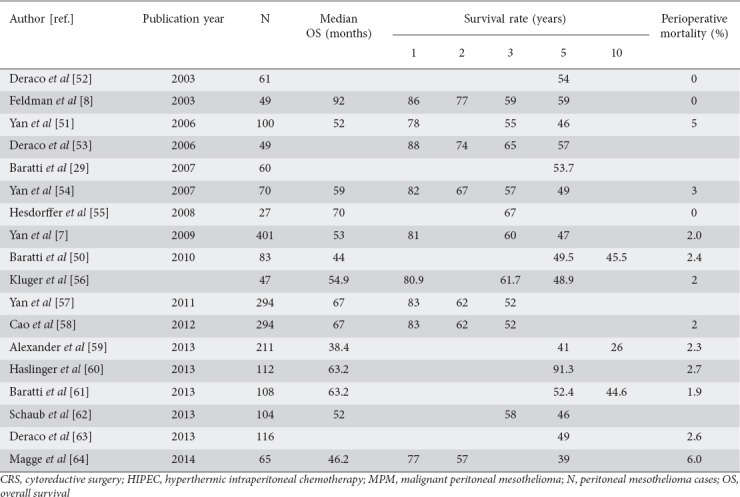
CRS with HIPEC has been recommended as the standard of care for patients with operable disease, and has been evaluated in a series of studies [7,8,29,50-64]. Details are reported in Table 2. CRS is the basis for the implementation of this therapeutic modality, whereas HIPEC offers enhanced therapeutic activity via distribution of high-dose intraperitoneal chemotherapy to all peritoneal surfaces in parallel with hyperthermia [24].
Table 2.
Summary of CRS plus HIPEC studies in the treatment of MPM during the last 15 years (2003-2018)
The aim of CRS prior to intraperitoneal chemotherapy is the achievement of complete resection of the macroscopic tumor and lysis of preexistent intra-abdominal adhesions, with the prospect of optimal exposure to intraperitoneal drugs. In this sequence of procedures, postponement of bowel reconstruction following resections until after the chemotherapy perfusion is considered, to reduce the risk of tumor cell seeding at anastomotic sites. Intraperitoneal therapy seems to be beneficial only in those residual tumor nodules smaller than 3 mm. There are six different peritonectomy procedures that can be performed either separately or combined: greater omentectomy-splenectomy, left upper quadrant peritonectomy, right upper quadrant peritonectomy, lesser omentectomy-cholecystectomy with stripping of the omental bursa, pelvic peritonectomy with sleeve resection of the sigmoid colon, and antrectomy [65].
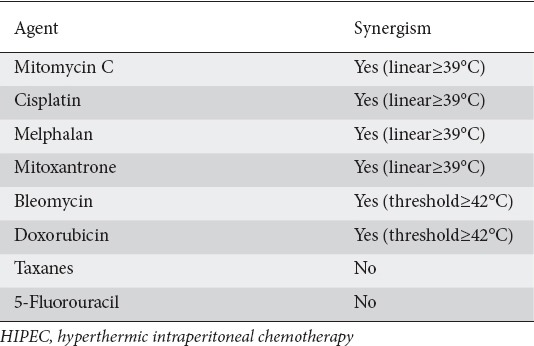
Hyperthermia has a direct cytotoxic effect caused by impaired DNA repair, denaturation of proteins, induction of heat-shock proteins, and apoptosis as well as inhibition of angiogenesis. In addition, hyperthermia acts synergistically with certain cytotoxic drugs, such as cisplatin, ifosfamide, melphalan, and mitomycin C, whereas it may also diminish the systemic toxicity of some drugs (e.g., doxorubicin and cyclophosphamide) by increasing their alkylation and/or excretion. Although enhancement of penetration depth should theoretically apply for all drugs, this has only been proven for cisplatin (Table 3) [65].
Table 3.
Interaction between hyperthermia and cytotoxic drugs used during HIPEC
Peritoneal expansion is applied in most centers to optimize exposure of the intra-abdominal organs and the parietal peritoneum to the perfusate. This can be achieved by several available methods. In the coliseum technique, the skin of the abdomen is attached to a retractor ring, above the laparotomy wound. The abdominal cavity is covered with a plastic sheet with a small opening in the centre allowing entrance for the surgeon's hand to stir the abdominal contents. A “peritoneal access device” to achieve optimal peritoneal expansion has also been described. Peritoneal expansion based on this technique permits large volumes of perfusion fluid to be added, enabling the small bowel to float in the cavity expander. Finally, there is a perfusion system in which the abdomen is closed during perfusion by a running suture of the skin. Thus, the whole peritoneal surface is exposed and drug spillage and heat loss are prevented [65].
Preoperative evaluation should determine whether optimal or complete CRS is feasible. Contraindications for CRS and HIPEC include severe cardiac, pulmonary, hepatic or renal dysfunction, and poor performance status [66]. In addition, high-volume peritoneal disease, extensive involvement of small bowel or mesentery, large tumor masses in the lesser omentum, disease burden outside the peritoneal cavity, and para-aortic lymph node metastases are contraindications, as they reduce the probability of optimal or complete CRS and are associated with poor outcomes [67].
The need to improve patient selection has led to various prognostic scoring systems that evaluate candidates preoperatively for CRS and HIPEC. The preoperative parameters used in those scoring systems include histopathology, symptoms, and tumor burden. Overall, the risks of perioperative morbidity and mortality, analogous to those of major gastrointestinal surgeries, should be weighed against the anticipated survival benefit, which depends on the extent of the disease and the feasibility of achieving complete CRS [67].
Immediately following a CRS and prior to intestinal reconstruction and abdominal closure, the abdomen and pelvis must be prepared for HIPEC, achieving complete hemostasis. Mechanical cleansing of the peritoneal space by irrigation should be performed, followed by HIPEC in patients who undergo complete or near-complete cytoreduction. No randomized clinical trials has been conducted for the comparison of the several available HIPEC chemotherapy regimens. Retrospective reports have described high-dose cisplatin (250 mg/m2) monotherapy [8,59,62,68-70] or dual therapy, such as cisplatin combined with either doxorubicin [7,51,53,54,57,58,61,63,71-75] or mitomycin [50,52,55,56,76-78].
In a multi-institutional retrospective analysis of 405 patients with MPM treated with CRS-HIPEC [7], HIPEC, mainly in combination with cisplatin and doxorubicin, was administered to 92% of participants. An additional 23% subsequently received systemic chemotherapy, mainly with paclitaxel, in an adjuvant setting during the early postoperative period (days 1-5). Median OS was 53 months and 5-year survival was achieved by 47%. Likewise, a recent meta-analysis of 20 studies, which included 1047 patients with MPM treated with CRS-HIPEC, reported a 5-year survival of 42% in the 67% of patient who underwent complete or near-complete cytoreduction prior to HIPEC [79]. Myelosuppression is a common complication associated with HIPEC, while laparotomy and CRS may cause wound infections, prolonged ileus, bowel obstruction, urinary tract infections, sepsis, and fistula formation. Despite these known side effects of CRS-HIPEC, the benefit is significant, with median OS and 5-year survival rates of 29.5-100 months and 17-91.3%, respectively (Table 2). This broad range is obviously explained by the widely heterogeneous nature of differing study populations, tumor biology and experience of the surgical team. CRS and HIPEC were also effective in the management of variable origins of peritoneal carcinomas and malignant ascites [60,80-83], as well as in disease recurrence[84].
Early postoperative intraperitoneal chemotherapy with paclitaxel, combined with systemic chemotherapy, has been reported to be beneficial. The recommended intraperitoneal/systemic chemotherapy regimens are similar to those implemented in ovarian cancer [85].
Systemic chemotherapy
CRS-HIPEC is considered as the standard first-line treatment for MPM, whereas systemic chemotherapy is the alternative approach for inoperable/unsuitable patients or for those patients who seek non-surgical management. Perioperative systemic chemotherapy has also been recommended in those with high-risk histology or extensive disease.
Limited clinical trials have been performed for the evaluation of systemic chemotherapy in patients with MPM[66]. Despite the fact that pleural and peritoneal mesothelioma are distinct, especially in terms of biology, the effectiveness of chemotherapeutic agents is similar for both entities. Neither single-agent systemic chemotherapy nor combinations are effective, and they correlate with a poor response rate of less than 15-20% [3]. The pemetrexed/cisplatin combination is approved for the treatment of MPM, based on the definitive phase III trial by Vogelzang et al [86].
The efficacy of pemetrexed for MPM, either alone or in combination with cisplatin, was reported in two studies[87,88]. The estimated median OS times were 8.7 and 13.1 months for pemetrexed monotherapy and the doublet systemic chemotherapy with cisplatin, respectively. There were no significant differences in the responses between chemotherapy-naïve patients and those previously treated with another agent. Pemetrexed was well tolerated, with low rates of reported grade 3 or 4 side effects, most often hematologic (2%) or non-hematologic toxicities such as dehydration (7%), nausea (5%), and vomiting (5%) [87]. A phase II trial revealed that the treatment with pemetrexed plus gemcitabine provides a significantly improved median OS of 26.8 months. However, the response rate of 15% still remains low [89]. Taking into consideration the increased incidence of severe toxicity and the inferior disease control rate with this combination, the option of pemetrexed with cisplatin/carboplatin is still considered as the standard first-line systemic treatment. The remaining drug combinations are reserved as a second-line option. Nevertheless, no therapies have shown a survival benefit as second-line treatments for relapsed or refractory disease. Failure to obtain disease control should prompt a switch to cisplatin combined with either irinotecan, or gemcitabine. Additional alternatives for second-line systemic treatment include the single agent vinorelbine, as well as the molecular agent tremelimumab, a monoclonal antibody that targets the cytotoxic T-lymphocyte antigen 4 (CTLA4). All these second-line therapies are still under investigation and enrollment in clinical trials should always be considered.
The use of perioperative systemic chemotherapy has also been investigated in MPM patients who underwent CRS-HIPEC, while neoadjuvant chemotherapy was independently associated with a worse outcome [90]. The 5-year OS achieved with this approach was 40%, compared to 56%, 67% and 62% in patients who had no systemic chemotherapy, or were treated in an adjuvant setting or perioperatively, respectively.
Molecular therapy
Deregulated expression of growth factors or proteins that function in downstream signaling pathways is crucial in the malignant transformation of mesothelial cells. A variety of molecular targets have been identified in MPM and relevant targeted agents have been investigated (Fig. 1). However, there is no consensus in the literature concerning the presence of epidermal growth factor receptor (EGFR) mutations in MPM. These mutations were identified in 31% of patients diagnosed with MPM [91], a similar rate to that reported for non-small cell lung cancer [92]. The presence of EGFR mutations is predictive of optimal cytoreduction—the only surrogate factor that predicts long-term survival [8]—treatment response and improved outcome as compared to the wild-type MPM [91]. On the other hand, in another study direct sequencing of the entire EGFR tyrosine kinase domain revealed that patients with MPM do not harbor somatic mutations in that domain that would make them sensitive to an EGFR tyrosine kinase inhibitor [93]. It is difficult to interpret the contradictory findings of these studies.
Overexpression of the closely interacting phosphoinositide 3-kinase (PI3K) and mammalian target of rapamycin (mTOR) pathways has emerged as an important molecular alteration that promotes a malignant phenotype of MPM [5]. Loss of phosphatase and tensin homolog (PTEN) function has been detected in 30-60% of cases [94]. Therefore, pharmacological inhibition of the PI3K-PTEN-AKT-mTOR pathways could be therapeutically beneficial in mesothelioma and clinical trials in this setting are ongoing [95]. In a case series of patients treated with CRS and HIPEC, upregulation in genes related to the PI3K and mTOR signaling pathways was associated with shorter OS [5]. Mesothelin is a cell surface glycoprotein expressed in both mesothelial and peritoneal cells. Three agents targeting mesothelin have been evaluated: SS1P, a recombinant immunotoxin targeting mesothelin; MORAb-009, a chimeric IgG1 anti-mesothelin monoclonal antibody; and CRS-207, a live-attenuated Listeria monocytogenes vector encoding human mesothelin [96]. Some novel mesothelin-targeted agents, including the immunocytokine interleukin (IL)-12, appear to have equivalent antitumor activity to SS1P in a murine model of MPM [97]. Furthermore, studies revealed that MORAb-009 blocks the binding of mesothelin to CA-125 and thus could be a promising approach for the prevention of tumor metastasis[98]. Finally, the recombinant anti-mesothelin immunotoxin SS1(dsFv)PE38 demonstrated preclinical cytotoxic activity and is under clinical investigation [99].
An interesting molecular target is the glycoprotein MUC1. One study revealed that MUC1 was expressed in 90% of patients with MPM and may carry some negative prognostic value [100]. Bromelain, a complex of proteolytic enzymes, has been proposed to target MUC1. Preliminary research indicates that chemoresistant peritoneal mesothelioma cell lines demonstrate increased sensitivity to bromelain combination therapy [101].
The NF2/Hippo signaling pathway appears to be disrupted in the majority of mesotheliomas [102]. Indeed, experimental animal models suggest that this event, together with a deficiency in CDKN2A, is crucial for the development of mesothelioma. Therefore, targeting molecules involved in the NF2/Hippo pathway is considered essential for the treatment of MPM. In addition, NF2 alterations lead to activation of focal adhesion kinase (FAK) and merlin deficiency predicts sensitivity to FAK inhibitors [103].
The genomic profiling of MPM revealed recurrent mutations in the epigenetic regulatory genes BAP1, SETD2, and DDX3X [104]. In this regard, transcriptional deregulation is a key oncogenic mechanism in mesothelial tumorigenesis that can lead to novel therapeutic implications for the treatment of MPM. Preclinical data suggest that inhibitors of epigenetic modifiers, including histone deacetylases and the histone methyltransferase EZH2, may be therapeutically beneficial in mesothelioma [105]. Those mesotheliomas that harbor inactivating events affecting both BAP1 and other transcriptional regulators, including SETD2 and DDX3X, probably constitute a molecular subgroup with altered transcriptional programs that may respond therapeutically to these agents. Potentially targetable alterations have also been identified, such as MET, which can be targeted with the small molecule inhibitor cabozantinib, and WEE1 with AZD1775 for the subset of MPM harboring SETD2 inactivation [106]. Furthermore, in one study ALK rearrangements were identified in 3% of patients with MPM, mostly in younger women [107]. Interestingly, the ALK-rearranged cases lacked the typically genetic alterations present in MPM, i.e., BAP1, SETD2 or NF2. Therefore, oncogenic ALK fusion may represent a distinct pathogenetic mechanism for a subset of patients with MPM who may be treated with ALK targeting agents.
Immunotherapy
Data from animal studies and small-cohort clinical trials suggested that malignant mesothelioma could be responsive to immunotherapy [108]. A chronic inflammatory reaction represented by infiltrating lymphocytes and plasma cells is associated with improved prognosis [109]. Indeed, tumor necrosis factor-α, IL-6, interferon and granulocyte-macrophage colony-stimulating factor have been demonstrated to be effective in the treatment of mesothelioma [3]. In mice models, pulsed dendritic cells were shown to be powerful in controlling the growth of mesothelioma and may be implemented in the adjuvant setting to control local recurrence [110]. There is a genuine need for more phase II/III clinical trials to allow investigation in the field of these novel immunotherapies.
Cancer cells usually inhibit T-cell activation and evade immune surveillance. Activated T cells express CTLA-4. CTLA-4-blocking monoclonal antibodies represent the standard of care of certain cancers, including melanoma [111]. In a phase II trial, the anti-CTLA-4 antibody tremelimumab has been evaluated as second-line treatment in mesothelioma [112]. In this study, a disease control rate of 31% and a PFS of 6 months were achieved, prompting further assessment of this agent in this setting.
Expression of programmed death-ligand 1 (PDL-1) allows cancers to escape from the host immune system by interaction with programmed cell death-1 (PD1), and has been demonstrated in mesothelioma tumor tissue [113]. This could lead to the development of a PD1/PDL-1 targeting agent for this disease. However, the predictive value of immunohistochemical screening regarding the response to anti-PD-L1 treatment for epithelioid MPM remains to be investigated.
Prognostic factors
MPM is a biologically heterogeneous tumor. Because of its rarity and the variability of treatment approaches, prognostic factors have not been clearly identified. Well-established prognostic factors are vital for optimizing the treatment of patients with MPM and multi-institutional registries must play a fundamental role in addressing this need [28,37]. Several patient- and treatment-related factors can be used for risk stratification in MPM patients undergoing CRS and HIPEC treatment [59,64]. One of the most consistent factors useful for predicting survival in MPM is the histologic type. It has been suggested that the epithelioid subtype is a favorable prognostic factor, while sarcomatoid and biphasic subtypes are associated with a dismal prognosis [7,49,62,75]. Accordingly, one study revealed that CRS-HIPEC in the sarcomatoid and biphasic groups may not be beneficial, with a median OS of 10.5 as compared to 51.5 months for those with a more favorable histology [64]. Survival is strongly affected by the completeness of cytoreduction [59,75]. In addition, outcomes from numerous studies identified stage as a prognostic factor [57]. A novel nomogram has been used for predicting survival, partly based on the peritoneal carcinomatosis index ranges[62]. In addition, it has been suggested that cell proliferation biomarkers such as Ki-67 may play a prognostic role in patients with MPM; high Ki-67 in association with a high peritoneal cancer index resulted in a median OS of only 10 months [57].
Older age is a negative predictive factor, even though the age of sample populations has varied among different studies. In general, patients older than 65 years have a dismal prognosis compared with those younger than 65 [64]. A possible explanation is that advanced age may increase post-surgical morbidity and mortality per se. There are certain differences in terms of the disease prognosis between the sexes, with female sex being associated with better survival in univariate analysis [19,58,59]. Less asbestos exposure, favorable histologic features, and the expression of estrogen receptors (ER-β) probably contribute to the better prognosis of female patients compared to male [24,114].
A large, single-center experience revealed that preoperative thrombocytosis predicts shortened survival in patients with MPM who undergo CRS and HIPEC [115]. It seems that those with a high platelet count were more likely to undergo suboptimal debulking surgery. These data suggest that patients with baseline thrombocytosis are not good candidates for immediate CRS and HIPEC. Overall, thrombocytosis at diagnosis predicts an aggressive biological behavior of MPM, thus suggesting that platelets and other immunologic cytokines could represent potential targets for the development of new therapeutic agents.
Concluding remarks
MPM remains a rare disease with limited therapeutic options and a poor outcome. Immunohistochemical loss of nuclear BAP1 is highly specific in the distinction of MPM from benign mesothelial proliferations. In addition, PAX8 immunostaining is valuable for differentiating MPM from serous ovarian cancer. The management of MPM requires meticulous patient selection and appropriate use of CRS and HIPEC in experienced centers. Optimal or suboptimal cytoreduction increases the chances of long-term survival in these patients. Systemic chemotherapy with the combination of pemetrexed and cisplatin in a first-line setting is reasonable for unresectable tumors, but the response remains limited. It is hoped that the molecular characterization of MPM tumors with novel sequencing technologies will lead to the identification of novel molecular targets in this disease. To date, overexpression of the PI3K/mTOR/AKT pathway appears to be a driver of the malignant phenotype of this tumor and represents an important target for the development of novel therapeutic interventions. Standardization of the treatment of peritoneal mesothelioma is crucial and will only be achieved through international collaboration and prospective clinical trials.
Biography
Medway NHS Foundation Trust, Kent, UK; Sarah Cannon Research Institute, London, UK; University of Ioannina, Greece; General Hospital G. Hatzikosta, Ioannina, Greece
Footnotes
Conflict of Interest: None
References
- 1.Yang H, Testa JR, Carbone M. Mesothelioma epidemiology, carcinogenesis, and pathogenesis. Curr Treat Options Oncol. 2008;9:147–157. doi: 10.1007/s11864-008-0067-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fasola G, Puglisi F, Follador A, Aita M, Di Terlizzi S, Belvedere O. Dramatic tumour response to pemetrexed single-agent in an elderly patient with malignant peritoneal mesothelioma: a case report. BMC Cancer. 2006;6:289. doi: 10.1186/1471-2407-6-289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Robinson BW, Lake RA. Advances in malignant mesothelioma. N Engl J Med. 2005;353:1591–1603. doi: 10.1056/NEJMra050152. [DOI] [PubMed] [Google Scholar]
- 4.Liu S, Staats P, Lee M, Alexander HR, Burke AP. Diffuse mesothelioma of the peritoneum: correlation between histological and clinical parameters and survival in 73 patients. Pathology. 2014;46:604–609. doi: 10.1097/PAT.0000000000000181. [DOI] [PubMed] [Google Scholar]
- 5.Varghese S, Chen Z, Bartlett DL, et al. Activation of the phosphoinositide-3-kinase and mammalian target of rapamycin signaling pathways are associated with shortened survival in patients with malignant peritoneal mesothelioma. Cancer. 2011;117:361–371. doi: 10.1002/cncr.25555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Munkholm-Larsen S, Cao CQ, Yan TD. Malignant peritoneal mesothelioma. World J Gastrointest Surg. 2009;1:38–48. doi: 10.4240/wjgs.v1.i1.38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Yan TD, Deraco M, Baratti D, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: multi-institutional experience. J Clin Oncol. 2009;27:6237–6242. doi: 10.1200/JCO.2009.23.9640. [DOI] [PubMed] [Google Scholar]
- 8.Feldman AL, Libutti SK, Pingpank JF, et al. Analysis of factors associated with outcome in patients with malignant peritoneal mesothelioma undergoing surgical debulking and intraperitoneal chemotherapy. J Clin Oncol. 2003;21:4560–4567. doi: 10.1200/JCO.2003.04.150. [DOI] [PubMed] [Google Scholar]
- 9.Sugarbaker PH, Alderman R, Edwards G, et al. Prospective morbidity and mortality assessment of cytoreductive surgery plus perioperative intraperitoneal chemotherapy to treat peritoneal dissemination of appendiceal mucinous malignancy. Ann Surg Oncol. 2006;13:635–644. doi: 10.1245/ASO.2006.03.079. [DOI] [PubMed] [Google Scholar]
- 10.Kotova S, Wong RM, Cameron RB. New and emerging therapeutic options for malignant pleural mesothelioma: review of early clinical trials. Cancer Manag Res. 2015;7:51–63. doi: 10.2147/CMAR.S72814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Baratti D, Kusamura S, Deraco M. Diffuse malignant peritoneal mesothelioma: systematic review of clinical management and biological research. J Surg Oncol. 2011;103:822–831. doi: 10.1002/jso.21787. [DOI] [PubMed] [Google Scholar]
- 12.Manzini VP, Recchia L, Cafferata M, et al. Malignant peritoneal mesothelioma: a multicenter study on 81 cases. Ann Oncol. 2010;21:348–353. doi: 10.1093/annonc/mdp307. [DOI] [PubMed] [Google Scholar]
- 13.Delgermaa V, Takahashi K, Park EK, Le GV, Hara T, Sorahan T. Global mesothelioma deaths reported to the World Health Organization between 1994 and 2008. Bull World Health Organ. 2011;89:716–724. doi: 10.2471/BLT.11.086678. 724A-724C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Blackham AU, Levine EA. Cytoreductive surgery with hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma. European J Clin Med Oncol. 2012;4:25–32. [PMC free article] [PubMed] [Google Scholar]
- 15.Boffetta P. Epidemiology of peritoneal mesothelioma: a review. Ann Oncol. 2007;18:985–990. doi: 10.1093/annonc/mdl345. [DOI] [PubMed] [Google Scholar]
- 16.Kim J, Bhagwandin S, Labow DM. Malignant peritoneal mesothelioma: a review. Ann Transl Med. 2017;5:236. doi: 10.21037/atm.2017.03.96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Marinaccio A, Corfiati M, Binazzi A, et al. ReNaM Working Group. The epidemiology of malignant mesothelioma in women: gender differences and modalities of asbestos exposure. Occup Environ Med. 2018;75:254–262. doi: 10.1136/oemed-2016-104119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rodríguez D, Cheung MC, Housri N, Koniaris LG. Malignant abdominal mesothelioma: defining the role of surgery. J Surg Oncol. 2009;99:51–57. doi: 10.1002/jso.21167. [DOI] [PubMed] [Google Scholar]
- 19.Yan TD, Popa E, Brun EA, Cerruto CA, Sugarbaker PH. Sex difference in diffuse malignant peritoneal mesothelioma. Br J Surg. 2006;93:1536–1542. doi: 10.1002/bjs.5377. [DOI] [PubMed] [Google Scholar]
- 20.Carbone M, Ly BH, Dodson RF, et al. Malignant mesothelioma: facts, myths, and hypotheses. J Cell Physiol. 2012;227:44–58. doi: 10.1002/jcp.22724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cao SB, Jin S, Cao JY, Shen J, Zhang JW, Yu Y. Colonic invasion induced by malignant peritoneal mesothelioma. Int J Colorectal Dis. 2014;29:891–892. doi: 10.1007/s00384-014-1875-1. [DOI] [PubMed] [Google Scholar]
- 22.Salemis NS, Tsiambas E, Gourgiotis S, Mela A, Karameris A, Tsohataridis E. Peritoneal mesothelioma presenting as an acute surgical abdomen due to jejunal perforation. J Dig Dis. 2007;8:216–221. doi: 10.1111/j.1751-2980.2007.00309.x. [DOI] [PubMed] [Google Scholar]
- 23.Sugarbaker PH, Yan H, Grazi RV, Shmookler BM. Early localized peritoneal mesothelioma as an incidental finding at laparoscopy. Report of a case and implications regarding natural history of the disease. Cancer. 2000;89:1279–1284. doi: 10.1002/1097-0142(20000915)89:6<1279::aid-cncr12>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]
- 24.Acherman YI, Welch LS, Bromley CM, Sugarbaker PH. Clinical presentation of peritoneal mesothelioma. Tumori. 2003;89:269–273. doi: 10.1177/030089160308900307. [DOI] [PubMed] [Google Scholar]
- 25.Haliloglu M, Hoffer FA, Fletcher BD. Malignant peritoneal mesothelioma in two pediatric patients: MR imaging findings. Pediatr Radiol. 2000;30:251–255. doi: 10.1007/s002470050732. [DOI] [PubMed] [Google Scholar]
- 26.Low RN, Sebrechts CP, Barone RM, Muller W. Diffusion-weighted MRI of peritoneal tumors: comparison with conventional MRI and surgical and histopathologic findings—a feasibility study. AJR Am J Roentgenol. 2009;193:461–470. doi: 10.2214/AJR.08.1753. [DOI] [PubMed] [Google Scholar]
- 27.Cao Q, Lu M, Heath J, et al. 18F-FDG PET/CT in a recurrent diffuse malignant peritoneal mesothelioma. Clin Nucl Med. 2012;37:492–494. doi: 10.1097/RLU.0b013e3182478bb5. [DOI] [PubMed] [Google Scholar]
- 28.Iversen LH, Rasmussen PC, Laurberg S. Value of laparoscopy before cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal carcinomatosis. Br J Surg. 2013;100:285–292. doi: 10.1002/bjs.8908. [DOI] [PubMed] [Google Scholar]
- 29.Baratti D, Kusamura S, Martinetti A, et al. Circulating CA125 in patients with peritoneal mesothelioma treated with cytoreductive surgery and intraperitoneal hyperthermic perfusion. Ann Surg Oncol. 2007;14:500–508. doi: 10.1245/s10434-006-9192-8. [DOI] [PubMed] [Google Scholar]
- 30.Robinson BW, Creaney J, Lake R, et al. Mesothelin-family proteins and diagnosis of mesothelioma. Lancet. 2003;362:1612–1616. doi: 10.1016/S0140-6736(03)14794-0. [DOI] [PubMed] [Google Scholar]
- 31.Levy AD, Arnáiz J, Shaw JC, Sobin LH. From the archives of the AFIP: primary peritoneal tumors: imaging features with pathologic correlation. Radiographics. 2008;28:583–607. doi: 10.1148/rg.282075175. [DOI] [PubMed] [Google Scholar]
- 32.Ordóñez NG. The diagnostic utility of immunohistochemistry and electron microscopy in distinguishing between peritoneal mesotheliomas and serous carcinomas: a comparative study. Mod Pathol. 2006;19:34–48. doi: 10.1038/modpathol.3800471. [DOI] [PubMed] [Google Scholar]
- 33.Taube ET, Denkert C, Sehouli J, et al. Wilms tumor protein 1 (WT1)-- not only a diagnostic but also a prognostic marker in high-grade serous ovarian carcinoma. Gynecol Oncol. 2016;140:494–502. doi: 10.1016/j.ygyno.2015.12.018. [DOI] [PubMed] [Google Scholar]
- 34.Ali RH, Kalloger SE, Santos JL, Swenerton KD, Gilks CB. Stage II to IV low-grade serous carcinoma of the ovary is associated with a poor prognosis: a clinicopathologic study of 32 patients from a population-based tumor registry. Int J Gynecol Pathol. 2013;32:529–535. doi: 10.1097/PGP.0b013e31827630eb. [DOI] [PubMed] [Google Scholar]
- 35.Oe S, Hasegawa K, Nagase S, Kato R, Torii Y, Udagawa Y. Expression of podoplanin in epithelial ovarian carcinomas and its potential as a marker for clear cell adenocarcinoma. Int J Gynecol Pathol. 2010;29:405–410. doi: 10.1097/PGP.0b013e3181d3261e. [DOI] [PubMed] [Google Scholar]
- 36.Nofech-Mozes S, Khalifa MA, Ismiil N, et al. Immunophenotyping of serous carcinoma of the female genital tract. Mod Pathol. 2008;21:1147–1155. doi: 10.1038/modpathol.2008.108. [DOI] [PubMed] [Google Scholar]
- 37.Taşkın S, Gümüş Y, Kiremitçi S, Kahraman K, Sertçelik A, Ortaç F. Malignant peritoneal mesothelioma presented as peritoneal adenocarcinoma or primary ovarian cancer: case series and review of the clinical and immunohistochemical features. Int J Clin Exp Pathol. 2012;5:472–478. [PMC free article] [PubMed] [Google Scholar]
- 38.Husain AN, Colby T, Ordonez N, et al. International Mesothelioma Interest Group. Guidelines for pathologic diagnosis of malignant mesothelioma: 2012 update of the consensus statement from the International Mesothelioma Interest Group. Arch Pathol Lab Med. 2013;137:647–667. doi: 10.5858/arpa.2012-0214-OA. [DOI] [PubMed] [Google Scholar]
- 39.Takeda M, Kasai T, Enomoto Y, et al. Comparison of genomic abnormality in malignant mesothelioma by the site of origin. J Clin Pathol. 2014;67:1038–1043. doi: 10.1136/jclinpath-2014-202465. [DOI] [PubMed] [Google Scholar]
- 40.Bowen NJ, Logani S, Dickerson EB, et al. Emerging roles for PAX8 in ovarian cancer and endosalpingeal development. Gynecol Oncol. 2007;104:331–337. doi: 10.1016/j.ygyno.2006.08.052. [DOI] [PubMed] [Google Scholar]
- 41.Ordóñez NG. Value of PAX8, PAX2, claudin-4, and h-caldesmon immunostaining in distinguishing peritoneal epithelioid mesotheliomas from serous carcinomas. Mod Pathol. 2013;26:553–562. doi: 10.1038/modpathol.2012.200. [DOI] [PubMed] [Google Scholar]
- 42.Andrici J, Jung J, Sheen A, et al. Loss of BAP1 expression is very rare in peritoneal and gynecologic serous adenocarcinomas and can be useful in the differential diagnosis with abdominal mesothelioma. Hum Pathol. 2016;51:9–15. doi: 10.1016/j.humpath.2015.12.012. [DOI] [PubMed] [Google Scholar]
- 43.Singhi AD, Krasinskas AM, Choudry HA, et al. The prognostic significance of BAP1, NF2, and CDKN2A in malignant peritoneal mesothelioma. Mod Pathol. 2016;29:14–24. doi: 10.1038/modpathol.2015.121. [DOI] [PubMed] [Google Scholar]
- 44.Shinozaki-Ushiku A, Ushiku T, Morita S, Anraku M, Nakajima J, Fukayama M. Diagnostic utility of BAP1 and EZH2 expression in malignant mesothelioma. Histopathology. 2017;70:722–733. doi: 10.1111/his.13123. [DOI] [PubMed] [Google Scholar]
- 45.Chirac P, Maillet D, Leprêtre F, et al. Genomic copy number alterations in 33 malignant peritoneal mesothelioma analyzed by comparative genomic hybridization array. Hum Pathol. 2016;55:72–82. doi: 10.1016/j.humpath.2016.04.015. [DOI] [PubMed] [Google Scholar]
- 46.El Bezawy R, De Cesare M, Pennati M, et al. Antitumor activity of miR-34a in peritoneal mesothelioma relies on c-MET and AXL inhibition: persistent activation of ERK and AKT signaling as a possible cytoprotective mechanism. J Hematol Oncol. 2017;10:19. doi: 10.1186/s13045-016-0387-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Cimino-Reale G, Gandellini P, Santambrogio F, Recagni M, Zaffaroni N, Folini M. miR-380-5p-mediated repression of TEP1 and TSPYL5 interferes with telomerase activity and favours the emergence of an “ALT-like” phenotype in diffuse malignant peritoneal mesothelioma cells. J Hematol Oncol. 2017;10:140. doi: 10.1186/s13045-017-0510-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Tabrizian P, Jayakrishnan TT, Zacharias A, et al. Incorporation of diagnostic laparoscopy in the management algorithm for patients with peritoneal metastases: A multi-institutional analysis. J Surg Oncol. 2015;111:1035–1040. doi: 10.1002/jso.23924. [DOI] [PubMed] [Google Scholar]
- 49.Baratti D, Kusamura S, Cabras AD, Deraco M. Cytoreductive surgery with selective versus complete parietal peritonectomy followed by hyperthermic intraperitoneal chemotherapy in patients with diffuse malignant peritoneal mesothelioma: a controlled study. Ann Surg Oncol. 2012;19:1416–1424. doi: 10.1245/s10434-012-2237-2. [DOI] [PubMed] [Google Scholar]
- 50.Baratti D, Kusamura S, Cabras AD, Laterza B, Balestra MR, Deraco M. Lymph node metastases in diffuse malignant peritoneal mesothelioma. Ann Surg Oncol. 2010;17:45–53. doi: 10.1245/s10434-009-0756-2. [DOI] [PubMed] [Google Scholar]
- 51.Yan TD, Yoo D, Sugarbaker PH. Significance of lymph node metastasis in patients with diffuse malignant peritoneal mesothelioma. Eur J Surg Oncol. 2006;32:948–953. doi: 10.1016/j.ejso.2006.05.009. [DOI] [PubMed] [Google Scholar]
- 52.Deraco M, De Simone M, Rossi CR, et al. An Italian Multicentric Phase II study on peritonectomy and intra peritoneal hyperthermic perfusion (IPHP) to treat patients with peritoneal mesothelioma. J Exp Clin Cancer Res. 2003;22:41–45. [PubMed] [Google Scholar]
- 53.Deraco M, Nonaka D, Baratti D, et al. Prognostic analysis of clinicopathologic factors in 49 patients with diffuse malignant peritoneal mesothelioma treated with cytoreductive surgery and intraperitoneal hyperthermic perfusion. Ann Surg Oncol. 2006;13:229–237. doi: 10.1245/ASO.2006.03.045. [DOI] [PubMed] [Google Scholar]
- 54.Yan TD, Edwards G, Alderman R, Marquardt CE, Sugarbaker PH. Morbidity and mortality assessment of cytoreductive surgery and perioperative intraperitoneal chemotherapy for diffuse malignant peritoneal mesothelioma—a prospective study of 70 consecutive cases. Ann Surg Oncol. 2007;14:515–525. doi: 10.1245/s10434-006-9187-5. [DOI] [PubMed] [Google Scholar]
- 55.Hesdorffer ME, Chabot JA, Keohan ML, et al. Combined resection, intraperitoneal chemotherapy, and whole abdominal radiation for the treatment of malignant peritoneal mesothelioma. Am J Clin Oncol. 2008;31:49–54. doi: 10.1097/COC.0b013e3180684181. [DOI] [PubMed] [Google Scholar]
- 56.Kluger MD, Taub RN, Hesdorffer M, Jin Z, Chabot JA. Two-stage operative cytoreduction and intraperitoneal chemotherapy for diffuse malignant peritoneal mesothelioma: Operative morbidity and mortality in phase I and II trials. Eur J Surg Oncol. 2010;36:997–1003. doi: 10.1016/j.ejso.2010.07.001. [DOI] [PubMed] [Google Scholar]
- 57.Yan TD, Deraco M, Elias D, et al. Peritoneal Surface Oncology Group. A novel tumor-node-metastasis (TNM) staging system of diffuse malignant peritoneal mesothelioma using outcome analysis of a multi-institutional database*. Cancer. 2011;117:1855–1863. doi: 10.1002/cncr.25640. [DOI] [PubMed] [Google Scholar]
- 58.Cao C, Yan TD, Deraco M, et al. Peritoneal Surface Malignancy Group. Importance of gender in diffuse malignant peritoneal mesothelioma. Ann Oncol. 2012;23:1494–1498. doi: 10.1093/annonc/mdr477. [DOI] [PubMed] [Google Scholar]
- 59.Alexander HR, Jr, Bartlett DL, Pingpank JF, et al. Treatment factors associated with long-term survival after cytoreductive surgery and regional chemotherapy for patients with malignant peritoneal mesothelioma. Surgery. 2013;153:779–786. doi: 10.1016/j.surg.2013.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Haslinger M, Francescutti V, Attwood K, et al. A contemporary analysis of morbidity and outcomes in cytoreduction/hyperthermic intraperitoneal chemoperfusion. Cancer Med. 2013;2:334–342. doi: 10.1002/cam4.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Baratti D, Kusamura S, Cabras AD, Bertulli R, Hutanu I, Deraco M. Diffuse malignant peritoneal mesothelioma: long-term survival with complete cytoreductive surgery followed by hyperthermic intraperitoneal chemotherapy (HIPEC) Eur J Cancer. 2013;49:3140–3148. doi: 10.1016/j.ejca.2013.05.027. [DOI] [PubMed] [Google Scholar]
- 62.Schaub NP, Alimchandani M, Quezado M, et al. A novel nomogram for peritoneal mesothelioma predicts survival. Ann Surg Oncol. 2013;20:555–561. doi: 10.1245/s10434-012-2651-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Deraco M, Baratti D, Hutanu I, Bertuli R, Kusamura S. The role of perioperative systemic chemotherapy in diffuse malignant peritoneal mesothelioma patients treated with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol. 2013;20:1093–1100. doi: 10.1245/s10434-012-2845-x. [DOI] [PubMed] [Google Scholar]
- 64.Magge D, Zenati MS, Austin F, et al. Malignant peritoneal mesothelioma: prognostic factors and oncologic outcome analysis. Ann Surg Oncol. 2014;21:1159–1165. doi: 10.1245/s10434-013-3358-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Witkamp AJ, de Bree E, Van Goethem R, Zoetmulder FA. Rationale and techniques of intra-operative hyperthermic intraperitoneal chemotherapy. Cancer Treat Rev. 2001;27:365–374. doi: 10.1053/ctrv.2001.0232. [DOI] [PubMed] [Google Scholar]
- 66.Turner K, Varghese S, Alexander HR., Jr Current concepts in the evaluation and treatment of patients with diffuse malignant peritoneal mesothelioma. J Natl Compr Canc Netw. 2012;10:49–57. doi: 10.6004/jnccn.2012.0008. [DOI] [PubMed] [Google Scholar]
- 67.Spiliotis J, Halkia E, de Bree E. Treatment of peritoneal surface malignancies with hyperthermic intraperitoneal chemotherapy-current perspectives. Curr Oncol. 2016;23:e266–e275. doi: 10.3747/co.23.2831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Park BJ, Alexander HR, Libutti SK, et al. Treatment of primary peritoneal mesothelioma by continuous hyperthermic peritoneal perfusion (CHPP) Ann Surg Oncol. 1999;6:582–590. doi: 10.1007/s10434-999-0582-6. [DOI] [PubMed] [Google Scholar]
- 69.Blackham AU, Shen P, Stewart JH, Russell GB, Levine EA. Cytoreductive surgery with intraperitoneal hyperthermic chemotherapy for malignant peritoneal mesothelioma: mitomycin versus cisplatin. Ann Surg Oncol. 2010;17:2720–2727. doi: 10.1245/s10434-010-1080-6. [DOI] [PubMed] [Google Scholar]
- 70.Wong J, Koch AL, Deneve JL, Fulp W, Tanvetyanon T, Dessureault S. Repeat cytoreductive surgery and heated intraperitoneal chemotherapy may offer survival benefit for intraperitoneal mesothelioma: a single institution experience. Ann Surg Oncol. 2014;21:1480–1486. doi: 10.1245/s10434-013-3341-7. [DOI] [PubMed] [Google Scholar]
- 71.Costamagna D, Scuderi S, Vaira M, Barone R, De Simone M. Treatment of peritoneal mesothelioma using cytoreduction and intraperitoneal hyperthermic chemotherapy. Tumori. 2003;89:40–42. [PubMed] [Google Scholar]
- 72.Baratti D, Kusamura S, Nonaka D, Oliva GD, Laterza B, Deraco M. Multicystic and well-differentiated papillary peritoneal mesothelioma treated by surgical cytoreduction and hyperthermic intra-peritoneal chemotherapy (HIPEC) Ann Surg Oncol. 2007;14:2790–2797. doi: 10.1245/s10434-007-9475-8. [DOI] [PubMed] [Google Scholar]
- 73.Yan TD, Brun EA, Cerruto CA, Haveric N, Chang D, Sugarbaker PH. Prognostic indicators for patients undergoing cytoreductive surgery and perioperative intraperitoneal chemotherapy for diffuse malignant peritoneal mesothelioma. Ann Surg Oncol. 2007;14:41–49. doi: 10.1245/s10434-006-9169-7. [DOI] [PubMed] [Google Scholar]
- 74.Gómez Portilla A, Cendoya I, Muriel J, et al. Malignant peritoneal mesothelioma. Our experienced with triple combined therapy: cytoreduction, intraperitoneal perioperative chemotherapy and hyperthermia. Cir Esp. 2007;81:82–86. doi: 10.1016/s0009-739x(07)71268-x. [DOI] [PubMed] [Google Scholar]
- 75.Chua TC, Yan TD, Morris DL. Outcomes of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal mesothelioma: the Australian experience. J Surg Oncol. 2009;99:109–113. doi: 10.1002/jso.21177. [DOI] [PubMed] [Google Scholar]
- 76.Deraco M, Casali P, Inglese MG, et al. Peritoneal mesothelioma treated by induction chemotherapy, cytoreductive surgery, and intraperitoneal hyperthermic perfusion. J Surg Oncol. 2003;83:147–153. doi: 10.1002/jso.10255. [DOI] [PubMed] [Google Scholar]
- 77.Brigand C, Monneuse O, Mohamed F, et al. Peritoneal mesothelioma treated by cytoreductive surgery and intraperitoneal hyperthermic chemotherapy: results of a prospective study. Ann Surg Oncol. 2006;13:405–412. doi: 10.1245/ASO.2006.05.041. [DOI] [PubMed] [Google Scholar]
- 78.Passot G, Cotte E, Brigand C, et al. Peritoneal mesothelioma: treatment with cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy. J Chir (Paris) 2008;145:447–453. doi: 10.1016/s0021-7697(08)74654-4. [DOI] [PubMed] [Google Scholar]
- 79.Helm JH, Miura JT, Glenn JA, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: a systematic review and meta-analysis. Ann Surg Oncol. 2015;22:1686–1693. doi: 10.1245/s10434-014-3978-x. [DOI] [PubMed] [Google Scholar]
- 80.Levine EA, Stewart JH, 4th, Shen P, Russell GB, Loggie BL, Votanopoulos KI. Intraperitoneal chemotherapy for peritoneal surface malignancy: experience with 1,000 patients. J Am Coll Surg. 2014;218:573–585. doi: 10.1016/j.jamcollsurg.2013.12.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Randle RW, Swett KR, Swords DS, et al. Efficacy of cytoreductive surgery with hyperthermic intraperitoneal chemotherapy in the management of malignant ascites. Ann Surg Oncol. 2014;21:1474–1479. doi: 10.1245/s10434-013-3224-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Votanopoulos KI, Ihemelandu C, Shen P, Stewart JH, Russell GB, Levine EA. Outcomes of repeat cytoreductive surgery with hyperthermic intraperitoneal chemotherapy for the treatment of peritoneal surface malignancy. J Am Coll Surg. 2012;215:412–417. doi: 10.1016/j.jamcollsurg.2012.04.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Chua TC, Quinn LE, Zhao J, Morris DL. Iterative cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for recurrent peritoneal metastases. J Surg Oncol. 2013;108:81–88. doi: 10.1002/jso.23356. [DOI] [PubMed] [Google Scholar]
- 84.Ihemelandu C, Bijelic L, Sugarbaker PH. Iterative cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for recurrent or progressive diffuse malignant peritoneal mesothelioma: clinicopathologic characteristics and survival outcome. Ann Surg Oncol. 2015;22:1680–1685. doi: 10.1245/s10434-014-3977-y. [DOI] [PubMed] [Google Scholar]
- 85.Landrum LM, Java J, Mathews CA, et al. Prognostic factors for stage III epithelial ovarian cancer treated with intraperitoneal chemotherapy: a Gynecologic Oncology Group study. Gynecol Oncol. 2013;130:12–18. doi: 10.1016/j.ygyno.2013.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Vogelzang NJ, Rusthoven JJ, Symanowski J, et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol. 2003;21:2636–2644. doi: 10.1200/JCO.2003.11.136. [DOI] [PubMed] [Google Scholar]
- 87.Carteni G, Manegold C, Garcia GM, et al. Malignant peritoneal mesothelioma-Results from the International Expanded Access Program using pemetrexed alone or in combination with a platinum agent. Lung Cancer. 2009;64:211–218. doi: 10.1016/j.lungcan.2008.08.013. [DOI] [PubMed] [Google Scholar]
- 88.Jänne PA, Wozniak AJ, Belani CP, et al. Open-label study of pemetrexed alone or in combination with cisplatin for the treatment of patients with peritoneal mesothelioma: outcomes of an expanded access program. Clin Lung Cancer. 2005;7:40–46. doi: 10.3816/CLC.2005.n.020. [DOI] [PubMed] [Google Scholar]
- 89.Simon GR, Verschraegen CF, Jänne PA, et al. Pemetrexed plus gemcitabine as first-line chemotherapy for patients with peritoneal mesothelioma: final report of a phase II trial. J Clin Oncol. 2008;26:3567–3572. doi: 10.1200/JCO.2007.15.2868. [DOI] [PubMed] [Google Scholar]
- 90.Kepenekian V, Elias D, Passot G, et al. French Network for Rare Peritoneal Malignancies (RENAPE) Diffuse malignant peritoneal mesothelioma: Evaluation of systemic chemotherapy with comprehensive treatment through the RENAPE Database: Multi-Institutional Retrospective Study. Eur J Cancer. 2016;65:69–79. doi: 10.1016/j.ejca.2016.06.002. [DOI] [PubMed] [Google Scholar]
- 91.Foster JM, Radhakrishna U, Govindarajan V, et al. Clinical implications of novel activating EGFR mutations in malignant peritoneal mesothelioma. World J Surg Oncol. 2010;8:88. doi: 10.1186/1477-7819-8-88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Foster JM, Gatalica Z, Lilleberg S, Haynatzki G, Loggie BW. Novel and existing mutations in the tyrosine kinase domain of the epidermal growth factor receptor are predictors of optimal resectability in malignant peritoneal mesothelioma. Ann Surg Oncol. 2009;16:152–158. doi: 10.1245/s10434-008-0206-6. [DOI] [PubMed] [Google Scholar]
- 93.Kalra N, Ashai A, Xi L, et al. Patients with peritoneal mesothelioma lack epidermal growth factor receptor tyrosine kinase mutations that would make them sensitive to tyrosine kinase inhibitors. Oncol Rep. 2012;27:1794–1800. doi: 10.3892/or.2012.1725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Agarwal V, Campbell A, Beaumont KL, Cawkwell L, Lind MJ. PTEN protein expression in malignant pleural mesothelioma. Tumour Biol. 2013;34:847–851. doi: 10.1007/s13277-012-0615-9. [DOI] [PubMed] [Google Scholar]
- 95.Dolly SO, Migali C, Tunariu N, et al. Indolent peritoneal mesothelioma: PI3K-mTOR inhibitors as a novel therapeutic strategy. ESMO Open. 2017;2:e000101. doi: 10.1136/esmoopen-2016-000101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Hassan R, Ho M. Mesothelin targeted cancer immunotherapy. Eur J Cancer. 2008;44:46–53. doi: 10.1016/j.ejca.2007.08.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Kim H, Gao W, Ho M. Novel immunocytokine IL12-SS1 (Fv) inhibits mesothelioma tumor growth in nude mice. PLoS One. 2013;8:e81919. doi: 10.1371/journal.pone.0081919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Ma J, Tang WK, Esser L, Pastan I, Xia D. Recognition of mesothelin by the therapeutic antibody MORAb-009: structural and mechanistic insights. J Biol Chem. 2012;287:33123–33131. doi: 10.1074/jbc.M112.381756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Li Q, Verschraegen CF, Mendoza J, Hassan R. Cytotoxic activity of the recombinant anti-mesothelin immunotoxin, SS1(dsFv)PE38, towards tumor cell lines established from ascites of patients with peritoneal mesotheliomas. Anticancer Res. 2004;24:1327–1335. [PubMed] [Google Scholar]
- 100.Pillai K, Pourgholami MH, Chua TC, Morris DL. MUC1 has prognostic significance in malignant peritoneal mesothelioma. Int J Biol Markers. 2013;28:303–312. doi: 10.5301/jbm.5000038. [DOI] [PubMed] [Google Scholar]
- 101.Pillai K, Akhter J, Chua TC, Morris DL. Anticancer property of bromelain with therapeutic potential in malignant peritoneal mesothelioma. Cancer Invest. 2013;31:241–250. doi: 10.3109/07357907.2013.784777. [DOI] [PubMed] [Google Scholar]
- 102.Murakami H, Mizuno T, Taniguchi T, et al. LATS2 is a tumor suppressor gene of malignant mesothelioma. Cancer Res. 2011;71:873–883. doi: 10.1158/0008-5472.CAN-10-2164. [DOI] [PubMed] [Google Scholar]
- 103.Shapiro IM, Kolev VN, Vidal CM, et al. Merlin deficiency predicts FAK inhibitor sensitivity: a synthetic lethal relationship. Sci Transl Med. 2014;6:237ra68. doi: 10.1126/scitranslmed.3008639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Joseph NM, Chen YY, Nasr A, et al. Genomic profiling of malignant peritoneal mesothelioma reveals recurrent alterations in epigenetic regulatory genes BAP1, SETD2, and DDX3X. Mod Pathol. 2017;30:246–254. doi: 10.1038/modpathol.2016.188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.LaFave LM, Béguelin W, Koche R, et al. Loss of BAP1 function leads to EZH2-dependent transformation. Nat Med. 2015;21:1344–1349. doi: 10.1038/nm.3947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Pfister SX, Markkanen E, Jiang Y, et al. Inhibiting WEE1 selectively kills histone H3K36me3-deficient cancers by dNTP starvation. Cancer Cell. 2015;28:557–568. doi: 10.1016/j.ccell.2015.09.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Hung YP, Dong F, Watkins JC, et al. Identification of ALK rearrangements in malignant peritoneal mesothelioma. JAMA Oncol. 2018;4:235–238. doi: 10.1001/jamaoncol.2017.2918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Cao S, Jin S, Cao J, et al. Advances in malignant peritoneal mesothelioma. Int J Colorectal Dis. 2015;30:1–10. doi: 10.1007/s00384-014-2029-1. [DOI] [PubMed] [Google Scholar]
- 109.Suzuki K, Kadota K, Sima CS, et al. Chronic inflammation in tumor stroma is an independent predictor of prolonged survival in epithelioid malignant pleural mesothelioma patients. Cancer Immunol Immunother. 2011;60:1721–1728. doi: 10.1007/s00262-011-1073-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Hegmans JP, Hemmes A, Aerts JG, Hoogsteden HC, Lambrecht BN. Immunotherapy of murine malignant mesothelioma using tumor lysate-pulsed dendritic cells. Am J Respir Crit Care Med. 2005;171:1168–1177. doi: 10.1164/rccm.200501-057OC. [DOI] [PubMed] [Google Scholar]
- 111.Callahan MK, Wolchok JD. At the bedside: CTLA-4- and PD-1-blocking antibodies in cancer immunotherapy. J Leukoc Biol. 2013;94:41–53. doi: 10.1189/jlb.1212631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Calabrò L, Morra A, Fonsatti E, et al. Tremelimumab for patients with chemotherapy-resistant advanced malignant mesothelioma: an open-label, single-arm, phase 2 trial. Lancet Oncol. 2013;14:1104–1111. doi: 10.1016/S1470-2045(13)70381-4. [DOI] [PubMed] [Google Scholar]
- 113.Mansfield AS, Roden AC, Peikert T, et al. B7-H1 expression in malignant pleural mesothelioma is associated with sarcomatoid histology and poor prognosis. J Thorac Oncol. 2014;9:1036–1040. doi: 10.1097/JTO.0000000000000177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Pillai K, Pourgholami MH, Chua TC, Morris DL. Oestrogen receptors are prognostic factors in malignant peritoneal mesothelioma. J Cancer Res Clin Oncol. 2013;139:987–994. doi: 10.1007/s00432-013-1408-2. [DOI] [PubMed] [Google Scholar]
- 115.Li YC, Khashab T, Terhune J, et al. Preoperative thrombocytosis predicts shortened survival in patients with malignant peritoneal mesothelioma undergoing operative cytoreduction and hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol. 2017;24:2259–2265. doi: 10.1245/s10434-017-5834-2. [DOI] [PubMed] [Google Scholar]
- 116.Kato S, Tomson BN, Buys TP, Elkin SK, Carter JL, Kurzrock R. Genomic landscape of malignant mesotheliomas. Mol Cancer Ther. 2016;15:2498–2507. doi: 10.1158/1535-7163.MCT-16-0229. [DOI] [PubMed] [Google Scholar]
- 117.Tandon RT, Jimenez-Cortez Y, Taub R, Borczuk AC. Immunohistochemistry in peritoneal mesothelioma: a single-center experience of 244 cases. Arch Pathol Lab Med. 2018;142:236242. doi: 10.5858/arpa.2017-0092-OA. [DOI] [PubMed] [Google Scholar]