

Abstract
Objective:
To evaluate Australian and New Zealand chiropractic students' opinions regarding the identity, role setting, and future of chiropractic practice.
Methods:
An online, cross-sectional survey was administered to chiropractic students in all chiropractic programs in Australia and New Zealand. The survey explored student viewpoints about the identity, role/scope, setting, and future of chiropractic practice as it relates to chiropractic education and health promotion. Associations between the number of years in the program, highest degree preceding chiropractic education, institution, and opinion summary scores were evaluated by multivariate analysis of variance tests.
Results:
A total of 347 chiropractic students participated in the study. For identity, most students (51.3%) hold strongly to the traditional chiropractic theory but also agree (94.5%) it is important that chiropractors are educated in evidence-based practice. The main predictor of student viewpoints was a student's chiropractic institution (Pillai's trace =.638, F[16, 1368] = 16.237, p < .001). Chiropractic institution explained over 50% of the variance around student opinions about role/scope of practice and approximately 25% for identity and future practice.
Conclusions:
Chiropractic students in Australia and New Zealand seem to hold both traditional and mainstream viewpoints toward chiropractic practice. However, students from different chiropractic institutions have divergent opinions about the identity, role, setting, and future of chiropractic practice, which is most strongly predicted by the institution. Chiropractic education may be a potential determinant of chiropractic professional identity, raising concerns about heterogeneity between chiropractic schools.
Key Indexing Terms: Attitude, Chiropractic, Cross-Sectional Studies, Students, Surveys and Questionnaires
INTRODUCTION
Chiropractic has been described as a profession at a crossroads between mainstream and alternative medicine.1 There has been an increasing amount of evidence suggesting valuable metrics associated with chiropractic care,2,3 and chiropractic has been included in several evidence-based guidelines.4–8 As a primary care physician, chiropractors are involved in the diagnosis and management of spine and musculoskeletal conditions and are at the forefront in educating the community on the importance of health promotion and injury prevention.
A complicating factor inhibiting the chiropractic profession from fully progressing into a mainstream health profession may be the presence of differing ideological approaches to care and a perceived inability of the profession to act as a unified group.9,10 As health care has evolved toward shared decision-making and integrative care teams, it is important that the chiropractic profession has a clear understanding of its path toward establishing itself as a fully accepted, competent, and contributing member of the health care team. Gaining a more discernible understanding of the viewpoints within the chiropractic profession may provide a greater appreciation of the commonalities and mutual goals that exist between them.9 Importantly, a unified profession is essential to the personal and social well-being of both an individual and the community at large.
Chiropractic students are the future of the chiropractic profession and make up a considerable portion (about 33%) of the chiropractic field.11 Australian chiropractors study at university for a minimum of 5 years and are included in the Australian national registration scheme for health practitioners.12 The study of chiropractic students therefore provides insight into current opinions and may relate to future practitioner ideologies and practice patterns. Two recent studies have investigated North American–based chiropractic students' opinions relating to chiropractic's identity, role, and future.13,14 These studies suggest cognitive dissonance, particularly regarding traditional chiropractic theories and evidence-based practice. To the authors' knowledge, no such studies have involved chiropractic students enrolled in chiropractic programs in Australia and New Zealand. Hence, the aim of this study was to evaluate Australian and New Zealand chiropractic students' opinions regarding the identity, role, setting, and future of chiropractic practice.
METHODS
Ethical review for this study was approved on by the Human Research Ethics Committee (Medical Sciences) of Macquarie University, Australia.
Study Design and Setting
A Web-based cross-sectional survey of Australian and New Zealand chiropractic students was conducted between August and October 2016. The head of research at each institution with a chiropractic program in Australia and New Zealand were invited, via e-mail, to administer recruitment information for the study at their respective institution. All 5 eligible institutions participated in this study: Central Queensland University, Macquarie University, Murdoch University, New Zealand Chiropractic College, and RMIT University–Melbourne.
Participant recruitment involved the head of research or their designated faculty representative posting an electronic recruitment flyer on the institution's learning management system to notify potentially eligible chiropractic students of the study. In addition, each head of research or representative forwarded an initial e-mail invitation to potentially eligible participants at their respective institution, with 2 subsequent reminder e-mail invitations forwarded at 2 and 6 weeks. The total study period per institution was 8 weeks. The flyer and e-mail invitations contained a link to the Web-based survey. To incentivize participation, 2 $40 iTunes gift cards were promoted to be given away via lottery to randomly selected participants once the survey was closed.
Study data were collected and managed using REDCap software version 5.4.2 (Vanderbilt University, Nashville, TN) electronic data capture tools hosted at Macquarie University.15 REDCap (Research Electronic Data Capture) is a secure, Web-based application designed to support data capture for research studies.
Participants and Eligibility Criteria
Students who were then enrolled in a bachelor or master of chiropractic degree program at an eligible institution (Central Queensland University, Macquarie University, Murdoch University, New Zealand Chiropractic College, and RMIT University–Melbourne) at the time of this study were eligible for participation.
Survey Instrument
The survey was modified from the 23-item questionnaire used by Gliedt et al14 to study chiropractic student opinions in North America. The survey's original core statements (11 Likert response items and 4 nominal response items) about identity, role/scope, and setting were duplicated in the current survey, with additional items pertaining to future practice as it relates to public health education initiatives. Demographic items were modified to fit the regional context; for example, the local professional associations were contextualized to Australia and New Zealand. In total, the survey instrument consisted of 31 items. The first 8 items were structured to solicit demographic information, such as participants' age, sex, current enrollment status, education, and degrees achieved prior to enrollment as well as student chiropractic organization affiliations. The remaining 23 survey items explored participants' opinions concerning chiropractic's identity, role, scope, setting, and future practice.
Variables and Measurements
Chiropractic students' responses to statements about the identity, role and scope, setting, and future of chiropractic practice were summarized using construct scales that ranged from 0 = progressive/mainstream viewpoint to 100 = traditional/alternative viewpoint. Progressive/mainstream viewpoints were operationally defined as aligning with currently orthodox scientific views, whereas traditional/alternative viewpoints could be considered unorthodox to current evidence-based care and guidelines.9 Summary scores were based on a total of 16 statements that required a response on a 5-point Likert scale: 0 = strongly agree, 1 = agree, 2 = neutral, 3 = disagree, and 4 = strongly disagree. The construct score for identity was based on the average response to 4 statements: (1) it is important for chiropractors to be educated in evidence-based practice, (2) contemporary and evolving scientific evidence is more important than traditional chiropractic principles, (3) it is appropriate to allow for updating and enrichment of chiropractic theories based on current scientific advancements, and (4) it is important for chiropractors to hold strongly to the traditional chiropractic theory that adjusting the spine corrects “dis-ease.” Item 4 was reverse coded so that a positive opinion would be reflected by a higher summary score. The construct score for role/scope was based on the average response to 4 statements: (1) the chiropractic profession should expand its scope of practice to include prescribing medication, with appropriate advanced training; (2) the primary purpose of the chiropractic examination is to detect vertebral subluxations; (3) emphasis of chiropractic care is to eliminate vertebral subluxations; and (4) chiropractic care should consist of the chiropractic adjustment only. Items 2 to 4 were reverse coded so that a positive opinion would be reflected by a higher summary score. The construct score for setting was based on the average response to 3 statements: (1) the public health care setting (hospitals and local health districts) are appropriate settings for chiropractic health care, (2) inclusion of clinical chiropractic training internships in integrative medical settings is important to the progression of the chiropractic profession, and (3) chiropractic practitioners should maintain a primary care (direct access) status. The construct score for future practice was based on the average response to 4 statements about involvement in public health education initiatives: (1) chiropractic care should include screening for smoking; (2) chiropractic care should include healthy lifestyle advice and screening for poor nutrition, weight management, and body mass index range; (3) chiropractic care should include screening for hazardous alcohol consumption; and (4) chiropractic care should include healthy lifestyle advice and screening for physical inactivity. All summary scores were transformed to fall within a 0- to 100-point scale of opinion.
Statistical Methods
Data were collated, cleaned, and inspected, and descriptive statistics were generated for all variables. Only participants with completed questionnaires were included in the analyses. Participant characteristics were stratified by institution, highest entry degree, and year in chiropractic program. Descriptive analyses for each item were reported as frequency distributions, including those items utilizing a 5-point Likert scale. Summary score distributions were illustrated via box plots.
Statistically significant differences between factors (institution, highest entry degree, and year in program) and response summary scores (identity, role, setting, and future) were tested using multivariate analysis of variance (MANOVA). Prior to conducting the MANOVAs, a series of Pearson correlations were performed between the dependent scores to test the MANOVA assumption that the dependent variables would be correlated with each other in the moderate range.16 To satisfy the assumption of homoscedasticity, equality of covariance matrices was constructed and checked, estimating the covariances among the dependent variables split across the test groups. We reported Pillai's trace for the F test, which is robust to violations of MANOVA assumptions.17
As follow-up tests to the MANOVAs, a series of 1-way analysis of variance (ANOVA) tests were conducted to test for differences between institutions based on individual response summary scores: identity, role, setting, and future. A series of post hoc analyses were performed using Fisher's least significant difference (LSD) test to examine mean differences and effect size of differences across the 5 chiropractic institutions for student opinions on identity, role, setting, and future. All analyses were conducted using SPSS Statistics for Windows version 24.0 (IBM Corp, Armonk, NY). Graphical output of data was plotted using SigmaPlot version 12.3 (Systat Software, Inc, San Jose, CA).
RESULTS
Demographic Data
A total of 347 participants (53.3% female) completed the survey. The ages of participants were 18 to 25 years (63.4%), 26 to 35 years (24.2%), 36 to 45 years (8.4%), 46 to 55 years (3.2%), and >55 years (0.9%). The New Zealand Chiropractic College had the highest student response rate per institution (students completing the online survey) at 45.7%, followed by Central Queensland University at 34.0%, RMIT University–Melbourne at 13.8%, Macquarie University at 13.6%, and Murdoch University at 7.8%. From a total of 1853 enrolled chiropractic students across the 5 institutions, 18.7% completed the survey. Table 1 reports the number of chiropractic students who participated by institution, year of enrollment, and highest academic achievement prior to entering a chiropractic degree program. Approximately one-third (34.3%) of the participants were not a member of a professional association. The other two-thirds reported being members of local chiropractic associations: the Chiropractors' Association of Australia (CAA) (29.1%), the New Zealand Chiropractors' Association (NZCA) (15%), Chiropractic Australia (CA) (5.5%), CA and CAA (13.5%), CA and NZCA (0.3%), CAA and NZCA (1.4%), and CA, CAA, and NZCA (0.9%). Students feel adequately represented (70.4%) when they hold a professional association membership compared to students who are not a member of a professional association (82.2%). Chiropractic students that responded typically had completed a subject in evidence-based practice (85.3%) and were interested in higher-degree research (55.5%).
Table 1.
Description of Participants by Institution, Enrollment Status, and Highest Level of Education
|
Chiropractic Institution |
||||||
|
A,
n
= 53 (15.3%) |
B,
n
= 63 (18.2%) |
C,
n
= 31 (8.9%) |
D,
n
= 121 (34.9%) |
E,
n
= 79 (22.8%) |
Total,
n
= 347 |
|
| Current enrollment status in the chiropractic degree program | ||||||
| 1st-year bachelor of chiropractic science/health science (chiropractic) | 11 (20.8%) | 5 (7.9%) | 6 (19.4%) | 28 (23.1%) | 13 (16.5%) | 63 (18.2%) |
| 2nd-year bachelor of chiropractic science/Health Science (chiropractic) | 20 (37.7%) | 10 (15.9%) | 5 (16.1%) | 28 (23.1%) | 16 (20.3%) | 79 (22.8%) |
| 3rd-year bachelor of chiropractic science/health science (chiropractic) | 14 (26.4%) | 13 (20.6%) | 5 (16.1%) | 29 (24%) | 21 (26.6%) | 82 (23.6%) |
| 1st-year master of chiropractic/4th-year bachelor of chiropractic science | 4 (7.5%) | 18 (28.6%) | 4 (12.9%) | 24 (19.8%) | 14 (17.7%) | 64 (18.4%) |
| 2nd-year master of chiropractic/5th-year bachelor of chiropractic science | 4 (7.5%) | 17 (27%) | 11 (35.5%) | 12 (9.9%) | 15 (19%) | 59 (17%) |
| Education level prior to enrolment in chiropractic program | ||||||
| High school certificate | 23 (43.4%) | 34 (54%) | 20 (64.5%) | 29 (24%) | 44 (55.7%) | 150 (43.2%) |
| Diploma | 13 (24.5%) | 5 (7.9%) | 3 (9.7%) | 59 (48.8%) | 18 (22.8%) | 98 (28.2%) |
| Bachelor's degree | 14 (26.4%) | 20 (31.7%) | 7 (22.6%) | 31 (25.6%) | 17 (21.5%) | 89 (25.6%) |
| Master's degree | 3 (5.7%) | 4 (6.3%) | 1 (3.2%) | 2 (1.7%) | 0 (0%) | 10 (2.9%) |
Description of Survey Responses
Table 2 reports the distributions of participant responses to statements about the identity, role/scope, setting, and future of chiropractic practice. For identity, 75.2% of participants responded that chiropractors should be considered allied health care practitioners and 24.8% complementary/alternative health care practitioners. Responses for the most appropriate practice paradigm for the chiropractic profession were nonsurgical spine and musculoskeletal care experts (44.7%), detection and correction of subluxation only (28.5%), nervous system experts (15.6%), spine care only (0.9%), and other (10.4%). Regarding setting, students believe that the most appropriate setting for chiropractic health care was in integrative settings with other health care disciplines, including allopathic medicine (81.3%), followed by alone or with other chiropractors without integration with any other health care disciplines (13.5%) and integrative settings with alternative medicine practitioners only (5.2%). All (100%) participants believe that chiropractic research is important and believe that the primary focus of future research should be physiological mechanisms of chiropractic adjustments (63.1%), followed by outcomes/cost-effectiveness of chiropractic care (25.1%) and outcomes/cost-effectiveness of integrative care models (11.8%). Figure 1 illustrates the distribution of participant response summary scores to statements about identity, role/scope, setting, and future.
Table 2.
Frequency of Responses to Statements About Chiropractic Identity, Role/Scope, Setting, and Future
|
Strongly Agree |
Agree |
Neutral |
Disagree |
Strongly Disagree |
|
| Identity | |||||
| It is important for chiropractors to hold strongly to the traditional chiropractic theory that adjusting the spine corrects “dis-ease” | 91 (26.2%) | 87 (25.1%) | 52 (15%) | 61 (17.6%) | 56 (16.1%) |
| It is important for chiropractors to be educated in evidence-based practice | 222 (64%) | 106 (30.5%) | 16 (4.6%) | — | 3 (0.9%) |
| Contemporary and evolving scientific evidence is more important than traditional chiropractic principles | 71 (20.5%) | 113 (32.6%) | 110 (31.7%) | 45 (13%) | 8 (2.3%) |
| It is appropriate to allow for updating and enrichment of chiropractic theories based on current scientific advancements | 186 (53.6%) | 128 (36.9%) | 27 (7.8%) | 3 (0.9%) | 3 (0.9%) |
| Role/scope | |||||
| The primary purpose of the chiropractic examination is to detect vertebral subluxations | 110 (31.7%) | 80 (23.1%) | 57 (16.4%) | 62 (17.9%) | 38 (11%) |
| Emphasis of chiropractic care is to eliminate vertebral subluxations | 95 (27.4%) | 107 (30.8%) | 58 (16.7%) | 46 (13.3%) | 41 (11.8%) |
| Chiropractic care should consist of the chiropractic adjustment only | 29 (8.4%) | 57 (16.4%) | 39 (11.2%) | 94 (27.1%) | 128 (36.9%) |
| The chiropractic profession should expand its scope of practice to include prescribing medication, with appropriate advanced training | 24 (6.9%) | 40 (11.5%) | 45 (13%) | 74 (21.3%) | 164 (47.3%) |
| The scope of practice within the chiropractic profession is strongly placed to provide care of infants and young children | 141 (40.6%) | 92 (26.5%) | 80 (23.1%) | 28 (8.1%) | 6 (1.7%) |
| Setting | |||||
| The public health care setting (hospitals and local health districts etc.) are appropriate settings for chiropractic health care | 121 (34.9%) | 115 (33.1%) | 60 (17.3%) | 41 (11.8%) | 10 (2.9%) |
| Inclusion of clinical chiropractic training internships in integrative medical settings is important to the progression of the chiropractic profession | 110 (31.7%) | 100 (28.8%) | 72 (20.7%) | 42 (12.1%) | 23 (6.6%) |
| Chiropractic practitioners should maintain a primary care (direct access) status | 235 (67.7%) | 92 (26.5%) | 18 (5.2%) | 1 (0.3%) | 1 (0.3%) |
| Future | |||||
| It is appropriate for the chiropractic profession to distinguish and promote 2 separate subgroups of broad scope (providing manual and other nondrug procedures) and limited scope (providing subluxation correction only) | 20 (5.8%) | 48 (13.8%) | 113 (32.6%) | 100 (28.8%) | 66 (19%) |
| Chiropractic care should include preventive (wellness) care to prevent recurrence and exacerbations of a chronic condition | 204 (58.8%) | 104 (30%) | 32 (9.2%) | 5 (1.4%) | 2 (0.6%) |
| Chiropractic care should include screening for smoking | 67 (19.3%) | 120 (34.6%) | 94 (27.1%) | 34 (9.8%) | 32 (9.2%) |
| Chiropractic care should healthy lifestyle advice and screening for poor nutrition, weight management, and body mass index range | 88 (25.4%) | 142 (40.9%) | 68 (19.6%) | 25 (7.2%) | 24 (6.9%) |
| Chiropractic care should include screening for hazardous alcohol consumption | 71 (20.5%) | 130 (37.5%) | 83 (23.9%) | 33 (9.5%) | 30 (8.6%) |
| Chiropractic care should healthy lifestyle advice and screening for physical inactivity | 88 (25.4%) | 165 (47.6%) | 56 (16.1%) | 20 (5.8%) | 18 (5.2%) |
Figure 1.
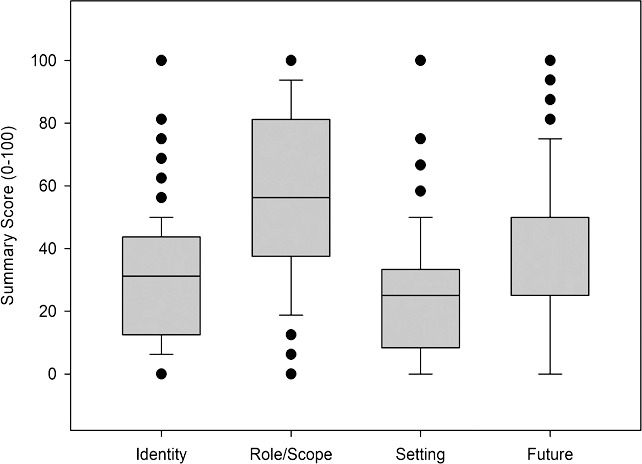
Distribution of participant summary scores for identity, role/scope, setting, and future.
Primary Analyses: Effect of Enrollment Status, Level of Education and Institution on Students' Opinions
There was a meaningful pattern of correlations observed among response summary scores to statements about identity, role/scope, setting, and future scores, suggesting the appropriateness of conducting 1-way MANOVA tests (Table 3) to test the hypotheses that there would be 1 or more significant differences between study factors: (1) enrollment status, (2) level of education at entry to chiropractic program, (3) chiropractic institution and outcomes: response summary scores (identity, role/scope, setting, and future). Student enrollment status was not significant as a predictor of student opinion summary scores (Pillai's trace = 0.057, F[16, 1368] = 1.234, p = .234). Level of education at entry into a chiropractic education program was a statistically significant predictor of summary scores (Pillai's trace = 0.124, F[12, 1026] = 3.682, p < .001). For the model, the effect size (partial eta-squared) was 0.041, suggesting that 4% of the variance in the summary scores was accounted for by level of education on entry to program. Chiropractic institution was statistically significant and the strongest predictor of summary scores (Pillai's trace = 0.638, F[16, 1368] = 16.237, p < .001). The multivariate effect size was estimated at 0.16, which implies that 16.0% of the variance around the summary scores was accounted for by chiropractic institution. Figure 2 illustrates the mean scores and 95% confidence intervals for the 3 general linear models.
Table 3.
Pearson Correlation Coefficients Suggest Positive Linear Relationships Between Identity, Role/Scope, Setting, and Future Scores
|
Identity |
Role/Scope |
Setting |
Future |
|
| Identity | 1 | |||
| Role/scope | r = 0.625*, n = 347, p < .001 | 1 | ||
| Setting | r = 0.322*, n = 347, p < .001 | r = 0.380*, n = 347, p < .001 | 1 | |
| Future | r = 0.330*, n = 347, p < .001 | r = 0.429*, n = 347, p < .001 | r = 0.366*, n = 347, p < .001 | 1 |
Correlation is significant at the .01 level (2-tailed).
Figure 2.

Mean and 95% confidence intervals for summary scores based on (1) enrollment status, (2) level of education at entry to chiropractic program, and (3) chiropractic institution.
Secondary and Post Hoc Analyses: Effect of Institution on Students' Opinions
All ANOVAs that tested the effects of chiropractic institution were statistically significant, with effects sizes ranging from 15% for setting to 56% for role/scope (Table 4). A series of post hoc analyses (Fisher's LSD) were performed to examine individual mean difference comparisons across all 5 chiropractic institutions and the 4 dependent summary scores. There was a trend across institutions for responses to all summary scores (Figure 2), with the most pronounced mean differences between institutions B and D. The largest mean differences were associated with the role/scope scores, accompanied by very large effect sizes18 as indicated by Cohen's d values greater than 1.2 (Table 5).
Table 4.
One-Way Analysis of Variance for Between-Subject Effects
|
Dependent Variable |
df |
Mean Square |
F |
Significance |
Partial Eta-Squared |
| Identity | 4 | 7943 | 36 | p < .001 | 0.294 |
| Role/scope | 4 | 37,009 | 108 | p < .001 | 0.557 |
| Setting | 4 | 4450 | 15 | p < .001 | 0.149 |
| Future | 4 | 13,976 | 26 | p < .001 | 0.235 |
Table 5.
Fisher's Least Significant Differences Test for Multiple Comparisons of Institutions
|
Dependent Variable |
Institution (I) |
Institution (J) |
Mean Difference (I − J) |
SDpooled |
SE |
Significance |
Cohen's
d |
| Identity | A | B | 9.79* | 16.946 | 2.786 | p = .001 | 0.578 |
| C | −0.02 | 19.061 | 3.38 | p = .996 | −0.001 | ||
| D | −16.42* | 16.734 | 2.462 | p < .001 | −0.982 | ||
| E | −6.44* | 19.824 | 2.654 | p = .016 | −0.325 | ||
| B | A | −9.79* | 16.225 | 2.786 | p = .001 | −0.603 | |
| C | −9.81* | 17.762 | 3.279 | p = .003 | −0.552 | ||
| D | −26.21* | 15.238 | 2.322 | p < .001 | −1.721 | ||
| E | −16.23* | 18.578 | 2.525 | p < .001 | −0.874 | ||
| C | A | 0.02 | 20.385 | 3.38 | p = .996 | 0.001 | |
| B | 9.81* | 19.789 | 3.279 | p = .003 | 0.496 | ||
| D | −16.41* | 19.608 | 3.009 | p < .001 | −0.837 | ||
| E | −6.42* | 22.303 | 3.168 | p = .043 | −0.288 | ||
| D | A | 16.42* | 15.779 | 2.462 | p < .001 | 1.041 | |
| B | 26.21* | 15.002 | 2.322 | p < .001 | 1.748 | ||
| C | 16.41* | 17.355 | 3.009 | p < .001 | 0.946 | ||
| E | 9.98* | 18.190 | 2.162 | p < .001 | 0.549 | ||
| E | A | 6.44* | 21.792 | 2.654 | p = .016 | 0.296 | |
| B | 16.23* | 21.236 | 2.525 | p < .001 | 0.765 | ||
| C | 6.42* | 22.959 | 3.168 | p = .043 | 0.280 | ||
| D | −9.98* | 21.067 | 2.162 | p < .001 | −0.474 | ||
| Role/scope | A | B | 14.02* | 21.372 | 3.456 | p < .001 | 0.656 |
| C | 2.04 | 24.468 | 4.192 | p = .628 | 0.083 | ||
| D | −39.36* | 20.326 | 3.054 | p < .001 | −1.936 | ||
| E | −7.96* | 24.347 | 3.292 | p = .016 | −0.327 | ||
| B | A | −14.02* | 20.981 | 3.456 | p < .001 | −0.668 | |
| C | −11.98* | 23.780 | 4.068 | p = .003 | −0.504 | ||
| D | −53.38* | 19.494 | 2.881 | p < .001 | −2.738 | ||
| E | −21.98* | 23.656 | 3.132 | p < .001 | −0.929 | ||
| C | A | −2.04 | 26.907 | 4.192 | p = .628 | −0.076 | |
| B | 11.98* | 26.597 | 4.068 | p = .003 | 0.450 | ||
| D | −41.40* | 25.764 | 3.732 | p < .001 | −1.607 | ||
| E | −9.99* | 29.042 | 3.93 | p = .011 | −0.344 | ||
| D | A | 39.36* | 18.787 | 3.054 | p < .001 | 2.095 | |
| B | 53.38* | 18.341 | 2.881 | p < .001 | 2.910 | ||
| C | 41.40* | 21.870 | 3.732 | p < .001 | 1.893 | ||
| E | 31.40* | 21.735 | 2.682 | p < .001 | 1.445 | ||
| E | A | 7.96* | 26.687 | 3.292 | p = .016 | 0.298 | |
| B | 21.98* | 26.375 | 3.132 | p < .001 | 0.833 | ||
| C | 9.99* | 28.940 | 3.93 | p = .011 | 0.345 | ||
| D | −31.40* | 25.534 | 2.682 | p < .001 | −1.230 | ||
| Setting | A | B | 4.1 | 17.738 | 3.209 | p = .203 | 0.231 |
| C | 2.5 | 20.856 | 3.893 | p = .522 | 0.120 | ||
| D | −13.43* | 19.405 | 2.836 | p < .001 | −0.692 | ||
| E | −0.92 | 19.242 | 3.057 | p = .764 | −0.048 | ||
| B | A | −4.1 | 17.647 | 3.209 | p = .203 | −0.232 | |
| C | −1.6 | 20.701 | 3.777 | p = .672 | −0.077 | ||
| D | −17.53* | 19.238 | 2.675 | p < .001 | −0.911 | ||
| E | −5.01 | 19.074 | 2.908 | p = .086 | −0.263 | ||
| C | A | −2.5 | 23.496 | 3.893 | p = .522 | −0.106 | |
| B | 1.6 | 23.427 | 3.777 | p = .672 | 0.068 | ||
| D | −15.93* | 24.713 | 3.465 | p < .001 | −0.645 | ||
| E | −3.41 | 24.586 | 3.649 | p = .35 | −0.139 | ||
| D | A | 13.43* | 20.862 | 2.836 | p < .001 | 0.644 | |
| B | 17.53* | 20.785 | 2.675 | p < .001 | 0.843 | ||
| C | 15.93* | 23.502 | 3.465 | p < .001 | 0.678 | ||
| E | 12.52* | 22.083 | 2.49 | p < .001 | 0.567 | ||
| E | A | 0.92 | 20.559 | 3.057 | p = .764 | 0.045 | |
| B | 5.01 | 20.481 | 2.908 | p = .086 | 0.245 | ||
| C | 3.41 | 23.233 | 3.649 | p = .35 | 0.147 | ||
| D | −12.52* | 21.940 | 2.49 | p < .001 | −0.570 | ||
| Future | A | B | 0.23 | 20.700 | 4.303 | p = .957 | 0.011 |
| C | −0.04 | 22.261 | 5.22 | p = .994 | −0.002 | ||
| D | −28.15* | 24.735 | 3.802 | p < .001 | −1.138 | ||
| E | −5.69 | 22.473 | 4.099 | p = .166 | −0.253 | ||
| B | A | −0.23 | 22.324 | 4.303 | p = .957 | −0.010 | |
| C | −0.27 | 25.205 | 5.064 | p = .957 | −0.011 | ||
| D | −28.38* | 27.414 | 3.586 | p < .001 | −1.035 | ||
| E | −5.92 | 25.392 | 3.899 | p = .13 | −0.233 | ||
| C | A | 0.04 | 25.149 | 5.22 | p = .994 | 0.002 | |
| B | 0.27 | 26.502 | 5.064 | p = .957 | 0.010 | ||
| D | −28.11* | 29.760 | 4.647 | p < .001 | −0.945 | ||
| E | −5.65 | 27.908 | 4.892 | p = .249 | −0.202 | ||
| D | A | 28.15* | 29.411 | 3.802 | p < .001 | 0.957 | |
| B | 28.38* | 30.575 | 3.586 | p < .001 | 0.928 | ||
| C | 28.11* | 31.653 | 4.647 | p < .001 | 0.888 | ||
| E | 22.46* | 31.803 | 3.339 | p < .001 | 0.707 | ||
| E | A | 5.69 | 25.524 | 4.099 | p = .166 | 0.223 | |
| B | 5.92 | 26.857 | 3.899 | p = .13 | 0.220 | ||
| C | 5.65 | 28.078 | 4.892 | p = .249 | 0.201 | ||
| D | −22.46* | 30.077 | 3.339 | p < .001 | −0.747 |
Mean difference is significant at the .05 level.
DISCUSSION
In our study, chiropractic students in Australia and New Zealand had progressive viewpoints about the identity, setting, and future practice of chiropractic but not the role/scope of chiropractic. Student opinions tended to be internally conflicting, where both alterative and mainstream viewpoints coexist. A chiropractic student's institution was the strongest predictor of their viewpoint about chiropractic identity, role/scope, setting, and future, albeit the level of internal contradiction in viewpoints varies between individuals from different chiropractic institutions. Between chiropractic institutions, there were divergent viewpoints among students that were most pronounced for opinions about the role/scope of chiropractic. Across several institutions, the effect size of the differences in student opinions was very large (based on Cohen's d), and the reasons for this are currently unclear.
Most Australian and New Zealand chiropractic students in this sample support the notion that subluxations cause and that adjustments prevent “dis-ease.” Furthermore, the primary purpose of the chiropractic examination and intervention was to identify and correct subluxations. Both viewpoints are aligned with traditional and unorthodox tenets of the chiropractic profession. The majority of chiropractic students also responded that learning concepts in evidence-based practice is important, and new and emerging science is preferred over traditional chiropractic theories. Moreover, chiropractic students responded that they wanted to be part of integrative, mainstream health care. Strong contradictory opinions such as these are also reported in large samples of chiropractic students from North America13,14 and may be explained by factors inherent to chiropractic students or their training. As noted by Gliedt et al,26 contrary viewpoints may be interpreted as cognitive dissonance, where internal inconsistencies in opinion are explained by a want or a need to justify historical theories of the chiropractic profession. A unique finding in the current study was that these internal inconsistencies were variable among students from different chiropractic institutions and that factors such as chiropractic institution and level of education before chiropractic study could explain much of the variance around a chiropractic student's opinion. While philosophical differences between chiropractic institutions have previously been noted,19 the current study provides the first data toward a link between institution and student opinion. Our study clearly highlights this association; however, further research is needed to investigate if this link infers a causal relationship.
Chiropractic education as a potential determinant of chiropractic professional identity is theoretically normalized via a process of accreditation that assesses graduate competencies and educational standards20 to produce graduates who focus on the diagnosis and treatment of spine and musculoskeletal disorders.21 The extent to which chiropractic institutions in Australia and New Zealand teach traditional chiropractic theories is currently unclear, but this may vary greatly according to institutional position and values.22,23 The transmission of norms, values, and beliefs conveyed in the classroom and the learning environments (eg, clinical internships) may explain the large differences in opinions found between students from different chiropractic institutions in the current study. Our findings raise new concerns over the legitimacy and effectiveness of the accreditation process, whereby education and competency standards24 may fail to definitively rule on the role of traditional knowledge in chiropractic curriculum. Our results also may suggest a lack capacity within the accreditation frameworks to quantify education content not covered by the accreditation standards, which may be addressed by accreditors formally evaluating student beliefs in addition to academic performance.
The most consistent viewpoints among chiropractic students were the settings most appropriate for chiropractic practice. Over three-quarters of respondents believed that an integrative setting is appropriate for chiropractic care, with two-thirds in favor of public health care settings such as hospitals and local health districts. Notwithstanding, Australian chiropractors currently service the community in private clinical practice settings, frequently alongside another chiropractors (57%) or massage therapists (30%).25 While over half of Australian chiropractors refer patients to general practitioners, seldom do they work in the same practice as other health providers. Results from the Australian Chiropractic Research Network reveal that chiropractors infrequently work alongside psychologists (12%), physiotherapists (9%), exercise physiologists (6%), and general practitioners (6%).25 Therefore, student opinions and, potentially, expectations as they relate to chiropractic setting do not currently align with the reality of clinical practice. Regarding future practice, most chiropractic students strongly agreed that care should include preventive (wellness) care for nonspecific chronic conditions. However, they were less strongly opinionated about the role of chiropractic care in screening for physical inactivity, poor nutrition, smoking, and hazardous alcohol consumption. This again suggests the possibility of disparate viewpoints with practice reality given that recent nationally representative data on chiropractic clinical management suggests that Australian chiropractors often discuss physical activity (85%), diet/nutrition (51%), and smoking/drugs/alcohol (25%) with patients.25 This may suggest that there is room for improvement within chiropractic educational programs to better engage students as conduits for public health education initiatives and potentially to manage expectations for future clinical practice.26 The fact that most students advocate future practice in integrative and public health settings may simply reflect the current accreditation requirements or best practice for clinical internships and case-mix loads.
In Australia and New Zealand, chiropractic is a registered health care profession that falls under the allied health banner,27 with an estimated 16% of the population using chiropractic care most frequently for musculoskeletal complaints.28 Respondents tended to identify chiropractors as allied health care practitioners (75%), most appropriately positioned as nonsurgical spine and musculoskeletal care experts (45%). This finding supports a recent commentary on the identity of chiropractors in which authors suggest that chiropractors internally accept the public view that they are in fact specialists for spine and musculoskeletal disorders.21 Nonetheless, several chiropractic students in the region did not hold identity views that align with either the national legislative frameworks or community demand, and opinions did not appear to change with increasing year level of study for students in the current sample. Added to this, 1 in 5 respondents oppose the view that chiropractic care should be integrated with other health care disciplines, including medicine. Musculoskeletal conditions (low back and neck pain) remain among the highest cause of disability burden in society globally.29 The majority of people who pursue or seek chiropractic care do so for musculoskeletal and spinal complaints, yet the presumption that chiropractors provide primarily a service that society wants and needs21,30 may be challenged if student opinions found in this study match those of graduate chiropractors. Incongruous expectations between student's/chiropractor's views and society's wants/needs may explain professional issues associated with limited cultural authority and integration into mainstream health in the region to date. Whether Australian and New Zealand student and graduate opinions correlate or student opinion remains congruent over time is currently unclear and an area for future research.
Study Strengths and Limitations
The current study provides unique insights into chiropractic student opinion from different institutions in Australia and New Zealand. We were expecting dissimilar student opinions to those of North American chiropractic students given that chiropractic training is exclusively university based in Australia. Our study is the first to provide data that suggest that chiropractic institution may indeed explain student opinion. On this, we adopted a stepwise analytical approach to minimize the possibility of incorrectly rejecting a true null hypothesis as it relates to between-school differences in opinion (inflating the type I error rate).31 We used a preexisting survey instrument14 to allow for comparability of findings with North America and future studies from other regions using the same tool. However, we acknowledge that the psychometric properties of these questions or the validity of summary scores are currently unclear. Despite the strengths, our study was limited by low response rate, with 1 in 5 students answering the online survey, which is comparable to the same North American study.14 Given this, we have interpreted these results with caution based on poor representativeness and generalizability. Inherent to cross-sectional study designs is the inability to determine the direction of associations or to imply causal inference. It may be that other factors beyond those studied here are predictive of local student viewpoints, and these remain an area for future research.
Practical Implications
Divergent viewpoints about the identity, scope, and future of chiropractic practice exist in our sample of Australian and New Zealand chiropractic students. The problem of conflicting professional identity is well reported in the chiropractic literature.32 The lack of a unified voice not only demoralizes chiropractors and chiropractic students it also may limit public acceptance of chiropractic and hinder the public from utilizing evidence-based care for common musculoskeletal pain.33 Our results provide a strong motivation for chiropractic institutions, along with local accreditation agencies (Council on Chiropractic Education Australia), to review their procedures for evaluating student applicants, program curriculum, and accreditation standards in order to ameliorate the disparity that exists in student opinion and therefore create consistency in the delivery of mainstream vs traditional models of chiropractic health care.
CONCLUSION
Chiropractic students in Australia and New Zealand simultaneously encompasses mainstream, orthodox, and potentially scientific views as well as traditional, unorthodox and potentially pseudoscientific opinions about chiropractic. A possible explanation for conflicting viewpoints may be factors associated with a student's chiropractic program of study. Indeed, viewpoints vary most when considering educational programs where there are internally conflicting and internally consisted opinions. What remains unclear is whether there is a causal relationship between institution and student opinion. Future prospective studies are now required that evaluate whether student opinions change over time and whether student opinion is moderated by additional education or experience gained in the field.
ACKNOWLEDGMENTS
We would like to thank those faculty members at each chiropractic program in Australia and New Zealand who assisted the investigators with dissemination of survey invitations and notifications to eligible participants.
FUNDING AND CONFLICTS OF INTEREST
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The authors declare that there are no conflicts of interest.
REFERENCES
- 1.Meeker WC, Haldeman S. Chiropractic: a profession at the crossroads of mainstream and alternative medicine. Ann Intern Med. 2002;136:216–227. doi: 10.7326/0003-4819-136-3-200202050-00010. [DOI] [PubMed] [Google Scholar]
- 2.Kosloff TM, Elton D, Shulman SA, Clarke JL, Skoufalos A, Solis A. Conservative spine care: opportunities to improve the quality and value of care. Popul Health Manage. 2013;16:390–396. doi: 10.1089/pop.2012.0096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Elton D, Kosloff TM. Using big data to advance value-based spine care. SpineLine, North American Spine Society. 2015;(September–October):17–22. [Google Scholar]
- 4.Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:478–491. doi: 10.7326/0003-4819-147-7-200710020-00006. [DOI] [PubMed] [Google Scholar]
- 5.Dagenais S, Tricco AC, Haldeman S. Synthesis of recommendations for the assessment and management of low back pain from recent clinical practice guidelines. Spine J. 2010;10:514–529. doi: 10.1016/j.spinee.2010.03.032. [DOI] [PubMed] [Google Scholar]
- 6.Hurwitz EL, Carragee EJ, van der Velde G, et al. Treatment of neck pain: noninvasive interventions: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine. 2008;33:S123–S152. doi: 10.1097/BRS.0b013e3181644b1d. [DOI] [PubMed] [Google Scholar]
- 7.Koes BW, van Tulder M, Lin C-WC, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur Spine J. 2010;19:2075–2094. doi: 10.1007/s00586-010-1502-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166:514–530. doi: 10.7326/M16-2367. [DOI] [PubMed] [Google Scholar]
- 9.McGregor M, Puhl AA, Reinhart C, Injeyan HS, Soave D. Differentiating intraprofessional attitudes toward paradigms in health care delivery among chiropractic factions: results from a randomly sampled survey. BMC Complement Altern Med. 2014;14:51. doi: 10.1186/1472-6882-14-51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Reggars JW. Chiropractic at the crossroads or are we just going around in circles? Chiropr Man Therap. 2011;19:11. doi: 10.1186/2045-709X-19-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chiropractic Board of Australia. Registrant Data (Reporting Period: 1 July 2016–30 September 2016) Melbourne: Chiropractic Board of Australia;; 2016. [Google Scholar]
- 12.Australian Health Workforce Ministerial Council. Regulatory Impact Statement for the Decision to Implement the Health Practitioner Regulation National Law. Canberra: Australian Health Minister's Advisory Council;; 2009. [Google Scholar]
- 13.Gliedt JA, Briggs S, Williams JSM, Smith DP, Blampied J. Background, expectations and beliefs of a chiropractic student population: a cross-sectional survey. J Chiropr Educ. 2012;26:146–160. doi: 10.7899/JCE-11-031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gliedt JA, Hawk C, Anderson M, et al. Chiropractic identity, role and future: a survey of North American chiropractic students. Chiropr Man Ther. 2015;23:4. doi: 10.1186/s12998-014-0048-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Meyers LS, Gamst G, Guarino A. Applied Multivariate Research: Design and Interpretation. Thousand Oaks, CA: Sage;; 2006. [Google Scholar]
- 17.Finch H. Comparison of the performance of nonparametric and parametric MANOVA test statistics when assumptions are violated. Methodol Eur J Res Methods Behav Soc Sci. 2005;1:27–38. [Google Scholar]
- 18.Sawilowsky S. New effect size rules of thumb. J Mod Appl Stat Methods. 2009;8:597–599. [Google Scholar]
- 19.Chiropractic 2025: Divergent Futures. Alexandria, VA: Institute for Alternative Futures;; 2013. Institute for Alternative Futures & NCMIC Foundation. [Google Scholar]
- 20.Innes SI, Leboeuf-Yde C, Walker BF. Similarities and differences of graduate entry-level competencies of chiropractic councils on education: a systematic review. Chiropr Man Ther. 2016. 24. [DOI] [PMC free article] [PubMed]
- 21.Schneider M, Murphy D, Hartvigsen J. Spine care as a framework for the chiropractic identity. J Chiropr Humanities. 2016;23:14–21. doi: 10.1016/j.echu.2016.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Clinical and professional chiropractic education: a position statement. 2016 https://http://www.mq.edu.au/_data/assets/pdf_file/0003/175755/Educational-Statements-PDF_2017.pdf Accessed August 1, 2017. [PMC free article] [PubMed]
- 23.Definition and position statement on the chiropractic subluxation. 2017 at http://www.therubicongroup.org/ - /policies. Accessed August 1, 2017.
- 24.Council on Chiropractic Education Australasia. Accreditation Standards for Chiropractic Programs. Canberra: Council on Chiropractic Education Australasia;; 2017. [Google Scholar]
- 25.Adams J, Lauche R, Peng W, et al. A workforce survey of Australian chiropractic: the profile and practice features of a nationally representative sample of 2,005 chiropractors. BMC Complement Altern Med. 2017;17:14. doi: 10.1186/s12906-016-1542-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gliedt JA, Schneider MJ, Evans MW, King J, Eubanks JE. The biopsychosocial model and chiropractic: a commentary with recommendations for the chiropractic profession. Chiropr Man Ther. 2017;25:16. doi: 10.1186/s12998-017-0147-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Commonwealth of Australia. National Registration and Accreditation Scheme. 2016 https://http://www.health.gov.au/internet/main/publishing.nsf/Content/work-nras Accessed 1 August 1, 2017.
- 28.Xue CC, Zhang AL, Lin V, Myers R, Polus B, Story DF. Acupuncture, chiropractic and osteopathy use in Australia: a national population survey. BMC Public Health. 2008;8:105. doi: 10.1186/1471-2458-8-105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:743–800. doi: 10.1016/S0140-6736(15)60692-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Walker BF. The new chiropractic. Chiropr Man Ther. 2016;24:26. doi: 10.1186/s12998-016-0108-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cramer EM, Bock RD. Multivariate analysis. Rev Educ Res. 1966;36:604–617. [Google Scholar]
- 32.Brown RA. Spinal Health: The Backbone of Chiropractic's Identity. J Chiropr Humanities. 2016;23:22–28. doi: 10.1016/j.echu.2016.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Qaseem A, Wilt TJ, McLean RM, Forciea M. for the Clinical Guidelines Committee of the American College of Physicians. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166:514–30. doi: 10.7326/M16-2367. [DOI] [PubMed] [Google Scholar]