

Abstract
Durability is an important quality of dental restorative materials, and the ability to autonomously heal damage incurred during their oral function is highly desirable.
Objective:
The objective was to evaluate the improvement in durability of self-healing dental composites (SHDCs) in terms of their resistance to fracture and capacity for healing of damage under monotonic and cyclic loading.
Methods:
SHDCs were prepared by incorporating dental resin composites with microcapsules containing healing liquid. Control specimens with the same mass fraction (5 % and 25 %) of microcapsules filled with water were also evaluated. Two sets of SHDCs were distinguished by the silane coupling agents that functionalized and bonded the microcapsules to resin network. One set used a methacrylate silane (MA-silane) that connected resin network through covalent bonds, and the other used a H-bonding forming hydroxyl silane (OH-silane). The fatigue crack growth resistance was assessed in terms of the threshold stress intensity range and the conventional Paris Law parameters. Cyclic loading was conducted at 5 Hz with maximum cyclic load ranged between approximately 1 N and 5 N. The efficiency of the autonomous healing was determined per the recovering of the fracture toughness and the extension of fatigue life.
Results:
The SHDCs with 5 wt% of healing microcapsules exhibited a larger fracture toughness than those with 25 wt% microcapsules. MA-silane SHDCs had approximately five times more responsive microcapsules triggered by fracturing of the composites. Consequently, the MA-silane SHDCs with 5 wt% of microcapsules achieved the best performance in terms of fracture toughness and healing efficiency. In regards to the fatigue crack growth behavior, there was a significant increase in the resistance to fatigue crack growth and 580 ± 15 % improvement in the fatigue life.
Significance:
Strong silanization is vital in SHDCs to simultaneously achieve clinically applicable mechanical performance and substantial healing capability. Moreover, the evaluation of self-healing under cyclic loading is a promising tool in quantifying the degree of fracture-induced healing.
Keywords: silane coupling agents, self-healing, dental composites, fatigue, fracture
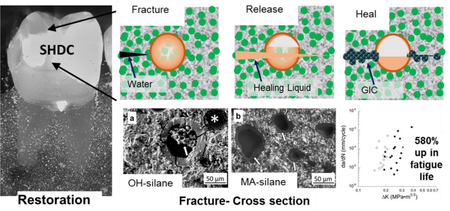
Graphical Abstract:
INTRODUCTION
Resin composites have become the primary restorative material in dentistry for direct restorations and are preferred over amalgams due to their superior aesthetics [1–6]. They contain three main components including a resin network, a filler and a coupling agent that bonds the resin and filler together [4, 5]. Resin composites currently suffer from short service life due to a variety of factors including the formation of secondary caries [7–11], resin degradation [12–14], microleakage generated by volumetric shrinkage of resin curing [12–18], and microcracks caused by stress and cyclic thermal changes in oral environments [19–22]. Synergism amongst these factors further increase the difficulty in achieving lifelong service.
A new Self-healing dental composite (SHDC) was recently designed to autonomously repair microcracks in the resin composite restorative [23]. The SHDC is based on an existing model of self-healing material originally proposed by White et al., [24] which has been adopted by others in developing SHDCs [25–28]. Our SHDC presents a biocompatible, cement-forming chemistry to replace the poisonous monomer-catalyst approach in White’s model. The SHDC heals cracks via formation of a clinically tested dental restorative material, glass ionomer cement (GIC) [29–32]. In addition, we used stronger silica microcapsules instead of polyurethane microcapsules. Specifically, in our SHDCs, GIC is produced when two healing components integrated into the material come into contact, namely calcium/strontium fluoroaluminosilicate particles and polyalkenoic acid (PAA) solutions, which are referred to as “healing powder (HP)” and “healing liquid (HL)”, respectively. The HL is protected by silica microcapsules to prevent premature GIC formation. Cracks extending within the SHDC cause fracture of the microcapsules and trigger release of the HL which then reacts with the HP. The newly formed GIC fills the cracks and heals the restorative [23].
Fatigue and fatigue crack growth are relevant modes of restored tooth failure because of the cyclic nature of mastication [33–37]. They are also relevant metrics that should be applied in evaluating the performance of SHDCs. The healing of engineered composite materials has largely focused on the recuperated fracture toughness after activation of the polymer catalyst As a consequence, prior evaluations on the self-healing efficiency of dental composites have been focused on the fracture toughness [23, 27]. Although bulk failure of the restoration occurs by fast-fracture, cracks reach a critical length because of cyclic crack extension. Therefore, the life of restorative materials is largely a function of their fatigue crack growth resistance, and any improvements resulting from the development of self-healing dental composites could make a substantial impact on the field of restorative dentistry.
In this study, the self-healing characteristics of experimental dental resin composites were evaluated in terms of the fracture toughness and the fatigue crack growth behavior. The SHDCs are compared to controls without HL and a quantification of the healing efficiency is explored.
MATERIALS & METHODS
Materials:
The resin monomers 2-bis(4-(2-hydroxy-3-methacryloxypropoxy)phenyl)-propane (Bis-GMA) and hydroxyethyl-methacrylate (HEMA) were supplied by Esstech Inc (Essington, PA, USA). The glass ionomer cement powder and healing liquid were purchased under the product name Riva Protect from SDI Ltd (Bayswater, VIC, Australia). All other reagents and solvents were purchased from Sigma-Aldrich (St. Louis, MO, USA) and used without treatment.
Micro-encapsulation of healing liquid:
The microcapsules containing healing liquid were prepared from a silica condensation method. A mixture of 4.0 mL SPAN 80 surfactant, 100 mL decahydronaphthalene, 4.0 mL milli-Q water, and 4.0 mL polyacrylic acid healing liquid was prepared as the water/oil emulsion. A separate silica mixture containing 4.0 mL TEOS and 1 mL hydrochloric acid (2 M) was mixed separately. After 1 hour, the silica mixture was added dropwise into the water/oil emulsion, and the combined mixture was stirred at 400 RPM. After one hour, the initial signs of precipitation were observed, and the stirring was continued with heating to 60 °C for 45 minutes. The resulting precipitate was collected by filtration and washed 3 times with ethanol to remove excess SPAN 80 surfactant. The precipitate formed was confirmed to have microcapsule structure from an examination performed by scanning electron microscopy.
Silanization of the microcapsules:
The microcapsules were surface-treated with silane to give them strong bonding with the methacrylate resins used in the composite, and to ensure that the microcapsules successfully rupture as the composite breaks. The microcapsules were added to a solution of 20 mL of hexane, 200 µL of bishydroxybutyl tetramethylsilane (OH-silane) or 3-methacryloxypropyltrimethoxy silane (MA-silane) and 20 µL of formic acid (88%), and stirred for 5 minutes. The microcapsules were re-collected by filtration and washed three times with hexane.
Construction of the SHDCs:
The Bis-GMA/HEMA resin mixture used for the SHDCs contained Bis-GMA (49.5%), HEMA (49.5%), camphorquinone (0.5%) and ethyl 4-(dimethylamino)benzoate (0.5%). The composite was made by mixing the following material: Bis-GMA/HEMA resin mixture (25%), strontium fluoroaluminasilicate glass powders (70 wt% or 50 wt%) and silanized microcapsules containing healing liquid (70 wt% or 50 wt%). This material was mixed using a speed mixer (DAC 150 FVZ, FlackTek, Landrum, SC, USA) at 3500 RPM for one minute, and then hand mixed carefully. The mixing process was repeated three times until the mixture became a uniformly mixed clay-like substance. The specimens evaluated by flexure were prepared in metal rectangular molds of the required dimensions, and photo-cured using a Triad 2000 Light-curing Unit (Dentsply, York, PA, USA) with a tungsten halogen light bulb (75 W and 120 V, 43 mW/cm2) for two min each from both open sides of the assembly. The hardened composite was then removed from the mold and polished by sandpaper (400 grit) until its surface become smooth. Variations in the material were achieved by increasing the wt% of microcapsules and reducing the wt% of the strontium fluoroaluminosilicate glass powders.
Crack growth resistance and healing efficiency testing:
For the crack growth resistance under monotonic loading and healing efficiency measurement, the SHDCs were molded into beams with a dimension of 4 × 3 × 25 mm3. A centrally located notch was placed on one side with a razor blade to achieve single edge v-notch beams (SEVNBs) as depicted in Figure 1a. The specimens were evaluated in 3-point bending using a universal testing machine (Instron 5500R, Instron Corp., Canton, MA, USA) with a loading rate of 1 mm/min. The specimens were loaded until the onset of fracture as identified by a sudden decrease in load, which was automatically recorded by the control software at the failure event. A drop of water was added into the notch of the specimen, and the specimen was rested for 3 days. The process was then repeated to measure the peak load to failure of the healed specimen. The healing efficiency for the apparent fracture toughness (Kc) was then calculated after Brown et al., according to [38]
| (1) |
Figure 1.

Schematic diagrams of the a) Single Edge V-Notch Beam (SEVNB) and, b) Compact Tension (CT) specimens used for evaluating the apparent fracture toughness and the fatigue crack growth resistance. All dimensions are listed in millimeters. For the CT specimen, the quantities a and W refer to the crack length and in-plane specimen width, respectively.
The fatigue crack growth resistance of the experimental resin composites under cyclic loading was evaluated using the compact tension (CT) specimen geometry. Specimens were prepared by first molding the body from the SHDC resin composite with dimensions of 2 × 6 × 8 mm3. A slicer/grinder (Chevalier, Smart H818II) was then used with diamond abrasive slicing heels to introduce a notch following the geometry in Figure 1b. The notches were sharpened using a razor blade and diamond paste, which served to facilitate the process of crack initiation. Two holes were also introduced using a miniature milling machine to accommodate Mode I loading. Detailed descriptions of this process have been described elsewhere [39, 40].
The CT specimens were subjected to a short period of cyclic loading using a commercial universal testing frame (BOSE, Model ELF 3100, Eden Prairie, MN, USA) and stress ratio (R = Pmin/Pmax) of 0.5 to initiate a crack from the prepared notch. Thereafter, cyclic loading was conducted at 5 Hz and stress ratio of 0.1. The maximum cyclic load ranged between approximately 1 and 5 N, depending on the resin composite formulation. Cyclic loading was conducted in increments of approximately 20K cycles after which the loading was stopped and the specimens were examined using a microscopic imaging system (Optem zoom 70xl 391940, QIOPTIQ, Luxembourg) with CCD camera to evaluate the crack length.
Using the crack length measurements and corresponding loads from the cyclic loading experiments, the stress intensity was calculated according to
| (2) |
where P is the opening load (Newtons) and the quantities α, and W are the measures of the specimen geometry (in mm) as illustrated in Figure 1b and the quantity B* refers to the specimen thickness. Note that Equation 2 is a simplified form of that applied for the inset CT specimen [39]. The configuration used in the present study has a uniform cross-section (without back-channel), a single elastic modulus and Poisson’s ratio (due to the absence of an inset), which enables the simplification.
The fatigue crack growth responses were evaluated in terms of the incremental rate of cyclic extension and the stress intensity range (ΔKI), which was obtained from the difference of the stress intensity at the maximum and minimum load of the fatigue cycle. For the fatigue crack growth responses, the steady state fatigue crack growth responses were characterized in terms of the Paris Law [Paris and Erdogan, 1963] according to
| (3) |
where C and m are the fatigue crack growth coefficient and exponent, respectively.
The healing efficiency was also calculated per results of the fatigue crack growth experiments. Due to the multiplicity of data obtained from these experiments, it was possible to quantify the efficiency of the SHDCs in two different manners. The stability of the fatigue crack growth response is represented by the overall range in stress intensity over which stable crack growth was achieved. For that measure of assessment, the efficiency was estimated according to
| (4) |
where ΔKhealed and ΔKcontrol are the average values of the total range in stress intensity that stable crack growth was achieved in the SHDC and control, respectively. It was also possible to evaluate the efficiency of healing in terms of the increase in life achieved from the onset of fatigue crack growth to unstable fracture. Considering the life, the efficiency of the SHDC was estimated according to
| (5) |
where Nhealed is the total number of cycles to failure for the samples with microcapsules filled with healing liquid and Ncontrol is the total number of cycles to failure for the material with microcapsules filled with water [41].
Scanning electron microscopy:
Selected specimens were mounted with carbon conductive tape on SEM stub and observed without coating under Hitachi 6600 field emission SEM (Tarrytown, NY, USA). Backscattering image was acquired under VP (variable pressure) mode, 60Pa vacuum with N2, and 15kV acceleration voltage.
Statistical analysis.
The fracture toughness values were analyzed using one-way analysis of variance (ANOVA) with a 95% confidence interval to indicate significant differences. The fatigue crack growth distributions were compared to establish significant differences between the groups using the Wilcoxon Rank Sum test with the critical value (alpha) set at 0.05.
RESULTS
Results from the experiments involving monotonic loading, including the apparent fracture toughness and the percentage of ruptured micro-capsules, are summarized in Table 1. Based on SEM image analyses, when MA-silane coupling agents were applied, approximately 72% of microcapsules at the fracture surface of composites were broken. In contrast, when OH-silane coupling agents were used, only approximately 17 % of the microcapsules were ruptured. This difference is due to the bonding strength between silane coupling agents and the resin network. The MA-silane formed covalent bonding with resin network through co-polymerization of vinyl (C=C) groups on MA-silane with the Bis-GMA and HEMA monomers, whereas the OH-silane coupling agents connected to resin network through much weaker hydrogen bonding. In addition, the potential wt% of broken microcapsules was calculated based on the wt% of microcapsules and the corresponding percentage of broken microcapsules, which is 72 % and 17% for MA-silane and OH-silane, respectively. The autonomous healing of SHDC was crack-induced, followed by reaction of HP and HL that is released from the broken microcapsules. Consequently, the wt% of broken microcapsules in SHDC played a significant role in healing because it determines the amount of available HL to react with HP.
Table 1.
The impact of silane coupling agents on fracture toughness and healing efficiency of the SHDCs and control composites
| wt % of microcapsules |
Material encapsulated |
Silane Coupling agent |
Broken micro-capsules |
KCini [MPa·m1/2] |
KCheal [MPa·m1/2] |
Healing efficiency [%] |
|
|---|---|---|---|---|---|---|---|
| % of micro- capsules |
wt% of composites |
||||||
| 0 % | No | no | -- | 0 | 0.92 ± 0.02 | -- | -- |
| 2.5 % | Water | MA-silane | 72 | 1.8 | 0.91 ± 0.07 | 0.07 ± 0.05 | 7.0 ± 6.0 |
| 2.5 % | HL | MA-silane | 72 | 1.8 | 0.90 ± 0.04 | 0.08 ± 0.02 | 9.1 ± 2.1 |
| 5 % | Water | MA-silane | 72 | 3.6 | 0.95 ± 0.04 | 0.11 ± 0.04 | 11.6 ± 3.4 |
| 5 % | HL | MA-silane | 72 | 3.6 | 0.91 ± 0.03 | 0.22 ± 0.03 | 24.2 ± 3.8 |
| 25 % | Water | MA-silane | 72 | 18.0 | 0.56 ± 0.07 | 0.14 ± 0.03 | 24.3 ± 2.0 |
| 25 % | HL | MA-silane | 72 | 18.0 | 0.57 ± 0.04 | 0.04 ± 0.01 | 6.8 ± 1.6 |
| 5 % | Water | OH-silane | 17 | 0.9 | 0.84 ± 0.07 | -- | -- |
| 5 % | HL | OH-silane | 17 | 0.9 | 0.83 ± 0.03 | -- | -- |
| 25 % | Water | OH-silane | 17 | 4.3 | 0.64 ± 0.10 | 0.13 ± 0.02 | 21.0 ± 3.0 |
| 25 % | HL | OH-silane | 17 | 4.3 | 0.75 ± 0.06 | 0.12 ± 0.04 | 16.0 ± 6.0 |
The fracture toughness of MA-silane composites were all determined by monotonic loading method. For the MA-silane SHDCs, the 5 wt% of microcapsule loading is pivotal: above this level, the fracture toughness was significantly decreased; below this level, no healing was achieved. As an example, the MA-silane SHDC containing 2.5 wt% of microcapsules didn’t heal after fracture, which suggests that there must be enough fractured microcapsules to provide sufficient healing materials to achieve crack-induced heal. Consequently, the 25 wt% OH-silane SHDCs may self-heal. However, due to its low initial apparent fracture toughness (Kc), the sensitivity of SEVNB method couldn’t differentiate SHDCs from the control composites with water-microcapsules. For the OH-silane SHDCs, the cyclic loading method was used to evaluate the fatigue crack growth response and healing efficiency.
A representative fatigue crack growth response for a OH-silane SHDC specimen with 25 wt% healing capsules is shown in Figure 2. The incremental fatigue crack growth measurements are labeled in this diagram to describe the history of cyclic crack extension. Note that there is an interesting change in the growth rate as a function of the stress intensity range. The data does not appear to occur sequentially, i.e. where increasing growth rate occurs because of the increase in magnitude of ΔK. The responses for the OH-silane SHDC with 5 wt% of microcapsules (H-5 %) and its water-containing control (NH-5 %) did not exhibit this behavior.
Figure 2.

Representative fatigue crack growth response for the self-healing dental composite with 25 wt% filler. The numbers denote the sequence of crack growth measurements (from 1 to7) over the history of incremental extension. Note the abrupt changes in crack growth rate (da/dN) from one point to the other and the retardation that takes place despite the increase in stress intensity range.
A comparison of the fatigue crack growth responses for the SHDCs (H-5 % and H-25 %) and their water-containing controls (NH-5 % and NH-25 %) is shown in Figure 3. Specifically, results for all of the samples prepared with 5 wt% and 25 wt% of microcapsules are shown in Figures 3a and 3b, respectively. According to the Wilcoxon Sum Rank Test, there was no significant difference (Z = −0.4834; p = 0.6288) in the fatigue crack growth responses of the 5%-SHDC, H-5%, and its control, NH-5%. However, for the SHDC with 25 wt% microcapsules, there was a significantly greater (Z = −4.4298; p = 0.000) fatigue crack growth resistance for the samples with healing liquid (H-25 %) in comparison to the formulation with water (NH-25 %) as apparent from the distribution in responses. A comparison of the data in Figures 3a and 3b shows that the SHDC with 25 wt% microcapsules exhibited lower fatigue crack growth resistance (i.e. underwent higher incremental crack growth) than the 5 wt% system.
Figure3.
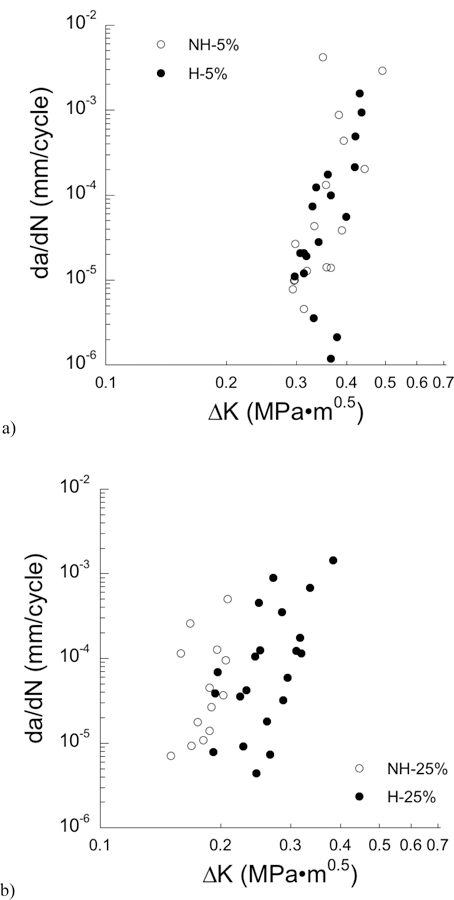
A comparison of the fatigue crack growth responses for the experimental composite with a) 5 wt% and b) 25 wt% filler particles in the healing (H) and non-healing (NH) conditions.
Due to the non-uniform nature of the fatigue crack growth responses of the SHDCs, the Paris Law parameters were not evaluated for the individual specimen responses. However, it was possible to pool the data obtained for the specimens prepared with each of the two formulations and to estimate the Paris Law parameters from the cumulative responses. For the SHDC with 5 wt% of microcapsules, the fatigue crack growth exponents were 9.5 and 10.0 for the capsules filled with healing liquid and water, respectively. Similarly, for the 25 wt% formulation, the fatigue crack growth exponents were 5.2 and 5.4 for the capsules with and without healing liquid, respectively. The larger value of fatigue crack growth exponent for the system with 5 wt% of microcapsules suggests that despite its larger fatigue crack growth resistance it is more sensitive to the stress intensity range and presence of a crack; it behaves in a more brittle manner.
The healing efficiency of the SHDC was calculated for the fatigue crack growth responses according to the measures described in equations 4 and 5. For the estimate based on the stress intensity range (Eqn. 4), the healing efficiency of the SHDC with 5 wt% and 25 wt% of healing capsules were 35 ± 30 % and 245 ± 80 %, respectively. For the estimate of efficiency based on the fatigue life (Eqn. 5), the healing efficiency of the SHDC with 5 wt% and 25 wt% healing capsules were approximately 80 ± 20 % and 580 ± 15 %, respectively. According to both of these measures, the SHDC with 25 wt% of microcapsules filled with healing liquid exhibited substantially greater healing efficiency.
The fracture surfaces of the OH-silane SHDC specimens were evaluated using scanning electronic microscopy and a representative micrograph from microcapsules-filled with healing liquid is shown in Figure 4a. A large microcapsule is evident near the center of this image and shows remnant healing liquid within the interior that has not reacted with the surrounding resin matrix. The shell of the microcapsule is clearly fractured. In addition, there is evidence of additional smaller microcapsules to the right, which have been pulled out of the surrounding matrix. The shell of the central microcapsule has also undergone partial separation from the surrounding resin matrix, which confirms the weak bonding between the microcapsule and the resin network. In contrast, the microcapsules were completely fractured in MA-silane SHDC. There is no gap at the interface of microcapsules and the rest of the composites, which positive indication for a good bonding (Figure 4b).
Figure 4.
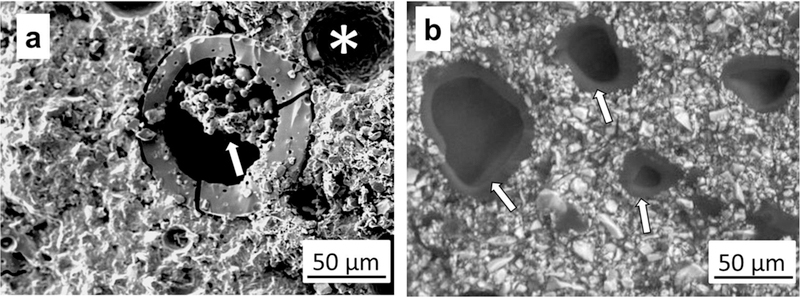
SEM images of SHDCs. a) OH-silane SHDC that contains healing liquid. The size of the microcapsules ranges between roughly 10 and 100 in diameter. Note that inside the large central microcapsule there is evidence of the reaction of healing liquid (arrow). In addition, the micrograph shows that not all the microcapsules were effective in releasing their healing liquid as some were pulled out from the surrounding matrix material (asterisk). b) MA-silane SHDC; arrows point at the edge of fractured microcapsules. Both large and small microcapsules were ruptured.
DISCUSSION
The results obtained from monotonic and cyclic loading of the OH-silane SHDC samples showed that healing was achieved under both conditions of loading. In addition, it was apparent from the differences in responses for the material with 5 wt% and 25 wt% microcapsules that the mass fraction of healing capsules, and their contents, had an important contribution to the durability. There were some interesting differences in the apparent healing of the SHDC from the fracture toughness and fatigue crack growth results that warrant discussion.
The OH-silane SHDC with 5 wt% microcapsules exhibited larger fracture toughness than the formulation with 25 wt% microcapsules, which was expected due to the larger mass fraction of healing capsules. Results from cyclic loading showed that both the 5 wt% and 25 wt% formulations exhibited capacity for healing. While the 5 wt% formulation did not change the degree of crack growth resistance, it did result in an increase in fatigue life as determined from the efficiency (λN). But in contrast to the results from monotonic loading, the SHDC with 25 wt% microcapsules exhibited greater healing efficiency. When evaluated in terms of the increase in crack growth stability, the addition of 25 wt% microcapsules with healing liquid resulted in approximately 240 % healing efficiency, whereas when quantified in terms of the fatigue life, the healing efficiency was nearly 600 %. These results exceed the degree of healing reported by Brown et al., for an epoxy composite [41]. Indeed, the larger fatigue crack growth resistance of the 25 wt% formulation with microcapsules filled with healing liquid is very apparent in Figure 3b. The larger healing efficiency for the 25 wt% system highlights the importance of the healing liquid in the repair process, as well as the importance of time. Clearly the healing liquid causes a larger degree of crack growth retardation due to the formation of GIC. While the volume fraction of microcapsules and their collective volume may not be sufficient to cover the entire surface area of the crack, the spatial distribution of GIC across the crack face form a family of bonded regions. Together they serve to tie the two crack faces together and promote extrinsic toughening, which imparts crack-tip shielding and reduces the magnitude of local (i.e. near-tip) stress intensity [42].
In reconciling the differences in healing efficiency estimated from results of monotonic and cyclic loading, there are two important considerations. First, although interrelated, the fatigue crack growth resistance and the fracture toughness are two different aspects of performance [42]. The addition of microcapsules within the resin matrix can increase the development of intrinsic microstructural damage under cyclic loading that facilitates fatigue crack growth. Debonding between the microcapsules and resin network (e.g. Figure 4a), as well as microcracking of the surrounding composites induced by the stress concentrations at the microcapsule boundaries are two such contributors. Those mechanisms can increase the incremental rate of cyclic extension, as noted in Figure 3, and are akin to those arising from the tubules during cyclic crack growth in dentin [43]. Due to the differences in these mechanisms of crack extension and toughening in fatigue and fracture, the effectiveness of healing will also be slightly different under monotonic and cyclic loading. Furthermore, it is necessary to consider the difference in time scale of crack extension and crack repair in the fracture toughness and fatigue crack growth processes. Those specimens subjected to monotonic loading were allowed to undergo healing for a period of three days before being evaluated again. In the case of fatigue, cyclic loading was performed continuously; the cracks grew progressively over the testing and took place over a few days or more. Thus, healing can occur under cyclic loading, but without a prolonged period of “rest”. As such, the rate of the polymerization that results after fracture of the microcapsules and the corresponding extrinsic toughening incurred are crucial considerations. This healing mechanism appears to be very effective at promoting an increase in fatigue resistance with 25 wt% microcapsules, but at the cost of a modest reduction of fracture toughness (Table 1).
In an assessment of self-healing epoxy composites, Brown et al. reported that the degree of crack-retardation and repair achieved was largely dependent on the stress intensity range [41]. If the operating stress intensity range was a significant percentage of the mode-I fracture toughness, a rest period was essential. At loading with moderate ΔK (ΔK = 0.5 to 0.7•Kc), they reported that in situ healing extended the fatigue life by over 200 %. Further improvements in fatigue life-extension were achieved by employing a rest period, which enabled permanent arrest at the aforementioned range of moderate ΔKI. At lower values of applied stress intensity range (and substantially smaller incremental fatigue crack growth rates), self-healing yielded complete arrest of fatigue cracks, thereby providing infinite fatigue life. One drawback of the present investigation of the SHDC is that the fatigue crack growth experiments did not incorporate a rest period. A rest period is expected to be an integral part of oral habits, and would be expected to increase the degree of healing efficiency achieved through the progression of polymerization. According to the intended application of SHDCs and the daily routine of mastication, it will be pertinent to design a fatigue loading protocol that is tuned to the oral environment and that is used routinely in future studies as a standard of assessment.
The present investigation is the first to evaluate the performance of dental composites designed with capacity for healing in terms of the fatigue crack growth resistance, and to compare the relative performance of SHDCs under monotonic and cyclic loading. Both manners of loading and the corresponding effectiveness of healing are clearly important to the ability of dental materials to support lifelong oral health. Nevertheless, there are important limitations to the investigation that pertain to methods of testing and the OH-silane SHDC. The fatigue crack growth experiments were conducted with a cyclic frequency of 5 Hz. That is greater than the frequency of mastication, which is roughly 2 Hz [44]. The cyclic loading protocol was chosen to balance concerns regarding clinical relevance and the time necessary to perform the experiments and obtain meaningful results. It also increases opportunity for comparison to results on the supporting hard tissues [37, 45]. The degree of self-healing is dependent on the time available for GIC curing, and could contribute to the measures of healing efficiency in fatigue. In this case, the reaction of HL and HP formed a solid GIC in 9 min (set-time of this GIC). Future SHDC design should consider to optimize the setting time of GIC, which should provide sufficient time for HL to reach HP and most importantly deliver the immediate heal to damages. Moreover, experiments may be conducted with a lower frequency to increase the clinical applicability of the data, especially on the MA-silane SHDCs. In addition, a testing protocol that involves cyclic loading intervals and intermittent periods of rest (i.e. without cyclic loading) may be considered in future evaluations as commented previously. It would be possible to design loading and rest schedules according to daily routines involving mastication.
There are also some limitations of the OH-silane SHDC that were recognized from the results of the experiments. In observation of the fracture surfaces corresponding to fatigue crack growth it was found that not all of the capsules were clearly fractured by interaction with the crack. Many of the microcapsules underwent pullout from the surrounding matrix, rather than fracture. That observation agrees well with our experimental design that the silanization treatment was not completely effective at binding the capsules to the methacrylate resin.
The use of MA-silane coupling agents overcame the limitations in OH-silane SHDCs owing to the enhanced bonding between microcapsules and resin network. First, the percentage of broken microcapsules was substantially increased, which will supply sufficient HL to form GIC with HP by using much less wt% of microcapsules. Second, there is no de-bonding at the microcapsule shell/matrix interface. In fact, it was nearly impossible to differentiate the shell of the microcapsules from the rest of the composites in the SEM analysis. Third, the average diameter of broken microcapsules was significantly reduced to approximately 20 µm. The overall impact of these improvements translated into significantly enhanced fracture toughness with the same healing efficiency. For example, the 5 % MA-silane SHDC achieved the same healing efficiency as that of the 25 wt% OH-silane SHDC, and is much tougher as evidenced by the 50 % greater fracture toughness.
CONCLUSION
In summary, the MA-silane SHDCs achieves the best balance of healing efficiency (24.2 ±3.8 %) and fracture toughness at 5 wt% loading of microcapsules. The structural durability of the OH-silane SHDCs was evaluated in terms of its apparent fracture toughness and with respect to the fatigue crack growth resistance. For the system with 25 wt% microcapsule, the healing efficiency determined from the relative crack stability and the increase in fatigue life achieved was 245 % and 580 %, respectively. This difference in fatigue life was not recognized by the monotonic loading method, due to the limited sensitivity posed by the relatively low fracture toughness of the SHDCs. The findings provide convincing evidence that the design and development of self-healing materials for dentistry may require an evaluation of performance that considers both monotonic and cyclic loading.
Highlights:
Self-healing dental composites (SHDC) heal cracks autonomously
SHDC heals under both monotonic and cyclic loading
Fatigue life of SHDC is enhanced up to 580 %.
Strong silanization is vital in SHDCs to simultaneously achieve clinically applicable mechanical performances and substantial healing capability.
Compact tension with cyclic loading is more sensitive and provides more information than monotonic SEVNB method in evaluating healing of SHDCs.
ACKNOWLEDGEMENTS
This work was funded by the National Institute of Dental and Craniofacial Research (U01DE023752). Financial support was also provided through the ADA Foundation. The authors would like to thank Dr. Rafael Bowen, Mr. Anthony Giuseppetti, and Mr. George Quinn for their technical recommendations. We also would like to thank Center for Nanoscale Science and Technology (CNST) at NIST for their technical support.
Support for the following investigation was provided by the National Institute of Dental and Craniofacial Research (U01DE023752) and the American Dental Association Foundation.
Acronyms and abbreviations:
- (Bis-GMA)
2-bis(4-(2-hydroxy-3-methacryloxypropoxy)phenyl)-propane
- (CT)
compact tension
- (GIC)
glass ionomer cement
- (HEMA)
hydroxyethyl-methacrylate
- (HL)
healing liquid
- (HP)
healing powder
- (MA-silane)
methacrylate silane
- (OH-silane)
hydroxyl silane
- (wt%)
Mass fraction
- (H-25 %)
OH-silane SHDC with 25 wt% of microcapsules
- (H-5 %)
OH-silane SHDC with 5 wt% of microcapsules
- (NH-25 %)
OH-silane water-containing control with 25 wt% of microcapsules
- (NH-5 %)
OH-silane water-containing control with 5 wt% of microcapsules
- (SEVNBs)
single edge v-notch beams
- (SHDCs)
self-healing dental composites
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- [1].Atai M, Watts DC, Atai Z. Shrinkage strain-rates of dental resin-monomer and composite systems. Biomaterials 2005;26:5015–20. [DOI] [PubMed] [Google Scholar]
- [2].Bacchi A, Consani RL, Martim GC, Pfeifer CS. Thio-urethane oligomers improve the properties of light-cured resin cements. Dental Materials 2015;31:565–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Cramer NB, Stansbury JW, Bowman CN. Recent Advances and Developments in Composite Dental Restorative Materials. Journal of Dental Research 2011;90:402–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Ferracane JL. Resin composite-State of the art. Dental Materials 2011;27:29–38. [DOI] [PubMed] [Google Scholar]
- [5].Ferracane JL. Resin-based composite performance: Are there some things we can’t predict? Dental Materials 2013;29:51–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Jandt KD, Sigusch BW. Future perspectives of resin-based dental materials. Dental Materials 2009;25:1001–6. [DOI] [PubMed] [Google Scholar]
- [7].Bourbia M, Ma D, Cvitkovitch DG, Santerre JP, Finer Y. Cariogenic bacteria degrade dental resin composites and adhesives. Journal of Dental Research 2013;92:989–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Manhart J, Chen HY, Hamm G, Hickel R. Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition. Oper Dent 2004;29:481–508. [PubMed] [Google Scholar]
- [9].Mjor IA, Toffenetti OF. Secondary caries: A literature review with case reports. Quintessence Int 2000;31:165–79. [PubMed] [Google Scholar]
- [10].Beck F, Lettner S, Graf A, Bitriol B, Dumitrescu N, Bauer P, et al. Survival of direct resin restorations in posterior teeth within a 19-year period (1996–2015): A meta-analysis of prospective studies. Dental Materials 2015;31:958–85. [DOI] [PubMed] [Google Scholar]
- [11].Opdam NJM, Bronkhorst EM, Loomans BAC, Huysmans M. 12-year survival of composite vs. Amalgam restorations. Journal of Dental Research 2010;89:1063–7. [DOI] [PubMed] [Google Scholar]
- [12].De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Braem M, et al. A critical review of the durability of adhesion to tooth tissue: Methods and results. Journal of Dental Research 2005;84:118–32. [DOI] [PubMed] [Google Scholar]
- [13].Delaviz Y, Finer Y, Santerre JP. Biodegradation of resin composites and adhesives by oral bacteria and saliva: A rationale for new material designs that consider the clinical environment and treatment challenges. Dental Materials 2014;30:16–32. [DOI] [PubMed] [Google Scholar]
- [14].Gonzalez-Bonet A, Kaufman G, Yang Y, Wong C, Jackson A, Huyang G, et al. Preparation of dental resins resistant to enzymatic and hydrolytic degradation in oral environments. Biomacromolecules 2015;16:3381–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Hakimeh S, Vaidyanathan J, Houpt ML, Vaidyanathan TK, Von Hagen S. Microleakage of compomer Class V restorations: Effect of load cycling, thermal cycling, and cavity shape differences. J Prosthet Dent 2000;83:194–203. [DOI] [PubMed] [Google Scholar]
- [16].Sun J, Eidelman N, Lin-Gibson S. 3D mapping of polymerization shrinkage using X-ray micro-computed tomography to predict microleakage. Dental Materials 2009;25:314–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Sun JR, Fang R, Lin N, Eidelman N, Lin-Gibson S. Nondestructive quantification of leakage at the tooth-composite interface and its correlation with material performance parameters. Biomaterials 2009;30:4457–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Taylor MJ, Lynch E. Microleakage. J Dent 1992;20:3–10. [DOI] [PubMed] [Google Scholar]
- [19].Drummond JL, Bapna MS. Static and cyclic loading of fiber-reinforced dental resin. Dental Materials 2003;19:226–31. [DOI] [PubMed] [Google Scholar]
- [20].Ferracane JL, Mitchem JC. Relationship between composite contraction stress and leakage in Class V cavities. Am J Dent 2003;16:239–43. [PubMed] [Google Scholar]
- [21].Moraes RR, Garcia JW, Barros MD, Lewis SH, Pfeifer CS, Liu JC, et al. Control of polymerization shrinkage and stress in nanogel-modified monomer and composite materials. Dental Materials . 2011;27:509–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Xu H, Eichmiller FC, Smith DT, Schumacher GE, Giuseppetti AA, Antonucci JM. Effect of thermal cycling on whisker-reinforced dental resin composites. Journal of Materials Science-Materials in Medicine 2002;13:875–83. [DOI] [PubMed] [Google Scholar]
- [23].Huyang G, Debertin AE, Sun JR. Design and development of self-healing dental composites. Mater Des 2016;94:295–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].White SR, Sottos NR, Geubelle PH, Moore JS, Kessler MR, Sriram SR, et al. Autonomic healing of polymer composites. Nature 2001;409:794–7. [DOI] [PubMed] [Google Scholar]
- [25].Hillewaere XKD, Du Prez FE. Fifteen chemistries for autonomous external self-healing polymers and composites. Prog Polym Sci 2015;49–50:121–53. [Google Scholar]
- [26].Lehn JM. Perspectives in Chemistry-Aspects of Adaptive Chemistry and Materials. Angewandte Chemie-International Edition 2015;54:3276–89. [DOI] [PubMed] [Google Scholar]
- [27].Wu JL, Weir MD, Zhang Q, Zhou CJ, Melo MAS, Xu HHK. Novel self-healing dental resin with microcapsules of polymerizable triethylene glycol dimethacrylate and N,N-dihydroxyethyl-p-toluidine. Dent Mater 2016;32:294–304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Zhu DY, Rong MZ, Zhang MQ. Self-healing polymeric materials based on microencapsulated healing agents: From design to preparation. Prog Polym Sci 2015;49–50:175–220. [Google Scholar]
- [29].Meyer JM, Cattani-Lorente MA, Dupuis V. Compomers: between glass-ionomer cements and composites. Biomaterials 1998;19:529–39. [DOI] [PubMed] [Google Scholar]
- [30].Mickenautsch S, Yengopal V, Banerjee A. Pulp response to resin-modified glass ionomer and calcium hydroxide cements in deep cavities: A quantitative systematic review. Dental Materials 2010;26:761–70. [DOI] [PubMed] [Google Scholar]
- [31].Nicholson JW. Polyacid-modified composite resins (“compomers”) and their use in clinical dentistry. Dental Materials 2007;23:615–22. [DOI] [PubMed] [Google Scholar]
- [32].Wilson AD, Kent BE. New translucent cement for dentistry - glass ionomer cement. Br Dent J 1972;132:133–&. [DOI] [PubMed] [Google Scholar]
- [33].Arola D, Huang MP, Sultan MB. The failure of amalgam dental restorations due to cyclic fatigue crack growth. Journal of Materials Science-Materials in Medicine 1999;10:319–27. [DOI] [PubMed] [Google Scholar]
- [34].Bajaj D, Sundaram N, Arola D. An examination of fatigue striations in human dentin: In vitro and In vivo. J Biomed Mater Res Part B 2008;85B:149–59. [DOI] [PubMed] [Google Scholar]
- [35].Nalla RK, Imbeni V, Kinney JH, Staninec M, Marshall SJ, Ritchie RO. In vitro fatigue behavior of human dentin with implications for life prediction. J Biomed Mater Res Part A 2003;66A:10–20. [DOI] [PubMed] [Google Scholar]
- [36].Yahyazadehfar M, Ivancik J, Majd H, An BB, Zhang DS, Arola D. On the mechanics of fatigue and fracture in teeth. Appl Mech Rev 2014;66:19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Arola D Fatigue testing of biomaterials and their interfaces. Dent Mater 2017;33:367–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Brown EN, Sottos NR, White SR. Fracture testing of a self-healing polymer composite. Exp Mech 2002;42:372–9. [Google Scholar]
- [39].Yahyazadehfar M, Nazari A, Kruzic JJ, Quinn GD, Arola D. An inset CT specimen for evaluating fracture in small samples of material. J Mech Behav Biomed Mater 2014;30:358–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Zhang D, Nazari A, Soappman M, Bajaj D, Arola D. Methods for examining the fatigue and fracture behavior of hard tissues. Exp Mech 2007;47:325–36. [Google Scholar]
- [41].Brown EN, White SR, Sottos NR. Retardation and repair of fatigue cracks in a microcapsule toughened epoxy composite - Part 1: Manual infiltration. Composites Science and Technology 2005;65:2466–73. [Google Scholar]
- [42].Ritchie RO. Mechanisms of fatigue-crack propagation in ductile and brittle solids. Int J Fract 1999;100:55–83. [Google Scholar]
- [43].Ivancik J, Neerchal NK, Romberg E, Arola D. The reduction in fatigue crack growth resistance of dentin with depth. J Dent Res 2011;90:1031–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Po JMC, Kieser JA, Gallo LM, Tesenyi AJ, Herbison P, Farella M. Time-frequency analysis of chewing activity in the natural environment. J Dent Res 2011;90:1206–10. [DOI] [PubMed] [Google Scholar]
- [45].Arola D, Bajaj D, Ivancik J, Majd H, Zhang D. Fatigue of biomaterials: Hard tissues. Int J Fatigue 2010;32:1400–12. [DOI] [PMC free article] [PubMed] [Google Scholar]