

Abstract
Although bystander programs to prevent relationship and sexual violence have been evaluated with college students, few evaluations have been conducted with high school students. This study evaluated the effectiveness of TakeCARE, a brief video bystander program designed to promote helpful bystander behavior in situations involving relationship violence among high school students. Students (N = 1,295; 52.5% female; 72.3% Hispanic) reported their bystander behavior at a baseline assessment. Classrooms (N = 66) were randomized to view TakeCARE or to a control condition, and high school counselors administered the video in the classrooms assigned to view TakeCARE. Students again reported their bystander behavior at a follow-up assessment approximately 3 months afterward. Results indicate that students who viewed TakeCARE reported more helpful bystander behavior at the follow-up assessment than students in the control condition. Results of exploratory analyses of the likelihood of encountering and intervening upon specific situations calling for bystander behavior are also reported. TakeCARE is efficacious when implemented in an urban high school by high school counselors.
Keywords: bystander intervention, adolescent relationship violence, randomized-controlled trial, high school
Introduction
Approximately 18% of teens in the United States (US) report experiencing physical or sexual violence in dating relationships (Taylor & Mumford, 2014), and ethnic minority students report higher rates than Whites (Kann et al., 2016). Such victimization contributes to a range of mental health and adjustment difficulties, including depressive symptoms (Banyard & Cross, 2008), suicidal ideation (Nahapetyan, Orpinas, Song, & Holland, 2014), relationship distress (Jouriles, Garrido, Rosenfield, & McDonald, 2009), and substance use (Foshee, Reyes, Gottfredson, Chang, & Ennett, 2013), as well as increased risk for re-victimization (Exner-Cortens, Eckenrode, & Rothman, 2013). A number of relationship violence and sexual assault prevention programs have been developed for teens, including several bystander programs (e.g., Cook-Craig et al., 2014; Katz, Heisterkamp, & Fleming, 2011; Miller et al., 2013). The goal of bystander programs is to increase helpful responses from bystanders—those who witness violent or potentially violent situations. More specifically, these programs attempt to prompt bystanders to act to prevent sexual and relationship violence from occurring, and to support victims of such violence. Examples of helpful bystander behavior include interrupting a heated argument between a friend and his or her partner, and expressing concern for a friend who has had an unwanted sexual experience.
TakeCARE is a video designed to promote helpful bystander behavior, with the broader goal of reducing relationship violence among high school and college students. Specifically, TakeCARE capitalizes on knowledge about the salience of peer relationships to adolescents (Steinberg & Monahan, 2007) and that adolescents are most likely to be victimized in settings in which friends are nearby (e.g., at school or at a friend’s house) (Young, Grey, & Boyd, 2008). As a result, TakeCARE contextualizes helpful bystander behavior as “friends helping friends.” Additionally, because self-efficacy is an important determinant of bystander behavior among adolescents and emerging adults (Jouriles, Rosenfield, Yule, Sargent, & McDonald, 2016), TakeCARE focuses on building self-efficacy to intervene. Furthermore, TakeCARE was designed with ease of administration and scalability in mind (Kleinsasser, Jouriles, McDonald, & Rosenfield, 2015). The video format allows it to be easily distributed to students across an entire high school or college campus; this is in contrast to many other bystander programs, which are typically administered by trained facilitators to students in a small-group format. The latter format, although potentially effective, can be cost-prohibitive for schools desiring campus-wide dissemination.
Previous evaluations of TakeCARE have been conducted with college student samples. In three separate trials, college students completed baseline questionnaires on helpful bystander behavior, and then were randomized to view either TakeCARE or a control video. Those assigned to view TakeCARE then watched the video at an individual computer in a small computer lab that was monitored by a research assistant. One to two months later, all students completed follow-up questionnaires on helpful bystander behavior. Results of each trial indicated that those who viewed TakeCARE reported engaging in more helpful bystander behavior during the follow-up period than those in the control condition (Kleinsasser et al., 2015; Jouriles et al., 2016). These three trials included students from two different universities and at different time points during their college careers, although all three samples were predominantly White; students also viewed TakeCARE under highly controlled conditions. Thus, although the findings from these evaluations of TakeCARE provide some promising empirical evidence of TakeCARE’s value, TakeCARE’s effectiveness with high-school students, with more ethnically diverse student populations, and when administered under less tightly controlled conditions is unclear.
There are important differences between high school and college students that have implications for whether findings based on samples of college students generalize to high school students. For example, there is some evidence that the determinants of bystander behavior differ for high school and college students, although self-efficacy appears to be important for both (Jouriles et al., 2016). Additionally, high-school aged adolescents tend to engage in more risky decision-making in the presence of peers than do college-aged young adults (Gardner & Steinberg, 2005), and decision-making style potentially influences whether or not an individual engages in helpful bystander behavior. There are also reasons to believe that findings with White college students may not generalize to minority youth. Rates of relationship violence (Kann et al., 2016) and helpful bystander behavior (Brown, Banyard, & Moynihan, 2014) are higher among minority youth, compared to White youth. It might be reasoned if students are already engaging in relatively high levels of bystander behavior in an attempt to address relationship and sexual violence, it is not clear if a brief program is likely to further increase bystander behavior. To our knowledge, there is no research that has explicitly examined how the ethnic composition of the sample might influence effects of a bystander program designed to help prevent violence. In short, it cannot simply be assumed that the documented positive effects of TakeCARE among college students will generalize to a diverse sample of high school students.
To date, the evaluations of TakeCARE have been conducted under highly controlled conditions (e.g., students viewed TakeCARE individually in a monitored computer lab) that are unlikely to occur in a typical high school setting. Effectiveness trials conducted in naturalistic settings (e.g., high school classrooms), with program implementation carried out by personnel for whom intervention dissemination is intended (e.g., school personnel), are necessary to get a true indication if TakeCARE can be effective in high schools (Weisz, Ng, & Bearman, 2014). Notably, few adolescent relationship and sexual violence prevention programs—bystander or otherwise—have been evaluated under real-world conditions (see Miller et al., 2013 as an example of a bystander program exception). In short, TakeCARE appears to be a promising, inexpensive, and easily scalable bystander program. However, it has not yet been evaluated with high school students, with ethnic minority samples, or under real-world conditions.
The Current Study
The primary aim of this study was to examine TakeCARE’s effects when administered to a sample comprised primarily of ethnic minority high school students—in their normal classroom setting by high school staff. We hypothesized that students who viewed TakeCARE, compared to those in the control condition, would report engaging in more helpful bystander behavior at a follow-up assessment conducted approximately three months following the intervention. This finding would extend findings from prior evaluations of TakeCARE to an ethnic minority high school sample, using an administration method that should not pose logistical or resource barriers to future administrations of TakeCARE in most high schools.
A second aim of the study was to explore the types of situations that high school students encounter that call for bystander behavior and to examine whether the likelihood of engaging in helpful bystander behavior differs across those situations. Specifically, engaging in bystander behavior is contingent upon encountering a situation that calls for such behavior, and certain situations that call for bystander behavior may occur less frequently than others. In addition, students may be more or less likely to intervene in these different situations, depending on characteristics of the situation (McMahon & Banyard, 2012). For example, seeing a friend in a heated argument with a partner, and being told by a friend that he or she had experienced an unwanted sexual experience, may both call for a helpful response. However, their relative frequency of occurrence, and whether they are equally likely to elicit a helpful response, is unknown. We expected considerable variability in the likelihood that students would encounter different situations that call for helpful bystander behavior. We also expected variability in the likelihood that students would respond to these different situations with helpful bystander behavior.
The third aim of the study was to evaluate TakeCARE’s effects after controlling for the variability in the different types of situations students encountered. Research on the evaluation of bystander programs has thus far not accounted for possible differences in the nature and frequency of situations that students may encounter at baseline and follow-up assessments. We hypothesized TakeCARE to increase the likelihood of helpful bystander behavior in situations students report encountering both at baseline and at follow-up. This essentially controls for variation in the situations students experienced.
Methods
Participants
Participants were 1,295 students recruited from an economically disadvantaged (84.3% of students qualified for free or reduced lunch), Title I, urban public high school. Participants (52.5% female) ranged from 13 to 19 years old (M = 15.27, SD = 0.88), and the sample included 449 (34.7%) 9th graders, 566 (43.7%) 10th graders, 248 (19.2%) 11th graders, and 6 (0.5%) 12th graders, with 26 students not reporting their grade. All students were enrolled in year-long social studies courses. The sample was predominantly Hispanic (n = 936, 72.3%), and of those who were not Hispanic, there were 233 (18.0%) Black, 18 (1.4%) “More than one race,” 15 (1.2%) Asian, 10 (0.8%) “Other,” 7 (0.5%) White, 4 (0.3%) American Indian/Alaska Native, and 1 (0.08%) Native Hawaiian or Other Pacific Islander. Seventy-one students (5.5%) did not provide their race or ethnicity. The racial and ethnic composition of our sample reflects that of the high school from which students were recruited.
Procedures
The university Institutional Review Board and the school district Research Review Board approved the research procedures. Participating students were informed that they would help evaluate new classroom materials by filling out questionnaires on two occasions, and watching an educational video. Participating students provided assent, but since study procedures were administered by school personnel (school counselors) as part of the curriculum provided by counselors, parental consent was not deemed necessary by the university’s nor the high school district’s review board.
Five school counselors (C1, C2, C3, C4, and C5) assisted with the evaluation, each of whom had responsibility for guest-teaching health topics in social-studies classes throughout the school year. The classrooms (n = 66) were randomly assigned to condition (TakeCARE or control), within counselor. Randomization resulted in the following condition assignments: C1: 5 TakeCARE, 5 control (234 students); C2: 9 TakeCARE, 9 control (348 students); C3: 8 TakeCARE, 8 control (319 students); C4: 10 TakeCARE, 7 control (288 students); and C5: 1 TakeCARE, 4 control (n = 106 students). The counselors were each assigned their own year - long social studies classes and students do not enroll in multiple social studies classes. Thus, it is highly unlikely that students in the control condition viewed TakeCARE in another classroom.
Students completed baseline questionnaires in November 2014, after which, those in classrooms assigned to view TakeCARE watched the TakeCARE video, and students in the control condition saw a presentation on another topic (see below). Students completed follow-up questionnaires no less than 3 months following the baseline assessment, in February, March, or April of 2015. The mean number of days between completion of the baseline and follow-up assessments was: M = 129.43, SD = 21.46. The TakeCARE and control conditions did not differ on the number of days between assessment points, F( 1, 919) = .082, p = .78. All procedures took place during regular school hours.
Although counselors collected baseline data in 66 classrooms, follow-up data were collected in only 57, due to counselor difficulty getting into all assigned classrooms toward the end of the school year. Thus, the final sample included 921 students with complete data (71% of the sample), and the analyses were conducted with the data provided by these 921 students. Students who completed follow-up assessments did not differ from those who did not on ethnicity, age, or baseline bystander behavior, χ2(1, N = 1228) = 0.36, p = .551, F(1, 1282) = 1.11, p = .292, and F(1, 1285) = .00, p = .96, respectively. Those with complete data, however, were more likely to be female (53.9% female), χ2(1, N = 1279) = 5.79, p = .016. Of the 921 students with complete data, 463 (n = 29 classes) viewed TakeCARE and 458 (n = 28 classes) were in the control condition.
Experimental Conditions
TakeCARE.
When initially developing TakeCARE, we held discussions about the problem of relationship and sexual violence, and perceptions of barriers to responsive bystander behavior, with diverse groups of students, staff, and administrators (over 30 meetings with over 250 individuals) from college and high school campuses. Initial meetings revealed that, from a student’s perspective, “not knowing what to do” was the biggest obstacle to responsive bystander action. Additionally, staff and administrators emphasized the desire to foster a sense of responsibility among teens and young adults for helping their peers. Consequently, a key outcome was the decision to target self-efficacy (i.e., students’ confidence that they can do something to help) and responsibility. Later meetings involved showing draft versions of TakeCARE and obtaining feedback. An important message received from these meetings was the need to be brief, engaging, tightly focused, and not to try to address all of the different barriers suggested by theory and research (e.g., lack of empathy for victims). Covering too much material diluted the impact of the message.
The TakeCARE video used in this research presents a series of vignettes involving dating violence, including a risky (i.e., potentially violent) situation, an actively violent situation, and one depicting support after a risky situation has already occurred. These vignettes depict situations of physical, sexual, and psychological relationship violence, including 1) an intoxicated couple at a party deciding to go to a bedroom (i.e., risk for sexual assault), 2) a couple is unsure whether sexual activity took place after a night of heavy drinking, and 3) a heated argument during which one partner slaps the other. By varying the gender of victim and perpetrator across vignettes, TakeCARE emphasizes that both males and females can be involved in relationship violence. Through voice-over narration and text, the video also presents information on identifying abusive dating relationships, the definition of and issues around consent to sexual activity (e.g., intoxication, value of affirmative consent), and providing support to someone who discloses that non-consensual or distressing consensual sex has already occurred (e.g., accompanying a friend to a health clinic). In each vignette, the actors respond as helpful bystanders to 1) prevent a negative consequence from occurring, 2) de-escalate a situation, or 3) support a friend after a risky situation has already happened. After each vignette, the narrator offers additional examples of helpful bystander responses that could have been provided. The video provides “TakeCARE” as an acronym for students to remember that an effective bystander is: C—Confident that they can help their friend avoid risky situations, A—Aware that their friends could get hurt in these kinds of situations, R—Responsible for helping, and E—Effective in how they help.
Control.
For the control condition, counselors gave a presentation on a topic of their choosing that was unrelated to relationship violence, sexual consent, or bystander behavior. Topics included adolescent wellbeing, bullying, and suicide prevention. Instructional methods included didactic presentation, videos, and worksheets. After follow-up data were collected from all classrooms, counselors were encouraged to re-show TakeCARE in the control classrooms, so that all students had the opportunity to view it.
Measures
Helpful bystander behavior.
At both assessments, students completed the 18-item Friends Protecting Friends Bystander Behavior Scale (FPF-BBS; Jouriles & McDonald, 2016), which draws heavily from the 45-item Bystander Behavior Scale for Friends (BBS-F; Banyard, et al., 2014). The 18 items of the FPF-BBS were selected for their relevance to high school students and to information presented in the TakeCARE video. For the first 12 items, students were asked to select the sentence that was “Most true for the past 3 months,” and that “partner,” includes boyfriends, girlfriends, or anyone that a person is attracted to. These items assessed bystander responses to discrete situations of relationship or sexual violence among friends (see Figure 1 for item content). Specifically, the FPF-BBS assessed whether or not the student engaged in helpful bystander behavior when encountering each of these situations, which is similar to the BBS-F. However, the FPF-BBS also distinguishes reasons for the absence of bystander behavior in each situation, by asking if the situation was not encountered, and if it was encountered but the student did not respond to it with a helpful bystander behavior. For example, for the item “saw a friend and their partner in a heated argument,” the response options were: “I did not see a friend and their partner in a heated argument” (did not encounter the situation); “I saw a friend and their partner in a heated argument, but there were some good reasons why I did not ask if everything was okay” (encountered the situation, but did not intervene); and “I saw a friend and their partner in a heated argument, and I asked if everything was okay” (encountered the situation and intervened).
Figure 1.
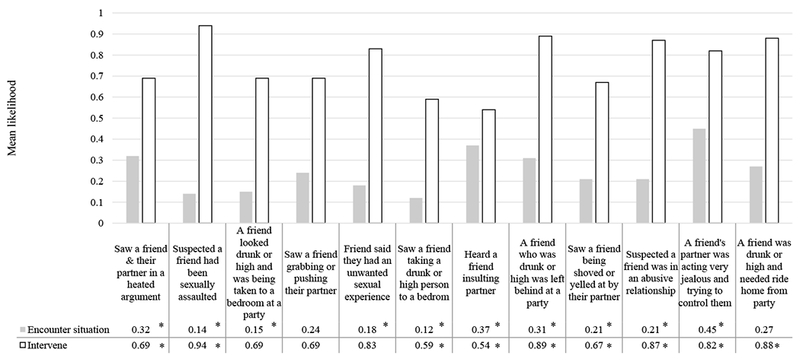
Mean likelihood of encountering and intervening in bystander situations in the 3 months prior to baseline. Likelihood of encountering is the % of students who encountered the situation. Likelihood of intervening is the % of students who encountered the situation and reported intervening in it. * Likelihood statistically differs from the average likelihood (23.2% for encountering the situation, and 78.2% for likelihood of intervening) across the 12 situations, using the Sidak correction for multiple comparisons. Since the number of students who reported encountering each situation varied, equal values for likelihood of encountering a given situation may not be equally statistically significant.
The remaining six items assessed proactive behavior and information gathering. Sample items include: “I talked with friends about going to parties together, staying together, and leaving together”, and “I tried to get more information about sexual abuse and/or relationship abuse and what I can do about it.”
Consistent with the conventional coding of the BBF-F and other commonly used measures of bystander behavior, helpful bystander was scored as: 0 - student did not intervene as a helpful bystander, regardless of whether the situation was encountered, or 1 - student encountered the situation and responded with helpful behavior. Scores on all 18 items were summed to derive a scale score. Thus, this scale reflected the count of the number of these situations in which the student intervened. The 921 students comprising the final sample, for the most part, completed all of the items on the BBF-F (99.7%). To be conservative, the few items that were not answered were counted as “0” (0 = student did not intervene as a helpful bystander). Coefficient alpha was .85 and .89 at baseline and follow-up, respectively. Consistent with theory and research on determinants of bystander behavior (Banyard et al., 2007; Jouriles et al., 2016), helpful bystander behavior and bystander self-efficacy (using a 5-item measure of bystander self-efficacy adapted from Banyard, Plante, & Moynihan, 2005) were correlated positively at baseline, r = .17, p < .001.
To examine bystander behavior in a way that accounts for the types of situations that students encountered, we computed a second measure of bystander behavior that included only the 12 situation items, and only those items the student reported encountering both at baseline and at follow-up. Responses across these situations (using the same 0/1 scale as described above) were summed to derive a score for situations reported to have been encountered at both assessments. This measure served as a more tightly controlled assessment of the change in a student’s behavior from baseline to follow-up.
Data Analysis
The outcome variable for our primary aim (helpful bystander behavior) followed a count distribution. Further, students were clustered within classrooms; thus, outcomes within classrooms might be correlated. Hence, to test our first hypothesis, we used Generalized Linear Mixed Models (GLMM) analyses, employing a log linking function and a Poisson distribution, clustering students within classrooms. We conducted the GLMM equivalent of an ANCOVA to evaluate TakeCARE’s effects on helpful bystander behavior. Specifically, treatment condition was a predictor of between-subjects differences; the dependent variable was helpful bystander behavior at follow-up, with helpful bystander behavior at baseline as the covariate. We used an ANCOVA-equivalent approach because it is not biased by regression to the mean and has less error than other approaches (e.g., analyses of change scores; Tabachnick & Fidell, 2013). Our model also included age, sex, and Hispanic ethnicity as additional covariates. Further, we included “counselors” as a dummy-coded predictor of helpful bystander behavior, in the event that counselor differences might have influenced outcomes. Additionally, we examined the TakeCARE × Counselor interaction effects in initial analyses to insure that the TakeCARE effects did not vary significantly by counselor: They did not, so the interactions were dropped and the analyses recomputed.
To address our second aim, we used GLMM to evaluate differences in the likelihood of encountering each of the 12 situations, and the likelihood of responding as a helpful bystander in those situations that were encountered. The scores for each individual were treated as 12 repeated measures nested within individuals, and the model was conducted using a binomial distribution with a logit link function. This model effectively performs the GLMM equivalent to a one-way repeated measures ANOVA (on dichotomous outcomes), with the 12 levels of the repeated measures being the 12 items. To determine the degree to which the mean likelihoods of encountering each situation varied across the 12 items, we compared the likelihood of encountering each item with the overall average likelihood of the 12 items, correcting for multiple comparison using the Sidak multiple comparisons test. We computed a similar analysis to determine the degree to which the mean likelihoods of intervening in each situation varied across the 12 items. Thus, two GLMM analyses were conducted: one for the likelihood of encountering each situation (0 = not encountered, 1 = encountered, whether they intervened or not), and one for the likelihood of intervening (0 = no, 1 = yes) if they had encountered it.
To address our third aim, to examine TakeCARE’s effects on helpful bystander behavior controlling for the situations actually encountered, we repeated the GLMM analysis used to address our primary aim, using our index of bystander behavior that included only the 12 situation items, and only those items the student reported encountering both at baseline and at follow-up. This essentially controls for variation in the situations each student experienced.
Results
Means and standard deviations for situations in which students engaged in helpful bystander behavior at baseline and follow-up for the TakeCARE and control conditions are presented in Table 1.
Table 1.
Means (standard deviations) for bystander behavior at baseline and follow-up for TakeCARE and control groups
| TakeCARE (n = 463) | Control (n = 458) | |||
|---|---|---|---|---|
| Variable | Baseline | Follow-up | Baseline | Follow-up |
| Helpful bystander behavior | 4.43 (4.16) | 4.81 (4.64) | 4.35 (3.71) | 4.25 (4.02) |
Note. Helpful bystander behavior scores ranged from 0 to 18. Higher scores reflect a larger number of situations in which students reported engaging in helpful bystander behavior.
TakeCARE effects on overall bystander behavior (aim 1)
The GLMM results indicated that students who viewed TakeCARE reported engaging in more helpful bystander behavior at follow-up than did students in the control condition, b = −.14, t(892) = 2.14, p = .032, d = .14. In addition, Hispanic students reported engaging in more helpful bystander behavior than non-Hispanic students, b = .18, t(892) = 2.51, p < .012, d = .17. Finally, helpful bystander behavior at baseline was highly predictive of helpful bystander behavior at follow-up, b = .12, t(892) = 14.79, p < .001, d = .99.
For descriptive purposes, we computed an additional GLMM analysis analogous to a repeated-measures ANCOVA (with condition, time [baseline/follow-up], and Condition × Time as the independent variables, and sex, age, and ethnicity as covariates), which showed that helpful bystander behavior increased from baseline to follow-up in the TakeCARE condition, b = .41, t(1793) = 2.14, p = .033, d = .10, but not in the control condition (see means in Table 1).
Helpful bystander behavior across the different potential bystander situations (aim 2)
Figure 1 presents likelihood estimates for each of the situations. As expected, the likelihood at baseline that a student had encountered each situation varied across the 12 situations, χ2 (11) = 330.9, p < .001. Those most likely to be encountered involved acts of psychological relationship aggression, such as a friend insulting or trying to control a partner, or a friend in a heated argument. Figure 2 presents percent of the total sample that reported encountering each situation at baseline and at the follow-up assessment.
Figure 2.
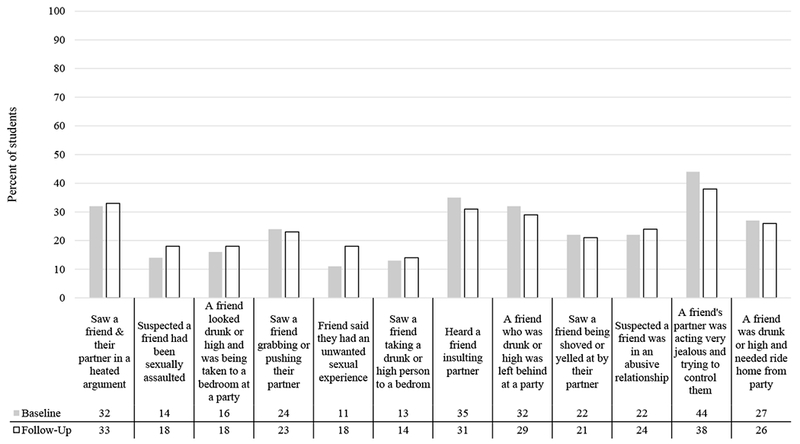
Percent of students who reported having encountered each situation at baseline and follow-up. N = 1,295 at baseline, N = 921 at follow-up.
The likelihood of responding to each encountered situation with helpful bystander behavior also varied considerably, χ2 (11) = 215.8, p < .001. The likelihood of helpful bystander behavior was greater than 50% for all situations encountered (range = 54% to 94%). However, some of the situations most likely to be encountered were those in which students were least likely to respond with helpful bystander behavior (e.g., friend insulting a partner). Helpful bystander behavior was most likely in situations that did not involve the presence of a designated “perpetrator”; examples include helping a friend after after a suspected sexual assault had already occurred or helping a friend who had been left behind at a party and/or needed a ride home.
TakeCARE effects on bystander behavior in situations encountered at both baseline and follow-up (aim 3)
These analyses included only those students who encountered the same situation(s) at both baseline and follow-up. Of the 921 students with data at both assessments, 411 reported encountering at least one situation both at baseline and at follow-up. Those who reported encountering at least one situation both at baseline and at follow-up (n = 411) did not differ from those who did not (n = 510) on any of the demographic variables (ps > .20). However, they did report encountering more bystander situations at baseline (M = 7.78 vs. M = 2.94), t(919) = 20.65, p < .001.
For situations encountered at both baseline and follow-up, students who viewed TakeCARE reported engaging in more helpful bystander behavior at follow-up, b = 10, t(396) = −2.38, p = .018, d = .24 (controlling for age, sex, and Hispanic ethnicity) than did those in the control condition. Hispanic students reported engaging in more helpful bystander behavior than non-Hispanic students, b = .26, t(396) = 4.73, p < .001, d = .48. In addition, helpful bystander behavior at baseline was positively associated with helpful bystander behavior at follow-up, b = .20, t(396) = 6.34, p < .001, d = .64.
We repeated this analysis controlling for the number of situations encountered at both assessments (in addition to age, sex, and Hispanic ethnicity), to investigate the effect of TakeCARE on one’s likelihood to intervene per situation encountered and to disentangle the likelihood of helpful bystander behavior with the likelihood of recognizing more situations as calling for bystander behavior (i.e., greater awareness of a given situation as risky). Again, students who viewed TakeCARE, compared to those in the control condition, reported more bystander behavior over the follow-up period, b = −.12, t(395) = −2.85, p = .005, d = .29. Since this analysis controlled for the number of potential bystander situations encountered at follow-up, it indicates that students in TakeCARE are more likely to intervene in a situation which they encounter. Also, Hispanic students reported engaging in helpful bystander behavior in more situations than non-Hispanic students, b = .24, t(395) = 4.50, p = .001, d = .45. Finally, both the number of situations in which helpful bystander behavior was reported at baseline, and the number of situations encountered at both baseline and follow-up, were positively related to helpful bystander behavior in those situations at follow-up, b = .10, t(395) = 5.25, p < .001, d = .53, and b = .10, t(395) = 5.66, p < .001, d = .57.
Exploratory analyses
It might be reasoned that the BBF-F can be scored to offer an indication of awareness of bystander behavior opportunities, by counting the number of bystander situations that students indicated they had encountered, regardless of whether or not they intervened. We thus conducted an exploratory analysis to examine whether viewing TakeCARE influenced the total number of bystander opportunities reported by performing the same GLMM used in aim 1, but with number of bystander opportunities as the dependent variable. Results indicated that students who viewed TakeCARE reported more bystander opportunities at follow-up than those in the control condition, M = 5.56 vs. 4.93, b = .14, t(395) = 2.28, p = .023, d = .23.
We followed this analysis by examining whether TakeCARE had an influence on the number of missed opportunities, or opportunities for bystander behavior in which no action was taken. We used the GLMM model from aim 1 with the dependent variable being the number of opportunities at follow-up in which the student did not intervene (and the baseline value for that variable as a covariate). Those who viewed TakeCARE did not report more missed opportunities in encountered bystander situations at follow-up than those in the control condition (p = .183).
Finally, we examined whether sex, Hispanic ethnicity, or age moderated the effect of TakeCARE on bystander behavior by adding the interaction between treatment condition and each one of these demographic variables to our aim 1 model. Each demographic variable was tested as a moderator in a separate analysis. There was no evidence that sex (p = .299), Hispanic ethnicity (p = .588), or age (p = .220) moderated the effects of TakeCARE on bystander behavior.
Discussion
Relationship violence and sexual assault are prevalent among teens, and bystander programs have been developed to help combat these problems. Yet research on bystander programs among high school students remains sparse. The present study demonstrated that TakeCARE, a video bystander program, increased helpful bystander behavior among high school students: Students who viewed TakeCARE reported engaging in helpful bystander behavior in more situations at the follow-up assessment than those in the control group. Moreover, these results emerged in a primarily Hispanic sample—a group known to be at greater risk than non-Hispanic youth for experiencing relationship violence (Kann et al., 2016)—and when the TakeCARE video was administered by school counselors, under naturalistic conditions, to students in an urban high school.
The magnitude of the documented effects of TakeCARE on helpful bystander behavior with high school students was in the small-to-medium range. These results are comparable to those from highly-controlled, college-student trials of TakeCARE (Kleinsasser et al., 2015; Jouriles et al., 2016). The demonstration of even a small effect of an easy-to-disseminate bystander program is important. To illustrate, the average number of situations in which helpful bystander behavior was reported by students at baseline was 4.39. In a high school of over 1,000 students, this translates to at least 4,390 helpful bystander behaviors over a 3-month period. The average difference in helpful bystander behavior between students who viewed TakeCARE and those in the control condition was 0.56 situations per student at follow-up, translating to an additional 560 helpful bystander behaviors over the follow-up period. Such an increase could make a considerable difference in reducing school victimization rates, and could help contribute to changing a school’s culture regarding tolerance of relationship violence.
It is noteworthy that Hispanic students were more likely to report engaging in helpful bystander behavior, which may speak to a broader Hispanic collectivistic culture that prizes shared responsibility and close relationships with fellow community members (Center for Disease Control and Prevention, 2013). This finding is also consistent with college bystander research suggesting that minority students engage in more helpful bystander behavior than Whites (Brown et al., 2014). It is also consistent with the notion that Hispanic youth may have more opportunities to engage in helpful bystander behavior to prevent relationship violence (Kann et al., 2016). That is, in the present sample, Hispanic youth may have been helping Hispanic youth who they perceived were at risk. Future research on bystander behavior should explore how race and ethnicity of the bystander, the perpetrator, and the victim might influence bystander behavior.
Exploratory analyses indicated that students were more likely to encounter certain types of situations than others; specifically, situations indicative of relationship violence were encountered more often than situations indicative of risk for sexual assault. Indeed, these results suggest that high school students frequently encounter situations in which a friend is experiencing psychological abuse from a partner; almost half the sample reported witnessing jealous or controlling behavior among partners at the baseline assessment. This is consistent with literature suggesting that this form of dating violence is particularly frequent and repetitive in adolescent dating relationships (Jouriles et al., 2009). Interestingly, our exploratory analyses also indicated that there was a lower than average likelihood of students reporting that they suspected a friend was in an abusive relationship. These two findings appear to be contradictory, but one interpretation of this pattern is that insults or jealous and controlling behavior are not labeled by students as “abusive,” but physical and sexual violence are. If so, this suggests a need to help educate students better about the nature and impact of psychological and verbal abuse.
Students were most likely to act as a helpful bystander after a risky circumstance had occurred, rather than to interrupt or prevent a risky situation in progress. To illustrate, 94% of students who reported suspecting that a friend had been sexually assaulted intervened by letting the friend know they were available to help, whereas only 54% of students who heard a friend insulting a partner reported that they said something to the friend to discourage such behavior. These different rates, however, can be interpreted many different ways. For example, this may suggest that students feel more comfortable helping friends who are victims of violence rather than confronting friends acting as potential perpetrators. Related to this point, students may be fearful of personal physical or social harm (e.g., damaged friendships) should they themselves intervene in an ongoing incident. They might also lack confidence in their ability to diffuse an ongoing situation, but have confidence that they can help a friend after the fact. Alternatively, with the specific example presented above, students might simply view some situations as more serious than others, with some calling for intervention and others not.
Results of our exploratory analyses suggest the need to consider the nature and context of risky situations when developing and evaluating effects of bystander programs. Because the risky situations assessed by the BBS-F are not equally likely to be encountered or intervened upon, it may be important to consider how to incrementally increase the likelihood of intervening in those situations that are more serious but for which students are less likely to respond helpfully. Helping students intervene in situations in which a clear perpetrator is present, in which a risky situation is in progress, or in which helpful bystander behavior may not be received as helpful may call for different approaches by bystander program developers.
The present research was not designed to evaluate the mechanisms by which TakeCARE increased bystander behavior, but our results suggest that TakeCARE may increase adolescents’ awareness of risky situations. Specifically, students who viewed TakeCARE reported encountering more risky situations at follow-up than those in the control condition, possibly suggesting a heightened awareness of risky situations among TakeCARE participants. However, it is not clear from this study if TakeCARE sensitizes students to notice risk, or results in them somehow being exposed to more high-risk situations. Examining awareness of bystander opportunity as a potential mediator of TakeCARE’s effects, along with other possible mediators such as self-efficacy and responsibility, is a possible area for future research.
There are several limitations to the current study. First, because of time restrictions in the collection of data in classrooms, we were limited to a single, self-report measure of bystander behavior. Self-report measures may be subject to reporter biases, including misremembering past events. Additionally, similar to other self-report measures of bystander behavior, ours did not yield information on the frequency, quality, or outcomes of bystander behavior. Assessing different dimensions of bystander behavior using multiple methods would help advance our understanding of the phenomenon, and convergence of findings across multiple methods would strengthen confidence in our findings. Second, although it is promising that a short video shows effects on bystander behavior for at least 3 months, a longer follow-up period is necessary to determine the duration of the program effects. Third, the real-world conditions of this study, while valuable in many ways, compromised the rigor of certain aspects of the evaluation. For example, the counselors did not collect follow-up data in 9 classrooms. It is noteworthy, however, that the differences between completers and non-completers were minimal and there were no observed counselor effects in our analyses. Fourth, the study was conducted in a single high school. It is possible that students who viewed TakeCARE talked about it with students in the control condition, potentially diminishing the magnitude of observed effects. In addition, it is not clear how generalizable the effects are to other high schools with different campus climates regarding bystander behavior and relationship violence.
Conclusion
This study extends previous research on TakeCARE by replicating its positive effects on helpful bystander behavior in a sample of primarily Hispanic high school students, under real-world conditions. The results are consistent with previous evaluations of TakeCARE with university students under highly controlled conditions (Kleinsasser et al., 2015; Jouriles et al., 2016), and provide further evidence that a short video about bystander intervention can be efficacious. This is especially encouraging in light of TakeCARE’s brevity and ease of dissemination, given that implementation barriers often prevent adolescents from being exposed to empirically-supported programs (Gottfredson & Gottfredson, 2002). Furthermore, the assessment of bystander behavior in this study sheds light on which risky situations of relationship violence adolescents are most likely to encounter and subsequently intervene. Research on the types of situations high school students face can be used to inform the development of stronger bystander prevention programs.
Acknowledgements
The authors would like to acknowledge Jennifer Reed, who helped coordinate data collection, assisted with data cleaning, and was integral to working with the high school at which the study took place.
Funding
This research was supported by a grant from the National Institutes of Health R21 HD075585. The content of this manuscript is solely the responsibility of the authors and does not represent the official views of the sponsor.
Biography
Kelli S. Sargent is a Clinical Psychology doctoral student in the Department of Psychology at Southern Methodist University. Her research focuses on intervention evaluation, specifically targeting violence prevention among adolescents and young adults. Her research interests also include adolescent risk factors that render teens more susceptible to negative consequences of violence and adverse experiences.
Ernest N. Jouriles is a Dedman Family Distinguished Professor in the Department of Psychology at Southern Methodist University. His research spans two overlapping programs: violence in adolescent romantic relationships and development of intervention programs to prevent such violence, and children’s exposure to interparental conflict and violence.
David Rosenfield is an Associate Professor in the Department of Psychology at Southern Methodist University. His research focuses on the application of recent advances in statistical methods to psychological research, with an emphasis on applying hierarchical linear modeling and structural equation modeling to longitudinal data analyses.
Renee McDonald is an Associate Dean for Research and Academic Affairs in the Dedman College of Humanities and Sciences at Southern Methodist University. Her research examines how child adjustment problems are associated with exposure to family conflict and violence, with particular attention to developing and disseminating effective interventions. Her research has also focused on prevention of sexual assault and racist behaviors, and reduction of risk for sexual assault victimization among high school and college students.
Footnotes
Conflicts of Interest
The authors report no conflicts of interest.
Compliance with Ethical Standards
Ethical Approval
This research was approved by the Southern Methodist University Institutional Review Board and the Dallas Independent School District Research Review Board.
Informed Consent
All participants provided informed consent for participation in this study.
References
- Banyard VL, & Cross C (2008). Consequences of teen dating violence understanding intervening variables in ecological context. Violence Against Women, 14, 998–1013. doi: 10.1177/1077801208322058 [DOI] [PubMed] [Google Scholar]
- Banyard VL, Moynihan MM, Cares AC, & Warner R (2014). How do we know if it works? Measuring outcomes in bystander-focused abuse prevention on campuses. Psychology of Violence, 4, 101–115. doi: 10.1037/a0033470 [DOI] [Google Scholar]
- Banyard VL, Moynihan MM, & Plante EG (2007). Sexual violence prevention through bystander education: An experimental evaluation. Journal of Community Psychology, 35, 463–481. doi: 10.1002/jcop.20159 [DOI] [Google Scholar]
- Banyard VL, Plante EG, & Moynihan MM (2005). Rape prevention through bystander education: Final report to NIJ for grant 2002-WG-BX-0009.Durham: University of New Hampshire. [Google Scholar]
- Brown AL, Banyard VL, & Moynihan MM (2014). College students as helpful bystanders against sexual violence gender, race, and year in college moderate the impact of perceived peer norms. Psychology of women quarterly, 38, 350–362. doi: 10.1177/0361684314526855 [DOI] [Google Scholar]
- Center for Disease Control and Prevention (2013). Our understanding: Culture insights communicating with Hispanic/Latinos. Retrieved from http://www.cdc.gov/nccdphp/dch/programs/healthycommunitiesprogram/tools/pdf/hispanic_latinos_insight.pdf
- Cook-Craig PG, Coker AL, Clear ER, Garcia LS, Bush HM, Brancato CJ, … & Fisher BS (2014). Challenge and opportunity in evaluating a diffusion-based active bystanding prevention program green dot in high schools. Violence Against Women, 20, 1179–1202. doi: 10.1177/1077801214551288 [DOI] [PubMed] [Google Scholar]
- Exner-Cortens D, Eckenrode J, & Rothman E (2013). Longitudinal associations between teen dating violence victimization and adverse health outcomes. Pediatrics, 131, 71–78. doi: 10.1542/peds.2012-1029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foshee VA, Reyes HLM, Gottfredson NC, Chang LY, & Ennett ST (2013). A longitudinal examination of psychological, behavioral, academic, and relationship consequences of dating abuse victimization among a primarily rural sample of adolescents. Journal of Adolescent Health, 53, 723–729. doi: 10.1016/j.jadohealth.2013.06.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gardner M, & Steinberg L (2005). Peer influence on risk taking, risk preference, and risky decision making in adolescence and adulthood: An experimental study. Developmental Psychology, 41, 625–635. doi: 10.1037/0012-1649.41.4.625 [DOI] [PubMed] [Google Scholar]
- Gottfredson DC, & Gottfredson GD (2002). Quality of school-based prevention programs: Results from a national survey. Journal of Research in Crime and Delinquency, 39, 3–35. doi: 10.1177/002242780203900101 [DOI] [Google Scholar]
- Jouriles EN, Garrido E, Rosenfield D, & McDonald R (2009). Experiences of psychological and physical aggression in adolescent romantic relationships: Links to psychological distress. Child Abuse & Neglect, 33, 451–460. doi: 10.1016/j.chiabu.2008.11.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jouriles EN, McDonald R, Rosenfield D, Levy N, Sargent K, Caiozzo C, & Grych JH (2016). TakeCARE, a video bystander program to help prevent sexual violence on college campuses: Results of two randomized, controlled trials. Psychology of Violence, 6, 410–420. 10.1037/vio0000016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jouriles EN, & McDonald R (2016). Friends Protecting Friends Bystander Behavior Scale. Unpublished measure . [Google Scholar]
- Jouriles EN, Rosenfield D, Yule K, Sargent KS, & McDonald R (2016). Predicting high-school students’ bystander behavior in simulated dating violence situations. Journal of Adolescent Health, 58, 345–351. doi: 10.1016/j.jadohealth.2015.11.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kann L, McManus T, Harris WA, Shanklin SL, Flint KA, Hawkin J, … & Zaza S. (2016). Youth risk behavior surveillance—United States. MMWR Surveillance Summary, 65, 1–174. [DOI] [PubMed] [Google Scholar]
- Katz J, Heisterkamp HA, & Fleming WM (2011). The social justice roots of the mentors in violence prevention model and its application in a high school setting. Violence Against Women, 17, 684–702. doi: 10.1177/107780121140972 [DOI] [PubMed] [Google Scholar]
- Kleinsasser A, Jouriles EN, McDonald R, & Rosenfield D (2015). An online bystander intervention program for the prevention of sexual violence. Psychology of Violence, 5, 227–235. doi: 10.1037/a0037393 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMahon S and Banyard V (2012) When can I help? A conceptual framework for the prevention of sexual violence through bystander intervention. Trauma, Violence and Abuse, 13, 3–14. [DOI] [PubMed] [Google Scholar]
- Miller E, Tancredi DJ, McCauley HL, Decker MR, Virata MCD, Anderson HA, … & Silverman JG (2013). One-year follow-up of a coach-delivered dating violence prevention program: a cluster randomized controlled trial. American Journal of Preventive Medicine, 45, 108–112. doi: 10.1016/j.amepre.2013.03.007 [DOI] [PubMed] [Google Scholar]
- Nahapetyan L, Orpinas P, Song X, & Holland K (2014). Longitudinal association of suicidal ideation and physical dating violence among high school students. Journal of Youth and Adolescence, 43, 629–640. [DOI] [PubMed] [Google Scholar]
- Steinberg L, & Monahan KC (2007). Age differences in resistance to peer influence. Developmental Psychology, 43, 1531–1543. doi: 10.1037/0012-1649.43.6.1531 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tabachnick BG, & Fidell LS (2013). Using Multivariate Statistics. (6th ed.) Upper Saddle River, NJ: Pearson. [Google Scholar]
- Taylor BG, & Mumford EA (2014). A national descriptive portrait of adolescent relationship abuse: Results from the National Survey on Teen Relationships and Intimate Violence. Journal of Interpersonal Violence, 31, 963–988. doi: 10.1177/0886260514564070 [DOI] [PubMed] [Google Scholar]
- Weisz JR, Ng MY, & Bearman SK (2014). Odd couple? Reenvisioning the relation between science and practice in the dissemination-implementation era. Clinical Psychological Science, 2, 58–74. doi: 10.1177/2167702613501307 [DOI] [Google Scholar]
- Young AM, Grey M, & Boyd CJ (2008). Adolescents’ experiences of sexua assault by peers: Prevalence and nature of victimization occuring within and outside of school. Journal of Youth and Adolescence, 38, 1072–1083. doi: 10.1007/s10964-008-9363-y [DOI] [PubMed] [Google Scholar]