

Abstract
Obstructive sleep apnoea (OSA) is a significant health issue. Patients with cardiovascular disease as well as patients with diabetes have a high prevalence of OSA, and the prevalence of coronary heart disease, heart failure, stroke and diabetes is increased in patients with obstructive sleep apnoea. Physiological responses to OSA include sympathetic activation, neurohumoral changes and inflammation, all of which are precursors for cardiovascular disease and diabetes. International guidelines are starting to recognise the importance of OSA for patients with cardiovascular conditions such as heart failure and hypertension. Diagnosis is important, and home-based sleep testing devices can facilitate this process. Treating OSA with continuous positive airway pressure (CPAP) has been shown to reduce blood pressure (BP) in patients with hypertension, but more research is needed to determine which components of the metabolic syndrome respond best to the addition of CPAP therapy.
Keywords: Obstructive sleep apnoea (OSA), sleep-disordered breathing (SDB), metabolic syndrome, diabetes, cardiovascular disease, heart failure, hypertension, coronary artery disease, obesity, continuous positive airway pressure (CPAP), screening
Introduction
The first major epidemiological study reporting the prevalence of obstructive sleep apnoea syndrome (OSAS), which is the presence of obstructive sleep apnoea (OSA) in combination with excessive sleepiness, was published by Young et al in 1993.1 OSA was documented in 2 % of middle-aged women and 4 % of middle-aged men. Later studies showed that OSA was even more common in the general population, with an overall prevalence of more than 20 % in men and 10 % in women, half of whom have moderate to severe sleep-disordered breathing.2 In 2000, four studies were published that demonstrated associations between OSA and hypertension.3–6 These were the first well-designed analyses conducted in large patient populations which showed the significant negative health effects of obstructive sleep apnoea. Since then, evidence for connections between OSA and numerous comorbidities has continued to grow. Interestingly, the presence of SDB in other cardiovascular diseases was found to be even higher than that in the general population for those aged 30–80 years.7
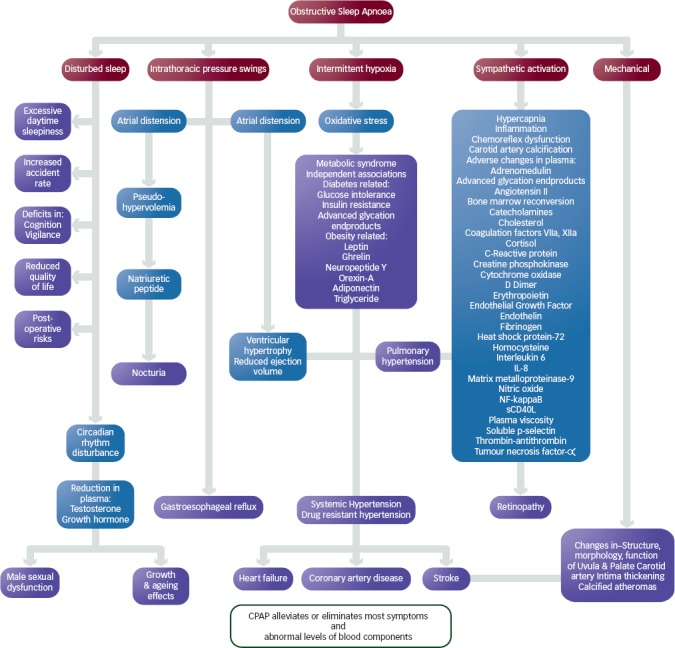
The medical consequences of OSA are currently attributed to complex interactions between five different factors – disturbed sleep, intrathoracic pressure swings, intermittent hypoxia, sympathetic activation and the mechanical consequences of snoring, resulting in a range of symptoms (see Figure 1).
Figure 1: Medical Consequences of Obstructive Sleep Apnoea [CBS ResMed, 2006].
Much research has been done on OSA in relation to car-accidents, and road, rail and air transport. It is well documented that timely and effective OSA treatment reduces motor vehicle crash risk.8 For this, and a wide variety of other reasons, sleep apnoea is widely considered to be a serious public health concern.9
In the last decade, treatment for OSA began to be considered to have potential beneficial cardiovascular effects, in addition to relief of daytime sleepiness. Research shows an increased prevalence of coronary heart disease, heart failure, stroke and diabetes in patients with an apnoea-hypopnoea index (AHI) of five or more per hour.10–14
Weight loss, upper airway surgery and, in severe cases, tracheotomy were the only available treatments for OSA until the 1980s. Collin Sullivan and his team invented continuous positive airway pressure (CPAP) as a noninvasive treatment approach. Since then numerous studies have documented the positive effects of positive airway pressure (PAP). Peer-reviewed literature demonstrates that PAP can effectively treat, and avoid further deterioration of, most of the secondary consequences of SDB.15–21 This has led to clinical acceptance of CPAP treatment as the optimal therapeutic strategy for OSA. Current CPAP devices are simple, straightforward and easy to use with a range of masks, allowing OSA treatment to be customised for each individual patient. Long-term compliance rates of at least 70 % after five years can be achieved.22 Age and gender also contribute to adherence with CPAP therapy.23
In this article we review associations between OSA and several components of the metabolic syndrome (MetS) and discuss what can be done to effectively screen and treat patients, especially those in the high-risk subgroup. Reliable screening studies at all care levels of chronic disease, complemented and justified by consistent clinical findings, need to be seriously considered by all involved in the management of the MetS, particularly in the context of spiralling health care costs and limited availability of overnight sleep-study resources. In fact, CPAP has been shown to be a cost effective strategy for management of OSA over a minimum treatment period of two years.24
Obstructive Sleep Apnoea and the Metabolic Syndrome (MetS)
Symptoms of OSA include the direct effects of sleep fragmentation – such as sleepiness, poor concentration and depressed mood – cognitive dysfunction, impaired work performance and decreased health-related quality of life, plus a number of other less-specific complaints including erectile dysfunction, nocturia, fatigue and headache.25 Women predominantly report insomnia, morning headaches and depression. It is important to recognise that subjective symptoms can be absent in a large proportion of patients.1
The physiological responses to recurrent respiratory events often leading to episodes of intermittent hypoxaemia are sleep fragmentation, sympathetic activation, neurohumoral changes and inflammation, which are precursors for cardiovascular disease and diabetes. Obesity has been consistently identified as a major risk factor for OSA,26 but there is growing evidence of increased morbidity and mortality in OSA independent of obesity.27-30 The strongest data regarding associations between components of MetS and OSA are for hypertension. Cardiovascular outcomes, glucose metabolism and the long-term complications of diabetes have been widely studied but results are inconclusive, most likely because of confounding factors and heterogeneity of the studied populations.31
The severity of OSA is defined by the AHI. In adults an AHI of 5–15 per hour is categorised as mild OSA, with an AHI of 15–30 or >30 defined as moderate or severe OSA, respectively. Consistent evidence indicates that the risk and occurrence of components of MetS increases in parallel with increasing apnoea-hypopnoea index.32 A large epidemiological study in 529 subjects with similar anthropomorphic and sleep characteristics, 51.2 % of whom had MetS, showed progressive metabolic impairment with increasing AHI severity. The most common combination of MetS indicators included increased waist circumference, hypertension and abnormal fasting glucose. There are unadjusted linear relationships between AHI and arterial oxygen saturation (SaO2) and each component of MetS. However, after adjustment for age, body mass index (BMI), smoking and sex, the only persistent significant relationships were for systolic and diastolic blood pressure. The authors of this study concluded that MetS occurs in about half of OSA patients, irrespective of daytime sleepiness.32
Data on the prevalence of OSA in patients with metabolic impairments are variable and difficult to compare. In a coronary artery disease population, accumulating MetS components like impaired glucose tolerance (IGT) and obesity, plus atrial fibrillation, increase the prevalence of sleep disordered breathing (SDB) dramatically.33
Obstructive Sleep Apnoea, Obesity and Insulin Resistance
Central obesity leads to insulin resistance34 and is a confounding factor in assessing the independent role of OSA in metabolic syndrome. Cross-sectional studies, however, provide a growing body of evidence for a positive and independent association between OSA and both insulin resistance/glucose intolerance and diabetes.35-38 OSA causes surges in sympathetic overactivity during apnoeic events leading to increased sympathetic tone during the day, as has been shown by muscle sympathetic nerve activity and catecholamine output.39-42 (see Figure 1). This affects other metabolic factors, including the renin-angiotensin system, insulin and adiponectin, which may all contribute to insulin resistance.39-44 OSA causes systemic inflammation, primarily due to the effects of intermittent hypoxia and oxidative stress,45 including activation of inflammatory cells and increased levels of pro-inflammatory biomarkers.46-51 Alterations can also be seen in cortisol secretion patterns, and changes in the duration and quality of sleep affect neuroendocrine and metabolic function. In addition to intermittent hypoxia, sleep fragmentation and loss of quality sleep also augment these effects. Healthy subjects exposed to sleep restriction in a laboratory setting show upregulation of the somatotrophic and hypothalamic-pituitary-adrenal axes.52,53 Short sleep duration has been associated with higher ghrelin and lower leptin levels.54 The evidence relating OSA, obesity and type 2 diabetes was strong enough to convince the International Diabetes Foundation to publish a consensus statement in 2008 outlining the need to screen for OSA in the diabetes clinic.55
Obstructive Sleep Apnoea and Cardiovascular Risk
In 2005 a collaborative network was established as part of the EU Cooperation around Cost and Technology (COST) B26 programme, with the aim of investigating the public health burden of OSA on the EU community and to assess the role of OSA in cardiovascular disease. Sixteen countries and 22 sleep centres participated in a cross-sectional study, enrolling a total of 5103 participants (3677 males). Mean age was 51.8 years and mean BMI 31.1 kg/m2. Median daytime sleepiness was moderate (Epworth Sleepiness Scale [ESS] score 10.8). Sleep apnoea was diagnosed in 79.4 % of patients with mean severity being higher in men (AHI 27.4) compared with women (AHI 18.3). Twenty-eight percent of patients had severe sleep apnoea (AHI >30), the majority of these were men. Cardiovascular comorbidity was frequent at 49.1 % and included systemic hypertension, ischaemic heart disease and, to a lesser extent, cerebrovascular disease. Other MetS components included hyperlipidaemia and diabetes. Despite the methodological limitations of this study with multiple centres and countries, it confirms that OSA is more severe in males but there is no difference between the genders in measures of sleepiness, as well as showing an increased prevalence of cardiovascular and metabolic disease with increasing apnoea-hypopnoea index.9
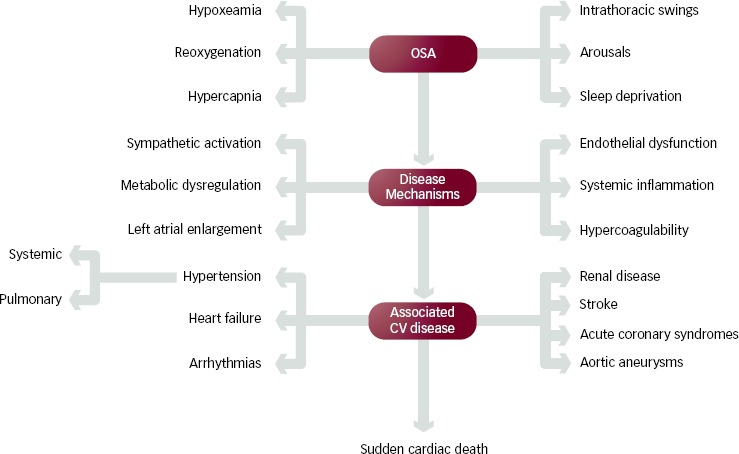
Figure 2 shows a number of the researched mechanisms of action of the association between OSA and cardiovascular risk, including central and reflex neural mechanisms, increased cardiovascular variability and changes in autonomic cardiovascular regulation mechanisms of ventilation (acute physiological effects of negative intrathoracic pressure), the renin-angiotensin-aldosterone system, endothelial dysfunction, inflammation and metabolic factors.56
Figure 2: Mechanisms that Promote Cardiovascular Disease [SOMERS, 2008].
After adjustment for confounding factors, the risk of new-onset hypertension was significantly reduced in OSA patients who adhered to CPAP therapy compared with those who were not treated with CPAP therapy or who were noncompliant with continuous positive airway pressure.57
During CPAP treatment in randomised controlled trials, mean arterial blood pressure could be reduced by 2.5 to 10 mmHg.16,58-64 In these trials there appeared to be a relationship between OSA and blood pressure, with greater reductions in those with more severe obstructive sleep apnoea.62
In 2010, a joint recommendation from the European Cost Action B26, the European Society of Hypertension and the European Respiratory Society was published after review of the evidence available on the interaction between OSA and arterial hypertension. This summarises the current state-of-the-art in epidemiology, diagnostic procedures and treatment options for the appropriate management of OSA in patients with hypertension as well as the treatment of hypertension in those with obstructive sleep apnoea.56,57,65,66
Obstructive Sleep Apnoea and Cancer
OSA has also been linked with cancer in the first study to investigate this association.67 The severity of OSA was independently correlated with an increased risk of incidence cancer, with hypoxia being the most likely pathologic link. However, the association appeared to be limited to males aged <65 years.67 Additional studies are required in this area to verify these potentially important findings and to investigate the potential role or influence of CPAP therapy.
Screening and Diagnosis of Obstructive Sleep Apnoea in Metabolic Syndrome Patients
When patients present with classical symptoms such as witnessed apnoeas, heavy snoring or daytime sleepiness there should be no delay in screening for OSA. Different questionnaires are used for identifying patients who need further OSA evaluation. The Berlin Questionnaire was specifically designed for the identification of patients in the general population likely to have OSAS,68 but while it is useful in the general population, it has not been shown to be useful in the presence of cardiovascular disease. The Epworth Sleepines Scale (ESS) is intended to measure daytime sleepiness.69
Alternative approaches to OSA diagnosis are being developed in the form of portable monitors. Home sleep testing devices facilitate evaluation for a definitive diagnosis. A recent review of published articles discussed the performance of ApneaLinkTM (see Figure 3) compared with polysomnography (PSG).70 ApneaLinkTM showed high diagnostic accuracy at AHI cut-off values of 10 (pooled sensitivity 93.3 %, specificity 90.7 %) and 15 (pooled sensitivity 91.4 %, specificity 93.8 %).
Figure 3: Details of ApneaLink Plus™ Device.
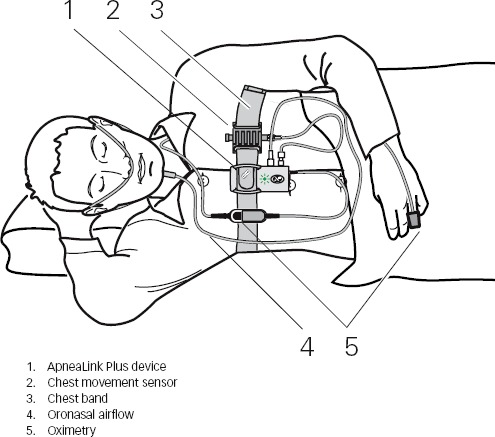
ApneaLink Plus is a 5-channel screening device for sleep apnoea detection based on pressure-transduced measurement of oronasal airflow, oximetry and a chest movement sensor. It summarises findings as apnoea-hypopnoea index per hour of recorded time.
Until relatively recently, the standard approach to OSA diagnosis was in-laboratory, technician-attended polysomnography (PSG), which monitors sleep, respiration, cardiac rhythm, snoring, limb movements and body position.71 Polysomnography, however, is labour-intensive, time-consuming and limited in its availability. This is why many countries have already changed their practice to home-based sleep testing to reduce the number of patients with OSA who go undiagnosed.72
Continuous Positive Airway Pressure Treatment
Continuous Positive Airway Pressure alleviates OSA and therefore reduces nocturia, and improves sleep quality, cognitive function, depression and quality of life.73,74 Improvements have also been shown in erectile dysfunction.75 Continuous Positive Airway Pressure reduces sympathetic drive in OSA patients and thus lowers blood pressure during sleep.76 The effect this has on daytime blood pressure is variable. Three meta-analyses looking at the effect of CPAP on blood pressure in OSA showed an average 24-hour reduction in mean arterial pressure of 2 mmHg.58,59,62 The effects varied from no decrease up to a reduction of 10 mmHg.16,17 Different inclusion criteria, particularly with respect to the severity of sleep apnoea, the inclusion of normotensive patients and the presence of symptoms of daytime sleepiness, are probably the reasons for the large differences in results between studies. The biggest effects have been shown in patients with resistant hypertension. In this cohort, OSA prevalence can be as high as 80 %.77,78 Interestingly, a recent study showed improvements in sleep apnoea severity after renal sympathetic nerve ablation for resistant hypertension.79
Two randomised trials evaluating the effect of CPAP therapy in patients with OSA and heart failure (HF) showed significant improvements in left ventricular ejection fraction (LVEF) after one and three months.19,20 In addition, improvements in quality of life and reduced sympathetic activity were documented. The existing data on OSA in CVD have led to a recommendation in the 2008 HF guidelines stating that OSA should be screened for and, if present, be treated with CPAP in patients with HF.80
Treatment of OSA with CPAP can alleviate nocturnal myocardial ischaemia.81 The benefit of CPAP therapy for other metabolic syndrome components appears to be variable, with some studies showing an immediate beneficial treatment effect, persisting over three to six months, and others showing no difference.78 Factors contributing to variability in the benefits of CPAP treatment benefit may be the severity of OSA, obesity and lipid abnormalities, small study populations and lack of rigour in controlled trials. More research needs to be done on which patient subgroups exhibiting one or more components of MetS will benefit from CPAP treatment.31
Compliance is crucial for any therapy to be successful, and early compliance with CPAP therapy is the most important factor. In addition, pre-treatment with drugs may play an important role.17,82 Current technological improvements in devices and masks (see Figure 4) can ensure compliance rates of >80 %.83
Figure 4: Use of Continuous Positive Airway Pressure Therapy at Home.

Conclusion
The complex links between OSA and MetS warrant further investigation. However, enough evidence already exists to recommend that greater attention be paid to the identification and treatment of OSA in MetS patients to reduce cardiovascular risk, improve quality of life, reduce cardiovascular morbidity and mortality, and decrease the number of OSA-related transport and work accidents; all of which will have beneficial health economic effects. Efficient networks and referral pathways between MetS and sleep health care professionals are a crucial component in testing and establishing routine interventions that are appropriate for both conditions.
Acknowledgments
Nicola Ryan provided English language and medical writing support funded by ResMed.
Funding Statement
Support: The publication of this article was funded by ResMed. The views and opinions expressed are those of the authors and not necessarily those of ResMed.
References
- 1.Young T, Palta M, Dempsey J et al. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230–5. doi: 10.1056/NEJM199304293281704. [DOI] [PubMed] [Google Scholar]
- 2.Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165(9):1217–39. doi: 10.1164/rccm.2109080. [DOI] [PubMed] [Google Scholar]
- 3.Young T, Finn L, Peppard PE et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep. 2008;31:1071–8. [PMC free article] [PubMed] [Google Scholar]
- 4.Peppard P, Young T, Palta M et al. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378–84. doi: 10.1056/NEJM200005113421901. [DOI] [PubMed] [Google Scholar]
- 5.Nieto FJ, Young TB, Lind BK et al. Association of sleep-disordered breathing sleep apnea and hypertension in a large community-based study, Sleep Heart Health Study. JAMA. 2000;283(14):1829–36. doi: 10.1001/jama.283.14.1829. [DOI] [PubMed] [Google Scholar]
- 6.Lavie P, Herer P, Hoffstein V. Obstructive sleep apnoea syndrome as a risk factor for hypertension: population study. Br Med J. 2000;320(7233):479–82. doi: 10.1136/bmj.320.7233.479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Somers VK, White DP, Amin R et al. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing. J Am Coll Cardiol. 2008;52(8):686–17. doi: 10.1016/j.jacc.2008.05.002. [DOI] [PubMed] [Google Scholar]
- 8.Tregear S, Reston J, Schoelles K et al. Continuous positive airway pressure reduces risk of motor vehicle crash among drivers with obstructive sleep apnea. Sleep. 2010;33(10):1373–1380. doi: 10.1093/sleep/33.10.1373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hedner J, Grote L, Bonsignore M et al. The European Sleep Database (ESDA) – report from 22 European Laboratories. Eur Resp J. 2011;38(3):635–642. doi: 10.1183/09031936.00046710. [DOI] [PubMed] [Google Scholar]
- 10.Barone MTU, Menna-Barreto L. Diabetes and sleep: A complex cause-and-effect relationship. Diabetes Research and Clinical Practice. 2010;91:129–37. doi: 10.1016/j.diabres.2010.07.011. [DOI] [PubMed] [Google Scholar]
- 11.Priou P, Le Vaillant M, Meslier N et al. Independent association between obstructive sleep apnea severity of glycated haemoglobin in adults without diabetes. Diabetes Care. 2012;35:1902–6. doi: 10.2337/dc11-2538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Andreas S, Schulz R, Werner GS et al. Prevalence of obstructive sleep apnoea in patients with coronary artery disease. Coron Artery Dis. 1996;7(7):541–5. [PubMed] [Google Scholar]
- 13.Mooe T, Rabben T, Wiklund U et al. Sleep-disordered breathing in men with coronary artery disease. Chest. 1996;109(3):659–663. doi: 10.1378/chest.109.3.659. [DOI] [PubMed] [Google Scholar]
- 14.Shahar E, Whitney CW, Redline S, Lee ET. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J Respir Crit Care Med. 2001;163(1):19–25. doi: 10.1164/ajrccm.163.1.2001008. [DOI] [PubMed] [Google Scholar]
- 15.Buchner NJ, Sanner BM, Borgel J et al. Continuous positive airway pressure treatment of mild to moderate obstructive sleep apnea reduces cardiovascular risk. Am J Respir Crit Care Med. 2007;176(12):1274–80. doi: 10.1164/rccm.200611-1588OC. [DOI] [PubMed] [Google Scholar]
- 16.Becker HF, Jerrentrup A, Ploch T et al. Effect of nasal continuous positive airway pressure treatment on blood pressure in patients with obstructive sleep apnea. Circulation. 2003;107(1):68–73. doi: 10.1161/01.cir.0000042706.47107.7a. [DOI] [PubMed] [Google Scholar]
- 17.Pepin JL, Tamisier R, Barone-Rochette G et al. Comparison of continuous positive airway pressure and valsartan in hypertensive patients with sleep apnea. Am J Respir Crit Care Med. 2010;182(7):954–60. doi: 10.1164/rccm.200912-1803OC. [DOI] [PubMed] [Google Scholar]
- 18.Middleton S, Vermeulen W, Byth K et al. Treatment of obstructive sleep apnoea in Samoa progressively reduces daytime blood pressure over 6 months. Respirology. 2009;14(3):404–410. doi: 10.1111/j.1440-1843.2009.01510.x. [DOI] [PubMed] [Google Scholar]
- 19.Mansfield DR, Gollogly NC, Kaye DM et al. Controlled trial of continuous positive airway pressure in obstructive sleep apnea and heart failure. Am J Respir Crit Care Med. 2004;169(3):361–6. doi: 10.1164/rccm.200306-752OC. [DOI] [PubMed] [Google Scholar]
- 20.Kaneko Y, Floras JS, Usui K et al. Cardiovascular effects of continuous positive airway pressure in patients with heart failure and obstructive sleep apnea. N Engl J Med. 2003;348(13):1233–41. doi: 10.1056/NEJMoa022479. [DOI] [PubMed] [Google Scholar]
- 21.Shahin SP, Nechanitzky T, Dittel C et al. Long term improvement of insulin sensitivity during CPAP therapy in the obstructive sleep apnoea syndrome. Med Sci Monit. 2008;14(3):117–21. [PubMed] [Google Scholar]
- 22.McArdle N, Devereux G, Heidarnejad H. Long-term use of CPAP therapy for sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med. 1999;159(4 Pt 1):1108–114. doi: 10.1164/ajrccm.159.4.9807111. [DOI] [PubMed] [Google Scholar]
- 23.Woehrle H, Graml A, Weinreich G. Age-and gender-dependent adherence with continuous positive airway pressure therapy. Sleep Med. 2011;12(10):1034–6. doi: 10.1016/j.sleep.2011.05.008. [DOI] [PubMed] [Google Scholar]
- 24.Guest JF, Helter MT, Morga A et al. Cost-effectiveness of using continuous positive airway pressure in the treatment of severe obstructive sleep apnoea/hypopnoea syndrome in the UK. Thorax. 2008;63:860–5. doi: 10.1136/thx.2007.086454. [DOI] [PubMed] [Google Scholar]
- 25.American Academy of Sleep Medicine Task Force. Sleeprelated breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. Sleep. 1999;22:667–689. [PubMed] [Google Scholar]
- 26.Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):136–143. doi: 10.1513/pats.200709-155MG. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Marin JM, Carrizo SJ, Vicente E et al. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–53. doi: 10.1016/S0140-6736(05)71141-7. [DOI] [PubMed] [Google Scholar]
- 28.McNicholas WT, Bonsignore MR. Sleep apnoea as an independent risk for cardiovascular disease: current evidence, basic mechanisms and research priorities. Eur Respir J. 2007;29(1):158–78. doi: 10.1183/09031936.00027406. [DOI] [PubMed] [Google Scholar]
- 29.Peker Y, Carlson J, Hedner J. Increased incidence of coronary artery disease in sleep apnoea: a long-term follow-up. Eur Respir J. 2006;28(3):596–602. doi: 10.1183/09031936.06.00107805. [DOI] [PubMed] [Google Scholar]
- 30.Wilcox I, McNamara SG, Collins FL et al. “Syndrome Z”: the interaction of sleep apnoea vascular risk factors and heart disease. Thorax. 1998;53(Suppl 3):S25–8. [PMC free article] [PubMed] [Google Scholar]
- 31.Pepin JL, Tamisier R, Levy P. Obstructive sleep apnoea and metabolic syndrome: put CPAP efficacy in a more realistic perspective. Thorax. 2012;67(12):1025–7. doi: 10.1136/thoraxjnl-2012-202807. [DOI] [PubMed] [Google Scholar]
- 32.Bonsignore MR, Esquinas C, Barcelo A et al. Metabolic Syndrome, insulin resistance and sleepiness in real-life obstructive sleep apnoea. Eur Respir J. 2012;39:1136–43. doi: 10.1183/09031936.00151110. [DOI] [PubMed] [Google Scholar]
- 33.Prinz C, Bitter T, Piper C et al. Sleep apnea is common in patients with coronary artery disease. Wien Med Wochenschr. 2010;160:349–355. doi: 10.1007/s10354-009-0737-x. [DOI] [PubMed] [Google Scholar]
- 34.Bjontorp P. Metabolic implications of body fat distribution. Diabetes Care. 1991;14(12):1132–43. doi: 10.2337/diacare.14.12.1132. [DOI] [PubMed] [Google Scholar]
- 35.Ip MS, Lam B, Ng MM et al. Obstructive sleep apnea is independently associated with insulin resistance. Am J Respir Crit Care Med. 2002;165(5):670–6. doi: 10.1164/ajrccm.165.5.2103001. [DOI] [PubMed] [Google Scholar]
- 36.Punjabi NM, Shahar E, Redline S et al. Sleep-disordered breathing glucose intolerance, and insulin resistance: The Sleep Heart Health Study. Am J Epidemiol. 2004;160:521–30. doi: 10.1093/aje/kwh261. [DOI] [PubMed] [Google Scholar]
- 37.Reichmuth KJ, Austin D, Skatrud JB et al. Association of sleep apnea and Type II diabetes: a population-based study. Am J Respir Crit Care Med. 2005;172(12):1590–5. doi: 10.1164/rccm.200504-637OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Tasali E, Ip MS. Obstructive sleep apnea and metabolic syndrome: alterations in glucose metabolism and inflammation. Proc Am Thorac Soc. 2008;5(2):207–17. doi: 10.1513/pats.200708-139MG. [DOI] [PubMed] [Google Scholar]
- 39.Dopp JM, Reichmuth KJ, Morgan BJ. Obstructive sleep apnea and hypertension; mechanisms, evaluation, and management. Curr Hypertens Rep. 2007;9(6):529–34. doi: 10.1007/s11906-007-0095-2. [DOI] [PubMed] [Google Scholar]
- 40.Grassi G, Facchini A, Trevano FQ et al. Obstructive sleep apnea-dependent and -independent adrenergic activation in obesity. Hypertension. 2005;46(2):321–5. doi: 10.1161/01.HYP.0000174243.39897.6c. [DOI] [PubMed] [Google Scholar]
- 41.Somers VK, Dyken ME, Clary MP et al. Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest. 1995;96(4):1897–1904. doi: 10.1172/JCI118235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Wolk R, Shamsuzzaman AS, Somers VK. Obesity, sleep apnea, and hypertension. Hypertension. 2003;42(6):1067–74. doi: 10.1161/01.HYP.0000101686.98973.A3. [DOI] [PubMed] [Google Scholar]
- 43.Lam JC, Xu A, Tam S et al. Hypoadiponectinemia is related to sympathetic activation and severity of obstructive sleep apnea. Sleep. 2008;31(12):1721–7. doi: 10.1093/sleep/31.12.1721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Pratt-Ubanama MN, Nishizaka MK, Boedefeld RL et al. Plasma aldosterone is related to severity of obstructive sleep apnea in subjects with resistant hypertension. Chest. 2007;131(2):453–9. doi: 10.1378/chest.06-1442. [DOI] [PubMed] [Google Scholar]
- 45.Lavie L. Oxidative stress – a unifying paradigm in obstructive sleep apnea and comorbidities. Prog Cardiovasc Dis. 2009;51(4):303–12. doi: 10.1016/j.pcad.2008.08.003. [DOI] [PubMed] [Google Scholar]
- 46.Chin K, Nakamura T, Shimizu K et al. Effects of nasal continuous positive airway pressure on soluble cell adhesion molecules in patients with obstructive sleep apnea syndrome. Am J Med. 2000;109(7):562–7. doi: 10.1016/s0002-9343(00)00580-5. [DOI] [PubMed] [Google Scholar]
- 47.Hui DS, Ko FW, Fok JP et al. The effects of nasal continuous positive airway pressure on platelet activation in obstructive sleep apnea syndrome. Chest. 2004;125(5):1768–75. doi: 10.1378/chest.125.5.1768. [DOI] [PubMed] [Google Scholar]
- 48.Leferbre B, Pepin JL, Baguet JP et al. Leukotriene B4: early mediator of atherosclerosis in obstructive sleep apnoea? Eur Resp J. 2008;32(1):113–20. doi: 10.1183/09031936.00137107. [DOI] [PubMed] [Google Scholar]
- 49.Punjabi NM, Beamer BA. C-reactive protein is associated with sleep disordered breathing independent of adiposity. Sleep. 2007;30(1):29–34. doi: 10.1093/sleep/30.1.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Schulz R, Mahmoudi S, Hattar K et al. Enhanced release of superoxide from polymorphonuclear neutrophils in obstructive sleep apnea. Impact of positive continuous airway pressure therapy. Am J Respir Crit Care Med. 2000;162(2 Pt 1):566–70. doi: 10.1164/ajrccm.162.2.9908091. [DOI] [PubMed] [Google Scholar]
- 51.Yokoe T, Minoguchi K, Matsuo H et al. Elevated levels of C-reactive protein and interleukin-6 in patients with obstructive sleep apnea syndrome are decreased by nasal continuous positive airway pressure. Circulation. 2003;107(8):1129–34. doi: 10.1161/01.cir.0000052627.99976.18. [DOI] [PubMed] [Google Scholar]
- 52.Ip M, Mokhlesi B. Sleep and glucose intolerance/diabetes mellitus. Sleep Med Clin. 2007;2(1):19–29. doi: 10.1016/j.jsmc.2006.12.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Van Cauter E, Holmback U, Knutson K et al. Impact of sleep and sleep loss on neuroendocrine and metabolic function. Horm Res. 2007;67(Suppl 1):2–9. doi: 10.1159/000097543. [DOI] [PubMed] [Google Scholar]
- 54.Taheri S, Lin L, Austin D et al. Short sleep duration is associated with reduced leptin elevated ghrelin, and increased body mass index. PLoS Med. 2004;1(3):e62. doi: 10.1371/journal.pmed.0010062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Shaw JE, Punjabi NM, Wilding JP et al. Sleep disordered breathing and type 2 diabetes: a report from the International Diabetes Federation Taskforce on Epidemiology and Prevention. Diabetes Res Clin Pract. 2008;81(1):2–12. doi: 10.1016/j.diabres.2008.04.025. [DOI] [PubMed] [Google Scholar]
- 56.Parati G, Lombardi C, Hedner J Joint Recommendations by The European Cost Action B26. The European Society of Hypertension and The European Respiratory Society. 2010. http://www.cost.eu/library/publications/10-46-European-Consensus-Document-on-OSA-and-Hypertension
- 57.Marin JM, Agusti A, Villar I et al. Association between treated and untreated obstructive sleep apnoea and risk of hypertension. JAMA. 2012;307(20):2169–76. doi: 10.1001/jama.2012.3418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Alajmi M, Mulgrew AT, Fox J et al. Impact of continuous positive airway pressure therapy on blood pressure in patients with obstructive sleep apnea hypopnea: a meta-analysis of randomized controlled trials. Lung. 2007;185(2):67–72. doi: 10.1007/s00408-006-0117-x. [DOI] [PubMed] [Google Scholar]
- 59.Bazzano LA, Khan Z, Reynolds K et al. Effect of nocturnal nasal continuous positive airway pressure on blood pressure in obstructive sleep apnea. Hypertension. 2007;50(2):417–23. doi: 10.1161/HYPERTENSIONAHA.106.085175. [DOI] [PubMed] [Google Scholar]
- 60.Campos-Rodriguez F, Grilo-Reina A, Perez-Ronchel J et al. Effect of continuous positive airway pressure on ambulatory BP in patients with sleep apnea and hypertension: a placebo-controlled trial. Chest. 2006;129(6):1459–67. doi: 10.1378/chest.129.6.1459. [DOI] [PubMed] [Google Scholar]
- 61.Faccenda JF, Mackay TW, Boon NA et al. Randomized placebo-controlled trial of continuous positive airway pressure on blood pressure in the sleep apnea-hypopnea syndrome. Am J Respir Crit Care Med. 2001;163(2):344–8. doi: 10.1164/ajrccm.163.2.2005037. [DOI] [PubMed] [Google Scholar]
- 62.Haentjens P, Van Meerhaeghe A, Moscariello A et al. The impact of continuous positive airway pressure on blood pressure in patients with obstructive sleep apnea syndrome: evidence from a meta-analysis of placebo-controlled randomized trials. Arch Intern Med. 2007;167(8):757–64. doi: 10.1001/archinte.167.8.757. [DOI] [PubMed] [Google Scholar]
- 63.Hui DS, To KW, Ko FW et al. Nasal CPAP reduces systemic blood pressure in patients with obstructive sleep apnoea and mild sleepiness. Thorax. 2006;61(12):1083–90. doi: 10.1136/thx.2006.064063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Pepperel JC, Ramdassingh-Dow S, Crosthwaite N et al. Ambulatory blood pressure after therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: a randomised parallel trial. Lancet. 2002;359(9302):204–10. doi: 10.1016/S0140-6736(02)07445-7. [DOI] [PubMed] [Google Scholar]
- 65.Marin JM, Carrizo SJ, Vicente E et al. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–53. doi: 10.1016/S0140-6736(05)71141-7. [DOI] [PubMed] [Google Scholar]
- 66.Barbé F, Durán-Cantolla J, Sánchez-de-la-Torre M et al. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: a randomized controlled trial. JAMA. 2012;307(20):2161–8. doi: 10.1001/jama.2012.4366. [DOI] [PubMed] [Google Scholar]
- 67.Campos-Rodriguez F, Martinez-Garcia MA, Martinez M et al. Association between obstructive sleep apnea and cancer incidence in a large multicentre Spanish cohort. Am J Respir Crit Care Med. 2013;187:99–105. doi: 10.1164/rccm.201209-1671OC. [DOI] [PubMed] [Google Scholar]
- 68.Netzer N, Stoohs RA, Netzer CM et al. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Intern Med. 1999;131:485–91. doi: 10.7326/0003-4819-131-7-199910050-00002. [DOI] [PubMed] [Google Scholar]
- 69.Jones MW. Daytime sleepiness, snoring, and obstructive sleep apnea. The Epworth Sleepiness Scale, Chest. 1993;103:30–6. doi: 10.1378/chest.103.1.30. [DOI] [PubMed] [Google Scholar]
- 70.Weinrich G, Woehrle H. A review of ApneaLink as a screening device. ResMed Science Center. 2010.
- 71.American Sleep Disorders Association Report: Standards of Practice Committee. Practice parameters for the indications for polysomnography and related procedures. Sleep. 1997;20:406–22. [PubMed] [Google Scholar]
- 72.Young T, Evans L, Finn L et al. Estimation of the clinically diagnosed portion of sleep apnea syndrome in middle-aged men and women. Sleep. 1997;20:705–6. doi: 10.1093/sleep/20.9.705. [DOI] [PubMed] [Google Scholar]
- 73.Habukawa M, Uchimura N, Kakuma T et al. Effect of CPAP treatment on residual depressive symptoms in patients with major depression and coexisting sleep apnea: contribution of daytime sleepiness to residual depressive symptoms. Sleep Med. 2010;11:552–7. doi: 10.1016/j.sleep.2010.02.007. [DOI] [PubMed] [Google Scholar]
- 74.Sánchez AI, Martínez P, Miró E et al. CPAP and behavioural therapies in patients with obstructive sleep apnea: effects on daytime sleepiness mood and cognitive function. Sleep Med Rev. 2009;13:223–33. doi: 10.1016/j.smrv.2008.07.002. [DOI] [PubMed] [Google Scholar]
- 75.Zias N, Bezwada V, Gilman S et al. Obstructive sleep apnea and erectile dysfunction: still a neglected factor? Sleep Breath. 2009;13:3–10. doi: 10.1007/s11325-008-0212-8. [DOI] [PubMed] [Google Scholar]
- 76.Somers VK, Dyken ME, Clary MP et al. Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest. 1995;96(4):1897–1904. doi: 10.1172/JCI118235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Logan AG. Hypertension in aging patients. Expert Rev Cardiovasc Ther. 2011;9(1):113–120. doi: 10.1586/erc.10.171. [DOI] [PubMed] [Google Scholar]
- 78.Lozano L, Tovar JL, Sampol G et al. Continuous positive airway pressure treatment in sleep apnea patients with resistant hypertension: a randomized controlled trial. J Hypertens. 2010;28(10):2161–68. doi: 10.1097/HJH.0b013e32833b9c63. [DOI] [PubMed] [Google Scholar]
- 79.Witkowski A, Prejbisz A, Florczak E et al. Effects of renal sympathetic denervation on blood pressure sleep apnea course, and glycemic control in patients with resistant hypertension and sleep apnea. Hypertension. 2011;58(4):559–65. doi: 10.1161/HYPERTENSIONAHA.111.173799. [DOI] [PubMed] [Google Scholar]
- 80.Dickstein K, Cohen-Solal A, Filippatos G et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the diagnosis and treatment of acute and chronic heart failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM) Eur J Heart Fail. 2008;10(10):933–89. doi: 10.1016/j.ejheart.2008.08.005. [DOI] [PubMed] [Google Scholar]
- 81.Peled N, Abinader EG, Pillar G et al. Nocturnal ischemic events in patients with obstructive sleep apnea syndrome and ischemic heart disease: effects of continuous positive air pressure treatment. J Am Coll Cardiol. 1999;34(6):1744–9. doi: 10.1016/s0735-1097(99)00407-6. [DOI] [PubMed] [Google Scholar]
- 82.Punjabi NM et al. Do sleep disorders and associated treatments impact glucose metabolism? Drugs. 2009;69(Suppl 2):13–27. doi: 10.2165/11531150-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 83.Woehrle H, Graml A, Weinrich G. Age- and gender-dependent adherence with continuous positive airway pressure therapy. Sleep Medicine. 2011;12:1034–6. doi: 10.1016/j.sleep.2011.05.008. [DOI] [PubMed] [Google Scholar]