

Abstract
A 14-year-old young adult took an overdose of 1.2 g of fluoxetine, a selective serotonin reuptake inhibitor (SSRI) that he had been prescribed for depression. He had a generalised tonic/clonic seizure at 6 hours postingestion.
After the seizure, he developed signs consistent with serotonin syndrome: fine tremor, agitation, sweating and hyperreflexia. This was followed by severe muscle pain and rhabdomyolysis with peak creatine kinase (CK) of 33 941 at 74 hours. He was managed with intravenous fluids and analgesia and discharged after 4 days, having avoided renal injury. The use of SSRI’s such as fluoxetine in teenagers has increased in recent years. While it is generally considered benign in overdose, this report illustrates the severe consequences of overdose at high quantities and discusses appropriate management in these cases. We note that in this case, there was a delayed onset of rhabdomyolysis with peak CK at 74 hours postingestion.
Keywords: child and adolescent psychiatry (paediatrics), unwanted effects / adverse reactions
Background
Fluoxetine is a selective serotonin reuptake inhibitor (SSRI), which is converted into its active metabolite norfluoxetine in the body.1 It achieves a peak plasma concentration 6–8 hours after the ingestion.
Fluoxetine is a very commonly used drug for depression. The use of SSRIs in paediatric cases of depression has been increasing in recent years; supplanting tricyclic antidepressants, as they have a reduced side effect profile and better efficacy.2
Unfortunately, it is also frequently seen in cases of deliberate self-poisoning but is generally considered to be benign in overdose.3 However, in large quantities, dangerous symptoms can occur. This includes serotonin syndrome, a constellation of clinical signs resulting from an excess of serotonin acting on the nervous system including: high body temperature, agitation, hyperreflexia, dilated pupils, diarrhoea and fine tremor.4 It is a clinical diagnosis and cannot be confirmed through laboratory tests. Treatment is generally supportive and involves discontinuing medication and controlling symptoms, particularly hyperthermia.
Other worrying effects of include prolongation of the QT interval and seizures, which are rare, but have been reported in high quantity overdoses.5 6
Another serious effect of fluoxetine overdose is rhabdomyolysis7 which involves the large scale leakage of intracellular contents following injury to skeletal muscle. These intracellular contents are of particular concern, as there is the potential for secondary renal injury. Massive plasma myoglobin levels exceed protein blinding of haptoglobin and precipitate in the glomerular filtrate. This causes renal tubular obstruction and acute kidney injury.8 The mechanism as to how serotonin induces injury to skeletal muscle is not currently well understood.
There is little literature describing when creatine kinase (CK) levels are likely to rise in these patients, and this case report adds to our understanding on how to manage the condition and makes a case for a repeat CK level at >72 hours into admission, where a large overdose has been taken. Moreover, this case report shows that fluoxetine overdose, while generally considered benign, can have serious complications; in this case, a combination of serotonin syndrome, seizure and rhabdomyolysis.
Case presentation
A 14-year-old man with a history of anxiety, depression and self-harm, but otherwise medically well, ingested approximately sixty 20 mg tablets (1.2 g total) of fluoxetine that he was prescribed for his depression, in an attempt to commit suicide.
Having taken the overdose at approximately 02:00 hours. He started feeling unwell at around 09:00 hours. His parents were alerted to the sound of him vomiting but were unaware of the overdose. At approximately at 09:15 hours, he then had a generalised tonic/clonic seizure which lasted for 2–3 min and was witnessed by the parents who phoned for an ambulance.
Paramedics arrived in approximately 12–15 min. They noticed postictal symptoms of tiredness and confusion. The initial blood pressure (BP) was 145/91, with a sinus tachycardia with a pulse rate of 141 bpm. On arrival to Accident and emergency, he was more alert and had a temperature 36.9°C, heart rate 122 bpm, BP 122/68 respiratory rate was 22/min with O2 saturations of 98%.
He received two boluses of 500 mL normal saline at half an hour apart and was transferred to paediatric ward. On admission to the paediatric ward, he started displaying neurological signs consistent with serotonin syndrome, with a fine tremor, brisk reflexes bilaterally, 2–3 beats of clonus and down going plantars. Power in both upper limbs was normal, but was sligtly reduced in lower limbs due to mild pain. Pupils were slightly dilated but reactive to light. The rest of the clinical examination was normal.
Investigations
He was placed on a cardiac monitor and had a 12-lead ECG which showed sinus tachycardia and a normal QT interval. A venous blood gas was obtained which showed a normal acid–base balance, lactate and glucose.
Initial blood tests showed a moderately raised CK of 532 (normal value 0–500 µmol/L). The rest of his blood tests, which included urea, sodium, potassium, creatinine, calcium, magnesium, liver function tests (aspartate transaminase and alkaline phosphatase) and a full blood count were normal. Urine toxicology screen was only positive for paracetamol which he had taken for his leg pain. There was a normal urine dipstick with no blood.
He then received intravenous maintenance fluids with 0.9% saline with 5% dextrose, 500 mL bag over 8 hours. During this time, the muscular leg pain that the patient described worsened significantly. Repeat blood tests, at 36 hours, showed a dramatic increase in CK level to 12 645.
Differential diagnosis
While the fluoxetine overdose was admitted to, given the presence of serotonin syndrome, the possibility a mixed overdose with other drugs that are serotonergic such as ecstasy or cocaine were considered and urine toxicology sent. No positive result was found for any drugs of abuse.
Treatment
He was hydrated with intravenous maintenance fluids and received potassium replacement to correct his hypokalaemia. Regular ECGs were performed to monitor length of QRS complex.
He was referred to children and adolescents mental health service for assessment and treatment.
Outcome and follow-up
Following intravenous hydration and analgesia, the signs of serotonin syndrome started to resolve by 50 hours. However, he continued to with severe muscle aches. Another CK was completed which showed a marked increase at 74 hours postingestion to 33 941 µmol/L.
This was managed conservatively with simple analgesia (paracetamol) and oral fluids. Eventually, his pain lessened, and a further CK level at 98 hours showed a fall to 12 245. Figure 1 illustrates the rise in CK during his admission. The initial creatinine was 94 µmol/L (normal value 60–100 µmol/L). Figure 2 shows level of creatinine postingestion, showing that the creatinine level did not exceed normal values. Acute renal failure was therefore avoided during this admission, possibly as a result of the early intravenous hydration.
Figure 1.

Line graph showing creatine kinase levels postingestion of fluoextine.
Figure 2.
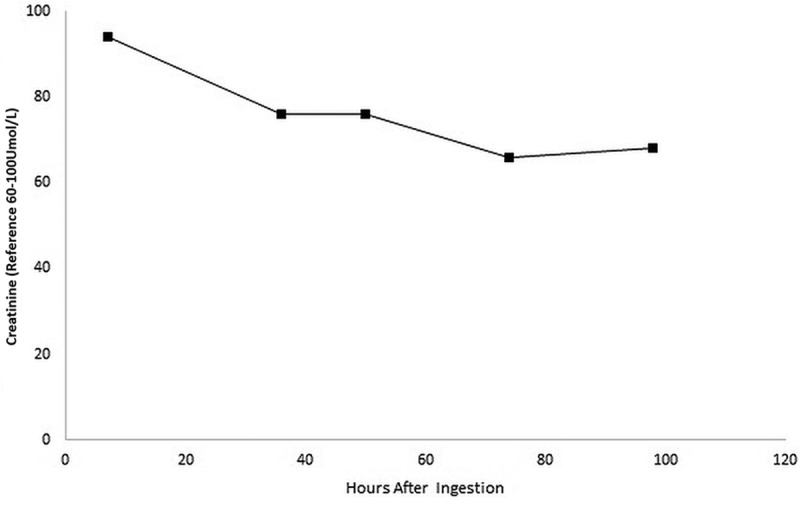
Line graph showing creatinine level postingestion of fluoxetine.
He was eventually discharged with support from the child and adolescent mental health team in the community.
Discussion
Seizures have been reported in cases of isolated fluoxetine ingestion6 but are thought to be a rare side effect; occurring more commonly in a mixed overdoses with other medications or in a child with pre-existing brain disease. As fluoxetine is an anticonvulsant (at low doses), this is perhaps not surprising.9 In a study comparing SSRI medication, fluoxetine had the lowest incidence of inducing seizures (1% vs 2% for sertraline, paroxetine and citalopram and 4% for fluvoxamine).10
Serotonin syndrome is a potentially life-threatening condition caused by overdose of seronergic medications (such as SSRIs, monoamine oxidase inhibits, tricyclic antidepressants, amphetamines or tramadol) or recreational drugs (including ecstasy and cocaine). It has previously been queried where fluoxetine, on its own, can cause serotonin syndrome11 as it is usually reported in combination with other medications. This case report adds to the evidence that both serotonin syndrome and seizures can be seen in an overdose of fluoxetine alone.
In this case, we observed that both clinical symptoms of rhabdomyolysis and laboratory CK levels had a delayed onset, worsening at around 36 hours, well after the seizure and development of serotonin syndrome. Current guidelines on management of fluoxetine overdose such as those developed by public health England via Toxbase.org recommend a period of observation of 6 hours if the patient is asymptomatic. A repeat CK level is recommended if there has been concern regarding muscle damage, however, there is no clear evidence or guidelines regarding timings to repeat the CK levels. In this case, we found that CK levels were slightly raised on admission but increased dramatically by 36 hours. For this reason, we would advocate that if a large overdose of fluoxetine is suspected, CK levels should be checked both on arrival and later into admission so that rhabdomyolysis can be detected early and intravenous hydration started. To our knowledge, this is the first case report to describe this delayed onset of rhabdomyolysis.
Learning points.
Selective serotonin reuptake inhibitor medications are now commonly prescribed in teenagers for depression. While most cases of overdose are mild, severe symptoms such as seizures, serotonin syndrome and rhabdomyolysis can be seen in large overdoses.
In this case, the onset of rhabdomyolysis was delayed, with creatine kinase (CK) levels within normal range on admission but rose rapidly at 36 hours and peaked at 74 hours.
This illustrates the importance of checking CK both on arrival and later into admission as early fluid replacement can help to prevent renal failure in these cases.
While small overdoses can be discharged from a medical standpoint after a short period of observation, larger overdoses may require several days inpatient stay to manage fluids and pain from rhabdomyolysis.
Footnotes
Contributors: RL-K: conceptualised the paper, drafted the manuscript, completed revision of the manuscript and created figures. SZ: drafted the manuscript with RL-K and completed revision of the manuscript. PM: revised the manuscript and figures. RL-K, SZ, PM: approved the final submission.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent: Parental/guardian consent obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Stark P, Fuller RW, Wong DT. The pharmacologic profile of fluoxetine. J Clin Psychiatry 1985;46(3 Pt 2):7–13. [PubMed] [Google Scholar]
- 2.Qin B, Zhang Y, Zhou X, et al. . Selective serotonin reuptake inhibitors versus tricyclic antidepressants in young patients: a meta-analysis of efficacy and acceptability. Clin Ther 2014;36:1087–95. 10.1016/j.clinthera.2014.06.001 [DOI] [PubMed] [Google Scholar]
- 3.Borys DJ, Setzer SC, Ling LJ, et al. . Acute fluoxetine overdose: a report of 234 cases. Am J Emerg Med 1992;10:115–20. 10.1016/0735-6757(92)90041-U [DOI] [PubMed] [Google Scholar]
- 4.Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005;352:1112–20. 10.1056/NEJMra041867 [DOI] [PubMed] [Google Scholar]
- 5.Braitberg G, Curry SC. Seizure after isolated fluoxetine overdose. Ann Emerg Med 1995;26:234–7. 10.1016/S0196-0644(95)70157-5 [DOI] [PubMed] [Google Scholar]
- 6.Gross R, Dannon PN, Lepkifker E, et al. . Generalized seizures caused by fluoxetine overdose. Am J Emerg Med 1998;16:328–9. 10.1016/S0735-6757(98)90118-8 [DOI] [PubMed] [Google Scholar]
- 7.Snyder M, Kish T. Sertraline-induced rhabdomyolysis: a case report and literature review. Am J Ther 2016;23:e561–5. 10.1097/MJT.0000000000000196 [DOI] [PubMed] [Google Scholar]
- 8.Zutt R, van der Kooi AJ, Linthorst GE, et al. . Rhabdomyolysis: review of the literature. Neuromuscul Disord 2014;24:651–9. 10.1016/j.nmd.2014.05.005 [DOI] [PubMed] [Google Scholar]
- 9.Jobe PC, Browning RA. The serotonergic and noradrenergic effects of antidepressant drugs are anticonvulsant, not proconvulsant. Epilepsy Behav 2005;7:602–19. 10.1016/j.yebeh.2005.07.014 [DOI] [PubMed] [Google Scholar]
- 10.Isbister GK, Bowe SJ, Dawson A, et al. . Relative toxicity of selective serotonin reuptake inhibitors (SSRIs) in overdose. J Toxicol Clin Toxicol 2004;42:277–85. 10.1081/CLT-120037428 [DOI] [PubMed] [Google Scholar]
- 11.Ghanizadeh A, Ghanizadeh M, Seifoori M. Can fluoxetine alone cause serotonin syndrome in adolescents? Psychopharmacol Bull 2008;41:76–9. [PubMed] [Google Scholar]