

Abstract
Introduction:
The SNAC wrist (Scaphoid nonunion advanced collapse) is one of the complications following scaphoid fractures treated conservatively and one of the causes of wrist arthritis that the hand surgeon has to face most frequently. In these cases surgical management is usually warranted.
Materials and Methods:
In the set time frame of 6 years we treated 15 SNAC wrist cases. On average patients underwent surgery five years after the trauma. All patients were treated via dorsal incision with partial carpal arthrodesis and total scaphoidectomy, associated with denervation of the posterior interosseous nerves. A plaster cast was applied to all patients for 3 weeks postoperatively. In the preoperative stage, X-rays of the healthy contralateral limb were taken for the measurement of the normal radiocarpal joint space. Clinical and radiographic follow-ups were conducted at 1,3, 6 and 12 months from the trauma; then every 12 months. Criteria for the evaluation of patients: visual analog pain scale (VAS), average time of radiographic fusion of wrist bones, Active Range of Wrist Motion (WAROM), subjective Mayo Wrist Score (MWS) and The Short Form ( 36) Health Survey (SF-36), return to the main tasks and complications. The evaluation endpoint was set at 60 months. Average time of surgery: 48.3 minutes. Average time of arthrodesis consolidation: 67.8 days. The VAS and WAROM showed a gradual improvement in seriated controls, returning to values almost identical to pre-trauma at a 5-year follow-up. By this time, the MWS and SF-36 scores were similar to pre-trauma. On average, the return to pre-injury daily activities occurred in 12.5 months after surgery. There were no complications.
Conclusions:
The partial carpal arthrodesis is a safe and effective procedure for the treatment of SNAC wrist cases. Our results show a progressive and significant improvement in ROM, VAS and great satisfaction from the patient.
Keywords: SNAC wrist, carpal fusion, hand outcome, scaphoid nonunion
1. INTRODUCTION
The SNAC wrist (Scaphoid nonunion advanced collapse) is one of the complications following scaphoid fractures treated conservatively and one of the causes of wrist arthritis that the hand surgeon has to face most frequently. Scaphoid fractures are a very common pattern of injury whose mechanism is usually associated with a fall onto an outstretched hand. Commonly experienced symptoms are: pain, tenderness at the level of the snuffbox, worsening of symptoms when trying to pinch or grasp an object. Non-union of the fracture occurs when a scaphoid fracture fails to heal (1, 2, 3).
The Watson & Ballet classification is the most widely used in clinical practice and in scientific works for the description of this pathological condition (4, 5, 6). It allows a standardized assessment of patients and subsequent appropriate management. It classifies and highlights three different stages:
Stage I: Osteoarthritis localized on the radial side of the scaphoid and the radial styloid process
Stage II: Stage 1 condition plus the scapho-capitatejoint involvement.
Stage III: Peri-scaphoid arthritis.
When conservative therapy fails, the patient has to undergo surgery (7, 8). There are multiple options for the treatment of SNAC wrist. They range from styloidectomy to scaphoid distal pole excision, denervation of the wrist, partial to total carpal arthrodesis, removal of the first carpal row, total arthrodesis of the wrist. The treatment of choice varies depending on personal preference of the surgeon as well as the stage of osteoarthritis (7, 8, 9). Often the decision is made intraoperatively after the articular surface status of the capitate is assessed (1, 7, 11). It is also possible to combine other procedures, such as the association of styloidectomy and denervation of the interosseous nerves, with those mentioned above (1, 6-12).
The aim of our study is to report our experience of a significant number of surgical treated patients with SNAC wrist after conservative management failure and compare it to the data present in the published literature.
2. MATERIALS AND METHODS
From January 2006 to December 2013, we treated 15 patients suffered by wrist osteoarthritis (OAW). The studied group had an average age of 47.8 years (range 29- 64 years), with a gender ratio of 2.75 males for every female (11m: 4f). In all cases osteoarthritis was the result of a scaphoid fracture conservatively treated (Table 1). Only one patient had been previously operated on for a scaphoid injury (Table 1). On average, patients underwent surgery 5.3 (range 3.4-88) years after the trauma. Exclusion criteria: use of corticosteroids as conservatively baseline therapy, pathological fractures caused by hematological or oncological diseases; patients who did not adhere to a minimum follow-up of 60 months. All patients were informed in a clear and exhaustive way of the various options of treatment and the corresponding surgical and conservative alternatives. Patients were treated according to the ethical standards of the Helsinki Declaration and were invited to read, understand and sign the informed consent form. Partial carpal arthrodesis was performed via dorsal incision for all patients, with Twin Fix Stryker® screws, without the use of bone grafts, total scaphoidectomy associated with denervation of the posterior interosseous nerves. All patients in the postoperative period were given a plaster cast for 3 weeks. X-rays of the healthy contralateral limb were taken for the measurement of the correctradio-carpal joint space in all cases in the preoperative period.
Table 1. Description of Population.
| Number of Patients | 15 |
| Average years old | 47.8 |
| Range of age | 29-64 |
| Gender ratio (m:f) | 2.75:1(11:4) |
| Dominant Hand | Right 12 Left 3 |
| Type of acuteCarpal Schapoid Fracture Herbet Classification (number) | Type A: 2 Type B:13 |
| Work Of Population:Number (%) | Agricultural Activity: 6 Industrial Sector: 6 Tertiary Industry: 3 |
| Causa del trauma: Number (%) | Fall from High: 3 Car Accident: 5 Work Accident: 7 |
| Average time of carpal arthrodesis stabilitation from trauma | 5.3 years |
| Range of time of carpal arthrodesis stabilitation from trauma | 3.4-8.8 years |
Clinical and radiographic follow-ups were conducted at 1, 3, 6 and 12 months after injury and every year thereafter.
The criteria for the assessment of patients were: the visual analog pain scale from the traumatized wrist (VAS), the average time for the radiographic fusion of the wrist bone, Active Range of Wrist Motion (WAROM), the subjective Mayo Wrist Score (MWS) and the Short Form (36) Health Survey (SF-36), the return to the daily activities and complications. The evaluation endpoint was set at 60 months.
Surgical Technique
This surgical procedure (especially indicated for all those cases with radiocarpal osteoarthritis where the mid-carpal joint is damaged) permits to achieve significant reduction of pain, without affecting the wrist joint and significantly guaranteeing all the benefits deriving from a minimally invasive surgical procedure. The procedure involves the resection of the scaphoid followed by the capitate, lunate, triquetrum and hamate fusion, also known as 4-corner fusion. The denervation of the interosseous nerve for effective pain control is also performed. The operation is performed via dorsal incision in order to avoid volar radiocarpal ligament injuries, thus preventing the ulnocarpal translation postoperatively. This procedure, despite being technically more complex when compared to techniques such as the resection of the first carpal row, has indeed some relevant advantages, such as maintaining the proper carpal height ratio and the congruence between the central portion and the third ulnocarpal.
3. RESULTS
Average operating time was 48.3 minutes (range 38.25-60.33). The average time of arthrodesis consolidation occurred in 67.8 days (35-94 days)(Fig.2). The VAS at the 5-years follow-up returned almost identical to the pre-injury values (Table 1).
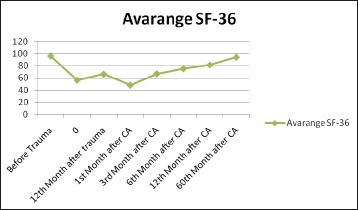
Figure 2. The trend of SF-36 before the trauma until 60th month from the CA surgery.
The average pre-injury WAROM levels (measured on the healthy limb) were: flexion 82.7 degrees, extension 83.5 degrees; abduction 13.4 degrees and adduction 43.7 degrees. At 12 months from the trauma, the levels were: flexion of 33.8 degrees, extension of 34.1 degrees; abduction of 3.4 degrees and adduction 22.8 degrees. At the 5-year follow-up after surgery, the average WAROM levels were: flexion 79.3 degrees, extension 81.2 degrees; abduction 11.8 degrees and adduction 40.6 degrees.
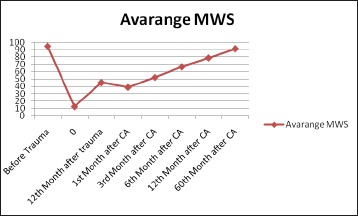
At the60-months follow-up, the MWS (Graph 1) and the SF-36 (Graph.2) scores could be compared to pre-trauma. On average, the return to the normal daily activities occurred in 12.5 months after surgery.
There were no complications
4. DISCUSSION
Pseudarthrosis of the carpal scaphoid bone, resulting from a non-recognized fracture of the scaphoid bone or a conservatively treated fracture, is a cause of carpal instability that can potentially lead to development of secondary osteoarthritis of the wrist with the X-ray picture of the SNAC wrist ( scaphoid nonunion advanced collapse) (1, 2,3).
The aim of the surgical procedure is to eliminate the significant experienced pain while attempting to preserve the maximum range of motion of the radiocarpal joint, and maintain adequate grip strength and functionality. Over the years, there has been numerous scientific publications showing satisfactory results of the partial arthrodesis procedures, associated with either the carpal scaphoidectomy or the 4 corner fusion procedure, confirming this technique as one of the most widely accepted treatments for SNAC wrist and more generally carpal instability cases (8, 9, 10, 13, 14).
Karakauer et al (in their series of 24 patients monitored for an average follow-up at 41 months) achieved a total or subtotal reduction of pain in 16 patients and gripping strength values equal to 78.5% compared to the contra lateral healthy limb (10). In the same year Ashamed at al also reported on their series of 100 patients (monitored for an average follow-up at 4 years) very satisfactory outcomes (11). These same patients were most likely included in the subsequent work of Watson at al showing satisfactory results in 252 patients during an average follow-up at 44 month (9).
In more recent years, Gregory I. Bain at al reported their experience with this technique in 31 patients who were monitored for an average follow-up of 10 years, also reporting excellent functional outcomes and improvement of symptoms (14).
From the data available in the literature it also appears that this technique permits the achievement of excellent functional and symptomatic outcomes in the medium and long term and with a low rate of complications, when compared with other techniques such as proximal carpectomy (12).
Among the various management option used to obtain partial carpal arthrodesis (circular plates, compression screws, K-wires) proposed in the literature, the use of screws is the method that provides the best results with fewer complications (15,16). It is in fact demonstrated that the use of circular rather than spider plates to obtain the fusion of the mid-carpal joints is subject to a higher rate of failures essentially due to no union, implant failures, tenosynovitis or chronic neuritis, impingement of the radial dorsal end in the extensor movements of the wrist and subsequent pain (15,17). Probably the greatest rate of failures with these methods is due to the greater technical difficulties in performing them (15), or, as illustrated by N. Maire at al, (16) the reasons could be of biomechanical nature. In fact, with circular plates, the compressive forces are directed in centripetal manner rather than perpendicular, to the inter-line of fusion as, instead, happens using compression screws (16) (Figure 1 and 2). Subjective data should also not be neglected.
Figure 1. The trend of MWS before the trauma until 60th month from the CA surgery.
In most of our cases the individual satisfaction rate of the patients (regardless of the of X-ray and /or final clinical outcomes) has been more satisfactory with the use of a minimally invasive techniques (compression screws, K-wires), than a greater invasiveness and longer operating times (spider and/or circular plates) (15). No significant differences were found from more invasive procedures (17).
We should not exclude the possibility, especially in the forms of pancarpal arthritis, of radio carpal prosthesis or total wrist arthrodesis as management option. Total wrist arthroplasty (TWA) has, over the years, received mixed fortunes. Nowadays there are only three implants approved by the FDA on the market: Universal 2, Maestro, Re-Motion, which are essentially the developments of the third generation prostheses introduced in the eighties. These devices, while reproducing more accurately the anatomy of the wrist and allowing movements on several levels, are currently of little use in routine clinical practice, since there is not enough evidence in the literature to predict the evolution of the implant in the long run (18). Arthrodesis of the wrist, while remaining a possibility available to the surgeon, to be considered for those patients with pancarpal arthritis and persistent, chronic, and crippling wrist pain, not responding to other physical and pharmacological treatments, implies in our opinion functional limitations which are unacceptable today. Even though, it has been shown in the literature that to perform the normal daily activities is sufficient a range of motion (ROM) of 30 ° in extension, 5 ° in flexion, 15 °in ulnar deviation and 10 ° in a radial deviation (19), According to some authors, it would be sufficient to conduct most of these activities with the following ROMs: 6 ° in extension, 5 ° in flexion, 6 ° in ulnar deviation and 7 in radial deviation (20). In our opinion, these angular values are unacceptable nowadays. The results obtained by us, even taking into account the limitations of the study, due to the low number of the samples analyzed, show that when possible, efforts should be made to preserve the maximum original anatomy of the joint, limiting the surgery to the minimum, thus ensuring to the patient an effective resolution of pain, not accompanied though by a significant loss of joint range of motion. Furthermore, the technique used by us, ensuring mini-invasiveness, allows a more rapid start of the rehabilitation therapy and a faster return to the daily activities.
5. CONCLUSIONS
The arthritis of the wrist is certainly a common and highly disabling pathology because of its impact on the daily activities. The study of the radiographic picture and an accurate preoperative planning represent key and essential moments for a good clinical outcome, in order to ensure the most appropriate treatment and the best possible results. Over the years, the technique has gradually gone from a mere symptomatic surgery performing arthrodesis to provide relief from the painful symptoms at the expense of joint functionality, to today where more attention is given to joint preservation and functionality. Due to the development of many surgical techniques it is possible to improve the pain symptoms and protect joint functionality.
In our opinion, in all the cases where this procedure is indicated, the partial carpal arthrodesis associated with total scaphoidectomy is certainly an interesting, effective and feasible technique which permits to achieve more than satisfactory functional and clinical results on the long run if performed by expert surgeons.
It seems that a more powered study with higher level of evidence is advisable in order to achieve better standardization of indications for treatments and planned follow ups, better interpretations of results and reduction of bias factors.
Author’s contribution:
Each author participated in each step of research. G.R. revised it critically. Each author gave final approval for final version of article.
Conflict of interest:
none declared.
Financial support and sponsorship:
None.
REFERENCES
- 1.Shah CM, Stern PJ. Scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC) wrist arthritis. Curr Rev Musculoskelet Med. 2013 Mar;6(1):9–17. doi: 10.1007/s12178-012-9149-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ruby L, Leslie B. Wrist arthritis associated with scaphoid non-union. Hand Clin. 1987;3:529–539. [PubMed] [Google Scholar]
- 3.Watson HK, Ryu J. Evolution of arthritis of the wrist. Clin Orthop Relat Res. 1986;202:57–67. [PubMed] [Google Scholar]
- 4.Watson HK, Ballet FL. The SLAC wrist: scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg. 1984;9A:358–365. doi: 10.1016/s0363-5023(84)80223-3. [DOI] [PubMed] [Google Scholar]
- 5.Vishwanathan K, Hearnden A, Talwalkar S, et al. Reproducibility of radiographic classification of scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC) wrist. J Hand Surg Eur. 2013;38(7):780–787. doi: 10.1177/1753193413484629. [DOI] [PubMed] [Google Scholar]
- 6.Penteado FT, Dos Santos JB, Caporrino FA, et al. Scaphoid nonunion advanced collapse classifications: a reliability study. J Hand Microsurg. 2012;4(1):12–15. doi: 10.1007/s12593-012-0062-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kiefhaber TR. Management of scapholunate advanced collapse pattern of degenerative arthritis of the wrist. J Hand Surg. 2009;34(8):1527–1530. doi: 10.1016/j.jhsa.2009.06.020. [DOI] [PubMed] [Google Scholar]
- 8.Ashmead Dt, Watson HK, Damon C, Herber S, Paly W. Scapholunate advanced collapse wrist salvage. J Hand Surg. 1994;19A:741–750. doi: 10.1016/0363-5023(94)90177-5. [DOI] [PubMed] [Google Scholar]
- 9.Watson HK, Weinzweig J, Guidera PM, Zeppieri J, Ashmead D. One thousand intercarpal arthrodeses. J Hand SurgAm. 1999;24 B:307–315. doi: 10.1054/jhsb.1999.0066. [DOI] [PubMed] [Google Scholar]
- 10.Krakauer JD, Bishop AT, Cooney WP. Surgical treatment of scapholunate advanced collapse. J Hand Surg. 1994;19A:751–759. doi: 10.1016/0363-5023(94)90178-3. [DOI] [PubMed] [Google Scholar]
- 11.Vanhove W, Vil JD, Van Seymortier P, et al. Proximal row carpectomy versus four-corner arthrodesis as a treatment for SLAC (scapholunate advanced collapse) wrist. J Hand Surg (Br) 2008;33E(2):118–125. doi: 10.1177/1753193408087116. [DOI] [PubMed] [Google Scholar]
- 12.Dacho AK, Baumeister S, Germann G, et al. Comparison of proximal row carpectomy and midcarpal arthrodesis for the treatment of scaphoid nonunion advanced collapse (SNAC-wrist) and scapholunate advanced collapse (SLAC-wrist) in stage II. J Plast Reconstr Aesthet Surg. 2008;61:1210–1218. doi: 10.1016/j.bjps.2007.08.007. [DOI] [PubMed] [Google Scholar]
- 13.Goldfarb CA, Stern PJ, Kiefhaber TR. Palmar midcarpal instability: the results of treatment with 4-corner arthrodesis. J Hand Surg. 2004;29A:258–263. doi: 10.1016/j.jhsa.2003.11.009. [DOI] [PubMed] [Google Scholar]
- 14.Bain GI, Watts AC. The outcome of scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years. J Hand Surg Am. 2010;35(5):719–725. doi: 10.1016/j.jhsa.2010.01.025. [DOI] [PubMed] [Google Scholar]
- 15.Vance MC, Hernandez JD, Didonna ML, Stern PJ. Complications and outcome of four-corner arthrodesis: circular plate fixation versus traditional techniques. J Hand Surg Am. 2005;30(6):1122–1127. doi: 10.1016/j.jhsa.2005.08.007. [DOI] [PubMed] [Google Scholar]
- 16.Maire N, Facca S, Gouzou S, Liverneaux P. Midcarpal fusion using break-away compression screw. Chir Main. 2012;31(1):24–29. doi: 10.1016/j.main.2011.11.003. [DOI] [PubMed] [Google Scholar]