

Abstract
Background
The Demirjian method has been the most widely tested method for the estimation of the dental age of children and adolescents. However, only three studies have compared Demirjian’s original and revised seven-tooth methods, four-tooth method and alternate four-tooth method, none of them conducted on an Indian population.
Aim
The present study aimed to compare the applicability of the original and revised seven-tooth and four-tooth and alternate four-tooth standards for age estimation of 1200 Indian children aged 5-15 years old.
Design
The study was designed as a retrospective cross-sectional study.
Results
Demirjian’s original seven-tooth method overestimated age by 0.64 ± 1.44, 0.75 ± 1.50 and 0.69 ± 1.46 years in boys, girls and the total sample, respectively. Demirjian’s revised seven-tooth method overestimated age by + 0.24 ± 0.80, + 0.11 ± 0.81 and + 0.19 ± 0.80 years in boys, girls and the total sample, respectively. Demirjian’s original four-tooth method overestimated age by 0.79 ± 1.59, 0.59 ± 2.77 and 0.72 ± 2.30 years in boys, girls and the total sample, respectively. Demirjian’s alternate four-tooth method overestimated age by 1.31 ± 1.07, 1.20 ± 1.10 and 1.26 ± 1.08 years in boys, girls and the total sample, respectively. Statistically significant differences were observed between dental and chronological ages with all methods (p < 0.001). Significant gender-based differences were observed only with Demirjian’s revised seven-tooth and original four-tooth methods (p < 0.05).
Conclusion
The revised seven-tooth standards most accurately predicted the age of the study sample (mean prediction error = 2.28 months), followed by the original seven-tooth, four-tooth and alternate four-tooth standards. The Demirjian original seven-tooth method was significantly more accurate in boys compared to girls, while the reverse was true for the Demirjian revised seven-tooth and original four-tooth methods.
Keywords: age estimation, Demirjian’s method, seven-tooth method, four-tooth method, Indian children
INTRODUCTION
On the back of much early research by several investigators that pointed to tooth formation being a more reliable indicator of dental age than tooth emergence, Demirjian, Goldstein and Tanner (1) developed a method of estimating dental maturity based on relative and not absolute measurements of eight stages which they described as observable during the development of the seven mandibular teeth of a French-Canadian population. The authors derived self-weighted maturity scores for each stage of each tooth, separate for males and females, and constructed centile charts that allowed the conversion of the numerical maturity score, derived by their method of assessment, to dental age. Following a subsequent study on a larger sample of the same French-Canadian origin, Demirjian and Goldstein (2) updated their original self-weighted scores.
Demirjian’s original and revised seven-tooth methods required an orthopantomograph (OPG) for assessment of the dental development. Where OPGs could not be obtained, Demirjian and Goldstein (2) recommended the use of periapical radiographs of four teeth (the molars and premolars), which they considered a separate system and for which they presented separate scores and standards. Where the first molar was missing, the central incisor was assessed in place of the molar, the development of the two teeth being chronologically almost the same. Separate scores and standards for this group of four teeth were also presented.
Since its introduction more than four decades ago, the Demirjian method (2) of age estimation has emerged as the most widely researched and applied technique in dental age estimation of children and adolescents. While a large majority of studies have tested the revised seven-tooth method, globally only three studies have compared Demirjian’s original and revised seven-tooth methods, four-tooth method and alternate four-tooth method. (3-5) No such study on any Indian population is yet available in the dental literature. Therefore, the present study aimed to compare the applicability of the original and revised seven-tooth and four-tooth and alternate four-tooth standards for age estimation of 5-15 year old Indian children.
MATERIALS AND METHODS
This study was designed as a cross-sectional observational study. Ethical clearance was obtained from the Ethical Committee, Pacific Dental College and Hospital, Udaipur, India. Parents/ guardians had signed an agreement with the dental institution that dental records and radiographs could be used only for research and educational purposes without the possibility of personal identification.
Sampling method: A convenience sampling method was employed, all radiographs being made during the period from January 2012 to September 2015 of children aged between 5.0 and 15.9 years who had sought treatment at the Department of Paediatric Dentistry, Pacific Dental College and Hospital, Udaipur, Rajasthan, India, and required an orthopantomograph (OPG) as part of the investigation protocol.
Selection criteria: Both parents of all children were of Indian origin and nationality. Only patients with a documented date of birth and date of radiography in the oral health record were included to facilitate verification of the chronological age (in completed years) for each subject. Panoramic radiographs with image distortion due to improper position or movement of the patient during exposure, and incomplete image or lack of clarity resulting from an improper exposure technique were excluded. Also, radiographs were excluded from the study if the patient had any history of surgical/medical treatment or systemic illness with the potential to cause significantly delayed or early development, significant numbers of teeth other than third molars missing either congenitally or due to disease and trauma, malformation of teeth or obvious dental pathology that could affect tooth development.
Final sample: Of the 1303 radiographs collected, 103 did not meet the selection criteria owing to either congenital absence of several teeth (22), lack of image clarity (8) or inadequate information regarding the date of birth (73). Thus, a final sample of 1200 OPGS of 699 male and 501 female Indian children aged 5 to 15 years was selected for the study. Radiographs of patients aged 5.0 to 5.9 years were included in age group 5, of those aged 6.0 to 6.9 years in age group 6 and so on. Thus, age group 15 consisted of children aged 15.0 to 15.9 years.
Calculation of chronological age: The dates of birth and of panoramic radiography were obtained from the hospital records. A function of Microsoft Excel was used to calculate the difference between the recorded date of birth and the date on which the panoramic radiograph was made, to obtain the chronological age (CA) in decimal years.
Calculation of dental age: All digital radiographs meeting the selection criteria were viewed on the same LCD monitor using a magnifying glass for improved visualization. Each OPG was coded with a numerical ID to avoid examiner bias. Age and sex of the subjects were thus unknown to the examiner. Nomenclature for teeth assessed was assigned according to the FDI system. For both seven-tooth methods, the seven mandibular teeth of the left side (excluding the third molar) were evaluated by the Demirjian’s dental staging method. (1) Once the stage that most accurately described the stage of development of the tooth in question was identified, the corresponding alpha-numeric rating (0 to H) was assigned to that tooth. In the original seven-tooth method (D7-O), the alpha-numeric stages 0 to H were converted to the original self-weighted gender-specific numerical scores of Demirjian and Goldstein and Tanner. (1) In the revised seven-tooth method (D7-R), the revised self-weighted scores of Demirjian and Goldstein (2) were utilized. In the four-tooth method (D4-O), the left mandibular premolars and first and second molars were assessed and in the alternate four-tooth method (D4-A), the left mandibular central incisor, premolars and second molar were assessed. Scoring for these two methods was done using the separate self-weighted scores described by Demirjian and Goldstein. (2) In all methods, the individual scores were summed to obtain a total maturity score or dental score, which was converted to a dental age (DA) using the Demirjian, Tanner and Goldstein tables. (1)
Reproducibility of measurements: A single examiner assessed all radiographs. Intra-examiner agreement was assessed by having one examiner re-evaluate the same 100 radiographs after a period of 2 months without any knowledge of gender or age or of the stages assigned in the first evaluation. Two well-trained examiners independently evaluated 100 radiographs using Demirjian’s method of dental staging, after a period of mutual calibration and without any knowledge of age or gender, in order to allow an analysis of inter-examiner agreement.
Data analysis: All statistical analyses and data management were performed using the Statistical Package for Social Sciences 19.0 (SPSS Inc., Chicago, IL, USA) for Windows and MS-Excel (Microsoft Office 2010). Analyses were made for each gender and age group, and for the total sample. Kolmogorov-Smirnov and Shapiro-Wilk tests were performed to test the normality of the data. As the sample showed a non-normal distribution, non-parametric tests were applied. For all tests, a p value ≤ 0.05 was considered statistically significant.
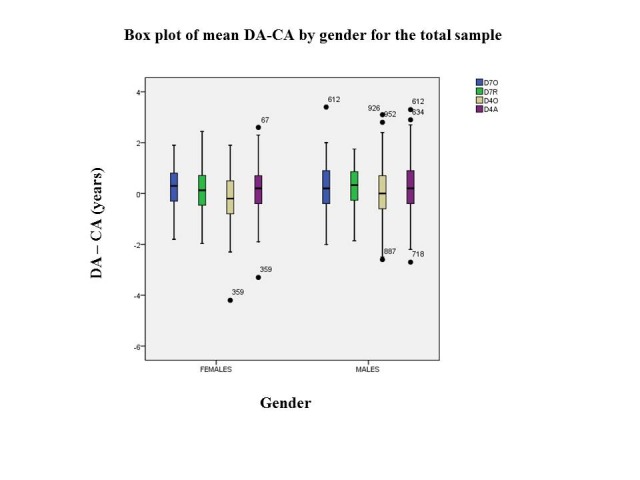
The accuracy of each method of age estimation was determined by the mean difference between the dental age and the chronological age (DA–CA) for each gender and age group, and the total sample. A positive result indicated an overestimation and a negative result indicated an underestimation of age. Box-plot graphs are used to present the mean DA-CA of each gender and age group, and the total sample, with whiskers indicating the range (Figures 1-5). Absolute accuracy was determined by means of the absolute differences between DA and CA of girls and boys and the total sample for each method. The Wilcoxon signed rank test was applied to assess the significance of DA-CA for both methods for each gender and age group, for the total sample and between methods. Independent t-test was employed for comparisons of DA-CA between genders. The correlation between DA and CA was analysed using Spearman’s rank correlation coefficient for each gender and for the total study sample. Intra- and inter-examiner agreements are expressed as percentages. Cohen’s kappa coefficient was used to calculate the degree of reliability of these agreements.
Figure 1.
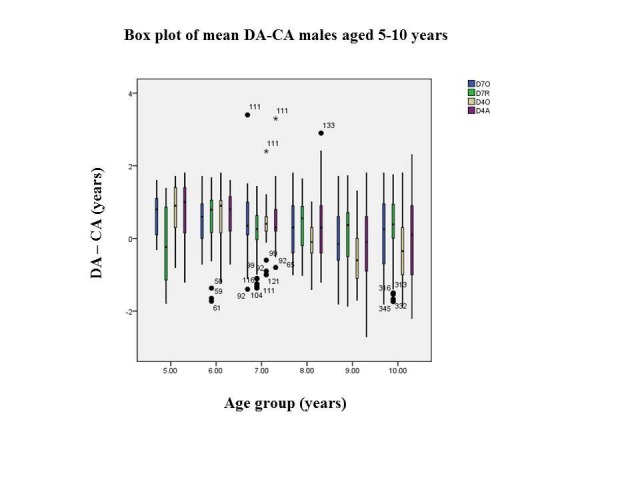
Box-plot of mean DA-CA males aged 5-10 years
Figure 2.
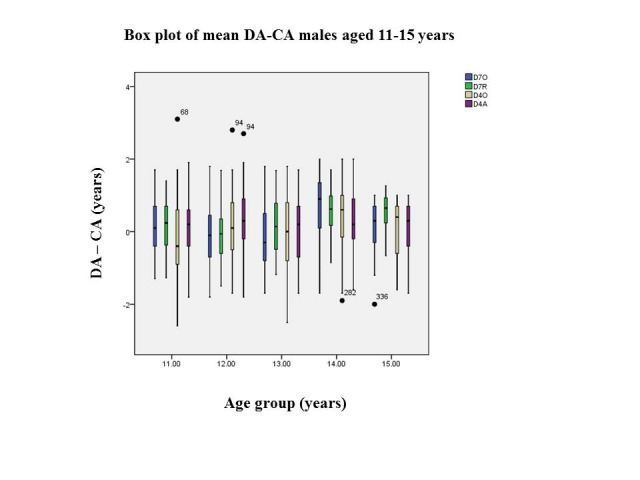
Box-plot of mean DA-CA males aged 11-15 years
Figure 3.
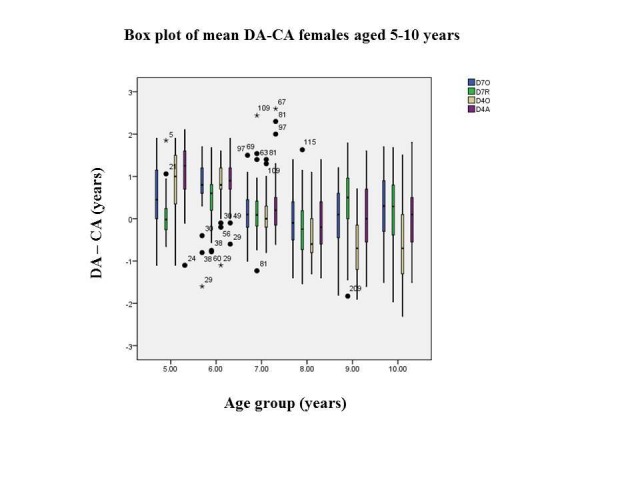
Box-plot of mean DA-CA females aged 5-10 years
Figure 4.
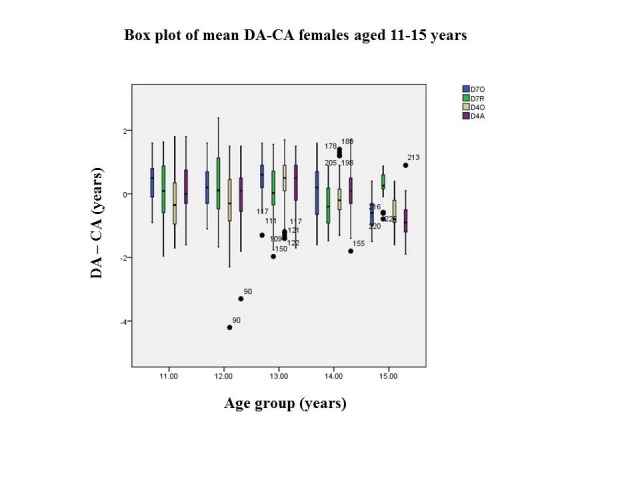
Box-plot of mean DA-CA females aged 11-15 years
Figure 5.
Box-plot of mean DA-CA females aged 11-15 years
RESULTS
The distribution of radiographs by age and gender is presented in Table 1.
Table 1. Distribution of the study sample by age and gender.
| Chronological age (years) | Females | Males | Total | ||||
|---|---|---|---|---|---|---|---|
| Age group | Age range | N | % | N | % | N | % |
| 5 | 5.0 - 5.9 | 24 | 4.79 | 23 | 3.29 | 47 | 3.92 |
| 6 | 6.0 - 6.9 | 39 | 7.78 | 40 | 5.72 | 79 | 6.58 |
| 7 | 7.0 - 7.9 | 46 | 9.18 | 58 | 8.30 | 104 | 8.67 |
| 8 | 8.0 - 8.9 | 50 | 9.98 | 58 | 8.30 | 108 | 9.00 |
| 9 | 9.0 - 9.9 | 55 | 10.98 | 78 | 11.16 | 133 | 11.08 |
| 10 | 10.0 - 10.9 | 55 | 10.98 | 100 | 14.31 | 155 | 12.92 |
| 11 | 11.0 - 11.9 | 40 | 7.98 | 82 | 11.73 | 122 | 10.17 |
| 12 | 12.0 - 12.9 | 55 | 10.98 | 91 | 13.02 | 146 | 12.17 |
| 13 | 13.0 - 13.9 | 57 | 11.38 | 82 | 11.73 | 139 | 11.58 |
| 14 | 14.0 - 14.9 | 59 | 11.78 | 58 | 8.30 | 117 | 9.75 |
| 15 | 15.0 - 15.9 | 21 | 4.19 | 29 | 4.15 | 50 | 4.17 |
| Total sample | 5.0 - 15.9 | 501 | 100 | 699 | 100 | 1200 | 100 |
The mean age (± SD) of the entire sample was 10.75 ± 2.72 years, those of girls and boys being 10.68 ± 2.87 and 10.81 ± 2.60, respectively. Intra- and inter-examiner agreements for Demirjian’s dental staging were 93% and 86% respectively, with Kappa values of 0.90 and 0.81 indicating almost perfect agreement.
In the present study, the mean D7-O dental ages for girls and boys were 11.42 ± 0.14 years and 11.44 ± 0.11 years, respectively. The mean DA-CA values for girls, boys and the total sample (+0.75 ± 1.50, +0.64 ± 1.44 and +0.69 ± 1.46 years, respectively) were statistically significant (p < 0.001). Significant differences between mean DA and CA were observed in all age groups (p < 0.001) except groups 9 and 15 in girls and 9, 12, 13 and 15 in boys (p ≤ 0.05). In girls, the D7-O method overestimated age by +0.17 to +1.12 years in all age groups. In boys, overestimations ranged from +0.16 to +1.34 years (Table 2).
Table 2. Comparison of chronological and D7-O dental ages by gender and age group.
| Gender | Age group (years) | N | CA | DA | DA-CA | p value# |
|---|---|---|---|---|---|---|
| Mean ± SD (years) | ||||||
| GIRLS | 5 | 24 | 5.46 ± 0.33 | 6.51 ± 0.36 | 1.05 ± 0.77 | 0.006 |
| 6 | 39 | 6.57 ± 0.32 | 7.52 ± 0.18 | 0.96 ± 1.01 | <0.001 | |
| 7 | 46 | 7.52 ± 0.26 | 7.99 ± 0.19 | 0.48 ± 1.32 | 0.020 | |
| 8 | 50 | 8.51 ± 0.31 | 8.76 ± 0.17 | 0.26 ± 1.11 | 0.556 | |
| 9 | 55 | 9.48 ± 0.30 | 10.23 ± 0.26 | 0.75 ± 1.93 | 0.010 | |
| 10 | 55 | 10.55 ± 0.32 | 11.37 ± 0.21 | 0.82 ± 1.62 | <0.001 | |
| 11 | 40 | 11.44 ± 0.32 | 12.56 ± 0.27 | 1.12 ± 1.64 | <0.001 | |
| 12 | 55 | 12.49 ± 0.32 | 13.15 ± 0.24 | 0.66 ± 1.86 | 0.004 | |
| 13 | 57 | 13.46 ± 0.30 | 14.56 ± 0.17 | 1.10 ± 1.19 | <0.001 | |
| 14 | 59 | 14.48 ± 0.28 | 15.19 ± 0.18 | 0.71 ± 1.37 | <0.001 | |
| 15 | 21 | 15.48 ± 0.27 | 15.64 ± 0.15 | 0.17 ± 0.64 | 0.192 | |
| Total | 501 | 10.68 ± 2.87 | 11.42 ± 0.14 | 0.75 ± 1.50 | <0.001 | |
| BOYS | 5 | 23 | 5.56 ± 0.29 | 6.90 ± 0.16 | 1.34 ± 0.76 | < 0.001 |
| 6 | 40 | 6.52 ± 0.31 | 7.62 ± 0.23 | 1.10 ± 1.37 | < 0.001 | |
| 7 | 58 | 7.48 ± 0.29 | 8.11 ± 0.12 | 0.63 ± 0.88 | < 0.001 | |
| 8 | 58 | 8.47 ± 0.29 | 9.25 ± 0.16 | 0.79 ± 1.24 | < 0.001 | |
| 9 | 78 | 9.46 ± 0.28 | 9.80 ± 0.20 | 0.34 ± 1.68 | 0.156 | |
| 10 | 100 | 10.45 ± 0.29 | 11.00 ± 0.15 | 0.56 ± 1.53 | 0.001 | |
| 11 | 82 | 11.51 ± 0.30 | 12.20 ± 0.17 | 0.70 ± 1.44 | < 0.001 | |
| 12 | 91 | 12.44 ± 0.30 | 12.98 ± 0.17 | 0.55 ± 1.62 | 0.012 | |
| 13 | 82 | 13.41 ± 0.31 | 13.92 ± 0.20 | 0.52 ± 1.73 | 0.005 | |
| 14 | 58 | 14.47 ± 0.31 | 15.39 ± 0.12 | 0.93 ± 0.93 | < 0.001 | |
| 15 | 29 | 15.24 ± 0.25 | 15.41 ± 0.22 | 0.16 ± 1.17 | 0.051 | |
| Total | 699 | 10.81 ± 2.60 | 11.44 ± 0.11 | 0.64 ± 1.44 | <0.001 | |
| Total sample | 1200 | 10.75 ± 2.72 | 11.44 ± 0.08 | 0.69 ± 1.46 | <0.001 | |
#Wilcoxon Signed Rank test: p ≤ 0.05 = significant
The mean D7-R dental ages for girls and boys were 10.79 ± 2.86 years and 11.05 ± 2.71 years, respectively. The mean DA-CA values for boys, girls and the total sample (+0.24 ± 0.80, +0.11 ± 0.81 and +0.19 ± 0.80 years, respectively) were statistically significant (p < 0.01). Significant differences between mean DA and CA were observed in age groups 6, 8, 9, 12, 14 and 15 in girls and 6, 7, 8, 10, 11, 14 and 15 in boys (p ≤ 0.05). In girls, the D7-R method overestimated age by +0.06 to +0.54 years in all age groups, with the exception of groups 8 and 14, for which underestimations of -0.21 and -0.37 years, respectively, were obtained. In boys, overestimations ranged from +0.15 to +0.59 years in most age groups, with underestimations of -0.13 and -0.02 years in groups 5 and 12, respectively (Table 3).
Table 3. Comparison of chronological and D7-R dental ages by gender and age group.
| Gender | Age group (years) | N | CA | DA | DA-CA | p value# |
|---|---|---|---|---|---|---|
| Mean ± SD (years) | ||||||
| GIRLS | 5 | 24 | 5.46 ± 0.33 | 5.53 ± 0.58 | + 0.07 ± 0.43 | 0.846 |
| 6 | 39 | 6.57 ± 0.32 | 7.11 ± 0.58 | + 0.54 ± 0.38 | < 0.001 | |
| 7 | 46 | 7.52 ± 0.26 | 7.65 ± 0.67 | + 0.13 ± 0.47 | 0.167 | |
| 8 | 50 | 8.51 ± 0.31 | 8.30 ± 0.73 | - 0.21 ± 0.44 | 0.048 | |
| 9 | 55 | 9.48 ± 0.30 | 9.84 ± 0.77 | + 0.36 ± 0.43 | 0.001 | |
| 10 | 55 | 10.55 ± 0.32 | 10.72 ± 0.85 | + 0.17 ± 0.52 | 0.101 | |
| 11 | 40 | 11.44 ± 0.32 | 11.58 ± 0.84 | + 0.14 ± 0.54 | 0.357 | |
| 12 | 55 | 12.49 ± 0.32 | 12.75 ± 0.87 | + 0.26 ± 0.53 | 0.049 | |
| 13 | 57 | 13.46 ± 0.30 | 13.52 ± 0.83 | + 0.06 ± 0.50 | 0.502 | |
| 14 | 59 | 14.48 ± 0.28 | 14.11 ± 0.62 | - 0.37 ± 0.39 | < 0.001 | |
| 15 | 21 | 15.48 ± 0.27 | 15.73 ± 0.51 | + 0.25 ± 0.26 | 0.023 | |
| Total | 501 | 10.68 ± 2.87 | 10.79 ± 2.86 | + 0.11 ± 0.81 | 0.002 | |
| BOYS | 5 | 23 | 5.56 ± 0.29 | 5.43 ± 0.98 | - 0.13 ± 0.42 | 0.503 |
| 6 | 40 | 6.52 ± 0.31 | 7.05 ± 0.78 | + 0.53 ± 0.44 | < 0.001 | |
| 7 | 58 | 7.48 ± 0.29 | 7.72 ± 0.67 | + 0.24 ± 0.46 | 0.004 | |
| 8 | 58 | 8.47 ± 0.29 | 8.89 ± 0.61 | + 0.42 ± 0.97 | < 0.001 | |
| 9 | 78 | 9.46 ± 0.28 | 9.61 ± 0.82 | + 0.15 ± 0.45 | 0.069 | |
| 10 | 100 | 10.45 ± 0.29 | 10.76 ± 0.84 | + 0.31 ± 0.47 | < 0.000 | |
| 11 | 82 | 11.51 ± 0.30 | 11.66 ± 0.70 | + 0.15 ± 0.37 | < 0.001 | |
| 12 | 91 | 12.44 ± 0.30 | 12.42 ± 0.74 | - 0.02 ± 0.45 | 0.541 | |
| 13 | 82 | 13.41 ± 0.31 | 13.56 ± 0.78 | + 0.15 ± 0.36 | 0.106 | |
| 14 | 58 | 14.47 ± 0.31 | 15.06 ± 0.58 | + 0.59 ± 0.46 | < 0.001 | |
| 15 | 29 | 15.24 ± 0.25 | 15.80 ± 0.40 | + 0.56 ± 0.35 | < 0.001 | |
| Total | 699 | 10.81 ± 2.60 | 11.05 ± 2.71 | + 0.24 ± 0.80 | < 0.001 | |
| Total sample | 1200 | 10.75 ± 2.72 | 10.94 ± 2.78 | + 0.19 ± 0.80 | < 0.001 | |
#Wilcoxon Signed Rank test: p ≤ 0.05 = significant
The mean D4-O dental ages for girls and boys were 11.27 ± 0.14 years and 11.60 ± 0.11 years, respectively. The mean DA-CA values for girls, boys and the total sample (0.59 ± 2.77, 0.79 ± 1.59 and 0.72 ± 2.30 years, respectively) were statistically significant (p < 0.05). Significant differences between mean DA and CA were observed in all age groups except 8, 9, 12 and 15 for girls and age groups 9 and 15 for boys (p ≤ 0.05). In girls, the method overestimated age by +0.07 to +1.59 years in all age groups. In boys, overestimations ranged from +0.26 to +1.66 years (Table 4).
Table 4. Comparison of chronological and D4-O dental ages by gender and age group.
| Gender | Age group (years) | N | CA | DA | DA-CA | p value# |
|---|---|---|---|---|---|---|
| Mean ± SD (years) | ||||||
| GIRLS | 5 | 24 | 5.46 ± 0.33 | 7.05 ± 0.27 | 1.59 ± 1.24 | < 0.001 |
| 6 | 39 | 6.57 ± 0.32 | 7.57 ± 0.13 | 1.00 ± 0.84 | < 0.001 | |
| 7 | 46 | 7.52 ± 0.26 | 8.02 ± 0.17 | 0.50 ± 0.96 | 0.003 | |
| 8 | 50 | 8.51 ± 0.31 | 8.58 ± 0.15 | 0.07 ± 0.79 | 0.660 | |
| 9 | 55 | 9.48 ± 0.30 | 9.99 ± 0.26 | 0.51 ± 1.49 | 0.154 | |
| 10 | 55 | 10.55 ± 0.32 | 11.00 ± 0.22 | 0.45 ± 1.76 | 0.048 | |
| 11 | 40 | 11.44 ± 0.32 | 12.11 ± 0.29 | 0.67 ± 2.00 | 0.019 | |
| 12 | 55 | 12.49 ± 0.32 | 12.87 ± 0.25 | 0.38 ± 2.35 | 0.109 | |
| 13 | 57 | 13.46 ± 0.30 | 14.38 ± 0.20 | 0.92 ± 2.95 | < 0.001 | |
| 14 | 59 | 14.48 ± 0.28 | 15.11 ± 0.19 | 0.63 ± 3.13 | < 0.001 | |
| 15 | 21 | 15.48 ± 0.27 | 15.60 ± 0.16 | 0.12 ± 2.71 | 0.313 | |
| Total | 501 | 10.68 ± 2.87 | 11.27 ± 0.14 | 0.59 ± 2.77 | < 0.001 | |
| BOYS | 5 | 23 | 5.56 ± 0.29 | 7.22 ± 0.12 | 1.66 ± 0.55 | < 0.001 |
| 6 | 40 | 6.52 ± 0.31 | 7.78 ± 0.20 | 1.26 ± 0.93 | < 0.001 | |
| 7 | 58 | 7.48 ± 0.29 | 8.10 ± 0.11 | 0.62 ± 0.59 | < 0.001 | |
| 8 | 58 | 8.47 ± 0.29 | 9.28 ± 0.18 | 0.81 ± 1.16 | < 0.001 | |
| 9 | 78 | 9.46 ± 0.28 | 9.72 ± 0.19 | 0.26 ± 1.58 | 0.541 | |
| 10 | 100 | 10.45 ± 0.29 | 11.02 ± 0.17 | 0.57 ± 1.68 | < 0.001 | |
| 11 | 82 | 11.51 ± 0.30 | 12.40 ± 0.18 | 0.89 ± 1.87 | < 0.001 | |
| 12 | 91 | 12.44 ± 0.30 | 13.42 ± 0.18 | 0.86 ± 1.97 | < 0.001 | |
| 13 | 82 | 13.41 ± 0.31 | 14.24 ± 0.19 | 0.65 ± 1.85 | < 0.001 | |
| 14 | 58 | 14.47 ± 0.31 | 15.16 ± 0.10 | 0.69 ± 0.90 | < 0.001 | |
| 15 | 29 | 15.24 ± 0.25 | 15.50 ± 0.26 | 0.26 ± 1.08 | 0.051 | |
| Total | 699 | 10.81 ± 2.60 | 11.60 ± 0.11 | 0.79 ± 1.59 | < 0.001 | |
| Total sample | 1200 | 10.75 ± 2.72 | 11.47 ± 0.08 | 0.72 ± 2.30 | < 0.001 | |
#Wilcoxon Signed Rank test: p ≤ 0.05 = significant
The mean D4-A dental ages for girls and boys were 9.57 ± 0.11 years and 11.28 ± 0.11 years, respectively. The mean DA-CA values for girls, boys and the total sample (1.20 ± 1.10, 1.31 ± 1.07 and 1.26 ± 1.08 years, respectively) were statistically significant (p < 0.05). Significant differences between mean DA and CA were observed in all age groups except 7, 10, 11 and 13 for girls and 9, 10 and 11 for boys (p ≤ 0.05). In girls, the method overestimated age by +0.60 to +1.69 years in all age groups. In boys, overestimations ranged from +0.70 to +1.67 years (Table 5).
Table 5. Comparison of chronological and D4-A dental ages by gender and age group.
| Gender | Age group (years) | N | CA | DA | DA-CA | p value# |
|---|---|---|---|---|---|---|
| Mean ± SD (years) | ||||||
| GIRLS | 5 | 24 | 5.46 ± 0.33 | 6.87 ± 0.25 | 1.69 ± 1.21 | < 0.001 |
| 6 | 39 | 6.57 ± 0.32 | 7.54 ± 0.14 | 1.05 ± 0.68 | < 0.001 | |
| 7 | 46 | 7.52 ± 0.26 | 7.73 ± 0.14 | 0.77 ± 1.05 | 0.122 | |
| 8 | 50 | 8.51 ± 0.31 | 8.18 ± 0.12 | 0.75 ± 0.64 | < 0.001 | |
| 9 | 55 | 9.48 ± 0.30 | 8.90 ± 0.20 | 1.36 ± 1.43 | < 0.001 | |
| 10 | 55 | 10.55 ± 0.32 | 10.04 ± 0.24 | 1.21 ± 1.18 | 0.016 | |
| 11 | 40 | 11.44 ± 0.32 | 11.26 ± 0.32 | 1.38 ± 1.27 | 0.595 | |
| 12 | 55 | 12.49 ± 0.32 | 11.52 ± 0.31 | 1.58 ± 1.18 | 0.021 | |
| 13 | 57 | 13.46 ± 0.30 | 11.57 ± 0.38 | 1.40 ± 0.93 | 0.002 | |
| 14 | 59 | 14.48 ± 0.28 | 10.11 ± 0.40 | 1.22 ± 0.99 | < 0.001 | |
| 15 | 21 | 15.48 ± 0.27 | 9.02 ± 0.57 | 0.60 ± 0.37 | < 0.001 | |
| Total | 501 | 10.68 ± 2.87 | 9.57 ± 0.11 | 1.20 ± 1.10 | < 0.001 | |
| BOYS | 5 | 23 | 5.56 ± 0.29 | 7.21 ± 0.11 | 1.67 ± 0.57 | < 0.001 |
| 6 | 40 | 6.52 ± 0.31 | 7.75 ± 0.16 | 1.31 ± 1.10 | < 0.001 | |
| 7 | 58 | 7.48 ± 0.29 | 8.01 ± 0.08 | 0.70 ± 0.73 | < 0.001 | |
| 8 | 58 | 8.47 ± 0.29 | 8.76 ± 0.15 | 1.14 ± 1.11 | 0.343 | |
| 9 | 78 | 9.46 ± 0.28 | 9.23 ± 0.18 | 1.25 ± 1.18 | 0.002 | |
| 10 | 100 | 10.45 ± 0.29 | 10.40 ± 0.17 | 1.37 ± 1.13 | 0.137 | |
| 11 | 82 | 11.51 ± 0.30 | 11.84 ± 0.22 | 1.37 ± 1.22 | 0.414 | |
| 12 | 91 | 12.44 ± 0.30 | 13.04 ± 0.21 | 1.50 ± 1.17 | 0.007 | |
| 13 | 82 | 13.41 ± 0.31 | 14.11 ± 0.21 | 1.57 ± 1.07 | < 0.001 | |
| 14 | 58 | 14.47 ± 0.31 | 15.61 ± 0.11 | 1.30 ± 0.57 | < 0.001 | |
| 15 | 29 | 15.24 ± 0.25 | 15.65 ± 0.21 | 0.96 ± 0.87 | 0.002 | |
| Total | 699 | 10.81 ± 2.60 | 11.28 ± 0.11 | 1.31 ± 1.07 | < 0.001 | |
| Total sample | 1200 | 10.75 ± 2.72 | 10.56 ± 0.09 | 1.26 ± 1.08 | 0.322 | |
#Wilcoxon Signed Rank test: p ≤ 0.05 = significant
Significant gender-based differences were observed in mean DA-CA with the D7-R and D4-O methods (p = 0.005 and < 0.001, respectively), but not with the D7-O and D4-A methods (p > 0.05). With both the D7-R and D4-O methods, the mean DA-CA was significantly lower in girls than in boys (Table 6).
Table 6. Intra-method comparison between genders of mean DA-CA.
| Gender | N | D7-O | D7-R | D4-O | D4-A | ||||
|---|---|---|---|---|---|---|---|---|---|
|
Mean DA-CA ± SD (years) |
p value |
Mean DA-CA ± SD (years) |
p value |
Mean DA-CA ± SD (years) |
p value |
Mean DA-CA ± SD (years) |
p value | ||
| Girls | 501 | 0.75 ± 1.50 | 0.200 | + 0.11 ± 0.81 | 0.005 | 0.59 ± 2.77 | <0.001 | 1.20 ± 1.10 | 0.083 |
| Boys | 699 | 0.64 ± 1.44 | + 0.24 ± 0.80 | 0.79 ± 1.59 | 1.31 ± 1.07 | ||||
Independent t-test; p≤ 0.05 = significant
Strong linear correlations were observed between CA and DA for girls, boys and the total sample with all methods (Table 7).
Table 7. Correlation between chronological and dental ages by method used.
| Method | r / p values | Females | Males | Total sample |
|---|---|---|---|---|
| D7-O | r value | 0.965 | 0.950 | 0.959 |
| p value | < 0.001 | < 0.001 | < 0.001 | |
| D7-R | r value | 0.957 | 0.962 | 0.961 |
| p value | < 0.001 | < 0.001 | < 0.001 | |
| D4-O | r value | 0.960 | 0.954 | 0.958 |
| p value | < 0.001 | < 0.001 | < 0.001 | |
| D4-A | r value | 0.959 | 0.947 | 0.953 |
| p value | < 0.001 | < 0.001 | < 0.001 |
Spearman’s rank correlation coefficient: r = Spearman’s rho, p = significant
An inter-method comparison of mean DA-CA values revealed statistically significant (p < 0.05) differences in girls, boys and the total sample (Table 8).
Table 8. Inter-method comparison of the accuracy of age estimation.
| Method with mean DA-CA | Difference in mean DA-CA | 95% CI of DA-CA | Absolute difference | p value# | ||
|---|---|---|---|---|---|---|
| (years ± SD) | Years | |||||
| Girls (N = 501) | D7-O | D7-R | -0.64 ± 0.84 | 0.049 to 0.197 | 0.51 | 0.004 |
| D4-O | -0.16 ± 0.84 | -0.417 to -0.269 | 0.68 | < 0.001 | ||
| D7-R | D4-O | 0.48 ± 1.10 | -0.315 to -0.123 | 0.86 | < 0.001 | |
| D4-A | 0.96 ± 0.97 | -0.045 to 0.125 | 0.69 | 0.983 | ||
| D4-O | D4-A | 0.61 ± 0.66 | 0.202 to 0.317 | 0.50 | < 0.001 | |
| D4-A | D7-O | -0.45 ± 0.65 | 0.026 to 0.140 | 0.48 | 0.001 | |
| Boys (N = 699) | D7-O | D7-R | 0.40 ± 0.87 | 0.000 to 0.286 | 0.47 | 0.077 |
| D4-O | 0.15 ± 0.90 | -0.162 to 0.043 | 0.72 | 0.277 | ||
| D7-R | D4-O | 0.55 ± 1.02 | -0.393 to -0.158 | 0.81 | < 0.001 | |
| D4-A | 1.07 ± 1.01 | -0.155 to 0.075 | 0.74 | 0.359 | ||
| D4-O | D4-A | 0.52 ± 0.83 | 0.126 to 0.249 | 0.65 | < 0.001 | |
| D4-A | D7-O | -0.67 ± 0.83 | -0.149 to 0.020 | 0.61 | 0.042 | |
| Total (N = 1200) | D7-O | D7-R | -0.50 ± 0.86 | -0.035 to 0.0.62 | 0.48 | 0.773 |
| D4-O | 0.03 ± 0.88 | -0.287 to -0.187 | 0.70 | < 0.001 | ||
| D7-R | D4-O | 0.53 ± 1.05 | -0.283 to -0.164 | 0.83 | < 0.001 | |
| D4-A | 1.07 ± 0.99 | -0.062 to -0.050 | 0.72 | 0.615 | ||
| D4-O | D4-A | 0.54 ± 0.76 | -0.174 to 0.261 | 0.59 | < 0.001 | |
| D4-A | D7-O | -0.57 ± 0.76 | -0.023 to 0.063 | 0.55 | 0.506 | |
# Wilcoxon Signed-rank test; p≤ 0.05 = significant
DISCUSSION
The Demirjian method (2) has been the most widely tested method for the estimation of the dental age of children and adolescents. However, only three studies have compared Demirjian’s original and revised seven-tooth methods, four-tooth method and alternate four-tooth method, (3-5) none of them conducted on an Indian population. Hence, the present study aimed to compare the applicability of these four methods to age estimation of a sample of 1200 Indian children - 501 female and 699 male - aged 5 to 15 years, selected by a convenience sampling method. This method is preferred by most researchers because it is fast, inexpensive and easy and the subjects are conveniently accessible.
Radiographic views of the developing maxillary permanent teeth are often obstructed by bony structures of the maxilla. The teeth of the mandible, on the other hand, are quite clearly visible in an OPG. Hence, only the mandibular teeth were evaluated in the present study, as in some other studies. (1, 4, 6) Since it has been well-established that a very high degree of symmetry exists between the teeth of the left and right sides, (1, 6, 7) only the mandibular teeth of the left quadrant were assessed. Third molar germs were excluded from assessment because of the high degree of variability observed in the genesis and development of these teeth. (8, 9) Further, studies have reported no improvement in accuracy of age estimation methods when the developmental status of the third molar was included. (10)
While assessing dental age, it is important to consider not only the proximity of the estimated age to the actual or chronological age, but also the reproducibility of the age estimation method. In the present study, agreements within and between examiners for Demirjian’s method of dental staging were obtained in percentages and measured by Cohen’s kappa coefficient, which is a more robust measure than simple percentage agreement calculation, taking into account the agreement occurring by chance. (11) Intra- and inter-examiner agreements for Demirjian’s dental staging were observed to be 90% and 91%, respectively, with a kappa coefficient of 0.83. The difference in mean DA-CA was not significant between two assessments by one examiner or between two examiners. Other studies have reported kappa values ranging from 0.67 to 0.96 for intra-examiner agreements (12, 13) and from 0.68 to 0.92 for inter-examiner agreements. (14, 15)
In the present study, overall as well as by age group, a significant difference was observed between the mean DA and CA with all four methods in both genders, a finding which is in agreement with the observations of Flood et al. (4) in a South Australian population. However, in an earlier study by Flood et al. (5) on a Western Australian population, no significant differences between the mean DA and CA were observed overall in males, with all but the Demirjian’s original seven-tooth method. In females, overall significant differences were observed with all except the four-tooth method.
Phillips reported an overestimation of age by an average of 0.89 years using the original seven-tooth method on Tygerberg dental patients; a random mixture of Caucasoid and Khoisanoid children. He also observed similar overestimations in samples of Indian and Negroid children from Kwa-Zulu Natal. He derived correction factors and found them to improve the accuracy of method significantly. (16, 17) The Demirjian’s revised seven-tooth method has been reported to consistently overestimate age in various populations by up to +1.23 years in males and +1.20 years in females. (18) A study by Flood et al. reported overestimations of +0.61 years (m) and +0.75 years (f), +0.49 years (m) and +0.47 years (f), +0.31 years (m) and +0.62 years (f) and +0.49 years (m) and +0.70 years (f), using the original seven-tooth, revised seven-tooth, four-tooth and alternate four-tooth standards, respectively, in a South Australian population. (4) Another study by Flood et al. reported overestimations of +0.51 years (m) and +0.63 years (f), +0.19 years (m) and +0.41 years (f), +0.04 years (m) and +0.25 years (f) and -0.20 years (m) and +0.37 years (f), using the original seven-tooth, revised seven-tooth, four-tooth and alternate four-tooth standards, respectively, in a Western Australian population. (5) A similar study by Akkaya et al. reported overestimations of +0.53 years (m) and +0.66 years (f), +0.33 years (m) and +0.62 years (f), +0.21 years (m) and +0.57 years (f) and +0.08 years (m) and +0.61 years (f), using the original seven-tooth, revised seven-tooth, four-tooth and alternate four-tooth standards, respectively, in a Turkish population. (3) In the present study overestimations were obtained, of +0.64 years (m) and +0.75 years (f), +0.24 years (m) and +0.11 years (f), +0.79 years (m) and +0.59 years (f) and +1.31 years (m) and +1.20 years (f), using the original seven-tooth, revised seven-tooth, four-tooth and alternate four-tooth standards, respectively.
Significant gender-based differences were observed with the D7-R and D4-O methods in the present study dental age of girls being more advanced than that of boys. This gender difference has been attributed to the faster biological and dental maturation in girls, which leads to a higher DA compared to CA. (19) However, some other studies (13, 20) have reported a higher DA compared to CA in boys than in girls.
Several factors can affect the accuracy or precision of an age estimating method, such as the quality of the reference material (sample), reliability of the method and biological variability in dental development. (21, 22) Hence, no age estimation method can be expected to predict the exact age of every individual. Differences between chronological and estimated ages of up to 12 months can be considered to be within normal standards, (23) although smaller intervals are desirable. (24) In the present study, mean prediction errors ranged from 1.32 to 15.72 months.
CONCLUSION
From the results of this study, it was concluded that all the four Demirjian methods overestimated age. The revised seven-tooth standards most accurately predicted the age of the study sample (mean prediction error = 2.28 months), followed by the original seven-tooth, four-tooth and alternate four-tooth standards. The Demirjian original seven-tooth method was significantly more accurate in boys compared to girls, while the reverse was true for the Demirjian revised seven-tooth and Demirjian original four-tooth methods. The Demirjian alternate four-tooth method was almost equally accurate in both genders. Significant differences between dental age and chronological age were observed with all the methods.
Footnotes
CONFLICT OF INTEREST: Authors have declared that no competing interests exist.
REFERENCES
- 1.Demirjian A, Goldstein H, Tanner JM. A new system of dental age assessment. Hum Biol. 1973. May;45(2):211–27. [PubMed] [Google Scholar]
- 2.Demirjian A, Goldstein H. New systems for dental maturity based on seven and four teeth. Ann Hum Biol. 1976. Sep;3(5):411–21. 10.1080/03014467600001671 [DOI] [PubMed] [Google Scholar]
- 3.Akkaya N, Yilanci HÖ, Göksülük D. Applicability of Demirjian’s four methods and Willems method for age estimation in a sample of Turkish children. Leg Med (Tokyo). 2015. Sep;17(5):355–9. 10.1016/j.legalmed.2015.04.003 [DOI] [PubMed] [Google Scholar]
- 4.Flood SJ, Franklin D, Turlach BA, McGeachie J. A comparison of Demirjian’s four dental development methods for forensic age estimation in south Australian sub-adults. J Forensic Leg Med. 2013. Oct;20(7):875–83. 10.1016/j.jflm.2013.07.002 [DOI] [PubMed] [Google Scholar]
- 5.Flood SJ, Mitchell WJ, Oxnard CE, Turlach BA, McGeachie J. A Comparison of Demirjian’s Four Dental Development Methods for Forensic Age Assessment. J Forensic Sci. 2011. Nov;56(6):1610–5. 10.1111/j.1556-4029.2011.01883.x [DOI] [PubMed] [Google Scholar]
- 6.Nolla CM. The development of the permanent teeth. ASDC J Dent Child. 1960;27:254–66. [Google Scholar]
- 7.Pinney LC. Calcification and development of mandibular teeth. In: thesis, Ann Arbor, University of Michigan; 1939: 59 p. [Google Scholar]
- 8.Nanda RS. Agenesis of the third molar in man. Am J Orthod. 1954;40(9):698–706. 10.1016/0002-9416(54)90058-5 [DOI] [Google Scholar]
- 9.Hellman M. Our third molar teeth, their eruption, presence and absence. Dent Cosmos. 1936;78:750. [Google Scholar]
- 10.Ramanan N, Thevissen P, Fieuws S, Willems G. Dental age estimation in Japanese individuals combining permanent teeth and third molars. J Forensic Odontostomatol. 2012;30(2):34–9. [PMC free article] [PubMed] [Google Scholar]
- 11.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977. Mar;33(1):159–74. 10.2307/2529310 [DOI] [PubMed] [Google Scholar]
- 12.Chen JW, Guo J, Zhou J, Liu RK, Chen TT, Zou SJ. Assessment of dental maturity of western Chinese children using Demirjian’s method. Forensic Sci Int. 2010. Apr 15;197(1-3):119.e1–4. 10.1016/j.forsciint.2009.12.009 [DOI] [PubMed] [Google Scholar]
- 13.Leurs IH, Wattel E, Aartman IH, Etty E, Prahl-Andersen B. Dental age in Dutch children. Eur J Orthod. 2005. Jun;27(3):309–14. 10.1093/ejo/cji010 [DOI] [PubMed] [Google Scholar]
- 14.Javadinejad S, Sekhavati H, Ghafari R. A comparison of the accuracy of four age estimation methods based on panoramic radiography of developing teeth. J Dent Res Dent Clin Dent Prospects. 2015. Spring;9(2):72–8. 10.15171/joddd.2015.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Feijóo G, Barbería E, De Nova J, Prieto JL. Permanent teeth development in a Spanish sample. Application to dental age estimation. Forensic Sci Int. 2012. Jan 10;214(1-3):213.e1–6. 10.1016/j.forsciint.2011.08.024 [DOI] [PubMed] [Google Scholar]
- 16.Phillips VM, van Wyk Kotze T. Dental age related tables for children of various ethnic groups in South Africa. J Forensic Odontostomatol. 2009;27(2):29–44. [PubMed] [Google Scholar]
- 17.Pinchi V, Gian-Aristide N, Pradella F, Vitale G, Rugo D, Nieri M. Comparison of the applicability of four odontological methods for age estimation of the 14 years legal threshold in a sample of Italian adolescents. J Forensic Odontostomatol. 2012;30(2):17–25. [PMC free article] [PubMed] [Google Scholar]
- 18.Abu Asab S, Noor SN, Khamis MF. The accuracy of Demirjian method in dental age estimation of Malay children. Singapore Dent J. 2011;32(1):19–27. 10.1016/S0377-5291(12)70012-3 [DOI] [PubMed] [Google Scholar]
- 19.Baghdadi ZD. Dental maturity in Saudi children using the Demirjian method: a comparative study and new prediction models. ISRN Dent. 2013;2013:390314. Epub 2013 Feb 26. 10.1155/2013/390314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gupta S, Mehendiratta M, Rehani S, Kumra M, Nagpal R, Gupta R. Age estimation in Indian children and adolescents in the NCR region of Haryana: a comparative study. J Forensic Dent Sci. 2015. Sep-Dec;7(3):253–8. 10.4103/0975-1475.172453 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Staaf V, Mörnstad H, Welander U. Age estimation based on tooth development: A test of reliability and validity. Scand J Dent Res. 1991. Aug;99(4):281–6. [DOI] [PubMed] [Google Scholar]
- 22.Bagić IČ, Sever N, Brkić H, Kern J. Dental age estimation in children using orthopantomograms. Acta Stomatol Croat. 2008;42(1):11–8. [Google Scholar]
- 23.Moraes ME, Bastos MS, Santos LR, Castilho JC, Moraes LC, Medici Filho E. Dental age in patients with down syndrome. Braz Oral Res. 2007. Jul-Sep;21(3):259–64. 10.1590/S1806-83242007000300012 [DOI] [PubMed] [Google Scholar]
- 24.Chaillet N, Nyström M, Demirjian A. Comparison of dental maturity in children of different ethnic origins: international maturity curves for clinicians. J Forensic Sci. 2005. Sep;50(5):1164–74. 10.1520/JFS2005020 [DOI] [PubMed] [Google Scholar]