

Abstract
Objectives:
The aim of this study was to compare the reproducibility of skeletal maturation assessments by raters with similar orthodontic experience using hand-wrist (HW) and cervical vertebral maturation (CVM) methods.
Methods:
HW and lateral cephalometric radiographs from 15 subjects (8 males and 7 females; ages, 9–16 years) were selected randomly. HW skeletal maturation was evaluated by the method of Greulich and Pyle, and CVM staging was evaluated by the method of Baccetti et al. Six orthodontic residents evaluated all images at three time periods: T1, initial evaluation; T2, re-evaluation after 7 days and T3, final evaluation after 5 weeks. Intra- and interexaminer reproducibility was evaluated with the intraclass correlation coefficient; the limits of agreement (LoA) were determined by using the Bland–Altman method.
Results:
The intraexaminer reliability assessed by intraclass correlation coefficient was scored as good for both of methods (T1-T2-T3 HW = 0.89 and CVM = 0.80; T1-T2 HW = 0.87 and CVM = 0.77; T2-T3 HW0 = 0.90 and CVM = 0.81), as well as the interexaminer evaluation, with the exception of HW-T1, which scored excellent (0.92). The width of LoA from Bland–Altman plot of cervical vertebra method was narrower (CVM T1-T2: −2.3 and +1.8; CVM T2-T3: −2.0 and +2.0) than the HW method (HW T1-T2: −3.9 and +4.8; HW T2-T3: −4.0 and +3.5).
Conclusions:
Both HW and CVM methods presented good reproducibility for intra- and interexaminer correlation assessments. The small LoA indicated that the CVM is a reproducible method.
Introduction
The prediction of the pubertal growth spurt is a widely used tool for the orthodontic and dentofacial orthopedic therapy of growing individuals, in that such knowledge helps determine optimal treatment timing when growth modification is considered.1, 2 In this way, the identification of the maturational stage is indispensable for the diagnosis and treatment planning of patients with imbalances in their facial growth pattern as it determines the favorable intervention time and treatment approach.2
Although physiological parameters such as pubertal signs, chronological age and dental staging are classic skeletal maturity indicators3, 4 that might indicate the individual stage of skeletal development, these parameters have not proven to be reliable methods of evaluation due to the wide range of individual patterns observed.4, 5
Both hand-wrist (HW)6–10 and cervical vertebrae maturation (CVM)11–16 methods have been evaluated extensively in the literature.1, 2,17,18 Previous studies demonstrated a significant correlation between HW and CVM stages,17, 19 supporting the validity of CVM to determine the stage of skeletal maturation. In addition to validity, it is expected that diagnostic tests demonstrate adequate reliability, once its measurements can be repeated by the same or different observers.20 A recent systematic review of the literature on the present study topic included studies where intraexaminer and interexaminer correlation tests were performed on expert examiners.21
The decision to not obtain a HW radiograph should be based on a CVM method that is superior to, or at least as efficient as the former. Considering that reliability assessments are susceptible to variations in study subjects, samples and observers,22 each method should be assessed and compared in order to help clinicians during the decision-making process, also taking into consideration their limitations for predicting individual subject’s skeletal maturation in clinical practice.9
Therefore, the objective of the present study was to evaluate how orthodontic residents can reproduce a method to assess individual skeletal stage of development and other for skeletal stage prediction, assessed by HW and cervical vertebrae (projections obtained from cone beam CT, CBCT) respectively.
Methods and materials
Sample
This project was approved by the research ethics committee of the Institute of Collective Health Studies from the Universidade Federal do Rio de Janeiro, Brazil. The sample included HW radiographs as well as lateral cephalograms reconstructed from cone beam CT (CBCT) scans of subjects who already had these records available due to previous acquisition for orthodontic diagnosis and treatment planning purposes (no treatment had been rendered yet at the time of data acquisition).
Sample size calculation guidelines for reproducibility studies was performed according to Walter et al23 where ρ0 = 0.5, ρ1 = 0.9, α = 0.05 and β = 0.2. Considering the reference values for five examiners at the conditions above cited, the minimum sample size required was 4.7, or 5 subjects after rounding up. The sample consisted of HW radiographs and perspective lateral cephalometric projections of 15 randomly selected patients (8 males and 7 females; ages, 9–16 years) from the Orthodontic Clinic of the Graduate course in Dentistry of the Universidade Federal do Rio de Janeiro in Brazil. The study inclusion criteria were: availability of CBCT Digital Imaging and Communications in Medicine files which field of view included full fourth cervical vertebra that allowed generation of lateral cephalograms; HW radiographs also had to be available. All subjects were in good health with an absence of any craniofacial syndrome or systemic growth abnormalities.
HW radiographs acquisition was carried out following an established protocol: the left hand was in contact with the film with the long axis of the middle finger aligned with the forearm. Fingers were separated from each other, and the thumb was oriented at approximately 30° relative to the forefinger. The X-ray tube was centralized on the third metacarpal.
For CVM assessment, two-dimensional lateral cephalometric radiographs perspective projections were obtained from the available CBCT scans using Dolphin Imaging software (v. 11.5, Dolphin Imaging & Management Solutions, Chatsworth, CA). CBCT scans were performed on an i-CAT scanner (Imaging Sciences International, Hatfield, PA) in accordance with standard acquisition parameters (120 kV, 5 mA, 13 × 17 cm field of view, 0.4 mm voxel and 20 s scanning time), with the patient in the upright position, Frankfort horizontal plane parallel to the ground and in maximum intercuspation.
The HW and cephalometric lateral radiographs were distributed randomly to six orthodontic residents for skeletal stage determination. They were previously instructed on how to perform both evaluations of the HW and cervical vertebra maturation methods. The training consisted of explanatory presentations containing systematic observational schemes, illustrations and radiographic images referring to examples of the maturation stages for each method. They also performed the evaluation in five cases not included in the sample.
Hand-wrist and cervical vertebrae evaluation
Both HW and lateral cephalometric radiographs images were stored as high-resolution image files. Each examiner received the material regarding the three measurements periods: T1, first evaluation; T2, second evaluation after 7 days and T3, third evaluation after 5 weeks. The sequence of images was altered randomly in consecutive evaluations. The observers were blinded for both HW and lateral cephalometric radiographs as to patients’ information and chronologic ages, with exception of their gender. All the exams were analyzed in a desktop computer in a darkened room.
The hand and wrist bones of each subject were compared visually with the standard radiographs (from subjects of the same sex) proposed by the method of Greulich and Pyle24. The Greulich and Pyle Atlas24 provides a series of radiographic standards of the hand and wrist from birth to 17/18 years for females and 19 years for males. The assessment of skeletal maturation consists of the comparison between the patient’s radiographic image with the closest matching standard from the Atlas.24 The standards were selected for the study according to the sample characteristics and ranged from standard 14 to 30 (corresponding to males between 5 and 18 years of age) and from standard 14 to 27 (corresponding to females in a similar age range; Figure 1).
Figure 1.

Patient’s hand-wrist radiograph and corresponding standard from Greulich and Pyle Atlas.24 (a) 9-year-old subject. (b) 12-year-old subject. (c) 15-year-old subject.
The morphology of the second, third and fourth cervical vertebrae (C2, C3 and C4) were classified visually according to the method proposed by Baccetti et al12 that scores Stages from 1 through 6, referring to pre-pubertal (Stages 1 and 2), pubertal growth spurt (Stages 3 and 4) and post-pubertal phases (Stages 5 and 6; Figure 2).
Figure 2.
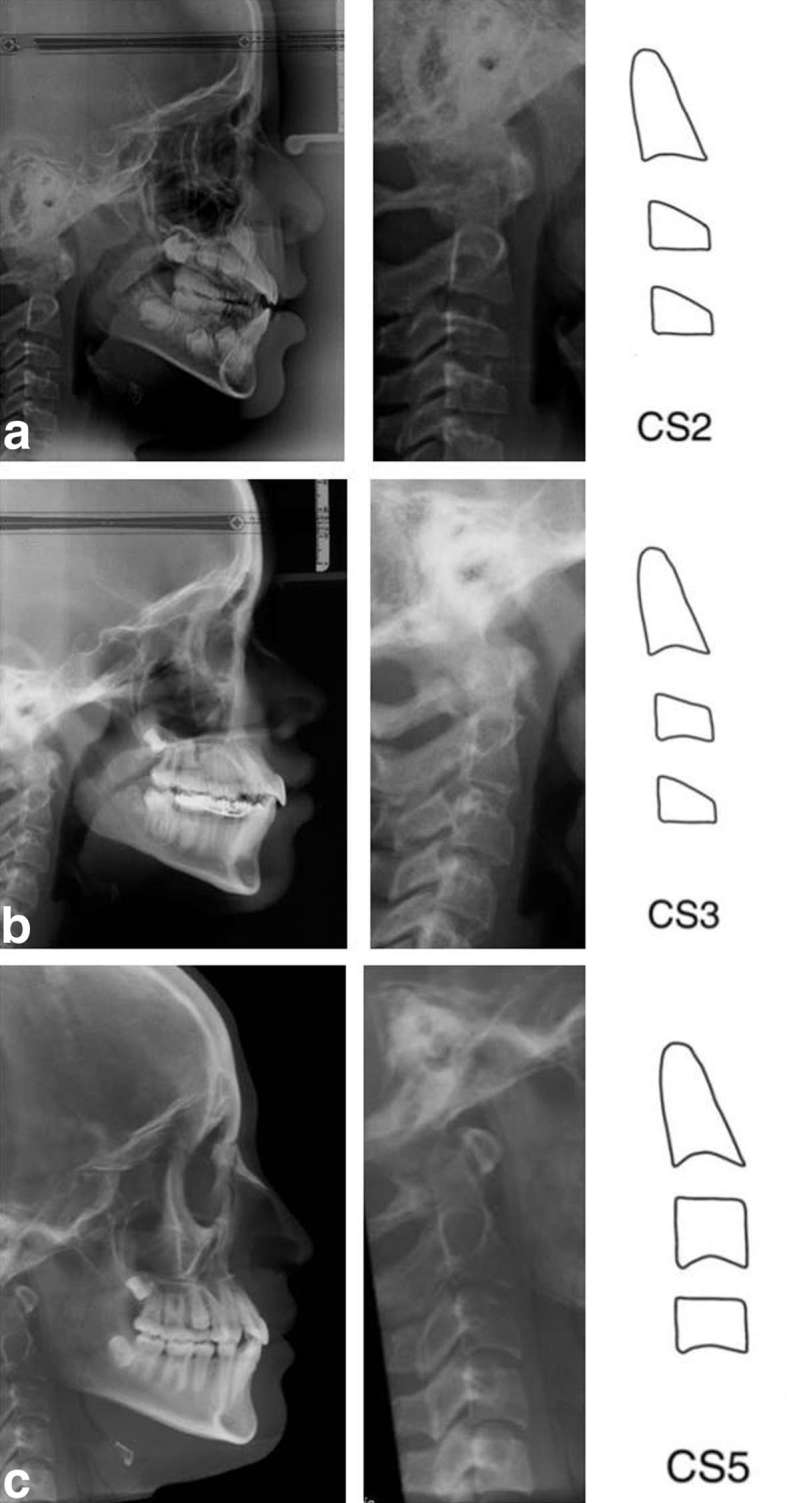
Patient’s lateral cephalometric radiograph (full size and closer view) with the correspondent schematic stage from Baccetti et al.12(a) 9-year-old subject. (b) 12-year-old subject. (c,) 15-year-old subject.
Statistical analysis
Statistical analysis was performed with the MedCalc statistical package (v. 14.10.2; MedCalc Software, Ostend, Belgium, http://www.medcalc.org). Intraexaminer reproducibility was tested using intraclass correlation coefficient (ICC).
Agreement between the repeated measurements was presented graphically via the Bland–Altman method, a statistical approach that is based on the quantification of the agreement between two quantitative measurements by studying the difference against their mean and estimating limits of agreement (LoA). A plot was created, with the difference of the two paired measurements plotted against the mean of the two measurements (HW and CVM). The analysis is based on calculating the standard deviation of differences between repeated measurements and the standard deviation of the differences between the means for each method separately. In a normally distributed sample, 95% of the differences will lie between the LoA, within ± 2 standard deviations from the mean difference.25
The interexaminer reproducibility was evaluated with the ICC by comparing their scores considering the three measurements periods. The results were classified according to the ICC value in: excellent, above 0.9; good, between 0.75 and 0.9; moderate, between 0.5 and 0.75; and poor, below 0.5.26 The degree of agreement of each method was evaluated through the Bland–Altman’s plot interpretation.
Results
The results for intraexaminer and interexaminer reproducibility estimated by ICC for each method are shown in Table 1. For both intraexaminer and interexaminer evaluations, the HW method presented higher ICC values in comparison to the cervical vertebra method. However, the reliability for both of methods was scored as good in all of the intraexaminer evaluations (T1-T2-T3 HW = 0.89 and CVM = 0.80; T1-T2 HW = 0.87 and CVM = 0.77; T2-T3 HW0 = 0.90 and CVM = 0.81). In the interexaminer evaluation, with the exception of HW in the first measurement, which scored excellent (0.92), all of the other evaluations were scored as good (T1 HW = 0.92 and CVM0 = 0.81; T2 HW = 0.81 and CVM = 0.76; T3 = 0.88 and CVM = 0.81).
Table 1.
Intra- and interexaminer reliability with 95% confidence intervals estimated for each measurement, by the ICC method
| Method | Intraexaminer reproducibility | ||||||||
| T1-T2-T3 | T1-T2 | T2-T3 | |||||||
| ICC | Lower 95% CI | Upper 95% CI | ICC | Lower 95% CI | Upper 95% CI | ICC | Lower 95% CI | Upper 95% CI | |
| Hand-wrist | 0.89 | 0.85 | 0.92 | 0.87 | 0.81 | 0.91 | 0.90 | 0.85 | 0.93 |
| CVM | 0.80 | 0.73 | 0.85 | 0.77 | 0.68 | 0.84 | 0.81 | 0.72 | 0.87 |
| Interexaminer reproducibility | |||||||||
| T1 | T2 | T3 | |||||||
| ICC | Lower 95% CI | Upper 95% CI | ICC | Lower 95% CI | Upper 95% CI | ICC | Lower 95% CI | Upper 95% CI | |
CI, confidence interval; CVM, cervical vertebrae maturation; ICC, intraclass correlation coefficient; T1, first measurement; T2, second measurement; T3, third measurement.
The results for the Bland–Altman test are shown in Figure 3. Both of the methods compared presented small LoA for all of the measurements evaluated. The width of LoA of cervical vertebra method was narrower (CVM T1-T2: −2.3 and +1.8; CVM T2-T3: −2.0 and +2.0) than the HW method (HW T1-T2: −3.9 and +4.8; HW T2-T3: −4.0 and +3.5).
Figure 3.

Bland–Altman plots for intraexaminer HW and cervical vertebra methods comparison of agreement. Dotted lines represent 95% limits of agreement. (a) HW method in T1 and T2. (b) HW method in T2 and T3. (c) Cervical vertebra method in T1 and T2. (d) Cervical vertebra method in T2 and T3. T1, first measurement; T2, second measurement; T3, third measurement; HW, hand-wrist; CVM, cervical vertebra; SD, standard deviation.
Most of the differences lied between the mean difference and ±1.96 SD, indicating a normally distributed sample. Also, the mean difference was close to zero in both of the methods (HW T1-T2: +0.5; HW T2-T3: −0.2; CVM T1-T2: −0.2; CVM T2-T3: 0.0). The HW method presented a higher range of variation through the measurements (0.7) in comparison with the CVM method (0.2).
Discussion
Of critical importance in the diagnosing and treatment planning of an orthodontic patient is the determination of maturational stage, particularly during the adolescent period. Two commonly used methods involve either comparing radiographs of the hand and wrist to standardized images in an Atlas24, 27 or by assessing indicators related to the pubertal growth curve by evaluating the morphology of the second, third and fourth cervical vertebrae.28, 29 The progressive modifications in the size and shape observed on these three vertebral bodies30, 31 have motivated investigations on the use of lateral cephalometric radiographs for cervical vertebra methods of determining skeletal maturation.11–13 A considerable advantage of the CVM method is the avoidance of additional radiation exposure in children, especially when a lateral cephalometric radiograph or CBCT imaging has been requested.
This study recruited orthodontic residents as observers; with the main purpose of investigating how reproducible was the skeletal maturation evaluation through HW and CVM methods assessed by raters at this level of experience. Understanding how reproducible these methods are when used by orthodontic residents represents an important issue for their confidence when choosing a method for treatment timing planning. Also, findings from Rongo et al indicated that the CVM method reproducibility was not improved by the level of experience in orthodontic practice, as the group with less than 1 year of clinical experience yielded better results.32 The Greulich and Pyle method24 for the HW evaluation and the CVM method of Baccetti and coworkers12 were chosen due to the quicker and more user-friendly approaches.12, 33
The validity and reliability of the CVM method in comparison with HW assessments have been investigated in a series of studies over the years, mainly through correlation and agreement coefficients, such as: ICC, Cohen’s κ coefficient, Kendall’s W coefficient, Pearson and Spearman correlation tests.1,2,9,10,16–18,34–37 Despite these previous studies, results considered the CVM maturation stages as valuable indicators of skeletal growth changes,1,2,9,10,16–18,34,36,37 the reproducibility concerning the difference between repeated measurements of each method against their mean has not been assessed directly. For this purpose, we used the Bland–Altman’s plot25 for evaluating how much the two method differed from each other.
In the current investigation, the HW method of Greulich and Pyle presented a notably larger number of maturation stages compared to the CVM method by Baccetti et al12 The HW stages, in fact, were almost triple the CVM stages. Considering that differences in scale of measurements certainly affects agreement but does not affect the correlation,25 we also opted for evaluating intraexaminer and interexaminer reproducibility by (ICCs.
The results for the Bland–Altman assessment indicated that both HW and CVM presented a small LoA for all of the measurements evaluated. In addition, the CVM presented even a narrower LoA (CVM T1-T2: −2.3 and +1.8; CVM T2-T3: −2.0 and +2.0) in comparison with the HW method (HW T1-T2: −3.9 and +4.8; HW T2-T3: −4.0 and +3.5), but this result does not represent a better reproducibility when compared to the HW method due to their difference in above-mentioned stage scales.
Results for intra- and interexaminer reproducibility estimated by ICC for each method revealed that the HW method presented higher correlation values of repeated measurements in comparison with the cervical vertebra method, however, reproducibility for both of methods was scored as good for the majority of evaluations. It is also important to notice that since 95% confidence intervals ranged from 0.07 to 0.29, the estimate of subject’s skeletal maturation stage may change from good to moderate, indicating its limited predictive value for use in individual patients. According to our findings, Flores-Mir et al9 pointed out the assessment of skeletal maturation as a valuable tool for orthodontic research field rather than in clinical situations, considering it limitations.
The present study showed that there was no significant difference when comparing the reproducibility of HW and CVM assessments of skeletal maturation. This means that both of the methods are considered adequate for clinical use by orthodontic residents. The availability of lateral cephalometric radiographs (routinely requested as orthodontic records or obtained from CBCTs) represents an advantage for CVM methods. However, HW may be used as an additional method to solve any doubt and help to confirm the treatment timing relative to the pubertal growth spurt.
Conclusions
Both HW and CVM methods presented good reproducibility for intraexaminer and interexaminer correlation assessments. The small LoA indicated that the CVM is a reproducible method.
ACKNOWLEDGMENTS
The authors express their gratitude to the Brazilian government agency, CAPES (Coordenação de Aperfeiçoamento de Pessoal de Nível Superior) for providing support for this research development.
Contributor Information
Amanda C Cunha, Email: ccunha.amanda@gmail.com.
Lucia HS Cevidanes, Email: luciacev@umich.edu.
Eduardo F Sant’Anna, Email: eduardo.franzotti@gmail.com.
Fabio R Guedes, Email: fabiorguedes@gmail.com.
Ronir R Luiz, Email: ronir@iesc.ufrj.br.
James A McNamara, Email: mcnamara@umich.edu.
Lorenzo Franchi, Email: lorenzo.franchi@unifi.it.
Antonio Carlos O Ruellas, Email: antonioruellas@yahoo.com.br.
REFERENCES
- 1.Soegiharto BM, Cunningham SJ, Moles DR. Skeletal maturation in Indonesian and white children assessed with hand-wrist and cervical vertebrae methods. Am J Orthod Dentofacial Orthop 2008; 134: 217–26. doi: 10.1016/j.ajodo.2006.07.037 [DOI] [PubMed] [Google Scholar]
- 2.Lai EH, Liu JP, Chang JZ, Tsai SJ, Yao CC, Chen MH, et al. . Radiographic assessment of skeletal maturation stages for orthodontic patients: hand-wrist bones or cervical vertebrae? J Formos Med Assoc 2008; 107: 316–25. doi: 10.1016/S0929-6646(08)60093-5 [DOI] [PubMed] [Google Scholar]
- 3.Moore RN. Principles of dentofacial orthopedics. Semin Orthod 1997; 3: 212–21. doi: 10.1016/S1073-8746(97)80054-0 [DOI] [PubMed] [Google Scholar]
- 4.Johnston FE,Hufham HP,Moreschi AF,Terry GP. Skeletal maturation and cephalofacial development. Angle Orthod 1965; 35: 1–11. doi: [DOI] [PubMed] [Google Scholar]
- 5.Demirjian A, Buschang PH, Tanguay R, Patterson DK. Interrelationships among measures of somatic, skeletal, dental, and sexual maturity. Am J Orthod 1985; 88: 433–8. doi: 10.1016/0002-9416(85)90070-3 [DOI] [PubMed] [Google Scholar]
- 6.Flores-Mir C, Nebbe B, Major PW. Use of skeletal maturation based on hand-wrist radiographic analysis as a predictor of facial growth: a systematic review. Angle Orthod 2004; 74: 118–24. doi: [DOI] [PubMed] [Google Scholar]
- 7.Iguma KE, Tavano O, Carvalho IM. Comparative analysis of pubertal growth spurt predictors: martins and sakima method and grave and brown method. J Appl Oral Sci 2005; 13: 58–61. doi: 10.1590/S1678-77572005000100012 [DOI] [PubMed] [Google Scholar]
- 8.Santos C, Ferreira M, Alves FC, Cunha E. Comparative study of greulich and pyle atlas and maturos 4.0 program for age estimation in a portuguese sample. Forensic Sci Int 2011; 212: 276.e1–276.e7. doi: 10.1016/j.forsciint.2011.05.032 [DOI] [PubMed] [Google Scholar]
- 9.Flores-Mir C, Burgess CA, Champney M, Jensen RJ, Pitcher MR, Major PW. Correlation of skeletal maturation stages determined by cervical vertebrae and hand-wrist evaluations. Angle Orthod 2006; 76: 1–5. doi: 10.1043/0003-3219(2006)076[0001:COSMSD]2.0.CO;2 [DOI] [PubMed] [Google Scholar]
- 10.Gandini P, Mancini M, Andreani F. A comparison of hand-wrist bone and cervical vertebral analyses in measuring skeletal maturation. Angle Orthod 2006; 76: 984–9. doi: 10.2319/070605-217 [DOI] [PubMed] [Google Scholar]
- 11.Baccetti T, Franchi L, McNamara JA. An improved version of the cervical vertebral maturation (CVM) method for the assessment of mandibular growth. Angle Orthod 2002; 72: 316–23. doi: [DOI] [PubMed] [Google Scholar]
- 12.Baccetti T, Franchi L, McNamara JA. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin Orthod 2005; 11: 119–29. doi: 10.1053/j.sodo.2005.04.005 [DOI] [Google Scholar]
- 13.Hassel B, Farman AG. Skeletal maturation evaluation using cervical vertebrae. Am J Orthod Dentofacial Orthop 1995; 107: 58–66. doi: 10.1016/S0889-5406(95)70157-5 [DOI] [PubMed] [Google Scholar]
- 14.Jaqueira LM, Armond MC, Pereira LJ, Alcântara CE, Marques LS. Determining skeletal maturation stage using cervical vertebrae: evaluation of three diagnostic methods. Braz Oral Res 2010; 24: 433–7. doi: 10.1590/S1806-83242010000400010 [DOI] [PubMed] [Google Scholar]
- 15.Mohammed RB, Kalyan VS, Tircouveluri S, Vegesna GC, Chirla A, Varma DM. The reliability of Fishman method of skeletal maturation for age estimation in children of South Indian population. J Nat Sci Biol Med 2014; 5: 297–302. doi: 10.4103/0976-9668.136170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zhao XG, Lin J, Jiang JH, Wang Q, Ng SH. Validity and reliability of a method for assessment of cervical vertebral maturation. Angle Orthod 2012; 82: 229–34. doi: 10.2319/051511-333.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Uysal T, Ramoglu SI, Basciftci FA, Sari Z. Chronologic age and skeletal maturation of the cervical vertebrae and hand-wrist: is there a relationship? Am J Orthod Dentofacial Orthop 2006; 130: 622–8. doi: 10.1016/j.ajodo.2005.01.031 [DOI] [PubMed] [Google Scholar]
- 18.Pasciuti E, Franchi L, Baccetti T, Milani S, Farronato G. Comparison of three methods to assess individual skeletal maturity. J Orofac Orthop 2013; 74: 397–408. doi: 10.1007/s00056-013-0164-x [DOI] [PubMed] [Google Scholar]
- 19.Mahajan S. Evaluation of skeletal maturation by comparing the hand wrist radiograph and cervical vertebrae as seen in lateral cephalogram. Indian J Dent Res 2011; 22: 309–16. doi: 10.4103/0970-9290.84310 [DOI] [PubMed] [Google Scholar]
- 20.Donatelli RE, Lee SJ. How to report reliability in orthodontic research: part 1. Am J Orthod Dentofacial Orthop 2013; 144: 156–61. doi: 10.1016/j.ajodo.2013.03.014 [DOI] [PubMed] [Google Scholar]
- 21.Cericato GO, Bittencourt MA, Paranhos LR. Validity of the assessment method of skeletal maturation by cervical vertebrae: a systematic review and meta-analysis. Dentomaxillofac Radiol 2015; 44: 20140270. doi: 10.1259/dmfr.20140270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Fleiss JL. The design and analysis of clinical experiments. New York: The British Institute of Radiology.; 1985. [Google Scholar]
- 23.Walter SD, Eliasziw M, Donner A. Sample size and optimal designs for reliability studies. Stat Med 1998; 17: 101–10. doi: [DOI] [PubMed] [Google Scholar]
- 24.Greulich W, Pyle S. Radiographic atlas of skeletal development of hand and wrist. 2nd ed Stanford, CA: The British Institute of Radiology.; 1959. 256. [Google Scholar]
- 25.Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: 307–10. [PubMed] [Google Scholar]
- 26.Mattos CT, Cruz CV, da Matta TC, Pereira LA, Solon-de-Mello PA, Ruellas AC, et al. . Reliability of upper airway linear, area, and volumetric measurements in cone-beam computed tomography. Am J Orthod Dentofacial Orthop 2014; 145: 188–97. doi: 10.1016/j.ajodo.2013.10.013 [DOI] [PubMed] [Google Scholar]
- 27.Tanner JM, Whitehouse RH, Cameron N, Marshall WA, Healy MJR, Goldstein H. Assessment of skeletal maturity and prediction of adult height (TW2 method). 2nd ed London: The British Institute of Radiology.; 1983. [Google Scholar]
- 28.Bowden BD. Epiphysial changes in the hand/wrist area as indicators of adolescent stage. Aust Orthod J 1976; 4: 87–104. [PubMed] [Google Scholar]
- 29.Fishman LS. Radiographic evaluation of skeletal maturation. A clinically oriented method based on hand-wrist films. Angle Orthod 1982; 52: 88–112. doi: [DOI] [PubMed] [Google Scholar]
- 30.Israel H. Progressive enlargement of the vertebral body as part of the process of human skeletal ageing. Age Ageing 1973; 2: 71–9. doi: 10.1093/ageing/2.2.71 [DOI] [PubMed] [Google Scholar]
- 31.Hellsing E. Cervical vertebral dimensions in 8-, 11-, and 15-year-old children. Acta Odontol Scand 1991; 49: 207–13. doi: 10.3109/00016359109005909 [DOI] [PubMed] [Google Scholar]
- 32.Rongo R, Valleta R, Bucci R, Bonetti GA, Michelotti A, D’Antò V. Does clinical experience affect the reproducibility of cervical vertebrae maturation method? Angle Orthod 2015; 85: 841–7. doi: 10.2319/080414-544.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.King DG, Steventon DM, O'Sullivan MP, Cook AM, Hornsby VP, Jefferson IG, et al. . Reproducibility of bone ages when performed by radiology registrars: an audit of tanner and whitehouse II versus greulich and pyle methods. Br J Radiol 1994; 67: 848–51. doi: 10.1259/0007-1285-67-801-848 [DOI] [PubMed] [Google Scholar]
- 34.Danaei SM, Karamifar A, Sardarian A, Shahidi S, Karamifar H, Alipour A, et al. . Measuring agreement between cervical vertebrae and hand-wrist maturation in determining skeletal age: reassessing the theory in patients with short stature. Am J Orthod Dentofacial Orthop 2014; 146: 294–8. doi: 10.1016/j.ajodo.2014.05.023 [DOI] [PubMed] [Google Scholar]
- 35.Ozer T, Kama JD, Ozer SY. A practical method for determining pubertal growth spurt. Am J Orthod Dentofacial Orthop 2006; 130: 131.e1–131.e6. doi: 10.1016/j.ajodo.2006.01.019 [DOI] [PubMed] [Google Scholar]
- 36.San Román P, Palma JC, Oteo MD, Nevado E. Skeletal maturation determined by cervical vertebrae development. Eur J Orthod 2002; 24: 303–11. doi: 10.1093/ejo/24.3.303 [DOI] [PubMed] [Google Scholar]
- 37.Wong RW, Alkhal HA, Rabie AB. Use of cervical vertebral maturation to determine skeletal age. Am J Orthod Dentofacial Orthop 2009; 136: 484.e1–484.e6. doi: 10.1016/j.ajodo.2007.08.033 [DOI] [PubMed] [Google Scholar]