

Introduction
Pulmonary torsion occurs when the entire lung or individual lobes rotate around the bronchovascular pedicle. This event is most commonly reported following chest trauma or thoracic surgery with an incidence rate of less than 0.2% of all patients undergoing thoracic surgery (1,2). Few cases of spontaneous whole-lung torsion have been reported in the literature. It may occur secondary to lobar collapse, pneumothorax, or pleural effusion (1) and is often associated with a congenitally absent inferior pulmonary ligament. Early detection and treatment is critical as this condition is potentially fatal secondary to hemorrhagic infarction and respiratory failure (3).
Case presentation
A 79-year-old woman presented with a 2-week history of progressive dyspnea, fatigue, and weakness. Her past medical history included treatment with pomalidomide for intraocular diffuse large B-cell non-Hodgkin’s lymphoma progressing to the cerebellum. She had no cough, hemoptysis, sputum production, or chest pain prior to this presentation. She was found to have a right pleural effusion on chest computed tomography (CT). The patient underwent a thoracentesis with removal of 600 mL of serous fluid that was exudative by LDH criteria, but negative for malignancy or infection. A repeat CT of the chest 5 days later showed recurrence of the right pleural effusion in addition to right upper lobe collapsed due to right lung torsion (Figure 1). The right upper lobe was rotated inferomedially with signs of abscess formation. Both right middle and upper lobes were rotated superiorly with the right lower lobe occupying much of the superior aspect of her chest. This constellation of findings is indicative of a clockwise rotation of the lung around the right hilum. Subsequent V/Q scan demonstrated decrease in right lung perfusion and ventilation when compared to the left, indicative of vascular and ventilation compromise.
Figure 1.

Thoracic Imaging of pulmonary torsion. (A) Axial chest CT revealed clockwise swirling around the right hilum with distortion of the bronchovascular bundle. Note moderate right pleural effusion. (B) Coronal images revealed inferomedial rotation of the collapsed right upper lobe with internal hypoattenuation representing a juxtadiaphragmatic abscess (arrow). (C) Anterior Tc-MAA perfusion image demonstrated markedly decreased right lung perfusion compared to the left. (D) Corresponding Xenon-133 ventilation scan showed right lung hypoventilation.
Bronchoscopy revealed purulent material in an externally compressed right upper lobe bronchus as well as torsion of the bronchus intermedius, middle lobe and lower lobe bronchi (Figure 2). Labs were notable for mildly elevated alkaline phosphatase of 167 and AST at 51.
Figure 2.

Bronchoscopy revealing pulmonary torsion. (A) Main carina with purulent material draining from the right mainstem; (B) distorted anatomy of the right lower lobe secondary to clockwise torsion; (C) right upper lobe take off, appearing extrinsically compressed, with purulent secretions.
A video-assisted thoracoscopic (VATS) right upper lobectomy was performed. The right upper lobe was located anterior and inferior to the two other remaining lobes (Figure 3). The right upper lobe was filled with abscess and had locally perforated and fistualized into the diaphragm (Figure 4). The entire right upper lobe was necrotic, so it was not salvageable despite correcting the torsion. The right lower lobe was rotated clockwise and was resting in the superior aspect of her chest, suggesting that the entire lung had rotated 180 degrees about the hilum. Her inferior pulmonary ligament was intact. The lung was dissected off of the diaphragm with 60 cc of purulent material suctioned out of the cavity followed by a circumferential dissection of the pleura. The lung was retracted anteriorly first to allow a posterior dissection of the subcranial and right upper lobe bronchial area. The lung was then retracted posteriorly and attention was directed toward encircling, stapling, and dividing the vasculature supplying the right upper lobe to complete the right upper lobectomy. The remaining lung parenchyma was tacked into place. The patient was discharged home on postoperative day five after an uncomplicated hospital course.
Figure 3.
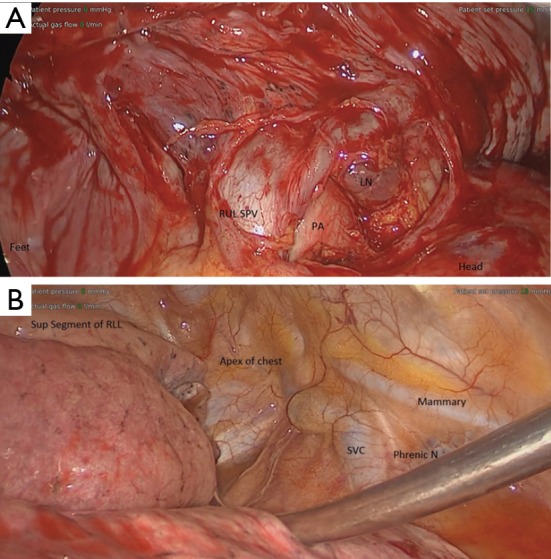
Intraoperative anatomy. (A) Intraoperative anatomy after dissecting the pleura from hilum and untwisting the RUL. The RUL SPV is caudally displaced, while the azygous vein is displaced cranially. (B) The entire lung is rotated 180 degrees clockwise, as demonstrated by the RLL resting in the apex of the chest. LN, lymph node, RUL SPV, right upper lobe superior pulmonary vein; PA, pulmonary artery; SVC, superior vena cava; phrenic N, nerve; RLL, right lower lobe.
Figure 4.
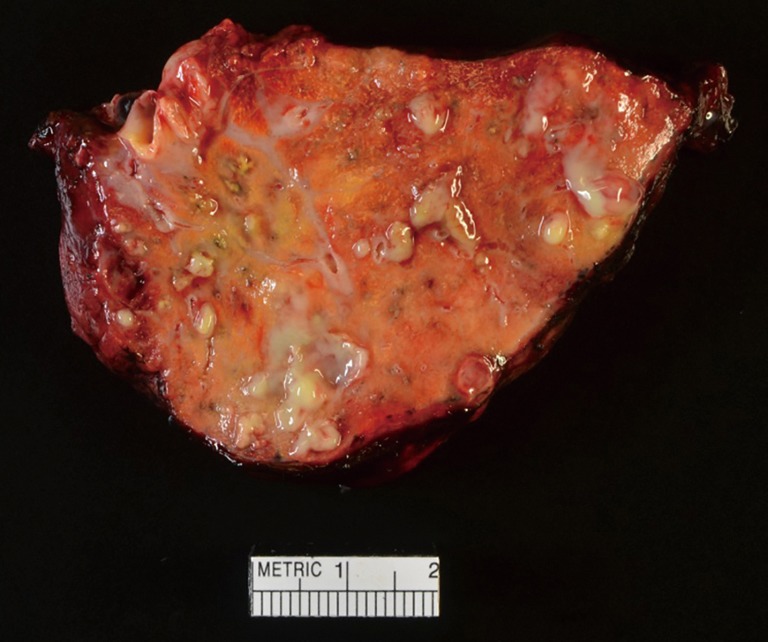
Right upper lobe after resection with significant abscess formation.
The patient returned one month later for a routine visit. She did not require any pain medications at the time of discharge and encountered no post-operative complications. A chest X-ray taken 5 weeks postoperatively showed well-expanded remaining lungs.
Discussion
Pulmonary torsion is a rare but potentially fatal event requiring prompt diagnosis. There have been 4 cases of spontaneous whole-lung torsion reported in the literature since 1988 (4-7). The presumed related etiology of each of these cases involved pneumonia or lung adenocarcinoma (Table 1). The presenting symptom was dyspnea in three of the reported cases, however, Irie et al. [2014] reported a patient presenting with leg edema and pain. Spontaneous whole-lung torsion has occurred in both males and females between the ages of 51 and 82 (4-7) (Table 1).
Table 1. Reported cases of spontaneous whole-lung torsion since 1988.
| Reference | Age/gender | Presenting symptom | Torsion | Management | Outcome | Presumed related etiology |
|---|---|---|---|---|---|---|
| (4) | 79/F | Left leg edema, pain | 120° R lung | Mini thoracotomy to remove pleural effusion, bronchoscopy, fibrin glue to chest wall | Survived | Pneumonia |
| (5) | 72/M | Dyspnea | 180° L lung | Thoracotomy, pneumonectomy | Survived | Lung adenocarcinoma |
| (6) | 51/F | Not reported | 180° R lung | Thoracotomy, three-point fixation of lung to chest wall | Survived | Pneumonia |
| (7) | 82/M | Dyspnea | 180° R lung | Thoracotomy, R upper lobectomy | Survived | Lung adenocarcinoma |
| Our case | 79/F | Dyspnea | 180° R lung | Thoracotomy, R upper lobectomy | Survived | Pneumonia |
This condition is best diagnosed with CT of the chest (2,8). Radiographic indications of lung torsion include hilar displacement, a collapsed or consolidated lobe in an abnormal position, change in the location of pulmonary vasculature, bronchial cutoff or distortion, and lobar air trapping (1). In our case, bronchoscopy was also used as a diagnostic tool. Early detection of a torsed lung is important to prevent hemorrhagic infarction, gangrene, or death with a mortality rate of 22% (2,3).
Emergency lobectomy of the compromised lobe is required to prevent further complication. In our case, the right upper lobe had developed abscesses, which made the removal of this lobe essential. In cases where the torsed lobe has not developed an abscess, salvage by detorsion of the lobe carries the risk of ischemia-reperfusion injury and thus lobectomy is recommended in all cases of lobar torsion (2). Our technique of using a minimally invasive VATS lobectomy proved successful in managing this case of spontaneous pulmonary torsion.
Acknowledgements
None.
Informed Consent: Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Footnotes
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- 1.Felson B. Lung torsion: radiographic findings in nine cases. Radiology 1987;162:631-8. 10.1148/radiology.162.3.3809475 [DOI] [PubMed] [Google Scholar]
- 2.Cohn SM, Dolich MO. Complications in surgery and trauma. 2nd ed. Boca Raton, FL: CRC Press, 2014. [Google Scholar]
- 3.Wong PS, Goldstraw P. Pulmonary torsion: a questionnaire survey and a survey of the literature. Ann Thorac Surg 1992;54:286-8. 10.1016/0003-4975(92)91386-N [DOI] [PubMed] [Google Scholar]
- 4.Irie M, Okumura N, Nakano J, et al. Spontaneous whole-lung torsion after massive pleural effusion and atelectasis. Ann Thorac Surg 2014;97:329-32. 10.1016/j.athoracsur.2013.04.133 [DOI] [PubMed] [Google Scholar]
- 5.Bell MT, Kelmenson DA, Vargas D, et al. Spontaneous Pulmonary Torsion Secondary to Left Upper Lobe Malignancy. J Thorac Oncol 2015;10:1653-4. 10.1097/JTO.0000000000000573 [DOI] [PubMed] [Google Scholar]
- 6.Trotter MC, McFadden PM, Ochsner JL. Spontaneous torsion of the right lung: a case report. Am Surg 1995;61:306-9. [PubMed] [Google Scholar]
- 7.Chrysou K, Gioutsos K, Filips A, et al. Spontaneous right whole-lung torsion secondary to bronchial carcinoma: a case report. J Cardiothorac Surg 2016;11:107. 10.1186/s13019-016-0506-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kita Y, Go T, Nii K, et al. Spontaneous torsion of the right upper lung lobe: a case report. Surg Case Rep 2017;3:37. 10.1186/s40792-017-0313-3 [DOI] [PMC free article] [PubMed] [Google Scholar]