

Abstract
Background:
Military pilots are exposed to harmful noise levels, and the two possible effects of this are hearing loss and tinnitus.
Objective:
This study was conducted to determine the prevalence of noise-induced hearing loss among Saudi military pilots and to determine its association with total flight hours and aircraft type (i.e., fixed and rotary wing).
Materials and Methods:
This cross-sectional study was conducted at the Armed Forces Aeromedical Centre, Dhahran, Saudi Arabia, between November 2015 and October 2016. A total of 150 Saudi military pilots were interviewed using a structured questionnaire. Pure-tone audiometry was used to measure hearing thresholds. Hearing threshold levels were compared between age groups and aircraft category. The association between total flying hours and the development of noise-induced hearing loss was analyzed.
Results:
The overall prevalence of noise-induced hearing loss in the military pilots was 18.4%, with a higher prevalence among fixed-wing pilots (42%) as compared with rotary-wing pilots (23%). Pilots with ≥2000 flying hours had a significantly higher hearing threshold compared with those in other categories. Age was a statistically significant risk factor.
Conclusions:
This study found that active pilots of both fixed- and rotary-wing aircrafts are at a high risk of noise-induced hearing loss; however, fixed-wing pilots with ≥2000 flying hours are at a higher risk. These findings support recommendations requiring instructions on the proper use of hearing protection devices to avoid noise-induced hearing loss.
Keywords: Aircraft, audiometry, flying time, hearing loss, military pilots, Saudi Arabia
INTRODUCTION
Hearing is a complex and crucial component of human communication, and its integrity is critical to the performance of military aviators. Military aviators are subjected to high levels of noise exposure, which can result in physiologic damage or psychological harm and decrease their quality of life.[1,2] Psychological trauma can manifest as sleep disturbances, adverse social and economic consequences and increased physiologic stress response.[1] In terms of physiological effects, in the United States, the most prevalent service-connected disability for veterans was tinnitus, followed by noise-induced hearing loss (NIHL).[2]
Military audiologists define NIHL as an “acoustic overstimulation of the sensory organ of hearing (cochlea) and associated acoustic energy conduction structures such as the eardrum and middle ear bones (ossicles).”[3] The terminology “Hearing Impairment and Noise-Induced Hearing Injury” includes tinnitus, acute acoustic trauma and hearing loss due to continuous or intermittent noise exposure.[3] Limited exposure to noise can lead to reversible hearing damage, as the temporary threshold shift eventually disappears after a few hours in a quiet environment. However, continued or repeated exposures to noise eventually result in irreversible sensory hair cell damage and concomitant permanent sensorineural hearing loss (permanent threshold shift).[4]
Functional hearing abilities, the required hearing abilities of a pilot to function in the aviation environment, depend on binaural hearing and central auditory processing. The most important functional auditory effect of NIHL is decreased speech perception and intelligibility, especially in conditions with substantially loud background noises. This, in turn, reduces the piloting ability and combating performance of the affected pilot.[5,6] In a study on helicopter pilots, the flight performance and speech intelligibility were negatively affected by increased workload and poor-quality communication.[7]
Although NIHL is a preventable and predictable disease, there is not sufficient evidence to determine the probability of acquiring NIHL or to estimate the elevated hearing threshold levels of NIHL that an individual is likely to experience from a given noise exposure.[8] Further, there is a lack of such studies from Saudi Arabia. Accordingly, the current study was conducted to determine the prevalence of NIHL among Saudi military pilots and to determine its association with total flight hours and aircraft type (i.e., fixed and rotary wing). The results of this study can provide useful data for policy makers when implementing hearing conservation measures in the military aviation environment.
MATERIALS AND METHODS
This cross-sectional study was carried out at Armed Forces Aeromedical Centre, Dhahran, Saudi Arabia, after the study protocol was approved by the Research and Ethics Committee of Northern Area Armed Forces Hospital, Hafar Al-Batin, Saudi Arabia, on February 15, 2015.
Saudi military pilots aged 23–55 years and who flew missions in aircraft during their annual medical checkups were included in this study. The inclusion range of flying time was 500–6000 h. A total of 150 participants were recruited by convenience sampling between November 1, 2015, and October 31, 2016. This study used an expanded version of a questionnaire previously developed and validated by Pelausa et al.[9] Participants were asked to complete this 15-item, multiple-choice questionnaire to determine the possible risk factors associated with hearing loss, if any.
The questionnaire elicited data on work-related noise exposure and leisure noise exposure. In addition, participants were also asked if they had a history of ear infections, ear symptoms, head injury and tinnitus, and if they had ever taken ototoxic medications. Each question had 4–5 alternative answers (e.g., no, occasionally, often or constantly).
Tonal audiograms were collected in a soundproof single-walled booth. The apparatus included a Maico MA50 audiometer (MAICO Diagnostics, Berlin, Germany) and TDH-39 matched headset (Telephonics Corp., Huntington, NY). Participants were individually tested in the soundproof booth. Hearing thresholds were measured by an audiologist in each ear at the following pure-tone frequencies: 0.25, 0.5, 1, 2, 3, 4, 6 and 8 kHz. The sound level was increased and decreased in steps of 5 dB to determine the hearing threshold separating the audible and inaudible ranges.
Pilots were stratified based on the degree and configuration of hearing loss as follows: pilots with a normal hearing level (i.e., audiometric pure-tone air conduction thresholds not more than 25 dB HL at all frequencies in both ears), those with a minimal-to-mild high-frequency hearing loss (i.e., audiometric pure-tone air conduction thresholds not more than 40 dB HL at 3, 4 and/or 6 kHz in either ear) and those with a moderate high-frequency hearing loss (i.e., audiometric pure-tone air conduction thresholds not more than 55 dB HL at 3, 4 and/or 6 kHz in either ear).
Differences in prevalence of hearing loss was assessed using the chi-square test. Repeated-measures, mixed-effects ANOVA was used to determine mean hearing thresholds, with an alpha level of 0.05. P < 0.05 was considered statistically significant. ANOVA was followed by Tukey's multiple comparison post hoc test, when appropriate. Data were analyzed using SPSS version 24 (IBM Corporation, Armonk, NY, USA).
RESULTS
All 150 Saudi military pilots who participated in the study were male and aged 23–55 years. Of these, 96 were fixed-wing pilots and 54 were rotary-wing pilots. Pilots were categorized based on age (23–40 and 40–55 years) and flying hours (<1000, 1000–1999 and ≥2000 flying hours) [Table 1]. The prevalence of hearing loss in the 25–40-year-old age group (12%; n = 12) was statistically different from that in the 40–55-year-old age group (35%; n = 16) (χ2= 9.6, P = 0.002), indicating increase in age was associated with greater hearing loss. Further, fixed-wing pilots were found to have a significantly higher prevalence of hearing loss (42%) compared with that of rotary-wing pilots (23%) (χ2= 6.0, P = 0.016).
Table 1.
The distribution of pilots by age and flying hours
| Aircraft type | Age (years) | Flying hours | |||
|---|---|---|---|---|---|
| 23-40 | 40-55 | <1000 | 1000-1999 | ≥2000 | |
| Fixed wing (n) | 66 | 30 | 39 | 29 | 28 |
| Rotary wing (n) | 37 | 17 | 29 | 15 | 10 |
| Total (%) | 103 (69) | 47 (31) | 68 (45) | 44 (29) | 38 (26) |
The overall prevalence of NIHL among the military pilots was 18.4%. Table 2 shows the mean threshold values for the right and left ears of both fixed- and rotary-wing pilots according to the audiograms. For both ears, the audiometric curves of the mean hearing level threshold showed a downward slope from 4 kHz with a notch at 6 kHz and subsequent improvement at 8 kHz. Hearing loss at 6 kHz was mild to moderate. However, the hearing threshold of rotary-wing pilots was found to be lower (i.e., better) than that of fixed-wing pilots.
Table 2.
Mean right and left ear hearing level thresholds (dB HL)
| Aircraft type | Ear | Frequency (kHz) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 0.25 | 0.5 | 1 | 2 | 3 | 4 | 6 | 8 | ||
| Fixed wing | Right | 10.3 | 11.2 | 10.5 | 8.7 | 12.6 | 13.6 | 17.3 | 16.7 |
| Left | 9.2 | 11.4 | 11.6 | 9.6 | 15.2 | 13.6 | 23.7 | 21.2 | |
| Rotary wing | Right | 7.4 | 9.8 | 9.9 | 7.4 | 11.0 | 12.6 | 10.5 | 8.7 |
| Left | 7.7 | 9.4 | 10.2 | 8.6 | 11.1 | 12.6 | 13.3 | 10.8 | |
ANOVA revealed a significant effect of flying hours and aircraft type on the mean hearing threshold level. The mean hearing threshold level at 3, 4 and 6 kHz in <000, 1000–1999 and ≥2000 flying hours were 10.84, 12.98 and 18.09 dB HL, respectively, indicating that pilots with ≥2000 flying hours experienced a greater hearing loss compared with those in other categories. Tukey's pairwise comparison test for aircraft type and flying time revealed that pilots of fixed-wing aircraft with ≥2000 flying hours had a significant higher mean hearing threshold than that of rotary-wing aircraft pilots (fixed-wing aircraft mean ± standard deviation [SD] = 27.50 ± 18.44; rotary wing aircraft mean ± SD = 23.03 ± 11.09) [Table 3 and Figure 1]. At <1000 flying hours, the mean hearing threshold was similar for both aircraft types (fixed-wing aircraft mean ± SD = 9.84 ± 11.76; rotary-wing aircraft ± SD = 8.84 ± 5.45), whereas at 1000–1999 flying hours, the difference increased (fixed-wing aircraft ± SD = 11.89 ± 20.58; rotary-wing aircraft ± SD = 10.17 ± 6.61) [Table 3].
Table 3.
Mean hearing thresholds and 95% confidence interval values for aircraft type and flying time
| Aircraft type | Flying hours | Mean (±SD) hearing (dB) | Lower 95% CI | Upper 95% CI |
|---|---|---|---|---|
| Fixed | <1000 | 9.84 (±11.76) | 7.4 | 12.2 |
| 1000-1999 | 11.89 (±20.58) | 7.7 | 16.0 | |
| ≥2000 | 27.50 (±18.44)* | 23.7 | 31.2 | |
| Rotary | <1000 | 8.84 (±5.45) | 7.3 | 10.3 |
| 1000-1999 | 10.17 (±6.61) | 8.3 | 11.9 | |
| ≥2000 | 23.03 (±11.09)** | 20.0 | 26.0 |
*P<0.05 for those with ≥2000 flying hours compared with those with 1000-1999 flying hours, **P<0.05 for those with ≥2000 flying hours compared with those with <1000 flying hours. SD – Standard deviation; CI – Confidence interval
Figure 1.
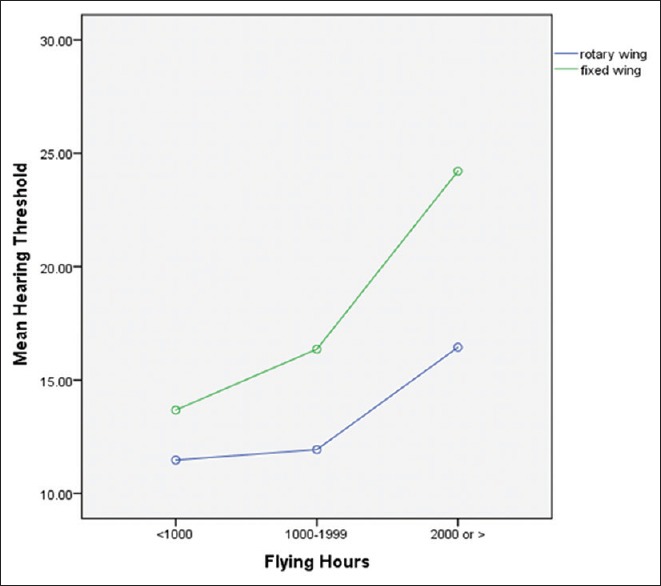
The effect of flying time on the mean hearing threshold levels of fixed-wing and rotary-wing pilots
From the response of the questionnaire, this study did not find any association between risk factors of hearing loss and abnormal hearing. Only 0.4% (n = 2) and 1% (n = 5) of the respondents had tinnitus constantly and often, respectively. There were no cases of permanent hearing loss from head injuries sustained outside of work, and there was no evidence that any pilot was suffering from a permanent hearing loss as a result of taking medications.
DISCUSSION
Hearing integrity is critical to the performance of military aviators, who are exposed to harmful noise levels that can lead to NIHL. NIHL is a preventable disease; however, previously, there was a lack of data on the probabilities of military pilots in Saudi Arabia acquiring NIHL with different aircraft types and flying hours. The current study found that aircraft type and its flying hours were significant factors in the prevalence of hearing loss among Saudi military aviators, with the prevalence of NIHL being higher among fixed-wing aviators with ≥2000 flying hours than that of other categories.
Several studies have corroborated an association between hearing loss and military occupation in the army and navy. For example, in the Belgian Armed Forces, the prevalence of hearing loss in the military population aged 18–55 years has been found to be high (~56%).[10] In comparison, a slightly higher prevalence of hearing loss was found in Finnish Defence Forces[11] and lower in Canadian military personnel[12] and US Marine Troops.[13] Worryingly, a study found that between 2007 and 2010, sensorineural hearing loss increased from 11% to 23% among active military personnel in the US Armed Forces.[14] Similarly, a recent study found a significant shift (23.0%) in the hearing threshold among personnel onboard the Royal Norwegian Navy's vessels between 2012 and 2014.[15]
Specifically, studies on the effects of exposure to high noise levels in military aviation of different countries have provided varying conclusions. A study of the US army aviators in 1983 found an association between flight hours and increase in hearing loss.[16] These findings were corroborated by a study on 178 US Army Aviators that found hearing loss was associated with both age and flight hours, both of which are time-dependent factors.[17] It is well established that age most consistently affects hearing abilities.[3,12,18] Unsurprisingly, the findings of the above-mentioned studies regarding NIHL being associated with age and flight hours are similar to that found in the present study. Alternatively, a study that assessed 200 helicopter aircrew in the Army Air Corps demonstrated a correlation between hearing loss and the number of years spent flying.[19] Similarly, Owen[20] found that, among helicopter pilots of the US Army, hearing impairment was related more to the length of flying career and age rather than the number of flight hours.
Although it seems axiomatic that aircraft noise exposure would be the major factor associated with hearing loss in military aircrew, recent studies have not always supported this assumption. For example, a study of >20,000 US Marine Corps personnel demonstrated that aviation personnel were no more likely to have elevated hearing thresholds than other Marines.[13] Surprisingly, a Finnish study by Kuronen,[21] using an international standardization for the estimation of occupation-related NIHL, found that Finnish military aviators had better hearing than predicted. A possible explanation for these unexpected findings is the improved level of noise attenuation offered by modern military flight helmets.
With regard to the impact of aircraft type on hearing loss, the majority of previous studies suggest that no significant effect exists.[17,22] However, the current study found fixed-wing pilots to be more affected than rotary-wing pilots. These findings are in contrast with a prevalence study among French military aviators that found helicopter aviators to have a significantly higher prevalence of abnormal hearing (55%) than fighter and transport aviators.[23] Nevertheless, the findings of the current study are consistent with a recent study that found that, in the United States, the average annual incidence rate of sensorineural hearing loss between 1997 and 2011 was higher among fixed-wing pilots than rotary-wing aviators. Interestingly, the same study also showed such hearing loss to be higher among US US Army and Air Force personnel than Navy and Marine aviators.[24] According to Wagstaff and Arva,[25] the differences in hearing between fixed-wing and right-wing pilots may be explained by the fact that rotary-wing pilots use circumaural headsets that provide a high degree of noise attenuation, resulting in these pilots having a hearing level similar to that of civilian airline pilots and air traffic controllers.
In the current study, for both ears, the audiometric curves of the mean hearing level threshold showed a downward slope from 4 k Hz with a notch at 6 kHz and improvement at 8 kHz. This finding is in contrast to that of Lang and Harrigan,[26] who found that, in helicopter pilots of British Army Air Corps, hearing was better than predicted at nearly all frequencies in both ears. Our findings are consistent with that of Abel,[12] who found that, in the studied Canadian military personnel, about 17% of the oldest age group (46–65 years) had a moderate-to-severe hearing at 4 and 6 kHz, whereas until the mid-40s, 85% of the military personnel had no more than a mild hearing loss of <30 dB HL at these two frequencies, highlighting age-related steep declines in hearing.[12] In the current study, the authors found that hearing threshold at mid-frequency (i.e., 3 kHz) is only mildly elevated, and thus pilots are likely to not have difficulty with speech understanding in quiet, but this can potentially compromise speech communication in the presence of background noise.
Although the current study found that NIHL was associated with flying hours and aircraft type, the authors believe that using proper personal protective equipment may prevent NIHL. Therefore, to decrease the incidence of NIHL, the authors recommend active surveillance of hearing protection practices. In addition, the authors recommend that audiological measures such as pure-tone audiometry and speech intelligibility in quiet should be carried out regularly to establish an objective relationship between hearing impairment and reduced functional hearing ability.
A limitation of this study is that the functional hearing abilities of the pilots were not evaluated, as speech audiometry testing was not carried out, and thus speech misperception was not objectively evaluated. Another limitation was that the age correction for hearing thresholds was not performed, and thus the presence of concomitant presbycusis or age-related hearing loss cannot be excluded. Finally, because the sample size of the current study was small and from a single location, the results of this study may not be representative of all military pilots throughout Saudi Arabia. Nevertheless, the results of the study provide important insight for Saudi Arabia's military aviation policymakers for implementing strategies to decrease the rate of NIHL among pilots.
CONCLUSIONS
This study found that pilots flying fixed- and rotary-wing aircraft are at a high risk of hearing loss. The prevalence of NIHL was higher among fixed-wing aviators, especially among those with ≥2000 flying hours. Instructions on proper use of hearing protection devices and periodic monitoring of the same should be made mandatory at all military facilities.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Seidman MD, Standring RT. Noise and quality of life. Int J Environ Res Public Health. 2010;7:3730–8. doi: 10.3390/ijerph7103730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yankaskas K. Prelude: Noise-induced tinnitus and hearing loss in the military. Hear Res. 2013;295:3–8. doi: 10.1016/j.heares.2012.04.016. [DOI] [PubMed] [Google Scholar]
- 3.Helfer TM, Canham-Chervak M, Canada S, Mitchener TA. Epidemiology of hearing impairment and noise-induced hearing injury among U.S. Military personnel, 2003-2005. Am J Prev Med. 2010;38:S71–7. doi: 10.1016/j.amepre.2009.10.025. [DOI] [PubMed] [Google Scholar]
- 4.Rajguru R. Military aircrew and noise-induced hearing loss: Prevention and management. Aviat Space Environ Med. 2013;84:1268–76. doi: 10.3357/asem.3503.2013. [DOI] [PubMed] [Google Scholar]
- 5.Blue-Terry M, Letowski T. Effects of white noise on callsign acquisition test and modified rhyme test scores. Ergonomics. 2011;54:139–45. doi: 10.1080/00140139.2010.540354. [DOI] [PubMed] [Google Scholar]
- 6.Norin JA, Emanuel DC, Letowski TR. Speech intelligibility and passive, level-dependent earplugs. Ear Hear. 2011;32:642–9. doi: 10.1097/AUD.0b013e31821478c8. [DOI] [PubMed] [Google Scholar]
- 7.Casto KL, Casali JG. Effects of headset, flight workload, hearing ability, and communications message quality on pilot performance. Hum Factors. 2013;55:486–98. doi: 10.1177/0018720812461013. [DOI] [PubMed] [Google Scholar]
- 8.Humes LE, Joellenbeck LM, Durch JS. Washington DC: The National Academies Press; 2006. Noise and Military service: Implications for Hearing Loss and Tinnitus. [Google Scholar]
- 9.Pelausa EO, Abel SM, Simard J, Dempsey I. Prevention of noise-induced hearing loss in the Canadian military. J Otolaryngol. 1995;24:271–80. [PubMed] [Google Scholar]
- 10.Collée A, Legrand C, Govaerts B, Van Der Veken P, De Boodt F, Degrave E, et al. Occupational exposure to noise and the prevalence of hearing loss in a belgian military population: A cross-sectional study. Noise Health. 2011;13:64–70. doi: 10.4103/1463-1741.73997. [DOI] [PubMed] [Google Scholar]
- 11.Ylikoski ME, Ylikoski JS. Hearing loss and handicap of professional soldiers exposed to gunfire noise. Scand J Work Environ Health. 1994;20:93–100. doi: 10.5271/sjweh.1415. [DOI] [PubMed] [Google Scholar]
- 12.Abel SM. Risk factors for the development of noise-induced hearing loss in Canadian Forces personnel. Defence Research and Development Canada–Toronto 2004; External Client Report No.: ECR. 2004. [Last accessed on 2017 Jun 17]. p. 116. Available from: http://www.veterans.gc.ca/pdf/about-us/research-directorate/risk-factors-hearing-loss-cdn-forces.pdf .
- 13.Barney R, Bohnker BK. Hearing thresholds for U.S. Marines: Comparison of aviation, combat arms, and other personnel. Aviat Space Environ Med. 2006;77:53–6. [PubMed] [Google Scholar]
- 14.Helfer TM. Noise-induced hearing injuries, active component, U.S. Armed forces, 2007-2010. MSMR. 2011;18:7–10. [PubMed] [Google Scholar]
- 15.Irgens-Hansen K, Baste V, Bråtveit M, Lind O, Koefoed VF, Moen BE, et al. Hearing loss in the Royal Norwegian Navy: A longitudinal study. Noise Health. 2016;18:157–65. doi: 10.4103/1463-1741.181999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Peters LJ, Ford H. Extent of Hearing Loss Amongst Army Aviators at Fort Rucker, Alabama. US Army Aeromedical Research Laboratories, Fort Rucker, Alabama: Report No 83; 12 August. 1983. [Last accessed on 2017 May 05]. Available from: http://www.dtic.mil/dtic/tr/fulltext/u2/a132069.pdf .
- 17.Fitzpatrick DT. An analysis of noise-induced hearing loss in army helicopter pilots. Aviat Space Environ Med. 1988;59:937–41. [PubMed] [Google Scholar]
- 18.International Organization for Standardization. ISO 7029:2017 Acoustics –Statistical Distribution of Hearing Thresholds Related to Age and Gender. [Last accessed on 2017 Apr 01]. Available from: https://www.iso.org/standard/42916.html .
- 19.Edgington KE, Oelman BJ. An Audiometric survey of army aircrew. Internal Report. HQ Director Army Aviation, Middle Wallop, Hampshire, England. 1982 [Google Scholar]
- 20.Owen MJ. A survey of hearing loss in army aircrew. Occup Med (Lond) 1996;46:53–8. doi: 10.1093/occmed/46.1.53. [DOI] [PubMed] [Google Scholar]
- 21.Kuronen P, Toppila E, Starck J, Pääkkönen R, Sorri MJ. Modelling the risk of noise-induced hearing loss among military pilots. Int J Audiol. 2004;43:79–84. [PubMed] [Google Scholar]
- 22.Owen JP. Noise induced hearing loss in military helicopter aircrew – A review of the evidence. J R Army Med Corps. 1995;141:98–101. doi: 10.1136/jramc-141-02-08. [DOI] [PubMed] [Google Scholar]
- 23.Raynal M, Kossowski M, Job A. Hearing in military pilots: One-time audiometry in pilots of fighters, transports, and helicopters. Aviat Space Environ Med. 2006;77:57–61. [PubMed] [Google Scholar]
- 24.Orsello CA, Moore JE, Reese C. Sensorineural hearing loss incidence among U.S. Military aviators between 1997 and 2011. Aviat Space Environ Med. 2013;84:975–9. doi: 10.3357/asem.3660.2013. [DOI] [PubMed] [Google Scholar]
- 25.Wagstaff AS, Arva P. Hearing loss in civilian airline and helicopter pilots compared to air traffic control personnel. Aviat Space Environ Med. 2009;80:857–61. doi: 10.3357/asem.1991.2009. [DOI] [PubMed] [Google Scholar]
- 26.Lang GT, Harrigan MJ. Changes in hearing thresholds as measured by decibels of hearing loss in British Army Air Corps lynx and apache pilots. Mil Med. 2012;177:1431–7. doi: 10.7205/milmed-d-11-00409. [DOI] [PubMed] [Google Scholar]