

INTRODUCTION
Confocal imaging uses a laser projected onto a point of a specimen and detects light reflecting back through a pinhole.[1] Endoscopic systems utilize a fiber-optic bundle, where each fiber acts as the light source and pinhole transmits reflected light to a detector, thereby creating an image of the tissue beneath the probe.[2] Its first use was described of the human eye in 1991[3] and subsequently in the skin, oral cavity, and gastrointestinal lumen in 2004.[4,5,6] In this review, we discuss the role of confocal endomicroscopy in pancreatic cystic lesions (PCLs).
OVERVIEW OF PANCREATIC CYST LESIONS
The prevalence of PCLs is approximately 2%.[7] PCLs are being diagnosed more frequently due to the increased use of cross-sectional imaging.[8] Management depends on the determination of the subset of cyst and potential for malignant transformation. Characterization of PCLs is determined by a patient's symptoms, imaging findings (EUS/computed tomography), and cyst fluid studies (viscosity, tumor markers, and pancreatic enzyme levels). EUS-FNA is used to obtain fluid for analysis. However, cyst fluid cytology has a pooled sensitivity of 63% and specificity of 88% due to the poor aspiration of epithelial cells.[9] The use of tumor markers such as carcinoembryonic antigen (CEA) (with a cutoff level of >192 ng/mL) has poor accuracy, misdiagnosing 39% of mucinous cystic neoplasms (MCNs) (premalignant PCLs) in one study.[10] Thus, the diagnosis of PCLs can be elusive and complicate the decision between surgical resection and surveillance. The unnecessary resection of serous cystadenomas (a benign type of PCL) is estimated to be 36% in one large international retrospective series of 2622 cases.[11]
PROCESS OF DEPLOYING CONFOCAL IMAGING DURING EUS
The process of confocal imaging during EUS guided needle-based confocal laser endomicroscopy (nCLE) is outlined by Kamboj et al. EUS is first performed using a standard linear endoscope.[12] Before nCLE, 5 mL of 10% fluorescein sodium is injected intravenously 2–3 min before nCLE imaging, illuminating the extracellular matrix and lamina propria. Intracystic images are obtained with the AQ-Flex nCLE mini-probe (Cellvizio, Mauna Kea Technologies, Paris, France) which is preloaded onto a 19-gauge FNA needle. The needle is then inserted into the endoscope under EUS guidance advanced into the PCL until it contacts the epithelial wall. The probe can be manipulated across the endothelial wall to identify characteristic lesions discussed below in Figures 1 and 2. Image acquisition and interpretation generally take 6–8 min.[12]
Figure 1.
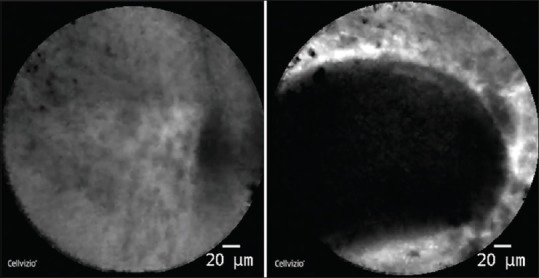
Needle-based confocal laser endomicroscopy images (left) of debris in a pseudocyst and (right) finger-like projection seen in all intraductal papillary mucinous neoplasm types
Figure 2.

Needle-based confocal laser endomicroscopy image of the superficial vascular network seen in low-risk serous cystadenomas (left) and a vascular network represented with white bands (right)
CURRENT TRIAL EVIDENCE DATA
The first human pilot feasibility study was completed in 2011 by Konda et al. with 18 cases (16 cysts and 2 solid lesions of the pancreas). Adequate images were obtained in 10/18 patients, and 2/18 (11%) developed postprocedural pancreatitis. The next study by Giovannini et al. in 2012 with 11 cases (4 pancreatic masses, 3 PCL, and 4 lymph nodes (LN)) demonstrated large dark clumps and leakage of fluorescein of the pancreatic masses and malignant LNs.[13]
Subsequent studies have attempted to identify histological patterns observed in subsets of PCLs. The first such trial, INSPECT (2013),[14] was an international, multicenter trial of 66 patients with PCLs evaluated with in vivo nCLE.First, an independent gastrointestinal histopathologist reviewed nCLE images and surgical pathology to correlate findings and create descriptive terms. Of the 66 patients, 14 (21.2%) had surgical histopathology. In the other patients, the diagnosis was determined by five independent investigators who reviewed the patient's clinical factors (imaging findings, cyst fluid appearance, viscosity, cytology, CEA, and amylase levels). Patients were classified as high or low confidence of diagnosis based on the level of consensus of the investigators, with 33 patients (50%) categorized as high confidence (complete consensus) and all other patients categorized as low confidence (10 patients; 15.1%). The main finding was that epithelial villous “finger-like structures” (P = 0.004) were the only significant nCLE finding associated (Figure 1) with pancreatic cystic neoplasm including intraductal papillary mucinous neoplasms (IPMNs) with a sensitivity of 59%, specificity of 100%, positive predictive value (PPV) of 100%, and negative predictive value (NPV) of 50%,[14] suggesting that IPMN could be diagnosed with a high level of specificity and PPV with nCLE.
In the CONTACT (2014), trial a “superficial vascular network” pattern visualized on nCLE corresponded histologically to a dense subepithelial (Figure 2) capillary vascularization only seen in superficial vascular networks. This was an important finding as Serous cystadenoma (SCA) lesions have low malignancy potential[11] and thus do not require surveillance. FNA studies of SCA generally reveal very low CEA levels and low viscosity.[15] The accuracy, sensitivity, specificity, PPV, and NPV of finding a superficial vascular network on nCLE for the diagnosis of SCA were 87%, 69%, 100%, 100%, and 82%, respectively, and interobserver agreement (IOA) was substantial at κ = 0.77.[16] The visualization of this criterion could have a direct impact on the management of patients by avoiding unnecessary surgery or repeated procedures for surveillance.
In a follow-up study, after the initial CONTACT study (2015), the authors retrospectively analyzed nCLE image in an attempt to identify additional patterns. MCNs are described as a “gray band with a thin dark line” which histologically represents inflammatory tissue lacking an epithelial lining. They also described findings for pseudocysts as a “field of bright, gray, and black particles” representing mixed inflammatory cells, and neuroendocrine neoplasm tumors as “dark irregular clusters” (neoplastic cells) surrounded by “gray areas” (fibrovascular stroma). The study's weaknesses included the fact that the diagnoses were not confirmed with surgical histopathology in a majority of the cases.
In the DETECT trial (2015), 30 patients were studied with nCLE and cystoscopy with Spyglass. In these patients, papillary projections and dark rings on nCLE had a sensitivity of 80%, specificity of 100%, PPV of 100%, NPV of 80%, and accuracy of 89% for a diagnosis of MCN when nCLE was combined with direct cystoscopy.[17] The trial was limited as it was a single-center study, and only two patients had the availability of surgical histopathology. In a majority of patients, the diagnosis was established on the level of agreement of two independent investigators.
Similar to the findings of INSPECT, in the INDEX trial (2016), four patients with each of the four subtypes of IPMN – gastric, intestinal, pancreaticobiliary, and oncocytic – were enrolled. Following EUS-nCLE, patients underwent surgical resection of PCL and histopathology was confirmed. The trial correlated findings on EUS-nCLE with histopathology findings. The findings on EUS-nCLE demonstrated epithelial bands with finger-like projections (or papillae) for all lesions. These papillae were easily seen in all four cases. These patterns likely represent gastric and intestinal type of IPMN.[17] In this study, the oncocytic subtype also demonstrated “fine clefts and a scale-like appearance” of the papillae which was distinct.[12]
In 2016, Karia et al. deidentified 15 nCLE video clips of PCLs and analyzed the IOA using Fleiss’ kappa statistic between six interventional endoscopists at five institutions. Unfortunately, the results revealed low IOA for specific nCLE imaging findings (κ ranging from −0.04 for vessels [poor agreement] to 0.22 for dark clumps [fair agreement]) as well as a low IOA on the final diagnosis κ = 0.13 (slight agreement).[18]
DISCUSSION
Initial management guidelines for PCLs favored a resection strategy for all suspected mucinous PCLs (MCN and IPMN) and therefore had high sensitivity (100%) but poor specificity for malignant pancreatic lesions (20%–30%).[8] In 2010, the revised “Fukuoka” guidelines were less rigorous but associated with unacceptably high false-negative malignancy rates due to the assumption that a correct diagnosis of IPMN and MCN can be made on the basis of clinical, laboratory, and imaging findings. On the other hand, less rigorous surgical recommendations seen in follow-up guidelines lead to a risk of missing advanced lesions and unnecessarily surveilling low-risk lesions. EUS-nCLE helps improve diagnostic accuracy to avoid these pitfalls. Studies demonstrate high specificity with nCLE for low-risk lesions such as SCA, potentially avoiding unnecessary surveillance or surgery. In addition, the finding of a papillary or villous finger-like projection is highly specific for IPMNs, with fine clefts and a scale-like appearance possibly signifying an oncocytic subtype. Leakage of dye was associated with pancreatic adenocarcinoma.[13]
Surgery with histopathology remains the gold standard for correct characterization of PCLs but is invasive. Endoscopists need additional tools to improve the sensitivity and specificity of the preoperative diagnosis. The goal should be to minimize patient harm (unnecessary surveillance) and to maximize diagnostic accuracy. EUS-nCLE imaging findings taken together with the results of cytology, tumor markers, and genetic studies may improve preoperative surveillance algorithms when cytology and FNA results are indeterminate. However, this technology is plagued by the same problems of the tests it is meant to augment, namely, low sensitivity. Although there is high specificity of certain imaging findings, there is low IOA of endoscopists reviewing preexisting images. In addition, heterogeneity within a single PCL may limit identification of highly specific findings.
CONCLUSION
EUS-nCLE can improve preoperative diagnosis of PCLs safely and efficiently when characteristic features of distinct PCL subtypes are identified. However, poor IOA and limitations in image acquisition from heterogeneity-induced sampling error have limited its widespread adoptability. Further studies should aim on ways to improve sensitivity and agreement between endoscopists performing nCLE.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Jabbour JM, Saldua MA, Bixler JN, et al. Confocal endomicroscopy: Instrumentation and medical applications. Ann Biomed Eng. 2012;40:378–97. doi: 10.1007/s10439-011-0426-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Delaney P, Harris M. Fiber-optics in scanning optical microscopy. In: Pawley JB, editor. Handbook of Biological Confocal Microscopy. Boston, MA: Springer US; 2006. pp. 501–15. [Google Scholar]
- 3.Cavanagh HD, Jester JV, Essepian J, et al. Confocal microscopy of the living eye. CLAO J. 1990;16:65–73. [PubMed] [Google Scholar]
- 4.Corcuff P, Lévêque JL. In vivo vision of the human skin with the tandem scanning microscope. Dermatology. 1993;186:50–4. doi: 10.1159/000247302. [DOI] [PubMed] [Google Scholar]
- 5.New KC, Petroll WM, Boyde A, et al. In vivo imaging of human teeth and skin using real-time confocal microscopy. Scanning. 1991;13:369–72. [Google Scholar]
- 6.Kiesslich R, Burg J, Vieth M, et al. Confocal laser endoscopy for diagnosing intraepithelial neoplasias and colorectal cancer in vivo . Gastroenterology. 2004;127:706–13. doi: 10.1053/j.gastro.2004.06.050. [DOI] [PubMed] [Google Scholar]
- 7.Gardner TB, Glass LM, Smith KD, et al. Pancreatic cyst prevalence and the risk of mucin-producing adenocarcinoma in US adults. Am J Gastroenterol. 2013;108:1546–50. doi: 10.1038/ajg.2013.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Girotra M, Park WG. Endoscopic ultrasound guided fine-needle aspiration and biopsy of pancreatic cysts. Tech Gastrointest Endosc. 2018;20:39–45. [Google Scholar]
- 9.Suzuki R, Thosani N, Annangi S, et al. Diagnostic yield of EUS-FNA-based cytology distinguishing malignant and benign IPMNs: A systematic review and meta-analysis. Pancreatology. 2014;14:380–4. doi: 10.1016/j.pan.2014.07.006. [DOI] [PubMed] [Google Scholar]
- 10.Gaddam S, Ge PS, Keach JW, et al. Suboptimal accuracy of carcinoembryonic antigen in differentiation of mucinous and nonmucinous pancreatic cysts: Results of a large multicenter study. Gastrointest Endosc. 2015;82:1060–9. doi: 10.1016/j.gie.2015.04.040. [DOI] [PubMed] [Google Scholar]
- 11.Jais B, Rebours V, Malleo G, et al. Serous cystic neoplasm of the pancreas: A multinational study of 2622 patients under the auspices of the International Association of Pancreatology and European Pancreatic Club (European Study Group on Cystic Tumors of the Pancreas) Gut. 2016;65:305–12. doi: 10.1136/gutjnl-2015-309638. [DOI] [PubMed] [Google Scholar]
- 12.Kamboj AK, Dewitt JM, Modi RM, et al. Confocal endomicroscopy characteristics of different intraductal papillary mucinous neoplasm subtypes. JOP. 2017;18:198–202. [PMC free article] [PubMed] [Google Scholar]
- 13.Giovannini M, Caillol F, Poizat F, et al. Feasibility of intratumoral confocal microscopy under endoscopic ultrasound guidance. Endosc Ultrasound. 2012;1:80–3. doi: 10.7178/eus.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Konda VJ, Meining A, Jamil LH, et al. A pilot study of in vivo identification of pancreatic cystic neoplasms with needle-based confocal laser endomicroscopy under endosonographic guidance. Endoscopy. 2013;45:1006–13. doi: 10.1055/s-0033-1344714. [DOI] [PubMed] [Google Scholar]
- 15.Elta GH, Enestvedt BK, Sauer BG, et al. ACG clinical guideline: Diagnosis and management of pancreatic cysts. Am J Gastroenterol. 2018;113:464–79. doi: 10.1038/ajg.2018.14. [DOI] [PubMed] [Google Scholar]
- 16.Napoléon B, Lemaistre AI, Pujol B, et al. A novel approach to the diagnosis of pancreatic serous cystadenoma: Needle-based confocal laser endomicroscopy. Endoscopy. 2015;47:26–32. doi: 10.1055/s-0034-1390693. [DOI] [PubMed] [Google Scholar]
- 17.Nakai Y, Iwashita T, Park DH, et al. Diagnosis of pancreatic cysts: EUS-guided, through-the-needle confocal laser-induced endomicroscopy and cystoscopy trial: DETECT study. Gastrointest Endosc. 2015;81:1204–14. doi: 10.1016/j.gie.2014.10.025. [DOI] [PubMed] [Google Scholar]
- 18.Karia K, Waxman I, Konda VJ, et al. Needle-based confocal endomicroscopy for pancreatic cysts: The current agreement in interpretation. Gastrointest Endosc. 2016;83:924–7. doi: 10.1016/j.gie.2015.08.080. [DOI] [PubMed] [Google Scholar]