

Abstract
Objectives:
The aim of this study was to test an intervention modifying officer physiology to reduce lethal force errors and improve health.
Methods:
A longitudinal, within-subjects intervention study was conducted with urban front-line police officers (n = 57). The physiological intervention applied an empirically validated method of enhancing parasympathetic engagement (ie, heart rate variability biofeedback) during stressful training that required lethal force decision-making.
Results:
Significant post-intervention reductions in lethal force errors, and in the extent and duration of autonomic arousal, were maintained across 12 months. Results at 18 months begin to return to pre-intervention levels.
Conclusion:
We provide objective evidence for a physiologically focused intervention in reducing errors in lethal force decision-making, improving health and safety for both police and the public. Results provide a timeline of skill retention, suggesting annual retraining to maintain health and safety gains.
Keywords: autonomic arousal, biofeedback, heart rate, heart rate variability, intervention, lethal force, occupational stress, performance, police, recovery, shooting, training, use of force
Learning Objectives
Become familiar with efforts to reduce error rates in the use of lethal force by police, including the findings of previous intervention studies.
Summarize the new intervention seeking to modify police officers’ physiology to reduce lethal force errors and improve health.
Discuss the findings of the new intervention study, including the effects on autonomic arousal and their persistence over follow-up.
Researchers have identified significant error rates in the application of lethal force among police in the United States.1 Lethal force errors result in significant personal and societal suffering, underscoring the urgency for effective interventions to reduce such errors. To date, interventions attempting to change psychosocial attitudes lack empirical support to improve health or demonstrate objective reductions in lethal force errors beyond what is achieved with skill-based (eg, tactical, weapons) occupational training.2 This study takes a novel approach to improving police health and safety outcomes by targeting physiological regulation during stress, and enhancing recovery following threatening encounters. Research has shown that excessive or prolonged responses to threat may interfere with occupational performance and raise health risks.3–7 The intervention applied in the current study aims to reduce negative health and safety outcomes by modulating the human physiological response to threat and stress, as discussed below.
Threat appraisal is a process occurring largely outside conscious awareness in neural circuits that are also responsible for imbuing meaning and personal relevance.8,9 During threat appraisal, the brain coordinates and stimulates cardiovascular physiology that supports metabolic and behavioral responses to threat, similar to meeting physical demands such as exercise. This neural coordination of rapid behavioral responses happens within milliseconds.8,10,11 Maladaptive physiological arousal (ie, too much or too little) in response to threat may hinder subsequent cognitive processes such as decision-making and situational awareness.12–15 Research conducted with police officers suggests that it is the modulation of cardiovascular arousal, rather than simply the reduction of arousal, that may be key in reducing lethal force decision errors. For example, researchers measured indices of autonomic arousal [heart rate (HR) and heart rate variability (HRV)] among police officers immediately before, and during, two high-intensity, realistic, and threatening encounters.16 Officers exhibiting excessive cardiovascular arousal before the scenarios were more likely to use lethal force when it was not necessary (ie, an error of inhibitory control), and that insufficient arousal led to missed threat cues that endangered the lives of the officers (ie, an error of disinhibition: not using lethal force when necessary).16 These findings demonstrate that autonomic arousal preceded the threat exposure, strengthening the hypothesis that maladaptive arousal plays a causative role in lethal force errors.
Responding to threat requires the engagement of the autonomic nervous system (ANS), which is comprised of sympathetic and parasympathetic branches. Good physical health and cognitive function are associated with a flexible balance between the two branches.10 Colloquial and empirical work often highlight activation of the sympathetic branch in response to threat, popularly referred to as the “fight or flight response.” Indeed, the impact of the fight or flight response can include perceptual distortions, tunnel vision, reduced fine motor skills, and loss of situational awareness; conditions that increase the probability of decision-making errors among police.13–15 Researchers have also identified that both chronic and acute stress are associated with impairments in inhibitory control (eg, shooting when not appropriate). For example, adults exposed to an intense social stressor displayed more inhibitory control errors on a subsequent rapid decision-making task than study participants not exposed to the acute social stress.12 Furthermore, researchers working with combat veterans found that those reporting PTSD, an anxiety condition associated with excessive sympathetic arousal, were more likely to make inhibitory control errors on a rapid decision-making task.17
Not to be overlooked, however, is the role of the parasympathetic branch in the regulation of arousal when facing a potential threat. Parasympathetic regulation of the heart, via the vagus nerve, is central in forming a flexible response to environmental demands. What is more, parasympathetic function is related to cognitive processes, such as decision-making and inhibitory control.12,18 Researchers have explored the role of parasympathetic engagement among police officers facing potentially threatening use of force encounters.19 Police officers were assigned to either reality-based scenario training (experimental condition) or static shooting training on a range (control condition). Results showed that officers in the experimental condition exhibited less suppression of parasympathetic influence during threat exposure and made fewer errors than officers in the control condition, who exhibited typical parasympathetic suppression.19,20 The findings contribute to the growing body of evidence showing that decision-making accuracy during threat exposure is reduced when there is a loss of parasympathetic influence.15
Maladaptive arousal associated with threat appraisal can be reduced by modifying HRV through conditioning. HRV biofeedback (HRV-BF) is one such method of teaching individuals to evoke periods of parasympathetic activation to modulate autonomic arousal during threat, and parasympathetic dominance for rapid recovery from threat (19, see p. 1 for explanation of HRV-BF). The ability to recover quickly following threat arousal is particularly relevant for police, considering how occupational stressors such as fatigue (eg, long hours, shift work) and multiple exposures to threat can impact decision-making and situational awareness.21 Fatigue is associated with maladaptive autonomic arousal that results in allostatic load, defined as “wear and tear on the body” that, over time, is associated with poor health and reduced cognitive function.10,18,22,23 Allostatic load also increases the probability of decision-making errors when an individual is fatigued or threatened, as evidenced by low and irregular cardiovascular arousal profiles.24 Previous research with police officers demonstrates the efficacy of using HRV-BF as an intervention to reduce errors in the decision to use lethal force.25 The current intervention utilized real-time HR and HRV biofeedback to stimulate physiologic changes that are consistent with parasympathetic activation. HR and HRV-BF techniques were applied during and following scenario-based threat exposures to train officers to (1) modulate autonomic arousal to match situational demands; and (2) condition rapid autonomic recovery to avoid fatigue. We hypothesized a reduction in lethal force decision errors following the intervention, and that the reduction in errors would be associated with autonomic arousal modulation and quicker recovery following threat exposure. The longitudinal study design is used to assess how long improvements following the study intervention may last, and at what time interval retraining or “booster sessions” are recommended.
METHODS
Participants
Fifty-seven active duty frontline police officers volunteered to participate in our within-subjects longitudinal study (Table 1). Participants were volunteers from a pool of approximately 750 frontline officers employed by a large urban police agency in Ontario, Canada. Participants provided informed consent before volunteering and were told that they could withdraw at any time with no consequence. A total of 81% of participants (47/57) returned for at least one follow-up evaluation at 6, 12, or 18 months, indicating a low attrition rate over the follow-up period [41 male, five female; M age = 33.4 (SD = 6.8), range = 23 to 47; M years of service = 7.5 (SD = 5.8), range = 1 to 28.6]. Of the officers who made errors at baseline, 89% (eight of nine) returned for follow-up assessment. All procedures were approved by the University of Toronto Research Ethics Board for Social Sciences and Humanities. All data, materials, and methods can be made available upon request to the corresponding author, with agreement to protect the confidentiality of research participants.
TABLE 1.
Demographic Information for Participants at Each Time Point During the Study
| Pre- and Post-intervention | 6-Month Evaluation | 12-Month Evaluation | 18-Month Evaluation | |
| n (Female) | 57 (7) | 39 (3) | 28 (3) | 29 (2) |
| M age (SD) | 32.8 (6.3) | 33.5 (6.9) | 33.6 (6.8) | 32.3 (6.0) |
| M years of service (SD) | 7.2 (5.6) | 7.7 (6.4) | 7.7 (7.0) | 6.9 (6.6) |
Sample size, mean age, mean years of service, and accompanying standard deviations are provided for pre- and post-intervention, 6-month, 12-month, and 18-month evaluations. Note that demographic data from one officer are missing.
Procedure
The present study used a longitudinal repeated-measures, within-subjects experimental design (Table 2). Officers were evaluated at five time points: pre-intervention, post-intervention (ie, on the final day of the intervention), 6-month evaluation, 12-month evaluation, and 18-month evaluation. At the beginning of each intervention and evaluation session, officers were fitted with training versions of their usual police equipment (eg, baton, conducted electrical weapon, gun, OC spray, full uniform), and a portable HR monitor that adhered to their skin under their clothing (Bodyguard 2; FirstBeat Technologies LTD, Jyväskylä, FI). On the pre-intervention evaluation day, officers completed four live-action, reality-based scenarios, one of which did not require a lethal force decision and was excluded from analyses. Therefore, pre-intervention evaluations are based on three lethal force decisions. Following the morning of pre-intervention evaluation, the intervention began with classroom-based lessons on HR and HRV-BF theory (see Table 2 for schedule). Day 2 to 3 consisted of practice sessions of HR monitoring, HRV-BF, and other training techniques (described in detail in25 and below) integrated during 12 scenarios. Day 4 consisted of the post-intervention evaluation that was a single extended scenario with three stages, and required three lethal force decisions. To maintain equivalency in number of decisions across time, 6-month, 12-month, and 18-month evaluations required officers to perform three scenarios with a single lethal force decision in each.
TABLE 2.
Experimental Design
| Schedule | Day 1 Evaluation | Day 2 Intervention | Day 3 Intervention | Day 4 Evaluation | 6-Month, 12-Month, and 18-Month Evaluation |
| Morning | Pre-intervention evaluation (three scenarios with one shoot/no shoot decision each) | Intervention: Reality-based training scenarios integrated with HRV-BF | Intervention: Reality-based training scenarios integrated with HRV-BF | Post-intervention evaluation: Three-stage, extended scenario with three shoot/no shoot decisions | Three scenarios with one shoot/no shoot decision each. Survey measures, equipment return |
| Afternoon | Intervention begins: Classroom psychoeducational component | Intervention: Reality-based training scenarios integrated with HRV-BF | Intervention: Reality-based training scenarios integrated with HRV-BF | Survey measures, equipment return |
HRV-BF, heart rate variability biofeedback.
Evaluation sessions at 6, 12, and 18 months were held during morning and afternoon blocks. Officers would attend either a morning or afternoon session, based on their schedule availability, and complete all three scenarios.
The Intervention
The components of the intervention include a classroom portion covering psychoeducational material (eg, brain and physiology, acute stress, allostatic load and the impact of stress on performance, situational awareness), and active occupationally relevant scenario-based training (described below). The classroom portion also explains what HRV-BF is and how to use it to increase parasympathetic activation during occupational exposures. In line with HRV-BF protocol by Lehrer and Gevirtz,20 participants were provided real-time, beat-by-beat HR data while engaging in HRV-BF exercises that produced a characteristic sine-wave-like curve of peaks and valleys in HR, indicating parasympathetic system activation. During the intervention period (Table 2), opportunities to engage in HRV-BF are provided during times of rest and before and after each scenario as a tool to train (1) the use of short periods of recovery to reduce allostatic load; and (2) the reduction of sympathetic dominance during psychologically threatening situations by activating parasympathetic activity.
Reality-Based Training Scenarios
Reality-based, live-action scenarios were utilized to enhance the ecological validity of the study, as they have been shown to stimulate motor learning neural pathways26,27 and induce autonomic conditioning that is comparable28 and robust to the stress of real-world encounters.29,30 To enhance ecological validity, the study was conducted at an empty school to allow for indoor and outdoor scenarios (eg, vehicle stops, room/apartment, and school environments), props were used to create realistic rooms and scenes (eg, blood, simulated weapons, scene-relevant attire, and furniture), scenario actors were comprised of experienced police officers and trainers, and firearms were loaded with Safe Shot blank ammunition that mimics the sound of live fire.
To adjust for potential confounds in scenario length and presentation, all scenarios were designed by expert Use of Force Instructors with more than 10 years of experience designing occupationally relevant training scenarios. The instructors were not part of the research team to avoid any research bias, and spent upwards of 3 months scripting, practicing and refining timing, movement and verbal communication in the scenarios to make sure they were challenging, but not unrealistic, in testing the fundamental police skills of situational awareness (ie, what is happening) and lethal force decision-making (shoot/no shoot).
Although all study scenarios required a lethal force decision, the content of the encounters was different to eliminate practice effects. However, inhibitory (no-shoot) and disinhibition (shoot) lethal force decisions were distributed across all evaluation time points (nine inhibitory control decisions and six disinhibition decisions in total). Given that this was a within-subjects design, with multiple (ie, three) use of force decisions made on each evaluation day, we are able to conclude that the order of lethal force decision type (inhibitory vs disinhibition) did not influence the probability that an error was made on subsequent decisions, as no participant made more than one error in a single evaluation day.
The scenarios used in the current study comprised of challenging encounters that officers are routinely exposed to. For the pre-intervention, 6-month, 12-month, and 18-month evaluations, scenarios involved responding to calls such as a break and enter, domestic disturbance, reported robbery, suicidal person, and an assault in progress. The post-intervention evaluation was an exceptionally challenging scenario (active school shooting). This post-test was selected to significantly challenge the officers so we could observe whether the intervention improved skills under severe stress.
Manipulation Check
To ensure scenarios were sufficiently realistic and stressful, changes in HR from rest to maximum during scenarios (HR_Max) were evaluated at each time point with paired samples t tests (Table 3). As with the main results analyses, HR_Max was averaged across multiple lethal force decisions performed during each evaluation. All scenarios revealed significant HR responses (P < 0.05) with large effect sizes. Resting HR did not differ across time points [F (3, 55) = 1.167, P = 0.331], and thus did not confound the HR_Max index analysis described in the following section.
TABLE 3.
Manipulation Check: Stress Responses to Critical Incident Scenarios
| Time | Baseline HR M (SD) | Max HR (During Scenario) M (SD) | t | P | Effect Size (d) |
| Pre-intervention (n = 57) | 76.73 (10.48) | 115.68 (19.57) | −16.670 | 0.000 | 2.48 |
| Post-intervention (n = 57*) | 76.73 (10.48) | 129.52 (25.46) | −14.499 | 0.000 | 2.71 |
| 6-month evaluation (n = 39) | 77.38 (10.18) | 122.53 (17.78) | −17.190 | 0.000 | 3.12 |
| 12-month evaluation (n = 28) | 82.31 (13.62) | 113.63 (16.88) | −12.631 | 0.000 | 2.04 |
| 18-month evaluation (n = 27) | 77.44 (11.85) | 111.31 (22.15) | −9.729 | 0.000 | 1.91 |
Heart rate was measured in beats per minute (bpm) and averaged across multiple lethal force decision-making opportunities at each evaluation. Mean and standard deviations for all participants are provided for each time point.
HR, heart rate.
*Average baseline HR was measured for each participant at the start of the 4-day intervention.
Measures
All of the following measures were recorded for each participant during the multiple scenarios presented on each of the five evaluation days.
Use of Force Decision-Making
Each time point evaluated three lethal force decisions. Errors in lethal force were defined as (1) failing to use lethal force when appropriate situational criteria have been met (error of disinhibition); or (2) use of lethal force when appropriate situational criteria had not been met (error of inhibition). All criteria for correct or incorrect performance were defined, observed, and evaluated by qualified and experienced Use of Force Instructors who were independent from the research study team.
Heart Rate
Continuous physiological HR data were recorded at a rate of 1 Hz (1 recording/sec) using Bodyguard 2 cardiovascular monitors (FirstBeat Technologies Ltd, Jyväskylä, FI) that have been validated for research purposes.31 Officers wore the monitors at each time point for the entire duration of study. One adhesive electrode patch was applied to the skin below the officers’ left collarbone and one was applied on the ribcage below the heart. Data were uploaded to a remote server, where they were de-identified (ie, officer badge number replaced with anonymous code) and analyzed offline. Two cardiovascular measures were analyzed in the present study: (1) an index of the peak HR (HR_Max) measured during critical incident scenarios relative to each officer's own average resting baseline HR (HR_Rest) recorded at the beginning of each evaluation day while seated, computed as [(HR_Max – HR_Rest)/(HR_Rest)], and (2) HR Recovery Time (HR_Recovery), which indicates the time (in seconds) for the officer's HR_Max to return to HR_Rest. Cases where the officer's HR_Max was equal to or less than their average HR_Rest (n = 14 of 424 total cases), or where HR did not recover to a value equal to or less than their individual HR_Rest (n = 13) were excluded from analyses. HR_Max and HR_Recovery values were averaged across scenarios to obtain a single value at each time point for each officer and were included in statistical analyses described in the following section.
Statistical Analyses
To determine the number of participants necessary to detect effects, we used G∗Power to conduct a power analysis with the following parameters: effect size f = 0.25, α = 0.05, power (1-β) = 0.8, number of groups (within-subjects) = 1, number of measurements (repeated-measures) = 4. The power analyses indicated a total sample size of 24 participants. Because our sample size at each time point exceeds this minimum, we have sufficient power to detect significant effects.
Use of force decision-making performance was operationalized by the error rate in use of lethal force at each time point. Error rates (risk ratio) were computed by dividing the total number of errors committed by all officers at each time point across all scenarios, by the total number of decision making opportunities at each time point. Computation of error rates was chosen as an appropriate method of analysis for our within-subject shoot/no shoot data. Results report the reduction in error rates relative to the pre-intervention baseline error rate.
Analyses of repeated-measures continuous physiological data (HR_Max and HR_Recovery) were conducted using generalized linear mixed model repeated-measures analyses of variance (ANOVAs)32 to account for unequal sample sizes at each time point (Table 1). Analyses were conducted in SPSS software (Version 24; IBM Canada LTD, Ontario, Canada). The exact sample sizes used to compute significance tests are reported in the axis legends in each figure. HR_Max had missing subject data post-intervention (n = 1) and at 18-month evaluations (n = 2) due to technical failure of the HR monitor. Missing subject data for HR_Recovery pre-intervention (n = 1) and post-intervention (n = 8) were due to participants not returning to their average resting HR following critical incident scenarios and having maximum HR lower than resting (n = 1). Two participants did not have HR_Recovery data at 18-month evaluation due to technical failure. A two-tailed criterion value of P less than 0.05 was used to establish statistical significance. Least squared difference (LSD) pairwise comparisons were conducted where applicable to probe differences in outcome measures between time points.
RESULTS
Impact of the Intervention on Lethal Force Decision-Making
To assess the impact of the intervention on lethal use of force decision-making (ie, performance), participant lethal force decision-making was assessed during critical incident scenarios. We calculated a risk ratio (number of errors/total number of decision-making opportunities) to assess the incidence of these high-stakes errors. The risk ratio indicated a relatively low incidence of lethal force decision errors pre-intervention, with only nine errors from a total of 171 decision-making opportunities (Fig. 1). Despite the low error at baseline, the intervention reduced subsequent post-intervention lethal force error rates by 67% to just three errors of a total 171 decisions. This reduction in performance error relative to pre-intervention was maintained at 6-month (84% reduction) and 12-month (77% reduction) follow-up, with only one error at each time point from a total of 117 and 84 decision-making opportunities, respectively. Although the lethal force error rate was still 35% below pre-intervention levels at 18-month evaluation (3 errors of 87 decision-making opportunities), it is an increase relative to all other post-intervention evaluation rates. All officers were exposed to the same scenarios in the same order. Scenarios were closely balanced in decisions of disinhibition6 and inhibition.9 The errors cannot be attributed to one single individual; with the exception of three instances (6 of all 17 errors in the study), all errors were made by different individuals. The majority of participants (80.7%, 46/57) returned for at least one follow-up evaluation, including those that made errors at baseline (eight of nine).
FIGURE 1.
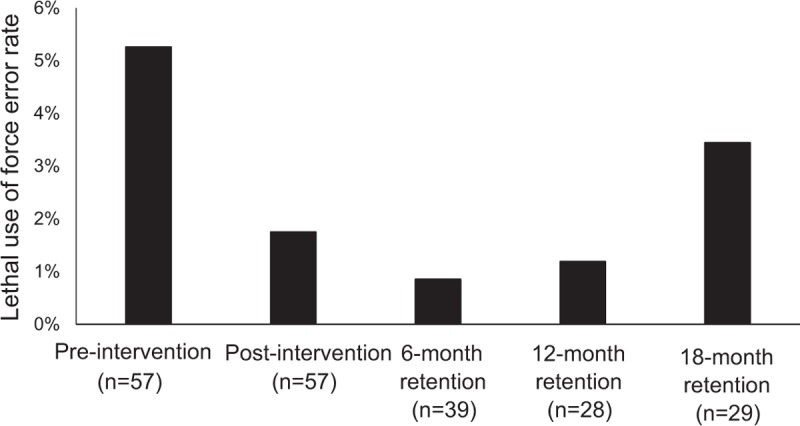
Lethal force error rates during critical incident scenarios before and after the physiological intervention. Performance (ie, correct shoot/no shoot decisions) was scored by expert Use of Force Instructors, and showed a 67% decrease in errors of lethal use of force following the physiological intervention (nine errors pre-intervention, three errors post-intervention of 171 opportunities), which was maintained at 6-month (1 error of 117 opportunities, 84% reduction) and 12-month (1 error of 84 opportunities, 77% reduction) evaluations. Gains in police performance began to reverse at 18-month retention evaluation (3 errors of 87 opportunities, 35% reduction relative to pre-intervention error rates). Retention of the participant sample was maintained throughout the study, with 81% of officers (46/57) returning for at least one follow-up evaluation conducted at 6, 12, and 18 months.
Autonomic Arousal
To assess the impact of the intervention on the modulation of autonomic arousal, we evaluated the average index HR_Max achieved during live action critical incident scenarios (see Methods for HR_Max Index calculation and scenario-type descriptions). A manipulation check ensured that all scenarios significantly stimulated autonomic arousal relative to officers’ individual resting HR (see Table 3). HR_Max significantly increased post-intervention (P = 0.002), decreased between 6 and 12 months (P = 0.000), and remained lower than post-intervention levels at 12-month and 18-month evaluations (P = 0.000) [F(4,57) = 8.894, P = 0.000] (Fig. 2). HR_Max was lower than pre-intervention levels at 12-month follow-up (P = 0.026) but began to increase at 18-month evaluation (P = 0.244).
FIGURE 2.
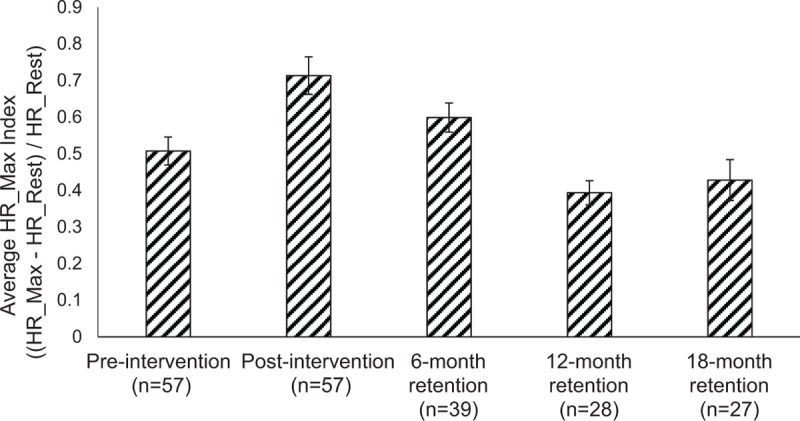
Indices of autonomic arousal during stressful critical incident scenarios. Relative to their individual resting baseline HR, officers’ maximum heart rate (HR_Max) increased significantly from pre- to post-intervention (P = 0.002). HR_Max at 12 months was significantly lower than all previous time points, but plateaued during scenarios evaluated at 18-month retention [F(4, 57) = 8.894, P = 0.000]. Error bars show standard error of the mean.
Recovery
To assess the impact of the intervention on the ability to recover from stressful police encounters, HR_Recovery (the time it took officers to return to their own average resting HR in seconds) was measured. HR_Recovery (Fig. 3) was significantly faster at 12-month follow-up relative to pre-intervention (p = 0.042), immediate post-intervention (P = 0.009), and 6-month evaluation (P = 0.004). HR_Recovery was also faster at 18-month follow-up relative to post-intervention (P = 0.019), and 6-month evaluation (P = 0.030), approaching significance relative to pre-intervention recovery time (P = 0.075), but was not different from 12-month recovery time (P = 0.177) [F(4, 61) = 5.094, P = 0.001]. HR_Recovery is a valid measure of parasympathetic engagement when the measurement follows physical activity, as it did in the current study.10 The variability in recovery time (shown by standard error bars) also decreased over time, demonstrating that the intervention was effective in reducing the number of outliers with extremely high or low recovery times.
FIGURE 3.

Autonomic recovery time following stressful critical incident scenarios. Recovery time (in seconds) from HR_Max during critical incident scenarios to average resting baseline was significantly faster at 12-month follow-up relative to pre-intervention (P = 0.042), post-intervention (P = 0.009), and 6-month evaluations (P = 0.004). Recovery time was also faster at 18-month follow-up relative to post-intervention (P = 0.019) and 6-month evaluations (P = 0.030), but plateaued after 12-month follow-up [P = 0.177) (F(4, 61) = 5.094, P = 0.001]. The variability (shown by error bars) in recovery time also decreased over time, demonstrating that the intervention was effective in reducing the number of outliers with extremely high or low recovery times. Error bars show standard error of the mean.
DISCUSSION
Our findings extend previous evidence supporting the efficacy of our HRV-BF intervention for enhancing police safety and health outcomes. The intervention, in conjunction with scenario-based training,25,28,33 suggests dramatically reduced objective errors in lethal force decision-making across an 18-month period (Fig. 1). Results also show significant improvements in the modulation of, not simply the reduction of, autonomic arousal appropriate to situational demands (Fig. 2). This is evident by mapping improvements in autonomic regulation relative to reductions in lethal force errors (Fig. 4). Further, significant improvement in the ability to recover from autonomic arousal after each scenario (Fig. 3) suggests that officers’ parasympathetic engagement was enhanced by practicing the intervention techniques over a 12-month follow-up period. The rise in lethal force errors and autonomic arousal at 18-month evaluation indicates that police retraining or “booster” sessions are recommended at a minimum frequency of every 12 months to maintain gains in health and safety.
FIGURE 4.
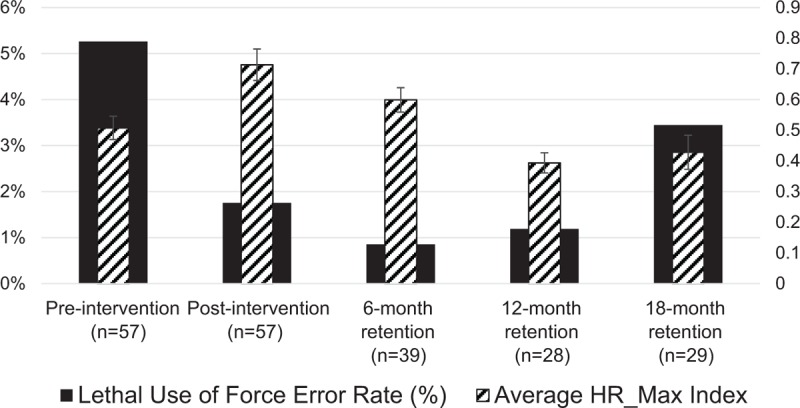
Mapping autonomic arousal and lethal use of force decision-making errors. When considered together, increased autonomic arousal at post-intervention and 6-month retention intervals (hatched bars) coupled with reduced lethal force errors (black bars) suggest improved modulation of autonomic arousal that is matched to the demands of threatening and occupationally relevant scenarios. With continued practice, autonomic arousal modulation and resultant improvements in police use of force decision-making (reflected by reduced error rates) are sustained at 12 and 18 months, supporting the efficacy of the current intervention.
Physiological Mechanism Underlying Gains in Performance and Health
Our findings fit well within the literature linking parasympathetic activation and scenario-based training with improved decision-making and inhibitory control during potentially threatening encounters.18,19 Autonomic arousal serves an important evolutionary advantage by promoting vigilance and attention to threat cues in the environment, while simultaneous parasympathetic activation balances the threat response by increasing perceptual accuracy. For example, researchers found that adults who were better able to regulate HR physiology in response to an acute social stressor (ie, parasympathetic engagement) displayed fewer inhibitory control errors on a rapid decision-making task.12 In relation to the current study, our results showing an increase in HR_Max during the post-intervention evaluation paired with low lethal force errors (Fig. 4) suggest that the intervention was successful in conditioning appropriate modulation of autonomic arousal to meet situational demands (ie, an active school shooting). Further, our results demonstrate that improvements in arousal modulation and lethal force decision making are sustained over time with continued practice.
Due to the physiologically demanding nature of shift work and multiple potentially threatening call outs per day, police are at risk of poor decision-making due to fatigue and allostatic load.21,24,34 Experimental evidence suggests that HRV-BF practice enhances automaticity of parasympathetic activity, in turn mediating the physiological benefits of recovery following stress.20 Just as with other physical skills, recovery is a physiological response that can be conditioned with repeated practice over time. Utilizing HRV-BF in combination with scenario-based training, the current intervention found improved recovery time following stressful encounters with continued practice. Specifically, recovery times ranged between 7 and 10 minutes at pre-intervention, post-intervention, and 6-month evaluations, and decreased significantly to 2.5 minutes at 12-month retention, and 3.6 minutes at 18-month retention (Fig. 3). Taken together, civilian and police research to date suggests that targeting parasympathetic regulation may be a valuable intervention for the enhancement of recovery and inhibitory control in general,12 and specifically among police, inhibiting shooting when not appropriate.16 The current findings lend support to using HRV-BF as an effective and ecologically valid intervention that does not require specialized equipment or significant time commitment once learned, and can combat occupationally induced fatigue to improve health and safety (ie, lethal force decision-making) among police.
Implications and Recommendations for Frequency and Duration of Training
The scientific literature does not indicate an exact duration or frequency of repeated physical practice to develop mastery or expertise of novel skills. It has been shown that the speed and proficiency of motor learning depends on many factors, including physicality, existing skill level (ie, novice vs expert learning), and the level of arousal during initial encoding.35–37 There are indications that functional brain activity begins to be altered after learning a novel motor sequence as early as 5 days into training nonexperts,38 and after 5 to 7 weeks of training among experts.39,40 These learning-induced changes to performance and neurophysiology can persist 2 to 4 months post-intervention with no further practice41 or even longer with continued practice and performance reflecting consolidation of novel procedural skills into implicit memory.39,42 Encouraging research from cognitive psychology that examines many types of experts suggests that as learning is reinforced over years of deliberate practice and/or regular “refresher” training, changes to brain organization are further solidified.42–46 Therefore, if the newly acquired skills are not rehearsed and done so repeatedly under a variety of conditions, there is a greater risk that they will fade.47 Although there is no existing neurological evidence for the extent and duration of learning-induced plasticity in police officers, the current results are in line with existing research supporting physiologically mediated efficacy of scenario-based training in improving police decision-making under stress.48,49 In addition, the current results demonstrate learning gains in performance after only 4 days of scenario training (Fig. 1), and in managing physiological stress responses and recovery after longer post-intervention durations. On the basis of this literature and the current findings, we recommend police use of force training should incorporate (1) scenario-based approaches that prepare the learner for a wide range of possible situations and outcomes in the real world,28,50–52 and allows for concurrent training and evaluation to occur; (2) Physiologically targeted methodology, including HRV-BF to condition the modulation of, and recovery from, autonomic stress responses33,53; and (3) refresher or recertification training at least every 12 months to ensure retention and consolidation of skill learning.
Our results build upon a pilot randomized controlled trial (RCT) using the same intervention with law enforcement (advanced tactical officers),25 indicating that the association between parasympathetic enhancement and improved lethal force decision-making occurs even in the presence of significant sympathetic arousal. In the RCT, all officers exhibited significant increases in HR arousal (65 to 91 bpm) during lethal force decision-making scenarios. Yet, officers in the experimental group who had received the HRV-BF intervention targeting parasympathetic enhancement exhibited significantly fewer errors in lethal use of force than officers in the control group despite significant sympathetic arousal.25 The current study extends these findings by demonstrating a maintenance in gains to performance and health up to 12 months post-intervention, after which errors in lethal use of force, autonomic arousal, and autonomic recovery times plateau. Although these measures do not return to pre-intervention levels, they suggest an optimal window for police retraining to be within 12 months. The increase in error rate from 12 to 18 months is not associated with a change in the MaxHR_Index. This suggests that the increase in error rate is associated with more subtle changes in stress physiology such as changes in HRV characteristic of parasympathetic withdrawal. This is an area for future investigation using a larger dataset.
Limitations
Given the significant challenges of conducting a longitudinal repeated-measures RCT within an ecologically valid setting, a control group was not included in this study. However, a within-subjects design allowed us to maximize power to detect effects and reveal the potential long-term maintenance of intervention gains (see Statistical Analysis section in Methods). In addition, we maintain a high level of participant retention, with 81% (46 of 57) of officers returning for at least one follow-up evaluation conducted 6, 12, and 18 months post-intervention. This level of attrition is especially impressive considering participants were active duty officers who took part in the study on a voluntary basis and did not receive extra compensation for their time and participation in the study.
IMPLICATIONS AND CONCLUSION
When considering the gravity of lethal force errors for public and police safety, any improvements in training lethal force decision-making can be translated into potential lives saved. Understanding the objective, physiological, and largely unconscious nature of the threat appraisal process and its associated behavioral responses sheds light on why occupational interventions that target purely cognitive pathways (eg, attitude change) or repetitive weapons practice (eg, traditional use of force training) may not result in dramatic reductions in lethal force decision errors related to threat responding. Our work addresses the broader scientific endeavor to understand the interaction between physiology and ecologically valid decision-making during high-stakes events. Simultaneously, our results reveal an empirically based approach to rapidly reducing objective errors in lethal force decisions among police, an application of significant societal concern.
Acknowledgments
The authors would like to acknowledge and thank all research assistants and volunteers in the Health Adaptation Research on Trauma (HART) Lab who assisted in the collection and cleaning/coding of the data. Thank you to all the police officers who participated in the study. Thank you to the agency who collaborated with us to make the data collection possible.
Footnotes
JPA did the conceptual framework, codevelopment of the intervention (psychophysiology), data collection, manuscript writing. PMD did the data analysis, manuscript writing. BB - data collection, data analysis, manuscript editing. EB did the data collection, data organization and analysis, manuscript preparation. HG did the codevelopment of the intervention (police tactics), data collection, manuscript editing. SP edited existing intervention materials to match the skill level of study participants, data collection, manuscript preparation. JA did the conceptual framework, intervention codevelopment (HRV-BF, cardiovascular physiology), manuscript writing.
Funding of this project was provided by a grant from the Government of Ontario Ministry of Labour (ROP 15-R-021), which funded data collection. However, the Ministry had no other involvement in the conceptualization, design, analysis, decision to publish, or preparation of this manuscript.
Data used in the current study are housed on a secure server at the University of Toronto and available on request from the lead author.
Andersen, Di Nota, Beston, Boychuk, Gustafsberg, Poplawski, and Arpaia have no relationships/conditions/circumstances that present potential conflict of interest.
The JOEM editorial board and planners have no financial interest related to this research.
REFERENCES
- 1.Ross CT. A multi-level Bayesian analysis of racial Bias in police shootings at the county-level in the United States, 2011–2014. PLoS One 2015; 10:2011–2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Paluck EL. Diversity training and intergroup contact: a call to action research. J Soc Issues 2006; 62:577–595. [Google Scholar]
- 3.Nieuwenhuys A, Oudejans RRD. Effects of anxiety on handgun shooting behavior of police officers: a pilot study. Anxiety Stress Coping 2010; 23:225–233. [DOI] [PubMed] [Google Scholar]
- 4.Nieuwenhuys A, Cañal-Bruland R, Oudejans RRD. Effects of threat on police officers’ shooting behavior: anxiety, action specificity, and affective influences on perception. Appl Cogn Psychol 2012; 26:608–615. [Google Scholar]
- 5.Nieuwenhuys A, Savelsbergh GJP, Oudejans RRD. Shoot or don’t shoot? Why police officers are more inclined to shoot when they are anxious. Emotion 2012; 12:827–833. [DOI] [PubMed] [Google Scholar]
- 6.Violanti JM, Gehrke A. Police trauma encounters: precursors of compassion fatigue. Int J Emerg Ment Health 2004; 6:75–80. [PubMed] [Google Scholar]
- 7.Violanti JM, Fekedulegn D, Andrew ME, et al. The impact of perceived intensity and frequency of police work occupational stressors on the cortisol awakening response (CAR): findings from the BCOPS study. Psychoneuroendocrinology 2017; 75:124–131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ginty AT, Kraynak TE, Fisher JP, Gianaros PJ. Cardiovascular and autonomic reactivity to psychological stress: neurophysiological substrates and links to cardiovascular disease. Auton Neurosci 2017; 207:2–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.LeDoux JE, Pine DS. Using neuroscience to help understand fear and anxiety: a two-system framework. Am J Psychiatry 2016; 173:1083–1093. [DOI] [PubMed] [Google Scholar]
- 10.Thayer JF, Sternberg E. Beyond heart rate variability: vagal regulation of allostatic systems. Ann N Y Acad Sci 2006; 1088:361–372. [DOI] [PubMed] [Google Scholar]
- 11.Barrett LF, Bar M. See it with feeling: affective predictions during object perception. Philos Trans R Soc B Biol Sci 2009; 364:1325–1334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Roos LE, Knight EL, Beauchamp KG, et al. Acute stress impairs inhibitory control based on individual differences in parasympathetic nervous system activity. Biol Psychol 2017; 125:58–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kalisch R, Müller MB, Tüscher O. A conceptual framework for the neurobiological study of resilience. Behav Brain Sci 2015; 38:e92. [DOI] [PubMed] [Google Scholar]
- 14.Klinger DA, Brunson RK. Police officers’ perceptual distortions during lethal force situations: informing the reasonableness standard. Criminol Public Policy 2009; 8:117–140. [Google Scholar]
- 15.Laborde S, Raab M, Kinrade NP. Is the ability to keep your mind sharp under pressure reflected in your heart? Evidence for the neurophysiological bases of decision reinvestment. Biol Psychol 2014; 100:34–42. [DOI] [PubMed] [Google Scholar]
- 16.Haller J, Raczkevy-Deak G, Gyimesine KP, Szakmary A, Farkas I, Vegh J. Cardiac autonomic functions and the emergence of violence in a highly realistic model of social conflict in humans. Front Behav Neurosci 2014; 8:364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Swick D, Honzel N, Larsen J, Ashley V, Justus T. Impaired response inhibition in veterans with post-traumatic stress disorder and mild traumatic brain injury. J Int Neuropsychol Soc 2012; 18:917–926. [DOI] [PubMed] [Google Scholar]
- 18.Thayer JF, Hansen AL, Saus-Rose E, Johnsen BH. Heart rate variability, prefrontal neural function, and cognitive performance: the neurovisceral integration perspective on self-regulation, adaptation, and health. Ann Behav Med 2009; 37:141–153. [DOI] [PubMed] [Google Scholar]
- 19.Saus E-R, Johnsen BH, Eid J, Riisem PK, Andersen R, Thayer JF. The effect of brief situational awareness training in a police shooting simulator: an experimental study. Mil Psychol 2006; 18:3–21. [Google Scholar]
- 20.Lehrer PM, Gevirtz R. Heart rate variability biofeedback: how and why does it work? Front Psychol 2014; 5:756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Vila BJ, Morrison GB, Kenney DJ. Improving shift schedule and work-hour policies and practices to increase police officer performance, health, and safety. Police Q 2002; 5:4–24. [Google Scholar]
- 22.Clark MS, Bond MJ, Hecker JR. Environmental stress, psychological stress and allostatic load. Psychol Health Med 2007; 12:18–30. [DOI] [PubMed] [Google Scholar]
- 23.McEwen BS. Sleep deprivation as a neurobiologic and physiologic stressor: allostasis and allostatic load. Metabolism 2006; 55 Suppl 2:23–26. [DOI] [PubMed] [Google Scholar]
- 24.Schmitt L, Regnard J, Desmarets M, et al. Fatigue shifts and scatters heart rate variability in elite endurance athletes. PLoS One 2013; 8:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Andersen JP, Gustafsberg H. A training method to improve police use of force decision making: a randomized controlled trial. SAGE Open 2016; 6:2. [Google Scholar]
- 26.Debarnot U, Sperduti M, Di Rienzo F, Guillot A. Experts bodies, experts minds: how physical and mental training shape the brain. Front Hum Neurosci 2014; 8:1–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bernstein LJ, Beig S, Siegenthaler AL, Grady CL. The effect of encoding strategy on the neural correlates of memory for faces. Neuropsychologia 2002; 40:86–98. [DOI] [PubMed] [Google Scholar]
- 28.Andersen JP, Pitel M, Weerasinghe A, Papazoglou K. Highly realistic scenario based training simulates the psychophysiology of real world use of force encounters: implications for improved police officer performance. J Law Enforc 2016; 5:1–13. [Google Scholar]
- 29.Pryor K. Don’t Shoot the Dog–the New Art of Teaching and Training (Revised). New York, NY: Bantam Books; 1999. [Google Scholar]
- 30.Smith AM, Floerke VA, Thomas AK. Retrieval practice protects memory against acute stress. Science 2016; 354:1046–1048. [DOI] [PubMed] [Google Scholar]
- 31.Teisala T, Mutikainen S, Tolvanen A, et al. Associations of physical activity, fitness, and body composition with heart rate variability-based indicators of stress and recovery on workdays: a cross-sectional study. J Occup Med Toxicol 2014; 9:16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Field A. Discovering Statistics Using SPSS. 2nd ed.2005; London, UK: Sage Publication, 821 p. [Google Scholar]
- 33.Andersen JP, Dorai M, Papazoglou K, Arnetz BB. Diurnal and reactivity measures of cortisol in response to intensive resilience and tactical training among special forces police. J Occup Environ Med 2016; 58:e242–e248. [DOI] [PubMed] [Google Scholar]
- 34.Anderson GS, Litzenberger R, Plecas D. Physical evidence of police officer stress. Polic An Int J Police Strateg Manag 2002; 25:399–420. [Google Scholar]
- 35.Calvo-Merino B, Grèzes J, Glaser DE, Passingham RE, Haggard P. Seeing or doing? Influence of visual and motor familiarity in action observation. Curr Biol 2006; 16:1905–1910. [DOI] [PubMed] [Google Scholar]
- 36.LaBar KS, Cabeza R. Cognitive neuroscience of emotional memory. Nat Rev Neurosci 2006; 7:54–64. [DOI] [PubMed] [Google Scholar]
- 37.Williams AM, Ericsson KA. Perceptual-cognitive expertise in sport: some considerations when applying the expert performance approach. Hum Mov Sci 2005; 24:283–307. [DOI] [PubMed] [Google Scholar]
- 38.Cross ES, Kraemer DJM, Hamilton AFDC, Kelley WM, Grafton ST. Sensitivity of the action observation network to physical and observational learning. Cereb Cortex 2009; 19:315–326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Bar RJ, DeSouza JFX. Tracking plasticity: effects of long-term rehearsal in expert dancers encoding music to movement. PLoS One 2016; 11:e0147731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Cross ES, Hamilton AF, Grafton ST. Building a motor simulation de novo: observation of dance by dancers. Neuroimage 2006; 31:1257–1267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Driemeyer J, Boyke J, Gaser C, Buchel C, May A. Changes in gray matter induced by learning: revisited. PLoS One 2008; 3:e2669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Di Nota PM, Levkov G, Bar R, DeSouza JFX. Lateral occipitotemporal cortex (LOTC) activity is greatest while viewing dance compared to visualization and movement: learning and expertise effects. Exp Brain Res 2016; 234:2007–2023. [DOI] [PubMed] [Google Scholar]
- 43.Ericsson KA. Deliberate practice and acquisition of expert performance: a general overview. Acad Emerg Med 2008; 15:988–994. [DOI] [PubMed] [Google Scholar]
- 44.Gaser C, Schlaug G. Brain structures differ between musicians and non-musicians. J Neurosci 2003; 23:9240–9245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lotze M, Scheler G, Tan HRM, Braun C, Birbaumer N. The musician's brain: functional imaging of amateurs and professionals during performance and imagery. Neuroimage 2003; 20:1817–1829. [DOI] [PubMed] [Google Scholar]
- 46.Calvo-Merino B, Glaser DE, Grèzes J, Passingham RE, Haggard P. Action observation and acquired motor skills: an fMRI study with expert dancers. Cereb Cortex 2005; 15:1243–1249. [DOI] [PubMed] [Google Scholar]
- 47.Miltenberger RG. Behavior Modification: Principles and Procedures. 3rd ed.Belmont, CA: Thomson Wadsworth; 2004. [Google Scholar]
- 48.Armstrong J, Clare J, Plecas D. Monitoring the impact of scenario-based use-of-force simulations on police heart rate: evaluating the Royal Canadian Mounted Police Skills Refresher Program. West Crim Rev 2014; 15:51–59. [Google Scholar]
- 49.Nieuwenhuys A, Oudejans RRD. Training with anxiety: short-and long-term effects on police officers’ shooting behavior under pressure. Cogn Process 2011; 12:277–288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Barney C, Shea SC. The art of effectively teaching clinical interviewing skills using role-playing: a primer. Psychiatr Clin North Am 2007; 30:31–50. [DOI] [PubMed] [Google Scholar]
- 51.McNaughton N, Ravitz P, Wadell A, Hodges BD. Psychiatric education and simulation: a review of the literature. Can J Psychiatry 2008; 53:85–93. [DOI] [PubMed] [Google Scholar]
- 52.Krameddine YI, DeMarco D, Hassel R, Silverstone PH. A novel training program for police officers that improves interactions with mentally ill individuals and is cost-effective. Front Psychiatry 2013; 4:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Brisinda D, Venuti A, Cataldi C, Efremov K, Intorno E, Fenici R. Real-time imaging of stress-induced cardiac autonomic adaptation during realistic force-on-force police scenarios. J Police Crim Psychol 2015; 30:71–86. [Google Scholar]