

To the Editor:
Cardiac rhabdomyoma is the most common fetal cardiac tumor.1 We report a case of progressively obstructive fetal cardiac rhabdomyomas with regression in utero during treatment of the mother with an oral mechanistic target of rapamycin (mTOR) inhibitor.
Cardiac rhabdomyomas were diagnosed in a fetus at 21 weeks of gestation by means of fetal echocardiography; the probable diagnosis of tuberous sclerosis complex was made by association. Progressive tumor growth and bilateral outflow tract obstruction were noted at 30 weeks of gestation (Fig. 1A), with supraventricular tachycardia and impending hydrops fetalis. Considerations of the multidisciplinary team included extensive surgical debulking, premature delivery with extracorporeal membrane oxygenation, and the use of prostaglandin; each of these options was limited by high risk and a low probability of success.
Figure 1. Findings on Echocardiography before and after Birth.
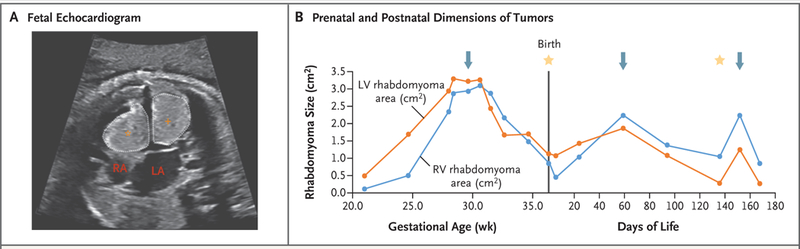
Panel A shows a fetal echocardiogram in the apical four-chamber view at 30 weeks of gestation. Two large echogenic intracardiac masses are shown: one in the right ventricle (RV) (star) and one in the left ventricle (LV) (cross). The dotted lines indicate the areas measured. RA denotes right atrium, and LA left atrium. Panel B shows changes over time in the area of the masses in the RV and the LV on the same echocardiographic view in serial studies. The points on each line denote individual echocardiographic measurements of the area of each mass, arrows the initiation of sirolimus, and stars discontinuation of sirolimus.
Oral sirolimus was initiated in the mother with a target maternal serum trough level of 10 to 15 ng per milliliter, with subsequent tumor regression in utero (Fig. 1B). Delivery occurred at 36 weeks of gestation. The cord-blood sirolimus level was 11.3 ng per milliliter, and the concurrent level in the mother was 6.9 ng per milliliter. After birth, the tumor progressed while the infant was not receiving therapy. Sirolimus was initiated in the infant at 2 months of age, with a target trough level of 10 to 15 ng per milliliter. Tumor regression was again noted after 3 weeks. A similar pattern occurred when sirolimus was discontinued at 4.5 months of age, with tumor progression and then repeat regression after restarting therapy. Brain imaging revealed no lesions.
At 9 months of follow-up, no clinical seizures or epileptiform activity were noted on electro-encephalography, and appropriate somatic growth and development had occurred. Genetic testing revealed a pathogenic variant, c.1781delT (p.Val594Glyfs*35), in TSC1, which confirmed the diagnosis of tuberous sclerosis complex (see the Supplementary Appendix, available with the full text of this letter at NEJM.org).
In this case, we used oral sirolimus in a mother to treat fetal cardiac rhabdomyomas noninvasively. The choice of therapy was based on a high likelihood of concurrent tuberous sclerosis complex1 and reports of success after birth with mTOR inhibitors for treatment of cardiac rhabdomyoma in infants with tuberous sclerosis complex.2,3 The dose of sirolimus used in the mother was based on accepted guidelines for solid-organ transplantation in adults.4 It is possible that the primary form of transplacental transfer was through a unidirectional enzyme transporter mechanism (see the Supplementary Appendix). Regression of tumors correlated with administration of sirolimus both prenatally and postnatally in a fetus with a high risk of death.5
At 9 months of follow-up, the infant continued to receive sirolimus with appropriate somatic growth and development. Further study is required to determine the efficacy, safety, and most appropriate dosing of oral sirolimus in mothers for the treatment of fetal cardiac rhabdomyoma.
Supplementary Material
Footnotes
Disclosure forms provided by the authors are available with the full text of this letter at NEJM.org.
Contributor Information
Benjamin T. Barnes, Johns Hopkins University, Baltimore, MD
David Procaccini, Johns Hopkins Hospital, Baltimore, MD
Jude Crino, Johns Hopkins Hospital, Baltimore, MD
Karin Blakemore, Johns Hopkins Hospital, Baltimore, MD
Priya Sekar, Johns Hopkins University, Baltimore, MD
Katelynn G. Sagaser, Johns Hopkins Hospital, Baltimore, MD
Angie C. Jelin, Johns Hopkins Hospital, Baltimore, MD
Lasya Gaur, Johns Hopkins University, Baltimore, MD
References
- 1.Fesslova V, Villa L, Rizzuti T, Mastrangelo M, Mosca F. Natural history and long-term outcome of cardiac rhabdomyomas detected prenatally. Prenat Diagn 2004;24:241–8. [DOI] [PubMed] [Google Scholar]
- 2.Breathnach C, Pears J, Franklin O, Webb D, McMahon CJ. Rapid regression of left ventricular outflow tract rhabdomyoma after sirolimus therapy. Pediatrics 2014;134(4):e1199–202. [DOI] [PubMed] [Google Scholar]
- 3.Demir HA, Ekici F, Yazal Erdem A, Emir S, Tunç B. Everolimus: a challenging drug in the treatment of multifocal inoperable cardiac rhabdomyoma. Pediatrics 2012;130(1):e243–e247. [DOI] [PubMed] [Google Scholar]
- 4.Costanzo MR, Dipchand A, Starling R, et al. The International Society of Heart and Lung Transplantation guidelines for the care of heart transplant recipients. J Heart Lung Transplant 2010;29:914–56. [DOI] [PubMed] [Google Scholar]
- 5.Chao AS, Chao A, Wang TH, et al. Outcome of antenatally diagnosed cardiac rhabdomyoma: case series and a meta-analysis. Ultrasound Obstet Gynecol 2008;31:289–95. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.