

Abstract
Study Design.
This study combined all prior research involving human volunteers in low-speed rear-end impacts and performed a comparative analysis of real-world crashes using the National Automotive Sampling System – Crashworthiness Data System.
Objective.
The aim of this study was to assess the rates of neck pain between volunteer and real-world collisions as well as the likelihood of an injury beyond symptoms as a function of impact severity and occupant characteristics in real-world collisions.
Summary of Background Data.
A total of 51 human volunteer studies were identified that produced a dataset of 1984 volunteer impacts along with a separate dataset of 515,601 weighted occupants in real-world rear impacts.
Methods.
Operating-characteristic curves were created to assess the utility of the volunteer dataset in making predictions regarding the overall population. Change in speed or delta-V was used to model the likelihood of reporting symptoms in both real-world and volunteer exposures and more severe injuries using real-world data. Logistic regression models were created for the volunteer data and survey techniques were used to analyze the weighted sampling scheme with the National Automotive Sampling System database.
Results.
Symptom reporting rates were not different between males and females and were nearly identical between laboratory and real-world exposures. The minimal risk of injury predicted by real-world exposure is consistent with the statistical power of the large number of volunteer studies without any injury beyond the reporting of neck pain.
Conclusion.
This study shows that volunteer studies do not under-report symptoms and are sufficient in number to conclude that the risk of injury beyond neck strain under similar conditions is essentially zero. The real-world injury analyses demonstrate that rear impacts do not produce meaningful risks of cervical injury at impacts of similar and greater severity to those of the volunteer research. Future work concerning the mechanism of whiplash-related trauma should focus on impacts of severity greater than those in the current literature.
Level of Evidence: 3
Keywords: NASS, neck strain, rear impact, volunteer, whiplash
Whiplash-associated disorder (WAD) is a major concern worldwide with neck pain being the most common complaint following a motor vehicle collision.1 The cost of whiplash is difficult to quantify, due to variations in definitions and data collection, but in the United States, WAD has been estimated to cost $2.7 billion per year. The United Kingdom, with an annual cost of over $3 billion, has been called “the whiplash capital of the world.”2,3 The UK also reports that about 70% of motor vehicle collision personal injury claims are for WAD.4
WAD has been studied using a variety of data sources and methods to answer specific or general questions about its etiology. These studies include retrospective analyses of the association between occupant characteristics, symptoms, and crash parameters as well as prospective testing using crash test dummies, cadavers, and human volunteers. Retrospective studies have found that crash environment, subject's age, anticipation of the crash, and gender play a role in the duration and severity of reported symptoms, revealing a mix of biological, psychological, and social factors involved in post-crash outcomes (63). Castro12 published a study documenting WAD symptoms in patients following a placebo rear-end collision. Twenty percent of these subjects reported whiplash-like symptoms within 3 days of the event, even though no crash took place [13]. Thus, a confounding factor in assessing WAD is that researchers use symptoms synonymously with injury. Pain is expected to immediately follow an acute traumatic injury, but the expression of pain does not necessarily mean that there has been an acute traumatic injury.
From a biomechanical perspective, low-speed events have been evaluated extensively using human volunteers.5–68 Experiments using large numbers of volunteers exposed to rear impacts have produced data regarding the kinematic and kinetic responses and reported symptoms of human occupants. These studies have used a wide range of subjects and conditions such as impact severity, awareness of the impending impact, initial position, posture, and seat and head restraint characteristics. The results reported vary by study and include head acceleration, kinematics, and high-speed cineradiography of the cervical spine during the test.
Previous authors have studied the volunteer literature at various times. In 1996, Szabo and Welcher58 compiled 284 volunteer crash tests at changes in velocity (delta V) up to 14 kph, including 10 publications and three sources of unpublished data. None of the volunteers had symptoms lasting longer than 7 days. In 2005, Moss et al.69 analyzed 28 studies, representing 206 exposures. Fifty-nine percent of those exposed had symptoms, most of which resolved within 12 days. In 2007, Nordhoff et al.70 published a collection of 18 papers and 62 abstracts regarding rear-end collisions, which represented a review of the state of biomechanical literature at that time. There has been extensive volunteer testing since, but no subsequent review until now.
The goal of this paper is to add to the number of volunteer exposures available for analysis and compare these data with real-world collisions of similar severity from the NASS CDS database.
MATERIALS AND METHODS
For this study, symptoms are not synonymous with injury, but only indicate that the volunteer reported symptoms for a given period of time. Within volunteer studies, symptoms are not only likely related to muscle strain but also may be due to the psychological influence of these events71 and, therefore, are not necessarily indicative of structural tissue damage. In this study, injury is defined as traumatic structural damage to a tissue (bone, ligament, tendon, disc) with an objective finding. If no injury is described in the article, then that volunteer is denoted as uninjured in our dataset. This is a reasonable assumption, as ethically authors would be obligated to report any traumatic injury and, from a scientific standpoint any objective injury would be described to provide data regarding what injuries are produced and under what conditions. Strains should also be differentiated from sprains in that strains are injuries of the musculature caused by stretching and tearing of the muscle fibers, whereas sprains are injuries of the ligaments resulting from stretching or tearing of the ligamentous tissue.
Data Sources
Volunteer Studies
The data used for this study were collected from individually published studies that performed rear impact testing on human volunteers. Studies were identified through an exhaustive search of the literature as well as obtaining referenced work within the articles themselves. Articles from the same authors or institution were screened to identify publications reporting the same tests to ensure that a single volunteer exposure was not included multiple times. When reported, volunteer or test identification was recorded in the final dataset to facilitate identification of repeated reporting of the same exposure. Some studies were excluded due to lack of sufficient data to identify the number of volunteers or number of exposures experienced by the volunteers. Otherwise, all studies using human volunteers were included regardless of the level of information provided regarding the test conditions.
Operating-characteristic (OC) curves were created to assess the utility of the volunteer dataset in making predictions regarding the overall population. OC curves are commonly used to assess the statistical power (Pa) that a sample (n) has in predicting the likelihood that there were no defective items (seriously injured volunteers) in the population of human subjects involved in experimental rear impacts. For this study, OC curves were calculated to determine the level of statistical confidence that the human population will not sustain an injury beyond the reported short-term symptoms during a minor rear impact based on the number of available individual volunteers. Multiple exposures of a single volunteer were not included in the OC curve calculations. The probability of acceptance is determined by the binomial distribution and assumes that the population is a random process taken from an infinite lot. The probability of acceptance is the likelihood that the actual number of defectives (d) is less than or equal to the acceptable number (c).
 |
In this study, the OC curve provides the level of certainty for an assumed underlying risk of injury for the population based on the number of injuries within the sample of volunteers. The OC curve will provide the likelihood that no volunteer would sustain an injury for a given number of samples and an assumed level of risk. The higher the underlying risk of injury, the more likely that an injured volunteer would be within the sample.
Real-World Outcomes
A second dataset of rear impacts was analyzed using the National Automotive Sample System (NASS) Crashworthiness Data System (CDS) database. The NASS database represents a collection of real-world crashes that are investigated by the National Highway Traffic Safety Administration (NHTSA). Approximately 4000 to 5000 crashes are investigated annually and about half are reconstructed to determine the change in speed experienced by the struck vehicle. In addition, a large number of variables describing the accident, vehicle, and occupants involved are collected. The NASS database was queried for vehicles exposed to rear impacts defined as having a Principal Direction of Force (PDOF) between 5 and 7 o’clock. Only those exposed to a single event, meaning the vehicle did not contact any other object during the accident, were included. The occupants were limited to the front outboard positions over the age of 16. Only vehicles with a known change in speed and occupants with a known treatment were included to ensure proper documentation of injured and uninjured occupants. The NASS database contains information regarding the injuries sustained by the occupants in the form of their Abbreviated Injury Scale (AIS) identifier.72 This number identifies the type of injury and the specific anatomical structure involved. The NASS dataset uses a specific code, which is defined as whiplash or a neck muscle strain (640278). This AIS code was used to identify occupants diagnosed with neck strain or who self-reported the presence of neck strain. The occurrence of neck strain in the NASS database was compared with that within the volunteer dataset
The two refined datasets were analyzed using the Statistical Analysis Software (SAS, 9.4, Cary, NC) and Microsoft Excel (2013, Redmond, WA). Statistics were performed to provide an understanding of the overall make-up of the available testing using human volunteers. Additional analyses were performed to answer specific questions based on the data available. Differences among proportional outcomes were tested for significance using the Fisher exact test.
RESULTS
Volunteer Database
A complete collection of the available volunteer literature resulted in a dataset of 1984 total volunteer exposures from 51 individual studies.5–10,12,15–18,22–26,28–32,34–41,43,46–54,56–59,61–64,66–68,73 On average, each study performed 40 tests with a range from 1 to 484 tests and used 51 subjects with a range of 1 to 65 volunteers per study. Many of the volunteers experienced more than one exposure (Figure 1). Within the complete dataset, 52% of the impacts were at a delta-V less than 2 mph and a significant number had repeated exposures at very low (<1.5 kph, ∼1 g impacts) severities. The acceleration produced by these impacts is not expected to produce a meaningful response of the volunteers in terms of producing injury and the large number of these exposures would weigh the dataset toward more minor events. Therefore, impacts with a change in speed less than 1.5 kph were removed from the complete dataset. This reduced the dataset to a total of 1251 volunteer exposures (Figure 2) and contained volunteers who were exposed to multiple impacts at the same or increasing severity.
Figure 1.
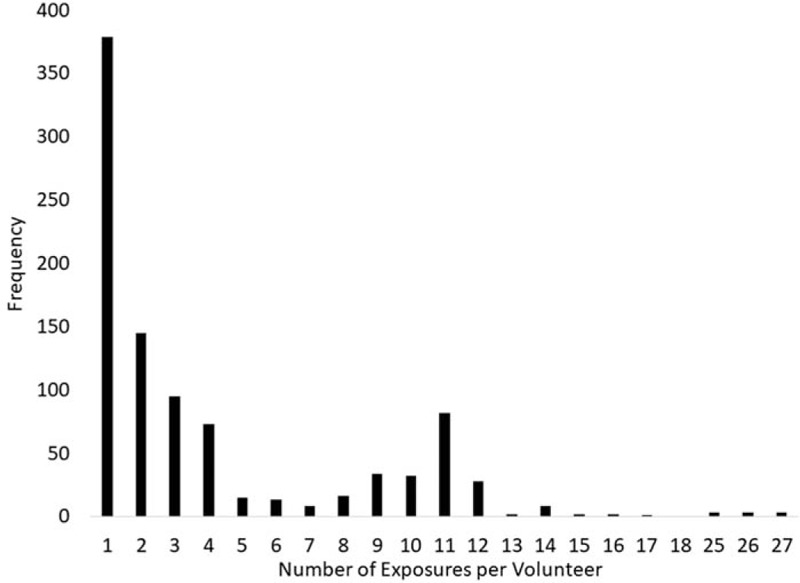
Distribution of the number of exposures for each volunteer showing that the majority of volunteers were exposed to less than five impacts.
Figure 2.
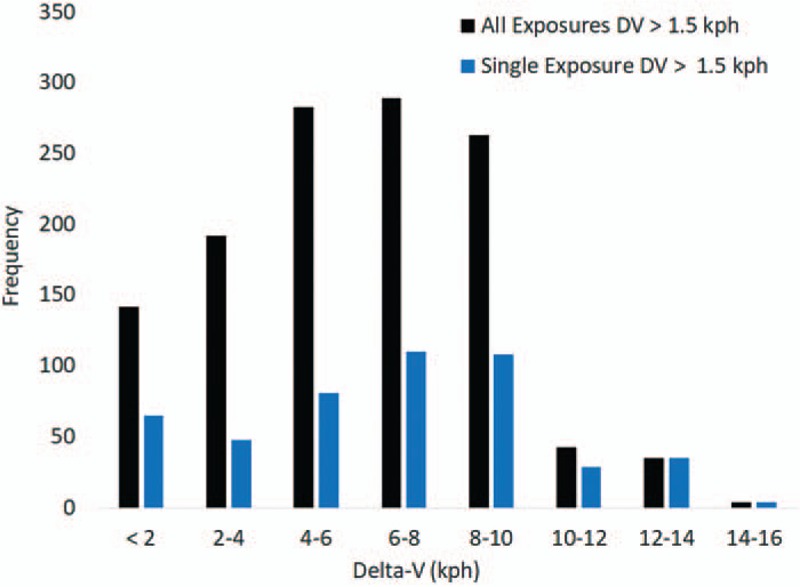
Distribution of impact exposures by vehicle change in speed for all exposures and for single exposure by volunteer at the greatest severity.
As the outcome of multiple impacts on a single volunteer would weigh the data artificially, separate analyses were conducted on a dataset containing repeated testing and a second dataset that only contained a single impact exposure with the greatest change in velocity. Eliminating the multiple impacts produced a dataset with 480 volunteers with a single exposure (Figure 2). In this dataset with a single exposure, if the volunteer reported symptoms following their exposure then the observation was counted as causing the symptom. In the dataset with multiple exposures for a single volunteer, if the volunteer reported symptoms after exposure to the entire series, each exposure was counted as causing symptoms unless the study was designed with a time gap between testing to allow symptoms to subside.
Symptoms
The incidence of neck symptoms within the volunteer database was assessed as a function of impact severity within the dataset containing single exposures above a delta-V of 1.5 kph. The symptom rate for males and females were similar and increased as delta-V increased from less than 8 to greater than 8 kph (Figure 3). On the basis of Fisher exact tests, only males (P = 0.026) showed a statistically significant increase in symptom rate between the 1.5 to 8 kph and 8 to 16 kph groups. There was no difference between symptom rates for the male and female volunteers. The lack of difference by gender means the entire dataset can be analyzed without accounting for gender.
Figure 3.
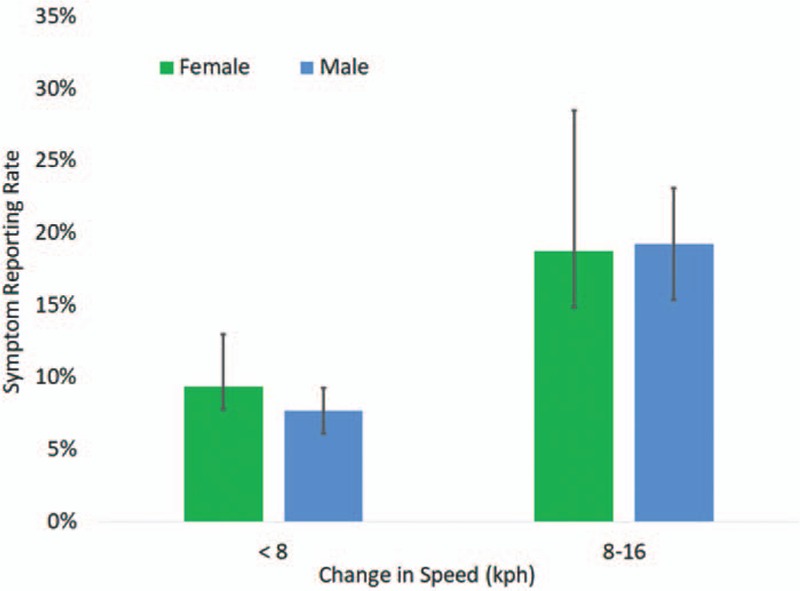
Incidence of neck symptoms for volunteers by gender and range in change in speed showing that there was no meaningful difference by gender.
Within the single exposure data, the majority of the volunteers were unaware of the impending impact (n = 422). A smaller portion indicated that the volunteer was braced (n = 28) at the time of the rear impact. The proportion of volunteers reporting symptoms was greater for those who were braced (25%) than those who were not braced (7.6%). This difference was statistically significant using Fisher exact test (P = 0.0065). The difference between impact severity for the braced (7.2, Std. Dev = 2.3 kph) and relaxed (6.3, Std. Dev = 3.3 kph) volunteers was 1 kph and was not statistically significant (P = 0.51).
Volunteer age was similar between males and females and ranged from 17 to 63 years (Figure 4). Within the single exposure data, volunteers who reported symptoms tended to be older (age = 37) than those who did not have symptoms (age = 31) (P < 0.0001).
Figure 4.
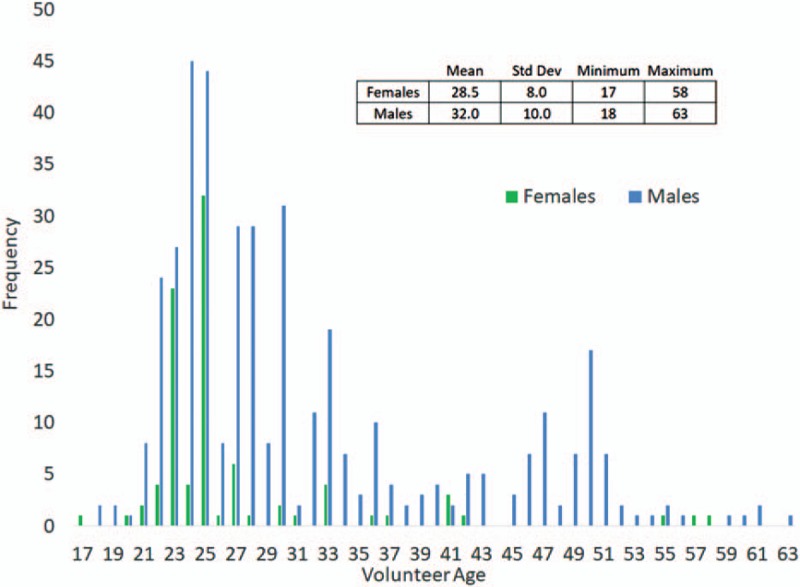
Distribution of volunteer age and the number of volunteers within the dataset by age and gender.
Operating Characteristic Curve
The OC curve was calculated on the basis of the 480 nonrepeated tests within the volunteer dataset. The level of certainty based on the entire single exposure dataset (Figure 5) showed that there would be a 95% chance of having a volunteer within the dataset that did sustain an injury if the underlying risk of injury was about 0.6%. For impacts with a change in speed less than and greater than 8 kph, the certainty was 84% and 64%, respectively. Therefore, the large number of single exposure volunteer tests provide a strong indicator that the likelihood of injury during a minor rear impact is remote. This is consistent with the general acceptance that human volunteers can be exposed to these events without a risk of injury.
Figure 5.
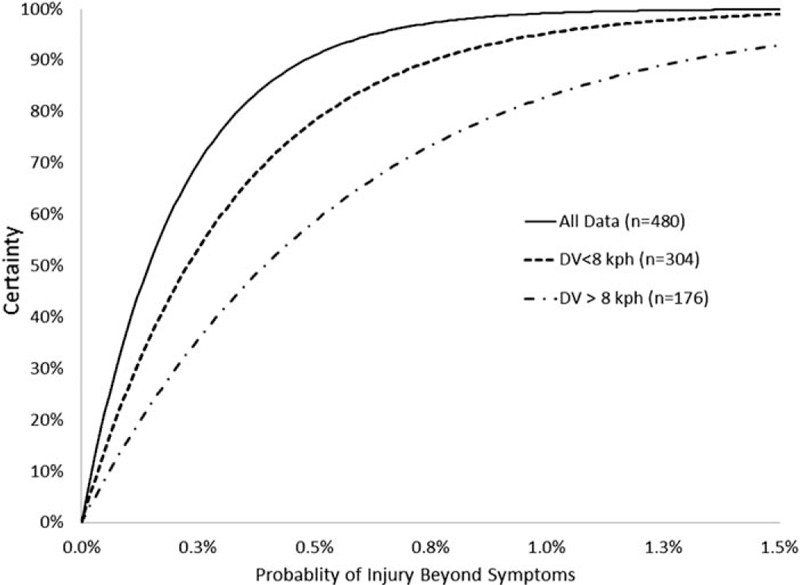
Operating characteristic curve showing the certainty of no injury beyond muscle strains occurring within the sample dataset as a function of the underlying likelihood of injury. Certainty plotted using a single exposure for each volunteer with a change in speed greater than 1.5 kph, volunteers exposed to an impact less than 8 kph (and greater than 1.5 kph), and volunteers exposed to impacts greater than 8 kph.
Head and Neck Biomechanics
The head acceleration and neck moments reported within the volunteer studies were summarized. Twelve studies reported head acceleration experienced by the volunteers.5,15,23,26,30,32,37,38,40,59,67,68 These studies provide 125 data points for head acceleration as a function of vehicle change in speed (Figure 6). These points were fit to a polynomial and power trendline, which produced similar accuracy. For the average change in speed of 7.2 kph (Std. Dev. = 3.2 kph), the average head acceleration was 8 g (Std. Dev. = 6 g).
Figure 6.
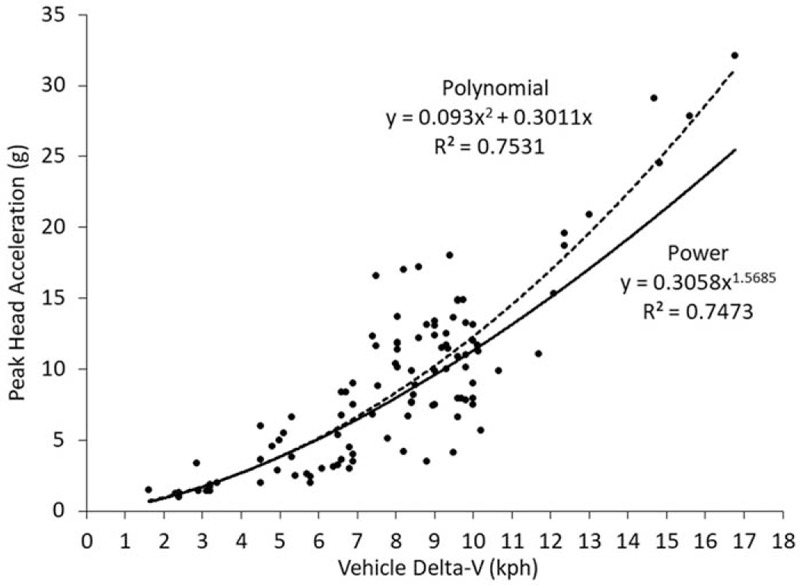
Head acceleration within the human volunteer dataset as a function of vehicle change in speed. Peak values were fit using a polynomial and power regression model.
Neck moments experienced by human volunteers have also been reported within previous studies (Figure 7). The values for neck extension were reported for volunteers with and without head restraints.64,74,75 These studies demonstrate the primary loading condition for the cervical spine in rear impacts is comprised of tension and extension forces. The magnitude of the extension moment experienced by the human volunteers during rear impacts is similar to those experienced by volunteer during everyday and vigorous activities.64,76,77
Figure 7.
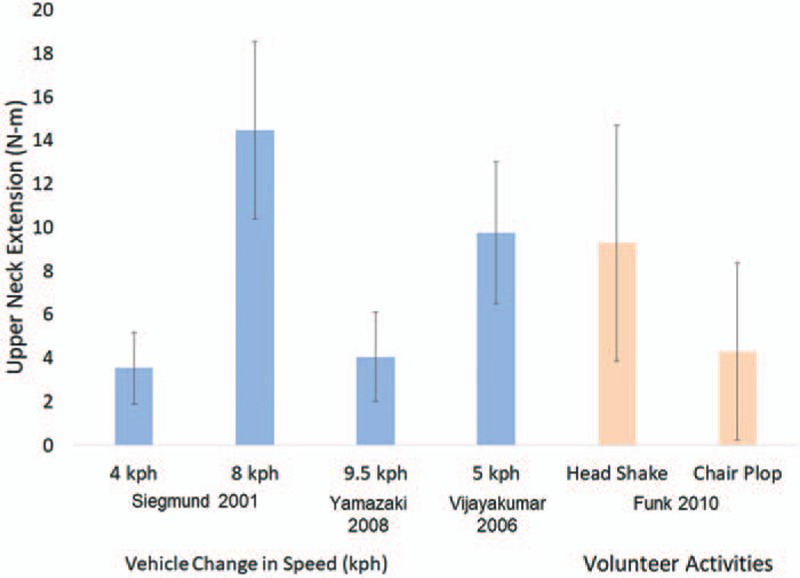
Peak neck extension experienced by volunteers during low-speed rear impacts and voluntary activities. Neck moment calculated at the upper neck using inverse dynamics and accounting for head restraint forces when applicable.
Real-world Rear Impacts
The dataset of real-world crashes derived from the NASS database consisted of 2058 raw occupants that represent 1,313,136 occupants nationally. Within these occupants, 644 raw and 515,601 weighted occupants were exposed to a rear impact with a change in speed of 16 kph or less. The average age of the complete set of occupants was 38 years and the average change in speed, or delta-V was 20 kph.
The distribution of neck strain within the real-world rear impacts was evaluated using the AIS code within NASS. The distribution of neck strain demonstrated a slight dependence on change in speed, but only across large changes of impact severity (Figure 8). For impacts with a change in speed less than 16 kph, the rate of neck strain was 21%.
Figure 8.
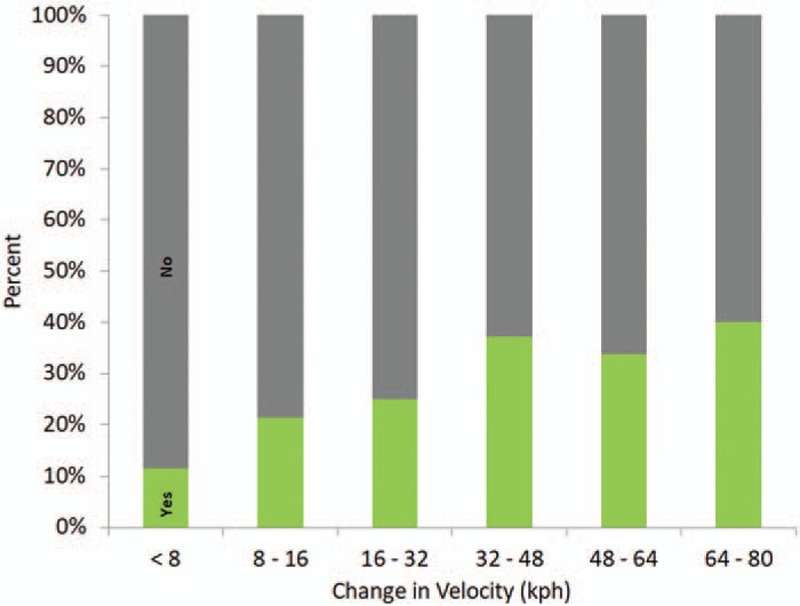
Distribution of neck strain within real-world crashes showing that the incidence of neck strain is not related to impact severity for impacts with a change in speed greater than 32 kph.
Within real-world rear impacts with a change in speed below 8 kph, females had a higher rate of symptoms; however, this difference was not statistically significant (P = 0.39). For impacts with a change in speed between 8 and 16 kph, the incidence of neck strain was greater for males, with no statistically significance from females (P = 0.60) (Figure 9). The rate of neck strain for rear impacts with a change in speed between 0 and 16 kph was 19% and 22% for the females and males, respectively.
Figure 9.
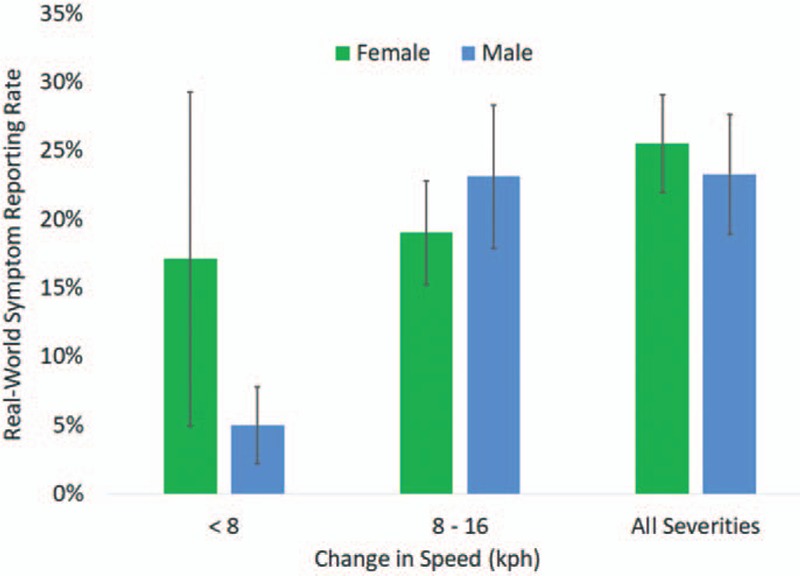
Incidence of neck strain by gender within real-world collisions. There were no statistically significant differences found between genders for the severity ranges.
Overall, the real-world data showed that the risk of any neck injury (AIS 2+) beyond muscle strain is small, even for high levels of change in speed (Figure 10). The likelihood of neck strain was significantly greater than more consequential, AIS 2+ injuries.
Figure 10.
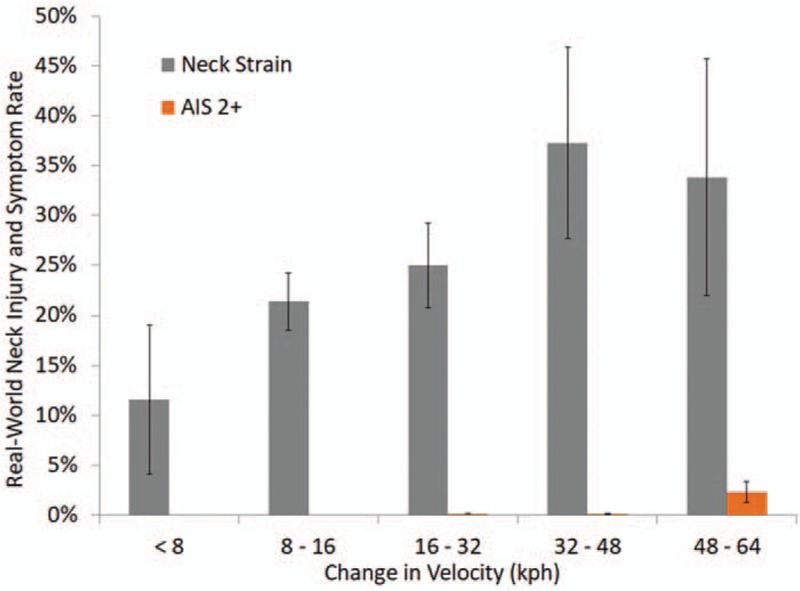
Risk of neck strain and AIS 2+ neck injuries in real-world database as a function of vehicle change in speed. The minimal risk of injuries at the AIS 2+ for impacts less than 16 kph is consistent with the lack of comparable injuries reported within the volunteer dataset.
Injury risk was also assessed using logistic regression analyses. For neck strain and AIS 2+ injuries, only a change in speed was found to be statistically significant. Age, gender, belt use, head restraint, and vehicle type were not statistically significant in predicting neck strain or AIS 2+ neck injuries.
DISCUSSION
The results of this study, using both experiment-based and real-world data, reinforce the general acceptance that human volunteers can be safely exposed to rear impacts of less than 18 kph without a meaningful risk of injury. Interestingly, both data sources produced similar rates of neck strain by gender and impact severity. This indicates that there is no reporting bias by the volunteers, some of whom are the authors of the articles. In addition, the similarity between the volunteer and real-world data indicate that any minor variation in head or body position that may be present in real-world collisions did not result in an increased rate of injury. Contrary to common belief, the volunteers that were reported as being braced had a higher rate of reporting symptoms than those that were not. The small underlying risk of injury indicated by the operating characteristic curve for the volunteer studies is consistent with the small risk of neck injury predicted by the real-world analysis.
The lack of injury to the volunteers results from the minor nature of the motion and forces they are exposed to as well as the direction of the forces applied to their bodies. Biomechanical research has shown that in order to produce a specific injury, a specific set of forces are required at the proper location and orientation. Experimental studies of the cervical and lumbar spine have demonstrated these mechanisms and have shown that spinal injury cannot be produced simply by being exposed to a motor vehicle collision. The lack of spinal injuries as a result of rear impacts is due to the lack of the specific mechanism to produce such injuries.
This study has limitations with respect to the conclusions that can be drawn. The volunteer dataset is limited to the information provided within the published work. The pre-impact screening of volunteers was not always addressed and when it was, there was only a brief discussion. Therefore, the health of the volunteers before the testing is not known at all, or to a limited extent for most of the volunteers.
The results of this study demonstrate that the incidence of symptoms of neck pain is directly related to the change in velocity experienced by the vehicle. This trend was similar for staged volunteer testing and real-world motor vehicle collisions. The number of volunteers and exposures within the volunteer testing is sufficient to provide a high degree of certainty that injury is not expected at the delta-V levels studied, even though subjective pain may occur for a short duration. This is not a surprising outcome given the lack of reported injuries, the minor nature of the motion and forces measured during these studies, and the ongoing use of research volunteers around the world. The similarities between real-world outcomes and staged collisions demonstrate that any preparation by the volunteers does not influence the risk of neck pain. Statistical analyses of real-world rear impacts confirm the low risk of more severe injuries at impacts of similar severity to the volunteer research.
Key Points
Previous biomechanical studies provided 1251 unique rear impact tests using human volunteers.
In volunteer studies, the rate of reporting symptoms of neck pain was related only to impact severity and was no different between male and female volunteers.
Real-world rear impacts and laboratory-based volunteer studies produced similar rates of neck strain indicating that the variations associated with real-world events do not alter the likelihood of neck strain during a minor rear impact.
The lack of injury beyond neck strain in the volunteer studies is consistent with the minute risk of cervical injury predicted from a large number of real-world collisions.
Acknowledgments
The authors would like to acknowledge Dr. Robert Banks of Biodynamic Research Corporation (BRC) for his initial work in developing the volunteer database and Dr. James Funk of Biomechanics Consulting and Research (BIOCORE) for his technical assistance.
Footnotes
The manuscript submitted does not contain information about medical device(s)/drug(s).
No funds were received in support of this work.
Relevant financial activities outside the submitted work: consultancy, expert testimony.
References
- 1.Versteegen GJ, Kingma J, Meijler WJ, et al. Neck sprain after motor vehicle accidents in drivers and passengers. Eur Spine J 2000; 9:547–552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alpini D, Brugnoni G, Cesarani A. Whiplash Injuries: Diagnosis and Treatment. 2nd ed.Milan; New York: Springer; 2014. [Google Scholar]
- 3.Palepu V. Biomechanical effects of initial occupant seated posture during rear end impact injury. Dissertation. University of Toledo; 2013. [Google Scholar]
- 4.Ministry of Justice. Reducing the number and costs of whiplash claims. A consultation on arrangements concerning whiplash injuries in England and Wales. Consultation Paper CP17/2012. 2012 Dec. ISBN: 978010842525. [Google Scholar]
- 5.Anderson RD, Welcher JB, Szabo TJ, et al. Effect of Braking on Human Occupant and Vehicle Kinematics in Low Speed Rear-End Collisions: 980298. Warrendale, PA: Society of Automotive Engineers; 1998. [Google Scholar]
- 6.Bailey MN, Wong BC, Lawrence JM. Data and Methods for Estimating the Severity of Minor Impacts. Society of Automotive Engineers: 950352. 1995; Warrendale, PA: Society of Automotive Engineers, 139-174. [Google Scholar]
- 7.Blouin JS, Inglis JT, Siegmund GP. Auditory startle alters the response of human subjects exposed to a single whiplash-like perturbation. Spine (Phila Pa 1976) 2006; 31:146–154. [DOI] [PubMed] [Google Scholar]
- 8.Brault JR, Wheeler JB, Siegmund GP, et al. Clinical response of human subjects to rear-end automobile collisions. Arch Phys Med Rehabil 1998; 79:72–80. [DOI] [PubMed] [Google Scholar]
- 9.Braun TA, Jhoun JH, Braun MJ, et al. Rear-End Impact Testing with Human Test Subjects. 2001-01-0168. Warrendale, PA: Society of Automotive Engineers; 2001. [Google Scholar]
- 10.Carlsson A, Linder A, Davidsson J, et al. Dynamic kinematic responses of female volunteers in rear impacts and comparison to previous male volunteer tests. Traffic Inj Prev 2011; 12:347–357. [DOI] [PubMed] [Google Scholar]
- 11.Carlsson A, Siegmund GP, Linder A, Svernsson M. Motion of the head and neck of female and male volunteers in rear impact car-to-car tests at 4 and 8 km/h. Proceedings of the International IRCOBI Conference on Biomechanics of Injury, September 15–16, 2010, Hanover, Germany; 2010:29–40. [Google Scholar]
- 12.Castro WHM, Schilgen M, Meyer S, et al. Do ‘whiplash injuries’ occur in low speed rear-end impacts? Eur Spine J 1997; 6:366–375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Croft A, Haneline M, Freeman M. Differential Occupant Kinematics and Forces Between Frontal and Rear Automobile Impacts at Low Speed: Evidence for a Differential Injury Risk. Munich, Germany: IRCOBI; 2002. [Google Scholar]
- 14.Croft A, Haneline M, Freeman M. Low speed frontal crashes and low speed rear crashes: Is there a differential risk for injury? Association for the Advancement of Automotive Medicine 46th Annual Proceedings. September 30–October 2, 2002, Tempe, AZ; 2002:79–92. [PubMed] [Google Scholar]
- 15.Croft A, Herring P, Freeman M, et al. The neck injury criterion: future considerations. Accid Anal Prev 2002; 34:247–255. [DOI] [PubMed] [Google Scholar]
- 16.Croft AC, Philippens M. The RID2 Biofidelic Rear Impact Dummy: A Validation Study Using Human Subjects in Low Speed Rear Impact Full Scale Crash Tests. Neck Injury Criterion (NIC) Society of Automotive Engineers: 2006-01-0067. Warrendale, PA: Society of Automotive Engineers; 2006. [Google Scholar]
- 17.Davidsson J, Deutscher C, Hell W, et al. Human volunteer kinematics in rear-end sled collisions. International Research Council on the Biomechanics of Impact (IRCOBI) Conference, SAE #1998-13-0020. September 16–18, 1998, Gothenburg, Sweden; 1998:289–302. [Google Scholar]
- 18.Dehner C, Elbel M, Schick S, et al. Risk of injury of the cervical spine in sled tests in female volunteers. Clin Biomech (Bristol, Avon) 2007; 22:615–622. [DOI] [PubMed] [Google Scholar]
- 19.Dehner C, Schick S, Kraus M, et al. Muscle activity influence on the kinematics of the cervical spine in rear-end sled tests in female volunteers. Traffic Inj Prev 2013; 14:369–377. [DOI] [PubMed] [Google Scholar]
- 20.Eichberger A, Geigl BC, Moser A, et al. Comparison of Different Car Seats Regarding Head-Neck Kinematics of Volunteers During Rear End Impact. Dublin, Ireland: International IRCOBI Conference on The Biomechanics of Impact; 1996. [Google Scholar]
- 21.Eichberger A, Steffan H, Geigl B, et al. Evaluation of the Applicability of the Neck Injury Criterion (NIC) in Reaf End Impacts on the Basis of Human Subject Tests. Goteborg, Sweden: International Conference on the Biomechanics of Impact; 1998. [Google Scholar]
- 22.Society of Automotive Engineers, Erickson M. Fidelity of Biodynamic Simulation Models for Low Speed Collinear Rear Crash Conditions. 2012. [Google Scholar]
- 23.Fugger TF, Jr, Randles BC, Welcher JB, et al. Vehicle and Occupant Kinematics in Low-Speed Override/Underride Collisions. 2003-01-0158. Warrendale, PA: Society of Automotive Engineers; 2003. [Google Scholar]
- 24.Furbish C, Ivory M, Hoffman M, et al. Steering column loads and upper extremity motions during low speed rear-end collisions. Rear Impact, Rollover, and Side Impacts, 2011 (SP-2303), Warrendale, PA, SAE #2011-01-0275. 2011. [Google Scholar]
- 25.Geigl BC, Steffan H, Leinzinger P, et al. The Movement of Head and Cervical Spine During Rearend Impact. International IRCOBI Conference on The Biomechanics of Impact. Lyon, France: IRCOBI Secretariat; 1994. 127–138. [Google Scholar]
- 26.Goodwin V, Martin D, Sackett R, et al. Vehicle and Occupant Response in Low Speed Car to Barrier Override Impacts. SAE Technical Paper: 1999-01-0442. Warrendale, PA: Society of Automotive Engineers; 1999. [Google Scholar]
- 27.Hell W, Schick S, Langwielder K, et al. Biomechanics of cervical spine injuries in rear end car impacts: influence of car seats and possible evaluation criteria. Traffic Inj Prev 2002; 3:127–140. [Google Scholar]
- 28.Hong S, Park S, Lee Y, et al. Low-speed rear impact sled tests involving human subjects. Ann Adv Automot Med 2013; 57:353–356. [PMC free article] [PubMed] [Google Scholar]
- 29.Hynd D, Willis C, Roberts A. TRL rear impact volunteer testing: Method and measurements. Proceedings of D16-WG 5.2 Workshop on Biomechanical Experiments, September 21, 2004, TRL Limited, Berks, United Kingdom; 2004:18–28. [Google Scholar]
- 30.Ivory MA, Furbish CJ, Hoffman MR, et al. Brake pedal response and occupant kinematics during low speed rear-end collisions. Accident Reconstruction, 2010, Warrendale, PA, SAE #2010-01-0067. 2010. [Google Scholar]
- 31.Kaneoka K, Ono K, Inami S, et al. Motion analysis of cervical vertebrae during whiplash loading. Spine (Phila Pa 1976) 1999; 24:763–769. discussion 70. [DOI] [PubMed] [Google Scholar]
- 32.Keifer OP, Layson PD, Reckamp BC. The effects of seated position on occupant kinematics in low-speed rear-end impacts. Accident Reconstruction 2005 (SP-1930). Warrendale, PA, SAE #2005-01-1204. 2005. [Google Scholar]
- 33.Kumar S, Ferrari R, Narayan Y. Kinematic and electromyographic response to whiplash-type impacts. Effects of head rotation and trunk flexion: summary of research. Clin Biomech (Bristol, Avon) 2005; 20:553–568. [DOI] [PubMed] [Google Scholar]
- 34.Kumar S, Ferrari R, Narayan Y. Effect of head rotation in whiplash-type rear impacts. Spine J 2005; 5:130–139. [DOI] [PubMed] [Google Scholar]
- 35.Kumar S, Narayan Y, Amell T. Role of awareness in head-neck acceleration in low velocity rear-end impacts. Accid Anal Prev 2000; 32:233–241. [DOI] [PubMed] [Google Scholar]
- 36.Lawrence J, Siegmund G. Seat back and head restraint response during low-speed rear-end automobile collisions. Accid Anal Prev 2000; 32:219–232. [DOI] [PubMed] [Google Scholar]
- 37.Linder A, Lovsund P, Steffan H. Validation of the BioRID P3 Against Volunteer and PMHS Test Data and Comparison to the Hybrid III in Low-Velocity Rear-End Impacts. 43nd Annual Proceedings of the Association for the Advancement of Automotive Medicine; 1999; Sitges, Spain:367--382. [Google Scholar]
- 38.Matsushita T, Sato TB, Hirabayashi K, et al. X-ray study of the human neck motion due to head inertia loading. Proceedings of the 38th Stapp Car Crash Conference (P-279). Warrendale, PA, SAE #942208. 1994:55–64. [Google Scholar]
- 39.McConnell WE, Howard RP, Guzman HM, et al. Analysis of human test subject kinematic responses to low velocity rear end impacts. Vehicle and Occupant Kinematics: Simulation and Modeling (SP-975). SAE #930889. Warrendale, PA, 1993:21–30. [Google Scholar]
- 40.McConnell WE, Howard RP, Van Poppel J, et al. Human head and neck kinematics after low velocity rear-end impacts: Understanding “whiplash”. 39th Stapp Car Crash Conference (P-299). Warrendale, PA, SAE #952724. 1995:215–238. [Google Scholar]
- 41.Mertz HJ, Patrick LM. Investigation of the kinematics and kinetics of whiplash. Proceedings of the 11th Stapp Car Crash Conference (P-20). Warrendale, PA SAE #670919. 1967:175–206. [Google Scholar]
- 42.Meyer S, Weber M, Castro W, et al. The Minimum Collision Velocity for Whiplash. Whiplash Injuries: Current Concepts in Prevention. Diagnosis and Treatment of the Cervical Whiplash Syndrome. 1998; Philadelphia, PA: Lippincott-Raven, 95–115. [Google Scholar]
- 43.Nielsen GP, Gough JP, Little DM, et al. Human subject responses to repeated low speed impacts using utility vehicles. Occupant Protection and Injury Assessment in the Automotive Crash Environment (SP-1231). Warrendale, PA, SAE #970394. 1997:189–212. [Google Scholar]
- 44.Nielsen GP, Gough JP, Little DM, et al. Repeated low speed impacts with utility vehicles and humans. Accident Reconstruction J 1996; 8:24.27–32,35–36,38. [Google Scholar]
- 45.Ono K, Ejima S, Yamazaki K, et al. Evaluation criteria for the reduction of minor neck injuries during rear-end impacts based on human volunteer experiments and accident reconstruction using human FE model simulations. International Research Council on the Biomechanics of Impact (IRCOBI) Conference, York, United Kingdom; 2009:381–398. [Google Scholar]
- 46.Ono K, Kaneoka K, Inami S. Influence of seat properties on human cervical vertebral motion and head/neck/torso kinematics during rear-end impacts. International Research Council on the Biomechanics of Impact (IRCOBI) Conference. Gothenburg, Sweden, SAE #1998-13-0021. 1998:303–318. [Google Scholar]
- 47.Ono K, Kaneoka K, Wittek A, Kajzer J. Cervical injury mechanism based on the analysis of human cervical vertebral motion and head-neck-torso kinematics during low speed rear impacts, SAE Technical Paper 973340, Warrendale, PA, 1997, 10.4271/973340. [DOI] [Google Scholar]
- 48.Ono K, Kanno M. Influences of the Physical Parameters on the Risk to Neck Injuries in Low Impact Speed Rear-end Collisions. Eindhoven, Netherlands: International IRCOBI Conference on the Biomechanics of Impacts; 1993. [DOI] [PubMed] [Google Scholar]
- 49.Pramudita J, Ono K, Ejima S, et al. Head/neck/torso behavior and cervical vertebral motion of human volunteers during low speed rear impact: Mini-sled tests with mass production car seat. International IRCOBI Conference. York, United Kingdom, 2007:219–232. [Google Scholar]
- 50.Roberts AK, Hynd D, Dixon PR, et al. Kinematics of the human spine in rear impact and the biofidelity of current dummies. Proceedings of the International Conference on Vehicle Safety 2002. Held May 22 at the IMECHE Headquarters, London, United Kingdom, 2002; 227–246. [Google Scholar]
- 51.Rosenbluth W, Hicks L. Evaluating low-speed rear-end impact severity and resultant occupant stress parameters. J Forensic Sci 1994; 39:1393–1424. [PubMed] [Google Scholar]
- 52.Sato F, Nakajima T, Ono K, et al. Dynamic Cervical Vertebral Motion of Female and Male Volunteers and Analysis of its Interaction with Head/Neck/Torso Behavior during Low-Speed Rear Impact. International Research Council on the Biomechanics of Impact (IRCOBI) Conference; September 10–12. Berlin, Germany; 2014:227–249. [Google Scholar]
- 53.Scott MW, McConnell WE, Guzman HM, et al. Comparison of human and ATD head kinematics during low speed rear end impacts. Human Surrogates: Design, Development and Side Impact Protection (SP-945). Warrendale, PA, SAE #930094. 1993:1–8. [Google Scholar]
- 54.Sekizuka M. Seat Designs for Whiplash Injury Lessening. Proc. 16th Int. Tech. Conf. on ESV. Windsor, Canada:1998. [Google Scholar]
- 55.Siegmund GP, Bailey MN, King DJ. Characteristics of specific automobile bumpers in low velocity impacts. Accident Reconstruction: Technology and Animation IV (SP-1030). SAE #940916. Warrendale, PA, 1994:333–372. [Google Scholar]
- 56.Siegmund GP, Sanderson DJ, Myers BS, et al. Rapid neck muscle adaptation alters the head kinematics of aware and unaware subjects undergoing multiple whiplash-like perturbations. J Biomech 2003; 36:473–482. [DOI] [PubMed] [Google Scholar]
- 57.Siegmund GP, Williamson PB. Speed Change (delta V) of Amusement Park Bumper Cars. Proceedings of the Canadian Multidisciplinary Road Safety Conference VIII. Saskatoon, Saskatchewan; 1993:299–308. [Google Scholar]
- 58.Society of Automotive Engineers, Szabo T, Welcher J. Human Subject Kinematics and Electromyographic Activity During Low Speed Rear Impacts. 1996; 962432. [Google Scholar]
- 59.Szabo TJ, Welcher JB, Anderson RD, et al. Human occupant kinematic response to low speed rear end impacts. Occupant Containment and Methods of Assessing Occupant Protection in the Crash Environment (SP-1045). Warrendale, PA, SAE #940532. 1994:23–36. [Google Scholar]
- 60.Tanner CB, Chen HF, Wiechel JF, et al. Vehicle and Car Occupant Response in Heavy Truck to Car Low-Speed Rear Impacts: 970120. Warrendale, PA: Society of Automotive Engineers; 1997. [Google Scholar]
- 61.Tencer A, Mirza S, Martin D. Yoganandan N, Pintar F, et al. Development of a retrofit anti-whiplash seat cushion based on studies of crash victims and human volunteers. Frontiers in Whiplash Trauma. The Netherlands: IOS Press; 2000. 389–405. [Google Scholar]
- 62.Tencer AF, Mirza S, Bensel K. The response of human volunteers to rear-end impacts; the effects of head restraint properties. Spine (Phila Pa 1976) 2001; 26:2432–2442. [DOI] [PubMed] [Google Scholar]
- 63.Van Den Kroonenberg A, Philippens M, Cappon H, et al. Human Head-Neck Response During Low-Speed Rear End Impacts: 983158. 1998; Warrendale, PA: Society of Automotive Engineers, 207–21. [Google Scholar]
- 64.Vijayakumar V, Scher I, Gloeckner DC, et al. Head Kinematics and Upper Neck Loading During Simulated Low-Speed Rear-End Collisions: A Comparison with Vigorous Activities of Daily Living: 2006-01-0247. Warrendale, PA: Society of Automotive Engineers; 2006. [Google Scholar]
- 65.Watanabe Y, Ichikawa H, Kayama O, et al. Relationships between occupant motion and seat characteristics in low-speed rear impacts. Occupant Protection (SP-1432). Warrendale, PA, SAE #1999-01-0635. 1999:13–22. [Google Scholar]
- 66.Welcher JB, Szabo TJ. Relationships between seat properties and human subject kinematics in rear impact tests. Accid Anal Prev 2001; 33:289–304. [DOI] [PubMed] [Google Scholar]
- 67.Welcher JB, Szabo TJ, Voss DP. Human Occupant Motion in Rear-End Impacts: Effects of Incremental Increases in Velocity Change: 2001-01-0899. Warrendale, PA: Society of Automotive Engineers; 2001. [Google Scholar]
- 68.West D, Gough J, Harper G. Low speed rear-end collision testing using human subjects. Accid Reconstr J 1993; 5:22–26. [Google Scholar]
- 69.Moss RT, Bardas AM, Hughes MC, Happer AJ. Injury symptom risk curves for occupants involved in rear end low speed motor vehicle collisions. Biomechanics 2005 (SP-1929). Warrendale, PA, SAE #2005-01-0296. 2005. [Google Scholar]
- 70.Nordhoff LS, Jr., Freeman MD, Siegmund GP. Human Subject Crash Testing. Innovations and Advances (PT-134). Warrendale, PA: SAE International; 2007; ISBN: 9780768019315. [Google Scholar]
- 71.Castro WH, Meyer SJ, Becke ME, et al. No stress: no whiplash? Prevalence of “whiplash” symptoms following exposure to a placebo rear-end collision. Int J Legal Med 2001; 114:316–322. [DOI] [PubMed] [Google Scholar]
- 72.AAAM. Abbreviated Injury Scale 2005: Update 2008. Association for the Advancement of Automotive Medicine; 2005. [PMC free article] [PubMed] [Google Scholar]
- 73.Blouin JS, Descarreaux M, Belanger-Gravel A, et al. Attenuation of human neck muscle activity following repeated imposed trunk-forward linear acceleration. Exp. Brain Res 2003; 150:458–464. [DOI] [PubMed] [Google Scholar]
- 74.Yamazaki K, Ono K, Ishii M. Biofidelity of Rear Impact Dummies in Low Speed Rear-End Impact: Comparison of Rigid Seat and Mass Production Car Seat in Human Volunteers. 2008; Bern, Switzerland: International Research Council on the Biomechanics of Injury, 323-38. [Google Scholar]
- 75.Siegmund G, Heinrichs B, Lawrence J, et al. Kinetic and kinematic responses of the RID2a, Hybrid III and human volunteers in low-speed rear-end collisions. Stapp Car Crash J 2001; 45:239–256. [DOI] [PubMed] [Google Scholar]
- 76.Bussone W, Prange M, Bove R, et al. Neck loads in playground activities in a pediatric population. SAE Int. J. Passeng. Cars - Mech. Syst 2012. 5. [Google Scholar]
- 77.Funk JR, Cormier JM, Bain CE, et al. Head and neck loading in everyday and vigorous activities. Ann Biomed Eng 2011; 39:766–776. [DOI] [PubMed] [Google Scholar]