

Abstract
Crossed renal ectopia with fusion is an extremely rare congenital anomaly with few reported cases of pelviureteric junction obstruction, which often involves the crossed-over kidney. To our knowledge, we describe the second case in literature to report an uncrossed kidney with pelviureteric junction obstruction and giant hydronephrosis, which obstructs the pelviureteric junction of the crossed-over kidney. The grossly hydronephrotic kidney was found to be poorly functioning and an aberrant crossing vessel was considered to be potentially involved, raising both diagnostic and management challenges. By reporting this case, we aim to stress the importance of adequate mapping collecting systems, drainage patterns and vascular supply in such crossed fused anomalies.
Keywords: Crossed fused renal ectopia, Pelviureteric junction obstruction, Hydronephrosis
Case history
A 47-year-old woman, with no known comorbidities, presented with a history of colicky abdominal pain in the right flank associated with progressive swelling, of 3 years’ duration. There was no history of change in bowel habits or genitourinary symptoms. Abdominal examination revealed a palpable lump occupying the entire right hemi-abdomen.
Abdominal ultrasonography revealed a grossly hydronephrotic kidney occupying the entire right flank and crossing the midline with empty left renal fossa. Her renal function was within normal limits. Computed tomography (CT) urography showed a cyst above and slightly anterior to the right kidney, 14 × 21 × 28 cm in size, with thickened and irregular wall and septa. There was a single ureter crossing the middle line to open into the left side of the bladder, consistent with a left-to-right crossed renal ectopia (Fig 1). The cyst was compressing the pelviureteric junction of the crossed-over kidney causing mild distended pelvis. There were neither calcified areas nor solid component or contrast level inside and no signs of metastatic disease were noticed elsewhere. A diagnosis of inferior crossed renal ectopia with fusion and giant hydronephrosis in the uncrossed kidney was considered. A possible renal artery pressing over the pelviureteric junction of the uncrossed kidney was also noted on CT. Static renal scan showed marked increased uptake in the crossed over kidney (87% of differential function), with no other renal tissue within the abdomen and pelvis (Fig 2).
Figure 1.
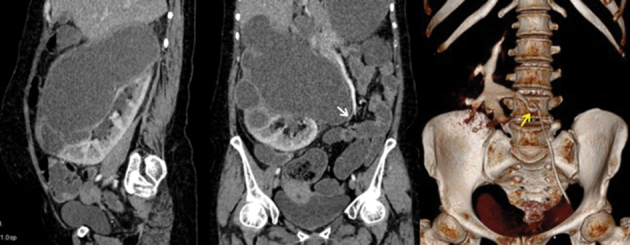
Sagittal and coronal computed tomography urography showing the left-to-right inferior crossed fused renal ectopia with giant hydronephrosis in the uncrossed kidney and mass effect on the pelviureteric junction of the crossed-over kidney (yellow arrow). An aberrant renal artery pressing over the pelviureteric junction of the uncrossed kidney was also noted (white arrow).
Figure 2.
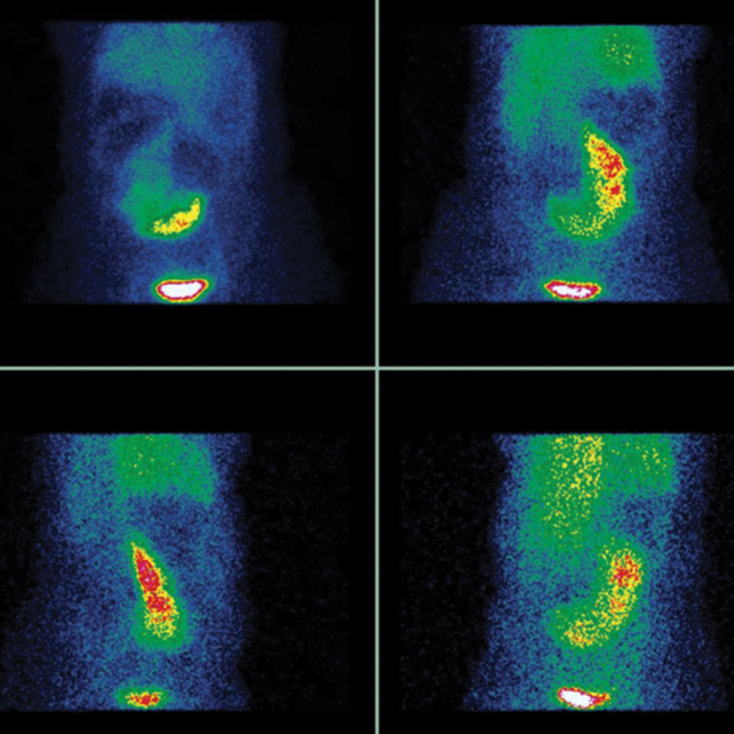
Static renal scan showing only one ectopic renal tissue of marked increased uptake (87% of differential function).
The patient consented to undergo retrograde insertion of double-J stent in the right ureter, with a plan to perform a pyeloplasty if ureteral stenting proved effective. Initial cystoscopic examination revealed two ureteric orifices and the right retrograde pyelography revealed a hairpin ureter filing into a grossly hydronephrotic ipsilateral collecting system, suggestive of pelviureteric junction obstruction in the uncrossed kidney (Fig 3). A double-J stent was successfully placed in the right ureter. Stenting of the ectopic ureter was also performed to allow intraoperative delineation and avoid iatrogenic injury if surgery would be indicated.
Figure 3.
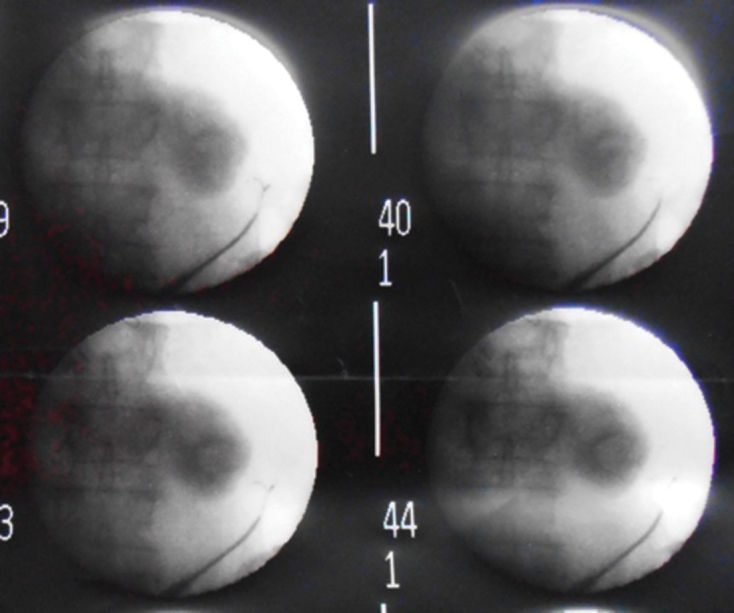
Right retrograde pyelogram showing a hairpin ureter filing into a grossly hydronephrotic ipsilateral collecting system.
The postoperative course was uneventful and the patient’s symptoms improved dramatically. Six weeks following stents placement, hydronephrosis was completely resolved in both renal moieties on CT urography, which also revealed no contrast uptake in the uncrossed kidney (Fig 4). The patient refused to have a nephrectomy, contrary to the clinical advice. Only definitive stent removal was performed and long-term follow-up strongly advised. During the 12 months following stent removal, the patient remained well, with normal renal function and no apparent evidence of hydronephrosis on follow-up ultrasound.
Figure 4.
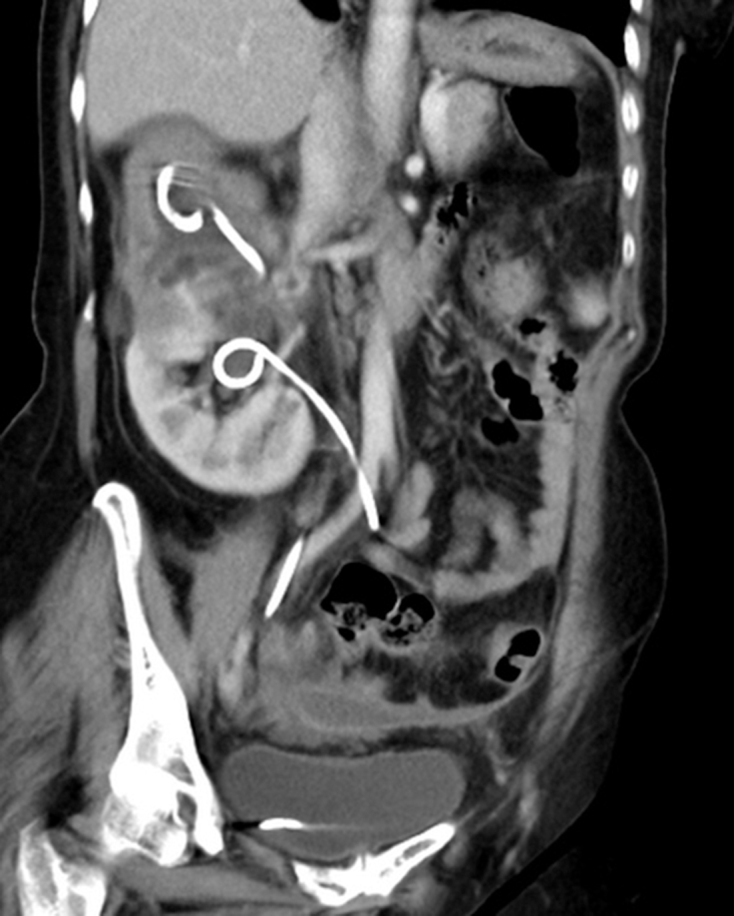
coronal computed tomography urography showing double J stents with neither hydronephrosis nor contrast uptake in the uncrossed kidney.
Discussion
Crossed renal ectopia is an uncommon congenital malformation, in which one kidney is located on the side opposite from which its ureter inserts into the bladder. Left to right crossover occurs more frequently than its counterpart and kidneys are fused together in roughly 90% of cases.1,2 Crossed fused ectopia is the most common fusion anomaly after horseshoe kidneys, detected in only 1:2000 autopsies with a slight male predominance (3:2). This entity is thought to result from the abnormal development and migration of the ureteric bud and metanephric blastema at 4–8 weeks of gestation.2 Crossed fused ectopia is divided into six subgroups based on the degree of fusion, location and rotation of the fused renal mass.1,2 Most commonly, the crossed ectopic kidney is inferior to the normally positioned kidney as in this case. Most cases remain unnoticed or are incidentally detected. Presenting symptoms include pain, dysuria, frequency, haematuria and a palpable mass. Complications like urinary tract infections, nephrolithiasis, pelviureteric junction obstruction and very rarely malignant tumours and renal dysplasia can be associated with such condition.1–3
The incidence of pelviureteric junction obstruction in ectopic kidneys ranges from 33% to 52%.3 Pelviureteric junction obstruction in crossed fusion anomalies, however, is uncommon, with only few cases listed in literature.3–5 Data regarding its incidence and natural history are currently lacking, but fused ectopic kidneys are more often involved.3,4 This is frequently due to their frequent abnormal shape, malrotation, high insertion of the ureter on the renal pelvis and aberrant crossing vasculature.3,5 Pelviureteric junction obstruction in orthotopic fused kidneys is an incredibly rare event. To our knowledge, only one such case has been documented in literature.3 Aside from potential aberrant vessels, the coexistence of these conditions is difficult to explain. The vascular supply to fused kidneys is actually variable and highly unpredictable; each kidney can be supplied by one or more vessels originating at a variable level from the aorta or common iliac vessels. As such, in fused inferior ectopia, vessels supplying the ectopic kidney might press over the pelviureteric junction and obstruct the collecting system of the orthotopic kidney, as seen in this case.
Crossed fused renal anomalies can usually be diagnosed and evaluated by multidetector CT urography or magnetic resonance imaging, which are reliable to assess the anatomy of collecting systems and ureters, vasculature supply and to screen for related complications.2 A renal static scan may also be a useful tool to diagnose such anomalies with a high degree of sensitivity and to evaluate the differential function of each moiety.6 In the current patient, these imaging techniques were limited by poor visualisation of the hypofunctional and grossly hydronephrotic uncrossed kidney, expanding the differential diagnosis to include cystic tumours and multicystic dysplasia. In these circumstances, cystoscopy with retrograde pyelography is often helpful in making a diagnosis, to screen for obstruction and to allow ureteral stenting if indicated, as in this case. Percutaneous nephrostomy with antegrade pyelography may offer an attractive, safe and effective alternative and should be considered in selected cases of obstructed fused kidneys, especially when retrograde manipulation is not indicated or has failed.7
Hydronephrosis in crossed-over kidney by compression effect of the grossly hydronephrotic uncrossed kidney is an unusual scenario.3 It may be explained by the fact that the ureters are closely adjacent to each other on their proximal portions in fused anomalies. A renal dynamic scan of the crossed moiety should have been performed before and after stents placement in our patient,3 to assess the drainage pattern and to identify the impact of extrinsic compression caused by the uncrossed unit.
There are currently no guidelines on the management of crossed fused renal ectopia. Fused kidneys rarely need to be separated. Asymptomatic patients should be followed without intervention. In a symptomatic patient, treatment should only be targeted at complications.1,2 This case could have been managed conservatively; open or laparoscopic pyeloplasty may be feasible and safe had initial ureteral stenting proved effective.3,4 Consequently, nephrectomy of the uncrossed kidney is a good treatment option, especially in symptomatic patients with mass effect on the collecting system of the crossed-over kidney. Unfortunately, our patient did refuse this surgical option and long-term follow-up was strongly recommended.
Conclusions
To our knowledge, this is only the second reported case in the literature of crossed fused renal ectopia with pelviureteric junction obstruction in the uncrossed kidney causing hydronephrosis in the crossed-over kidney. Individuals diagnosed with such a fused anomaly should be assessed for the drainage patterns of both kidneys as well as related aberrant or crossing vessels, especially in symptomatic patients who are candidate for surgical treatment. Conservative management can be used in selected cases. Nevertheless, nephrectomy of the hypofunctional and grossly hydronephrotic uncrossed kidney should have been the standard treatment option in this case.
References
- 1.Shapiro E, Bauer SB, Chow JS. Anomalies of the upper urinary tract : Wein AJ, Kavoussi LR, Novick AC, et al. Campbell-Walsh Urology. 10th ed. Philadelphia, PA: Saunders; 2012. 3140–145. [Google Scholar]
- 2.Bhatt K, Herts BR. Crossed fused renal ectopia. J Urol 2014. : 475–476. [DOI] [PubMed] [Google Scholar]
- 3.Hasan Z, Kumar B, Thakur A et al. Aberrant renal vessel causing hydronephrosis in crossed-fused ipsilateral ectopic kidney: a rare case report. Indian J Surg 2013; : 201–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Muruganandham K, Kumar A, Kumar S. Laparoscopic pyeloplasty for ureteropelvic junction obstruction in crossed fused ectopic pelvic kidney. Korean J Urol 2014; : 764–767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Guarino N, Tadini B, Camardi P et al. The incidence of associated urological abnormalities in children with renal ectopia. J Urol 2004; : 1,757–1,759. [DOI] [PubMed] [Google Scholar]
- 6.Moon EH, Kim MW, Kim YJ et al. Crossed fused renal ectopia: presentations on 99mTc-MAG3 Scan, 99mTc-DMSA SPECT, and Multidetector CT. Clin Nucl Med 2015; : 835–837. [DOI] [PubMed] [Google Scholar]
- 7.Bhojwani N, Hartman JB, Ahmed M et al. Management of ureteral obstruction in crossed fused renal ectopia: A case report. Can Urol Assoc J 2014; (9–10): E752–E754. [DOI] [PMC free article] [PubMed] [Google Scholar]