

Abstract
Our aim was to confirm earlier studies showing tcPO2 to be higher under clothing made with polyethylene terephalate (PET) fabric containing ceramic particles (CEL) compared to standard PET fabric. In previous studies PET garments were donned first to avoid possible persistent effects from ceramic particles. This study randomized donning sequence to avoid bias.
Methods
Subjects were randomized to don either PET shirts first (PETF n=73) or CEL first (CELF n=80), switching garments after 90 minutes. Skin temperature (ST), arterial oxygen saturation (O2sat), and tcPO2 were measured every 30 minutes.
Results
Baseline ST and O2 sat were nearly identical in the two groups. Baseline tcPO2 was modestly higher in the CELF group than with PETF: 66.4 ± 18.9 vs. 63.9 ± 18.8 mmHg (n.s). Independent of donning sequence, tcPO2 measurements 90 minutes after wearing CEL were 6.7% higher than after 90 minutes wearing PET (p<0.0003). Sequence analysis found tcPO2 in PETF subjects to gradually rise before and after switching garments, but tcPO2 fell immediately after switching garments in CELF subjects. PETF baseline O2sat of 98.1 ± 1.3 increased insignificantly after 90 minutes, and then increased further to 98.6 ± 0.8 after wearing CEL ninety minutes (p=0.0001). CELF baseline O2sat of 97.9 ± 1.7 increased to 98.5 ± 1.1 90 minutes after donning CEL (p=0.0002) and fell to 98.3 ± 1.0 ninety minutes after switching to PET (p=0.0033).
Conclusions
The ability of ceramic-embedded fabric to induce higher tcPO2 measurements is not due to sequence bias.
Keywords: FIR-emitting garments, Randomized controlled trial, Ceramic-embedded fabric, Ceramic-embedded clothing, Far-infrared radiation, Tissue oxygenation, Transcutaneous PO2, Donning sequence
Background
Far-infrared radiation (FIR) therapy has been used for the treatment of a variety of diseases and conditions [1-3], including pain [4-6], wound healing [7], recovery from exercise [8], heart failure [9], and disturbed sleep [10]. Often the FIR is delivered from an electrically-powered device such as an infrared heat lamp, an infrared sauna or a tourmaline/ jade heating pad. However, there is an alternative way to deliver FIR to the body, which is by the wearing of clothing constructed from ceramic particle-embedded fibers that emit FIR when powered by the wearer's own body heat [3]. Celliant® (CEL, Hologenix LLC, Santa Monica, CA) yarn for clothing is constructed from standard polyester (polyethylene terephthalate --PET) extruded molten from a two-barrel machine with a proprietary mixture of ceramic particles added to produce a bicompatible fiber, with the center-load containing approximately 1 micron diameter particles [11]. CEL has been designed to capture heat from the body and re-emit radiant far-infrared energy to induce health benefits, and is thought to improve sleep and speed recovery from exercise. In one randomized clinical trial CEL socks were found to decrease chronic foot pain [12]. Tree previous unpublished studies examined the effects of CEL garments on transcutaneous partial pressure of oxygen (tcPO2) using Clark electrodes placed on the skin underneath either control PET garments or active CEL garments (http://www.pureenergysleep.ca/ clinical-studies/). Lavery in 2003 studied 20 subjects with diabetes and peripheral vascular disease wearing socks and gloves made from PET or CEL while resting quietly. With PET socks, foot tcPO2 levels fell on average 2.6% from baseline over 60 minutes, compared to an increase of 4.7% after 60 minutes wearing CEL socks. Hand tcPO2 increased 15.4% while wearing PET gloves for 60 minutes, compared to a significantly greater increase (30.8%) wearing CEL. A study in 13 normal subjects (McClue and Lavery, 2005, unpublished) compared tcPO2 values of the hands and feet after wearing either PET or CEL garments. One hour of wearing CEL gloves induced mean tcPO2 values in the hand to be 25.0% higher than those found with PET. Foot tcPO2 was 10.2% higher under CEL socks than under PET socks; both hand and foot differences were significant.
Gordon in 2009 measured tcPO2 in 24 healthy volunteers wearing either PET or CEL shirts. After one hour the tcPO2 was 7.1% higher under CEL shirts compared to PET shirts (p<0.05). No significant differences in mean blood pressure, heart rate, or temperature were found comparing measurements obtained while wearing CEL or PET. Due to a possible concern that the effects of CEL might persist after switching from active CEL garments to PET control garments, in these studies the PET garments were always worn first, before switching to CEL garments. This protocol could induce bias if, for example, tcPO2 steadily rises in resting subjects independent of fabric type. The current study compared measurements of skin temperature (ST), arterial oxygen saturation (O2sat) and tcPO2 obtained while subjects wore PET shirts or CEL shirts. In one group PET shirts were worn first and in the second CEL garments were worn first, with the order sequence being randomized. Our goal was to confirm earlier findings without risk of bias from influences of the sequence of wearing.
Methods
Between October 2013 and January 2014, healthy volunteers aged 18 to 60 were recruited for an IRB approved protocol via on-line advertisement for subjects that paid $25. The trial was registered at clinicaltrials.gov NCT02798640 (https://clinicaltrials.gov/ct2/show/ NCT02798640). The protocol was in accordance with the Declaration of Helsinki and informed consent was obtained. Exclusion criteria included cardiovascular disease, smoking, recreational drug use within 6 months, pregnancy, or consumption of alcohol within 48 hours or caffeine within 4 hours of enrolment. The garments employed were short sleeved shirts. PET and CEL garments were constructed at the same mill using either standard PET fiber or CEL fiber containing 1.25 % (mass ratio) proprietary ceramic particles. CEL and PET shirts were of identical fabrication and dernier differing only in color: PET was white and CEL was a light grey color (Figure 1).
Figure 1.

Appearance of CEL and PET shirts.
Subjects were blinded to shirt composition and donning sequence. Assignment to either donning CEL shirts first (CELF) or control PET shirts first (PETF) was based 1:1 on a random allocation table. Studies were performed at the same constant temperature (24.0 ± 0.88°C), in a constant humidity (37.1 ± 5.0%) room with overhead fluorescent lighting. Prior to donning the first shirt, if necessary the anterior right shoulder skin was shaved, followed by gentle application of a fine abrasive and cleaning with tape and isopropyl alcohol. A probe with an electrolyte fluid ring, Clark electrode and a heating element set to heat the skin to 44°C was applied attached to a Periflux System 5000 monitor (Perimed, Kings Park, New York) with continuous monitoring software (Perisoft v2.55) as previously described [12]. Left forearm volar skin temperature (ST) was determined with an infrared thermometer. Fingertip pulse oximeter probes (CMS50DL, Crucial Medical Systems, and Atlanta, Georgia) monitored arterial oxygen saturation (O2sat). After preparation, subjects donned the first shirt, and sat quietly. Subjects were allowed to read or play video games but not sleep or converse.
Recordings of ST, O2sat, and tcPO2 began to be collected once tcPO2 measurements were deemed stable, which generally required 10 to 15 minutes. The tcPO2 signal representing mean ± s.d. was sampled at 32 Hz over 5 minutes. If s.d. was > 2 mmHg, the data was rejected as unstable. Cases in which the electrode membrane had to be replaced during measurements were also rejected. In 23 subjects data was excluded for one of these two problems, but all 23 returned on a later day to successfully repeat the entire protocol. No other data was excluded and all enrolled subjects completed the protocol.
Once the initial tcPO2 signal stabilized, baseline measurements were obtained followed by recordings 30, 60, and 90 minutes after baseline (A30, A60. A90). After the A90 measurement, subjects were encouraged to walk about, relieve themselves if necessary, and consume water and/or a small snack. The break interval was approximately 15 minutes. After the break, subjects donned the second shirt and resumed quiet sitting. A second set of measurements was obtained 30, 60, and 90 minutes after tcPO2 stabilized (B30, B60 and B90). Sample size was based on measurement of the variance in tcPO2 in 45 subjects with power analysis indicating that a minimum of 147 subjects would be required to achieve a 95% confidence level and power of 80%. Statistical analyses were performed only after all data had been acquired with subgroup analysis based only on gender and donning sequence.
Results
Table 1 shows the demographics of the study population. The subjects were 54.3% male; 62.5% of the CELF sequence and 45.2% of the ConF sequence subjects were male (p=0.047, chi square test with Yates' correction). The age, height, weight, and BMI distribution were similar in the CELF and ConF subjects with no significant differences. Overall 52% of the subjects were Caucasian, 22% African-American, 16% Hispanic, 8% Asian, and 1% other – the ethnic distributions were comparable in the active and control sequences (53, 18, 20, 9, and 1% versus 52, 26, 20, 9, and 1%) (Table 1).
Table 1. Subject demographics.
| Subject | % Male | Age (years) | Heights (inches) | Weights (ibs) | BMI |
|---|---|---|---|---|---|
| All (n=153) | 54.3 | 38.3 ± 12.3 | 67.4 ± 3.9 | 167.2 ± 42.9 | 25.7 ± 5.5 |
| CELF (n=180) | 62.5a | 37.9 ± 12.1 | 67.5 ± 3.8 | 171.3 ± 43.5 | 26.2 ± 5.7 |
| PETF (n=73) | 45.2a | 38.7 ± 12.6 | 67.2 ± 4.0 | 162.8 ± 40.3 | 25.0 ± 5.2 |
p=0.047, chi-square.
As shown in Table 2 is the baseline physiologic parameters. Mean baseline skin temperatures were nearly identical in the CELF and PETF groups 33.1 ± 0.9°C for CELF and 33.2 ± 1.1°C for PETF, as were baseline tcPO2 and O2sat. There were gender differences in baseline physiologic parameters: men had higher ST, lower O2sat, and lower tcPO2 then women. Mean baseline tcPO2 was 2.5 mmHg higher in the CELF group compared to the PETF group, (66.4 ± 18.9 versus 63.9 ± 18.8 mmHg) but not significantly (p=0.424 unpaired t test) (Table 2).
Table 2. Baseline physiologic parameters.
| Subject | tcPO2 (mmHg) | ST (°C) | %O2Sat |
|---|---|---|---|
| All (n=153) | 64.9 ± 18.5 | 33.1 ± 1.0 | 98.0 ± 1.3 |
| Male (n=83) | 60.2 ± 18.5a | 33.3 ± 0.9d | 97.6 ± 1.7f |
| Female (n=70) | 70.3 ± 17.2a | 32.9 ± 1.2d | 98.5 ± 1.1f |
| CELF (n=80) | 66.4 ± 18.9 | 33.1 ± 0.9 | 98.0 ± 1.0 |
| CELF Male (n=50) | 62.9 ± 18.1b | 33.3 ± 0.8e | 97.6 ± 1.9g |
| CELF Female (n=30) | 70.7 ± 18.1b | 32.6 ± 1.0e | 98.5 ± 0.9g |
| PETF (n=73) | 63.9 ± 18.8 | 33.2 ± 1.1 | 98.1 ± 1.3 |
| PETF Male (n=33) | 56.2 ± 18.6c | 33.3 ± 1.1 | 97.5 ± 1.3h |
| PETF Female (n=40) | 70.0 ± 16.7c | 33.3 ± 1.1 | 98.5 ± 1.3h |
p=0.0008
p=0.059
p=0.003
p=0.01
p=0.0009
p<0.001
p=0.023
p=0.003
Table 3 shows ST and O2sat measurements. The mean baseline ST for all subjects was 33.1 ± 1.0°C, significantly higher (p<0.0001, paired t test) than mean 32.7± 1.1°C ST for all combined B90 measurements (the last measurements in each groups (data not shown). The difference between baseline and final B90 ST was significant in the CELF group (p<0.0001, paired t test) but not in the PETF group.
Table 3. Effects of Garments on ST and O2Sat.
| ST (°C) | |||
|---|---|---|---|
| Baseline | CEL 90 minutes | PET 90 minutes | |
| All | 33.1 ± 1.0 | 32.8 ± 1.0 | 32.6 ± 1.0 |
| CELF | 33.1 ± 1.0a | 32.8 ± 1.0 | 32.4 ± 1.0a |
| PETF | 33.2 ± 1.1b | 32.9 ± 1.1b | 32.8 ± 1.0 |
| %O2 Sat | |||
| Baseline | CEL 90 minutes | PET 90 minutes | |
| All | 98.0 ± 1.3 | 98.5 ± 0.8c | 98.2 ± 1.0c |
| CELF | 97.9 ± 1.7e | 98.5 ± 1.1 e,f | 98.3 ± 1.0f |
| PETF | 98.1 ± 1.3d | 98.6 ± 0.8d | 98.2 ± 1.2 |
p<0.0001, paired t test
p=0.064, paired t test
p<0.0001 paired t test
p=0.0001, paired t test
p=0.0002, paired t test
p=0.003, paired t test
In contrast to the fall in ST observed from beginning to end of testing, O2sat increased from beginning to end. Combining all subjects, the mean baseline O2sat was 98.0 ± 1.3 compared to a mean value of 98.4 ± 0.9 for all B90 measurements (data not shown, p<0.0001, paired t test). Mean O2sat for all subjects after wearing CEL 90 minutes was significantly higher than O2sat for all subjects wearing PET 90 minutes (98.5 ± 0.8 vs. 98.2 ± 1.0, p<0.0001, paired t test). In PETF subjects, mean O2sat was 98.1 ± 1.3 at baseline and increased insignificantly (p=0.30 paired t test) to 98.2 ± 1.2 after ninety minutes, and then increased further to 98.6 ± 0.8 after wearing CEL shirts for ninety minutes (p=0.0001, paired t test). In the CELF group, however, mean baseline O2sat of 97.9±1.7 increased significantly to 98.5 ± 1.1 (p=0.0002, paired t test) after wearing CEL 90 minutes, then fell to 98.3 ± 1.0 after wearing PET 90 minutes (p=0.0033, paired t test) (Table 3).
Figure 2 shows tcPO2 for all the subjects combined, independent of donning sequence. Plotted are mean tcPO2 30, 60, and 90 minutes after donning each garment-the baseline value is the mean for all subjects. At each interval tcPO2 is significantly higher for CEL compared to controls (p ≤ 0.0003, paired t tests). At 30 minutes, the difference between CEL and PET tcPO2 levels was 3.42 ± 11.29 mmHg (5.5%); at 60 minutes 4.30 ± 10.16 mmHg (6.4%); and at 90 minutes 4.44 ± 9.51 mmHg (6.7%). Each point represents the combined mean ± s.e.m tcPO2 for all subjects at the specified time interval after establishment of stable tcPO2 measurements after donning PET or CEL shirts (Figure 2).
Figure 2.

Combined tcPO2 measurements for PET and CEL garments independent of donning sequence.
Figure 3 shows the same analysis performed comparing female and male subjects' responses to PET and CEL-the same pattern was observed, but the differences in tcPO2 levels based on garment worn were more pronounced in women. Each point represents mean values ± s.e.m combining data from one gender at the specified time interval after establishment of stable tcPO2 measurements (Figure 3).
Figure 3.
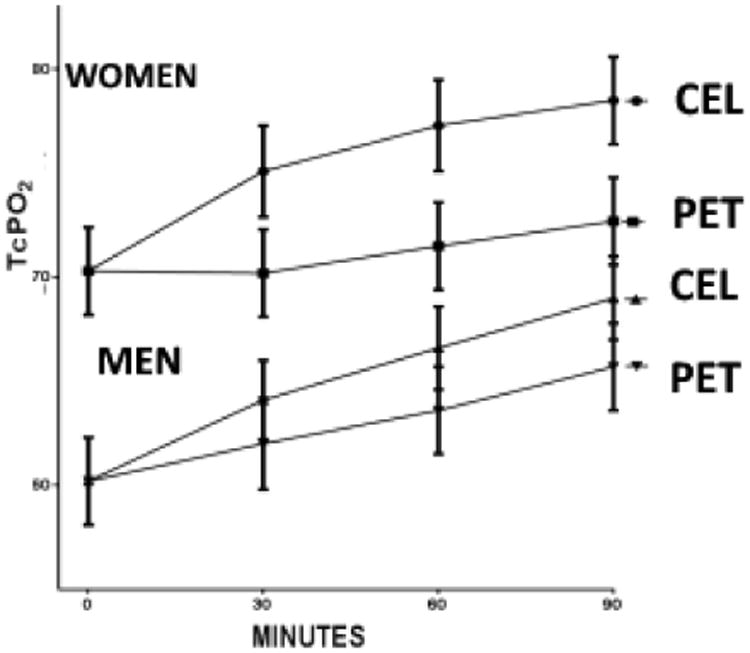
TcPO2 measurements based on gender.
Figure 4 shows the results of separating tcPO2 measurements based on donning sequence. The CELF and PETF baseline values are different. Mean tcPO2 is plotted in the temporal sequence with which it was measured. The PETF plot shows 30, 60, and 90 minute measurements obtained under PET shirts followed by 30, 60, and 90 minute measurements under CEL shirts. The plot for CELF subjects has the temporal sequence reversed: measurements obtained under CEL shirts are plotted before PET measurements. In the PETF group tcPO2 rose from baseline through A90 and continued to increase after switching garments. In contrast, tcPO2 levels in the CELF group increased through the A90 measurement but then fell after switching to PET. When the differences between tcPO2 measurements at each time interval are separately compared within sequence groups, i.e., 30 minute tcPO2 values for PET versus CEL in the CELF group, without inclusion of data from the PETF group and vice versa, two separate trends emerge. In the PETF group, differences between tcPO2 levels under PET vs. CEL are highly significant (p<0.0001) for each 30-minute interval by paired t testing. In contrast, in the CELF group, differences in tcPO2 between CEL and PET garments at 30 and 60 minutes are not significant, but approach significance at 90 minutes (p=0.051). Data from male and female subjects were combined and depicted in the sequence with which they were obtained (Figure 4).
Figure 4.

TcPO2 based on donning sequence.
When the same sequence analysis was applied to each gender, the same patterns were seen: tcPO2 levels fell in both CELF male and female subjects after switching from CEL to PET shirts, but continued to increase in both male and female PETF subjects after switching from PET to CEL (data not shown).
Discussion
This study measured changes in tcPO2 at 30 minute intervals up to 90 minutes using Clark electrodes placed under either PET and CEL shirts which differed only by the presence or absence of ceramic particles in otherwise identical PET fibers. Subjects were randomized to wear either PET or CEL garments first. In general, tcPO2 levels tended to increase while wearing either garment from baseline to end of the complete protocol. When tcPO2 measurements were combined without reference to the sequence with which garments were worn, measurements under CEL garments were 5.5% higher at 30 minutes and 6.7% higher at 90 minutes (p<0.05). A different pattern of tcPO2 measurements emerges, however, when tcPO2 is plotted based on donning sequence (Figure 4). In subjects who wore CEL first, tcPO2 fell immediately after switching to control PET garments, but the opposite result was seen in subjects who donned PET first--tcPO2 continued to rise after switching to CEL. The sequence data support the conclusion that wearing CEL is associated with greater increases in tcPO2 than PET, independent of donning sequence. Interestingly, the differences in tcPO2 measured at each interval between garments (e.g., mean A60 and mean B60 values) within the PETF group were significant, but not in the CELF group. This finding, in conjunction with the sequence pattern suggests that CEL effects might persist long enough to influence measurements taken after switching to PET. The 9.7% difference in mean tcPO2 levels between PET and CEL in the PETF group at 90 minutes (68.2 mmHg versus 74.9 mmHg) is comparable to results of the previous studies which employed that sequence.
CELF subjects had a mean baseline tcPO2 that was 2.5 mmHg higher than mean for PETF baseline, but this alone should not skew this analysis as most comparisons are based on paired measurements of the same individual, as, for example, the results shown in Figure 2. As baseline measurements were obtained after subjects donned the first garment, the higher baseline in CELF subjects conceivably resulted from ceramic particles influencing tcPO2 during the interval required to achieve stable measurements.
Another factor, the greater proportion of males to females in the CELF group versus PETF (62.5% vs. 45.2%) could have skewed the data analysis to show more of effects by CEL than is indeed the case, but as the men had lower baseline tcPO2 levels, and showed a moderately lower response to CEL than women, this seems unlikely.
If ST or core temperatures were higher under CEL than PET, then differences in tcPO2 might be due to heat induced vasodilation of the dermal microcirculation. Our study did not directly measure either core temperature or ST directly under the shirts, but the ST measurements from the subject's uncovered forearm make this explanation seem unlikely-ST generally fell throughout the protocol while tcPO2 generally rose. If temperature were the dominant factor influencing tcPO2, the later should have fallen in parallel with ST. Further, tcPO2 measurements entail heating skin to 44 °C, which should minimize the impact of variations in core or surface temperatures.
O2sat measurements differed when data from both sequence groups were combined. Ninety minutes after wearing CEL, mean O2sat was 98.5% for all subjects, significantly higher than the mean O2sat of 98.2% measured 90 minutes after donning PET. The pattern of change in O2sat with time in each group paralleled that observed with tcPO2. In PETF subjects, baseline O2sat rose slightly after 90 minutes of wearing PET, and then rose significantly more after 90 minutes wearing CEL With CELF subjects, baseline O2sat increased significantly over 90 minutes while wearing CEL, and after switching garments decreased significantly over 90 minutes while wearing PET. The modest similarity in the kinetic patterns observed with O2sat and tcPO2 measurements suggests they might be the result of the same ceramic particle influence. This raises the question of what is the underlying mechanism for the tcPO2 changes observed. Ceramic particles absorb heat (whether that be radiant, converted or conducted) emitted from the body, and then re-emit the thermal energy as IR (with a peak at 9.4 μm) back into the body. Re-emission occurs near the same wavelength as absorption, but may be at slightly a longer wavelength due to differences in temperature between the body and the fabric. This is not an energy neutral phenomenon, as the ceramics decrease the loss of infrared energy away from the body, those otherwise escapes through normal clothing.
The likely net result is increased absorption of FIR energy into the skin and underlying tissues. A recent study by scientists at Exponent Consulting compared the emissivity of PET fabric with or without CEL particles using sophisticated optical spectroscopic techniques. The intensity of infrared emission between 7.5 to 14 μm was 2.1% greater with fabric containing CEL particles (1.22% by weight) compared to fabric without ceramic particles [13]. This finding is consistent with the finding that the absorption co-efficient of the ceramic particles in the infrared spectrum was higher than the absorption co-efficient of pure PET fibers. In other words, the PET fibers are semi-transparent to infrared radiation, while the CEL particles are opaque. A follow-up study from the same group examined in more detail the influence of the ceramic particles on the infrared reflectance of the PET fabric, and measured the transmission, and absorption [14]. This analysis modeled the effects of the particles on infrared radiation incident upon the skin, as a function of wavelength, skin temperature, and ambient temperature, proportion of ceramic particles, air velocity, and influence of sunlight. The findings confirmed that the addition of ceramic particles to PET fabric leads to increased incidence of infrared radiation upon the skin at wavelengths longer than 4 μm, with a maximum effect at approximately 9.4 μm. The effect was attributed to increased absorption of infrared radiation at shorter wavelengths and reemission at longer wavelengths.
Increased emission of infrared from PET fibers with ceramic particles has the potential to interact with molecular and cellular structures by increasing the vibrational energy stored in chemical bonds, particularly in water clusters in cell membranes and cellular organelles. Perturbation of the vibrational energy of water clusters could affect the tertiary conformation of protein molecules tightly associated with this “nanostructured” water [15,16]. Low intensity far infrared (FIR-wavelength >14 um) lamps and topically applied (non-powered) FIR-emitting ceramic materials have been shown to induce cellular changes in vitro, and produce physiologic changes in both preclinical animal models and clinical studies. In none of these studies were the effects associated with significant changes in temperature, consistent with the low power associated with both far infrared lamps and non-powered ceramics in thermal equilibrium with skin (on the order of 0.1-1 mW/cm2 [3]. In vitro studies have found infrared radiation to inhibit cellular proliferation and be associated with increased reactive oxygen species; decreased production of intracellular nitric oxide and heat shock protein; inhibition of prostaglandin E2 synthesis; inhibition of kinase dependent nuclear signalling; and decreased production of inflammatory mediators and cell adhesion molecules [4,5,17-19].
Preclinical studies of infrared effects have shown inhibition of prostaglandin mediated inflammation in a rabbit arthritis model and delayed onset of muscle contraction induced fatigue [20]. Particular relevant to our findings are two reports in rats, one showing that infrared increased skin blood flow [21] and the other showed that infrared accelerated wound healing [7].
Three clinical studies have reported that blood flow was increased by infrared exposure from powered IR sources or non-powered ceramics [2,22,23] and one clinical study found alleviation of the symptoms of Raynaud's syndrome with ceramic impregnated gloves [24]. Other clinical studies with topically applied ceramic materials have demonstrated changes in body measurements (fat loss) [25,26], reduced dysmenorrhea [27], and improved lactation [28].
The increase in tcPO2 observed in this study likely is a consequence of increased oxygen availability in infrared illuminated tissue, possibly through a vasodilatory effect on the dermal circulation or, alternatively, effects on oxygen binding to hemoglobin. Although our understanding of the mechanism responsible for the effect of ceramic polyester composites on tcPO2 still incomplete, our data confirm that it is a real scientific phenomenon. Even without completely understanding the effect, it may be possible to design ceramic polyester composite garments or dressings that could improve wound healing, which is both sensitive to tissue perfusion and a critical problem for patients with diabetes. The recent decision by the US FDA that CEL garments will be regulated as medical devices and as general wellness products (http://www.medicaldevices-business-review.com/news/fda-determines-celliant-products-meet-criteria-as-medical-devices-260717-5882229) encourages clinical testing in multiple disease indications.
Conclusion
The present study has added to the body of evidence that suggest that FIR-emitting garments can exert real measurable physiological effects, and deserve further study for medical indications. Especially the potential for ceramic-embedded fabrics to improve skin and wound perfusion has particular relevance to diabetes and warrants further study.
Acknowledgments
Funding: Conduct of the study was supported entirely by Hologenix LLC. Michael R Hamblin was supported by US NIH grant R01AI050875.
Footnotes
Ethics Approval and Consent to Participate: Between October 2013 and January 2014, healthy volunteers aged 18 to 60 were recruited for an IRB approved protocol via on-line advertisement for subjects that were paid $25. The trial was registered at clinicaltrials.gov NCT02798640 (https://clinicaltrials.gov/ct2/show/NCT02798640). The protocol was in accordance with the Declaration of Helsinki and informed consent was obtained.
Consent to Publish: Not applicable, no identifying data
Availability of Data and Materials: The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding authors on reasonable request.
Competing Interests: KW was an employee of Hologenix, the other authors have received consulting fees and sponsored research support from Hologenix.
References
- 1.Tsai SR, Hamblin MR. Biological effects and medical applications of infrared radiation. J Photochem Photobiol B. 2017;170:197–207. doi: 10.1016/j.jphotobiol.2017.04.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Inoue S, Kabaya M. Biological activities caused by far-infrared radiation. Int J Biometeorol. 1989;33:145–150. doi: 10.1007/BF01084598. [DOI] [PubMed] [Google Scholar]
- 3.Vatansever F, Hamblin MR. Far infrared radiation (FIR): its biological effects and medical applications. Photonics Lasers Med. 2012;4:255–266. doi: 10.1515/plm-2012-0034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lai CH, Leung TK, Peng CW, Chang KH, Lai MJ, et al. Effects of far-infrared irradiation on myofascial neck pain: a randomized, double-blind, placebo-controlled pilot study. J Altern Complement Med. 2014;20:123–129. doi: 10.1089/acm.2013.0122. [DOI] [PubMed] [Google Scholar]
- 5.Lai YT, Chan HL, Lin SH, Lin CC, Li SY, et al. Far-infrared ray patches relieve pain and improve skin sensitivity in myofascial pain syndrome: A double-blind randomized controlled study. Complement Ther Med. 2017;35:127–132. doi: 10.1016/j.ctim.2017.10.007. [DOI] [PubMed] [Google Scholar]
- 6.Lee CH, Roh JW, Lim CY, Hong JH, Lee JK, Min EG. A multicenter, randomized, double-blind, placebo-controlled trial evaluating the efficacy and safety of a far infrared-emitting sericite belt in patients with primary dysmenorrhea. Complement Ther Med. 2011;19:187–193. doi: 10.1016/j.ctim.2011.06.004. [DOI] [PubMed] [Google Scholar]
- 7.Toyokawa H, Matsui Y, Uhara J, Tsuchiya H, Teshima S, et al. Promotive effects of far-infrared ray on full-thickness skin wound healing in rats. Exp Biol Med (Maywood) 2003;228:724–729. doi: 10.1177/153537020322800612. [DOI] [PubMed] [Google Scholar]
- 8.Loturco I, Abad CCC, Nakamura FY, Ramos SP, Kobal R, et al. Effects of far infrared rays emitting clothing on recovery after an intense plyometric exercise bout applied to elite soccer players: a randomized double-blind placebo-controlled trial. Biol Sport. 2016;33:277–283. doi: 10.5604/20831862.1208479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lima MV, Ochiai ME, Vieira KN, Scipioni A, Cardoso JN, et al. Thermal vasodilation using a portable infrared thermal blanket in decompensated heart failure. Int Heart J. 2014;55:433–439. doi: 10.1536/ihj.14-096. [DOI] [PubMed] [Google Scholar]
- 10.Honda K, Inoue S. Sleep-enhancing effects of far-infrared radiation in rats. Int J Biometeorol. 1988;32:92–94. doi: 10.1007/BF01044900. [DOI] [PubMed] [Google Scholar]
- 11.Schnurer JH, Klein RM, Horinek DD. Polymeric fiber composition and method U.P.U. B2, Editor. USA; 2004. [Google Scholar]
- 12.York RM, Gordon IL. Effect of optically modified polyethylene terephthalate fiber socks on chronic foot pain. BMC Complement Altern Med. 2009;9:10. doi: 10.1186/1472-6882-9-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pooley MA, et al. Engineered emissivity of textile fabrics by the inclusion of ceramic particles. Opt Express. 2016;24:10556–10564. doi: 10.1364/OE.24.010556. [DOI] [PubMed] [Google Scholar]
- 14.Anderson DM, et al. Infrared radiative properties and thermal modeling of ceramic-embedded textile fabrics. Biomed Opt Express. 2017;8:1698–1711. doi: 10.1364/BOE.8.001698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pollack GH. Water, Energy and Life: Fresh Views from the Water's Edge. Int J Des Nat Ecodyn. 2015;5:27–29. doi: 10.2495/DNE-V5-N1-27-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Martseniuk LS. The Properties of Water Nanostructures in Nanosystems. In: Fesenko O, Yatsenko L, editors. Nanoplasmonics, Nano-Optics, Nanocomposites, and Surface Studies. Springer; New York: 2001. pp. 133–148. 2014. [Google Scholar]
- 17.Leung TK, Chen CH, Tsai SY, Hsiao G, Lee CM. Effects of far infrared rays irradiated from ceramic material (BIOCERAMIC) on psychological stress-conditioned elevated heart rate, blood pressure, and oxidative stress-suppressed cardiac contractility. Chin J Physiol. 2012;55:323–330. doi: 10.4077/CJP.2012.BAA037. [DOI] [PubMed] [Google Scholar]
- 18.Leung TK, Kuo CH, Lee CM, Kan NW, Hou CW. Physiological effects of bioceramic material: harvard step, resting metabolic rate and treadmill running assessments. Chin J Physiol. 2013;56:334–340. doi: 10.4077/CJP.2013.BAB132. [DOI] [PubMed] [Google Scholar]
- 19.Leung TK, Lee CM, Tsai SY, Chen YC, Chao JS. A Pilot Study of Ceramic Powder Far-Infrared Ray Irradiation (cFIR) on Physiology: Observation of Cell Cultures and Amphibian Skeletal Muscle. Chin J Physiol. 2011;54:247–54. doi: 10.4077/CJP.2011.AMM044. [DOI] [PubMed] [Google Scholar]
- 20.Leung TK, Chen CH, Lai CH, Lee CM, Chen CC, et al. Bone and joint protection ability of ceramic material with biological effects. Chin J Physiol. 2012;55:47–54. doi: 10.4077/CJP.2012.AMM113. [DOI] [PubMed] [Google Scholar]
- 21.Yu SY, Chiu JH, Yang SD, Hsu YC, Lui WY, et al. Biological effect of far-infrared therapy on increasing skin microcirculation in rats. Photodermatol Photoimmunol Photomed. 2006;22:78–86. doi: 10.1111/j.1600-0781.2006.00208.x. [DOI] [PubMed] [Google Scholar]
- 22.Lin CC, Liu XM, Peyton K, Wang H, Yang WC, et al. Far infrared therapy inhibits vascular endothelial inflammation via the induction of heme oxygenase-1. Arterioscler Thromb Vasc Biol. 2008;28:739–45. doi: 10.1161/ATVBAHA.107.160085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Yoo BH, Park CM, Oh TJ, Han SH, Kang HH, et al. Investigation of jewelry powders radiating far-infrared rays and the biological effects on human skin. J Cosmet Sci. 2002;53:175–184. [PubMed] [Google Scholar]
- 24.Ko GD, Berbrayer D. Effect of ceramic-impregnated “thermofow” gloves on patients with Raynaud's syndrome: randomized, placebo-controlled study. Altern Med Rev. 2002;7:328–335. [PubMed] [Google Scholar]
- 25.Conrado LA, Munin E. Reduction in body measurements after use of a garment made with synthetic fibers embedded with ceramic nanoparticles. J Cosmet Dermatol. 2011;10:30–35. doi: 10.1111/j.1473-2165.2010.00537.x. [DOI] [PubMed] [Google Scholar]
- 26.Conrado LA, Munin E. Reductions in body measurements promoted by a garment containing ceramic nanoparticles: a 4-month follow-up study. J Cosmet Dermatol. 2013;12:18–24. doi: 10.1111/jocd.12027. [DOI] [PubMed] [Google Scholar]
- 27.Ke YM, Ou MC, Ho CK, Lin YS, Liu HY, et al. Effects of somatothermal far-infrared ray on primary dysmenorrhea: a pilot study. Evid Based Complement Alternat Med. 2012;2012:240314. doi: 10.1155/2012/240314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ogita S, Imanaka M, Matsuo S, Takebayashi T, Nakai Y, et al. Effects of far-infrared radiation on lactation. Ann Physiol Anthropol. 1990;9:83–91. doi: 10.2114/ahs1983.9.83. [DOI] [PubMed] [Google Scholar]